Significance of the Glasgow Prognostic Score in Predicting the Postoperative Outcome of Patients with Stage III Gastric Cancer


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Treatment
2.2. Data Collection and Follow-Up
2.3. Glasgow Prognostic Score
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bureau of Health Promotion Department of Health. Health Registry Annual Report 2016; Bureau of Health Promotion Department of Health: Beijing, China, 2016. Available online: https://www.hpa.gov.tw/Pages/List.aspx?nodeid=269 (accessed on 28 May 2019).
- National Cancer Institute. Cancer Stat Facts: Stomach Cancer; U.S. Department of Health & Human Services: Washington, DC, USA, 2016. Available online: https://seer.cancer.gov/statfacts/html/stomach.html (accessed on 28 May 2019).
- Chen, J.-S.; Hung, C.-Y.; Liu, K.-H.; Tsai, C.-Y.; Kuo, Y.-C.; Hsu, J.-T.; Chou, W.-C. Factors related to patient propensity to receive adjuvant chemotherapy and outcomes in stage III gastric cancer cases after D2 surgery. Asian J. Surg. 2019, 42, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Ejaz, A.; Kim, Y.; Squires, M.H.; Poultsides, G.A.; Fields, R.C.; Schmidt, C.; Weber, S.M.; Votanopoulos, K.; Maithel, S.K.; et al. Rates and Patterns of Recurrence after Curative Intent Resection for Gastric Cancer: A United States Multi-Institutional Analysis. J. Am. Coll. Surg. 2014, 219, 664–675. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Huang, C.; Sun, Y.; Su, X.; Cao, H.; Xue, Y.; Suo, J.; Tao, K.; He, X.; Wei, H.; et al. Morbidity and Mortality of Laparoscopic Versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: A Randomized Controlled Trial. J. Clin. Oncol. 2016, 34, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Maehara, Y.; Hasuda, S.; Koga, T.; Tokunaga, E.; Kakeji, Y.; Sugimachi, K. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer. BJS 2000, 87, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.-L.; Huang, K.-H.; Chen, J.-H.; Lo, S.-S.; Hsieh, M.-C.; Shen, K.-H.; Li, A.F.-Y.; Niu, D.-M.; Chiou, S.-H.; Wu, C.-W. Comparison of the Survival Difference Between AJCC 6th and 7th Editions for Gastric Cancer Patients. World J. Surg. 2011, 35, 2723–2729. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Tanaka, K.; Fushiya, N.; Koike, K.; Nishino, H.; Matsushima, M.; et al. The Glasgow Prognostic Score, an inflammation based prognostic score, predicts survival in patients with hepatocellular carcinoma. BMC Cancer 2013, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, O.H.; Akan, S.; Urkmez, A.; Yildirim, C.; Sahin, A.; Verit, A. Preoperative Glasgow prognostic score as a predictor of primary bladder cancer recurrence. Mol. Clin. Oncol. 2016, 5, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Hiki, N.; Nunobe, S.; Kumagai, K.; Kubota, T.; Aikou, S.; Sano, T.; Yamaguchi, T. Prognostic importance of the inflammation-based Glasgow prognostic score in patients with gastric cancer. Br. J. Cancer 2012, 107, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Ueno, D.; Matsumoto, H.; Kubota, H.; Higashida, M.; Akiyama, T.; Shiotani, A.; Hirai, T. Prognostic factors for gastrectomy in elderly patients with gastric cancer. World J. Surg. Oncol. 2017, 15, 59. [Google Scholar] [CrossRef] [PubMed]
- Inamoto, T.; Matsuyama, H.; Sakano, S.; Ibuki, N.; Takahara, K.; Komura, K.; Takai, T.; Tsujino, T.; Yoshikawa, Y.; Minami, K.; et al. The systemic inflammation-based Glasgow Prognostic Score as a powerful prognostic factor in patients with upper tract urothelial carcinoma. Oncotarget 2017, 8, 113248–113257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, S.; Nie, R.; Chen, Y.; Qiu, H.; Li, X.; Chen, X.; Xu, L.; Yang, L.; Sun, X.; Li, Y.; et al. Glasgow Prognostic Score is superior to ECOG PS as a prognostic factor in patients with gastric cancer with peritoneal seeding. Oncol. Lett. 2018, 15, 4193–4200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nozoe, T.; Iguchi, T.; Egashira, A.; Adachi, E.; Matsukuma, A.; Ezaki, T. Significance of modified Glasgow prognostic score as a useful indicator for prognosis of patients with gastric carcinoma. Am. J. Surg. 2011, 201, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.-X.; Su, Z.-J.; Zhang, J.-H.; Wang, C.-R.; Ke, S.-Y. A comparison of the prognostic value of preoperative inflammation-based scores and TNM stage in patients with gastric cancer. OncoTargets Ther. 2015, 8, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- Melling, N.; Grüning, A.; Tachezy, M.; Nentwich, M.; Reeh, M.; Uzunoglu, F.G.; Vashist, Y.K.; Izbicki, J.R.; Bogoevski, D. Prof Glasgow Prognostic Score may be a prognostic index for overall and perioperative survival in gastric cancer without perioperative treatment. Surgery 2016, 159, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-C.; Liu, K.-H.; Hung, C.-Y.; Tsai, C.-Y.; Hsu, J.-T.; Yeh, T.-S.; Chen, J.-S.; Kuo, Y.-C.; Hung, Y.-S.; Chou, W.-C. Adjuvant Chemotherapy Improves Survival in Stage III Gastric Cancer after D2 Surgery. J. Cancer 2018, 9, 81–91. [Google Scholar] [CrossRef]
- Charlson, M.; Wells, M.T.; Ullman, R.; King, F.; Shmukler, C. The Charlson Comorbidity Index Can Be Used Prospectively to Identify Patients Who Will Incur High Future Costs. PLOS ONE 2014, 9, e112479. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Jun, C.H.; Ki, H.S.; Lee, K.H.; Park, K.J.; Park, S.Y.; Cho, S.B.; Park, C.H.; Joo, Y.E.; Kim, H.S.; Choi, S.K.; et al. Impact of serum C-reactive protein level on the prognosis of patients with hepatocellular carcinoma undergoing TACE. Clin. Mol. Hepatol. 2013, 19, 70–77. [Google Scholar] [CrossRef]
- Allin, K.H.; Nordestgaard, B.G. Elevated C-reactive protein in the diagnosis, prognosis, and cause of cancer. Crit. Rev. Clin. Lab. Sci. 2011, 48, 155–170. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C.; Watson, W.S.; O’Gorman, P.; Preston, T.; Scott, H.R.; McArdle, C.S. Albumin Concentrations Are Primarily Determined by the Body Cell Mass and the Systemic Inflammatory Response in Cancer Patients with Weight Loss. Nutr. Cancer 2001, 39, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Porporato, P.E. Understanding cachexia as a cancer metabolism syndrome. Oncogenesis 2016, 5, e200. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.F.; Huang, P.W.; Chen, J.S.; Chen, Y.Y.; Lu, C.H.; Chang, P.H.; Hung, Y.S.; Chou, W.C. Prognostic Factors for Advanced Pancreatic Cancer Treated with Gemcitabine Plus S-1: Retrospective Analysis and Development of a Prognostic Model. Cancers 2019, 11, 57. [Google Scholar] [CrossRef] [PubMed]
- Mohri, Y.; Tanaka, K.; Ohi, M.; Toiyama, Y.; Yasuda, H.; Inoue, Y.; Uchida, K.; Kusunoki, M. Inflammation-based prognostic score as a predictor of postoperative gastric cancer. Anticancer Res. 2012, 32, 4581–4584. [Google Scholar] [PubMed]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [PubMed]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. MAGIC Trial Participants. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | GPS = 0 (n = 100), N (%) | GPS = 1 (n = 132), N (%) | GPS = 2 (n = 40), N (%) | p Value |
|---|---|---|---|---|
| Median age, year (range) | 63 (30–97) | 64 (26–90) | 70 (41–88) | 0.35 |
| Male sex | 56 (56.0) | 91 (68.9) | 29 (72.5) | 0.07 |
| ECOG PS | <0.001 | |||
| 0 or 1 | 88 (88.0) | 105 (79.5) | 23 (57.5) | |
| 2 | 10 (10.0) | 24 (18.2) | 10 (25.0) | |
| 3 | 2 (2.0) | 3 (2.3) | 7 (17.5) | |
| CCI | 0.11 | |||
| 0 | 50 (50.0) | 59 (44.7) | 11 (27.5) | |
| 1 | 33 (33.0) | 49 (37.1) | 15 (37.5) | |
| 2 | 13 (13.0) | 14 (10.6) | 8 (20.0) | |
| >2 | 4 (4.0) | 10 (7.6) | 6 (15.0) | |
| CEA, ng/dL | 0.87 | |||
| <5 | 85 (85.0) | 111 (84.1) | 35 (87.5) | |
| ≥5 | 15 (15.0) | 21 (15.9) | 5 (12.5) | |
| CA19-9, ng/dL | 0.54 | |||
| ≤37 | 85 (85.0) | 107 (81.1) | 31 (77.5) | |
| >37 | 15 (15.0) | 25 (18.9) | 9 (22.5) | |
| AJCC tumor stage | 0.005 | |||
| IIIA | 30 (30.0) | 25 (18.9) | 6 (15.0) | |
| IIIB | 42 (42.0) | 39 (29.5) | 17 (42.5) | |
| IIIC | 28 (28.0) | 68 (51.5) | 17 (42.5) | |
| Operation method | 0.11 | |||
| Total gastrectomy | 36 (36.0) | 59 (44.7) | 11 (27.5) | |
| Subtotal gastrectomy | 64 (64.0) | 73 (55.3) | 29 (72.5) | |
| Resection Margin | 0.038 | |||
| Positive | 7 (7.0) | 23 (17.4) | 8 (20.0) | |
| Negative | 93 (93.0) | 109 (82.6) | 32 (80.0) | |
| Adjuvant Chemotherapy | 0.15 | |||
| Yes | 74 (74.0) | 94 (71.2) | 23 (57.5) | |
| No | 26 (26.0) | 38 (28.2) | 17 (42.5) |
| Variable | Category | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | ||
| ECOG PS | 0 or 1 | 1 | 1 | ||
| 2 | 2.45 (1.72–3.47) | <0.001 | 2.23 (1.49–3.34) | <0.001 | |
| >3 | 5.30 (2.29–9.92) | <0.001 | 3.28 (1.58–6.79) | 0.001 | |
| CCI | 0 | 1 | 1 | ||
| 1 | 1.57 (1.14–2.17) | 0.006 | 1.20 (0.85–1.70) | 0.31 | |
| ≥2 | 1.87 (1.25–2.79) | 0.002 | 0.88 (0.54–1.43) | 0.61 | |
| AJCC stage | 3A | 1 | 1 | ||
| 3B | 1.67 (1.09–2.58) | 0.020 | 1.60 (1.02–2.50) | 0.040 | |
| 3C | 3.26 (2.15–4.94) | <0.001 | 2.36 (1.51–3.70) | <0.001 | |
| Body weight loss | <5% | 1 | 1 | ||
| ≥5% | 2.50 (1.84–3.41) | <0.001 | 1.75 (1.25–2.47) | 0.001 | |
| Vascular invasion | No | 1 | 1 | ||
| Yes | 1.70 (1.26–2.30) | 0.001 | 1.40 (1.00–1.97) | 0.050 | |
| Resection margin | Negative | 1 | 1 | ||
| Positive | 2.27 (1.50–3.43) | <0.001 | 1.44 (0.92–2.25) | 0.12 | |
| Operation method | TG | 1 | 1 | ||
| STG | 0.56 (0.44–0.79) | <0.001 | 1.60 (1.02–2.50) | 0.040 | |
| Adjuvant chemotherapy | No | 1 | |||
| yes | 0.47 (0.35–0.64) | <0.001 | 0.52 (0.38–0.72) | <0.001 | |
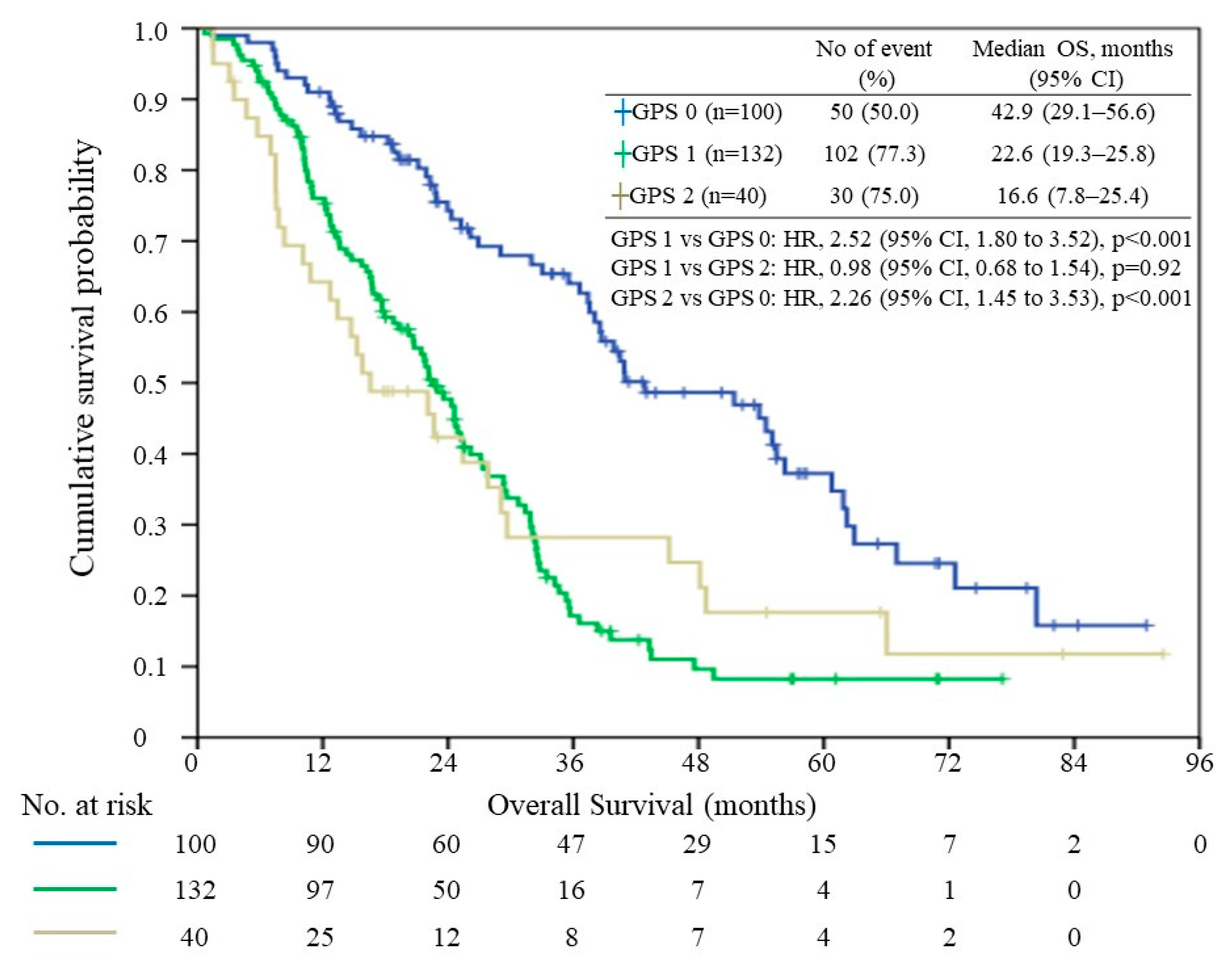
| GPS | 0 | 1 | |||
| 1 | 2.52 (1.80–3.52) | <0.001 | 1.97 (1.36–2.86) | <0.001 | |
| 2 | 2.26 (1.45–3.53) | <0.001 | 1.57 (0.96–2.57) | 0.07 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsueh, S.-W.; Liu, K.-H.; Hung, C.-Y.; Kuo, Y.-C.; Tsai, C.-Y.; Hsu, J.-T.; Hung, Y.-S.; Tsang, N.-M.; Chou, W.-C. Significance of the Glasgow Prognostic Score in Predicting the Postoperative Outcome of Patients with Stage III Gastric Cancer. J. Clin. Med. 2019, 8, 1448. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091448
Hsueh S-W, Liu K-H, Hung C-Y, Kuo Y-C, Tsai C-Y, Hsu J-T, Hung Y-S, Tsang N-M, Chou W-C. Significance of the Glasgow Prognostic Score in Predicting the Postoperative Outcome of Patients with Stage III Gastric Cancer. Journal of Clinical Medicine. 2019; 8(9):1448. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091448
Chicago/Turabian StyleHsueh, Shun-Wen, Keng-Hao Liu, Chia-Yen Hung, Yung-Chia Kuo, Chun-Yi Tsai, Jun-Te Hsu, Yu-Shin Hung, Ngan-Ming Tsang, and Wen-Chi Chou. 2019. "Significance of the Glasgow Prognostic Score in Predicting the Postoperative Outcome of Patients with Stage III Gastric Cancer" Journal of Clinical Medicine 8, no. 9: 1448. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091448