Oral Rehabilitation of Hypodontia Patients Using an Endosseous Dental Implant: Functional and Aesthetic Results

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Privacy
2.2. Study Design
2.3. Exclusion Criteria
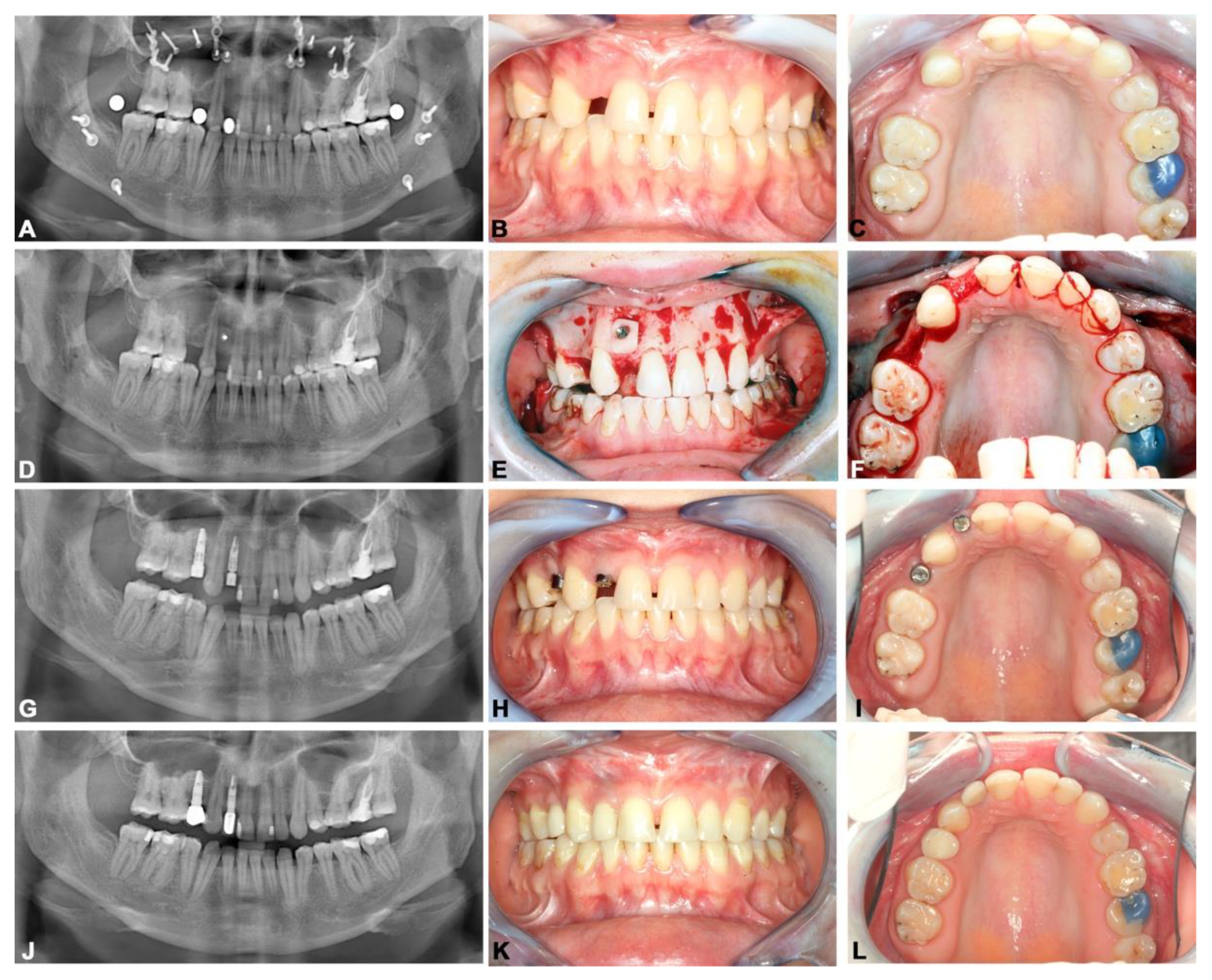
2.4. Surgical Procedures
2.5. Measured Variables
2.6. Statistical Analysis
3. Results
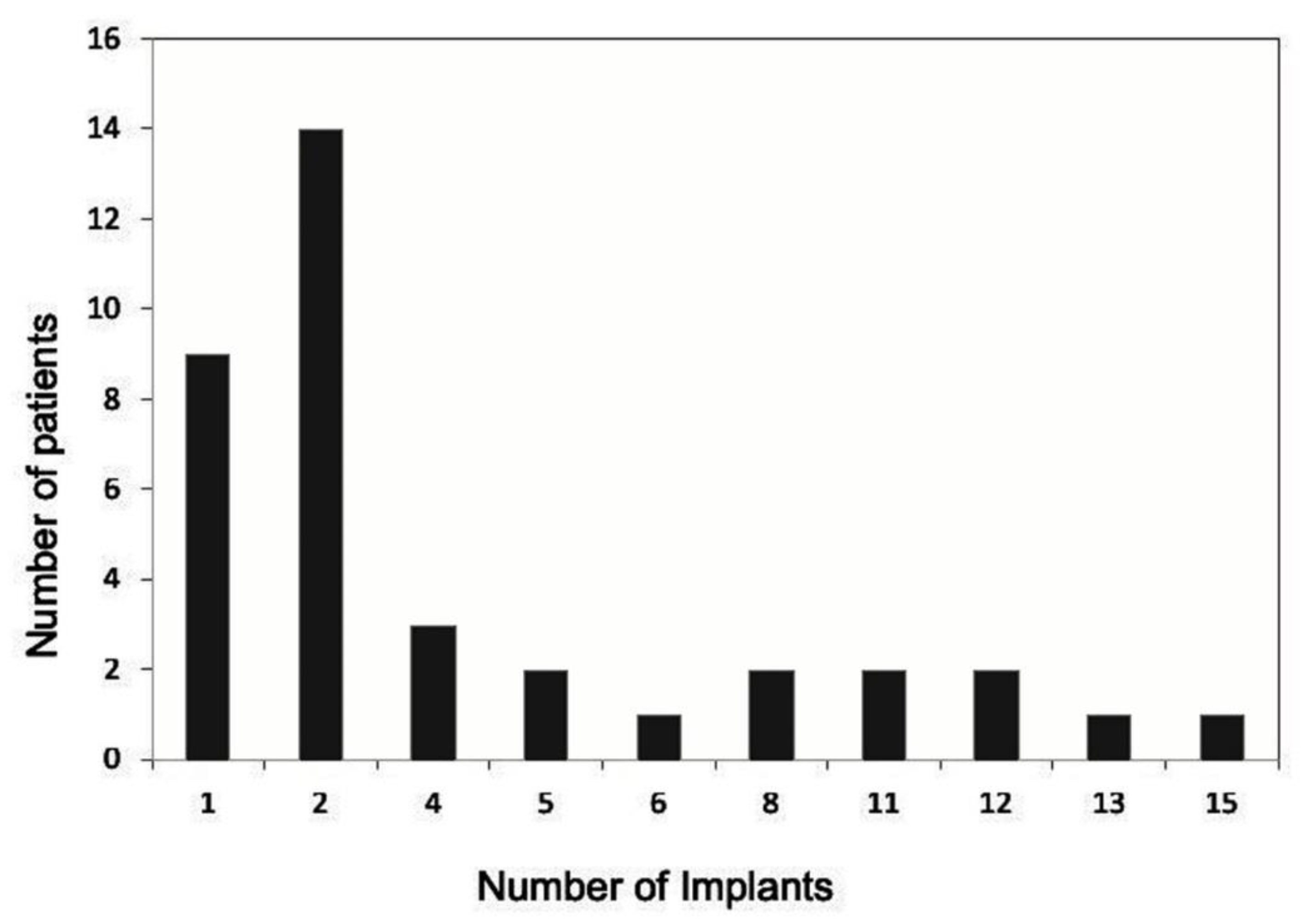
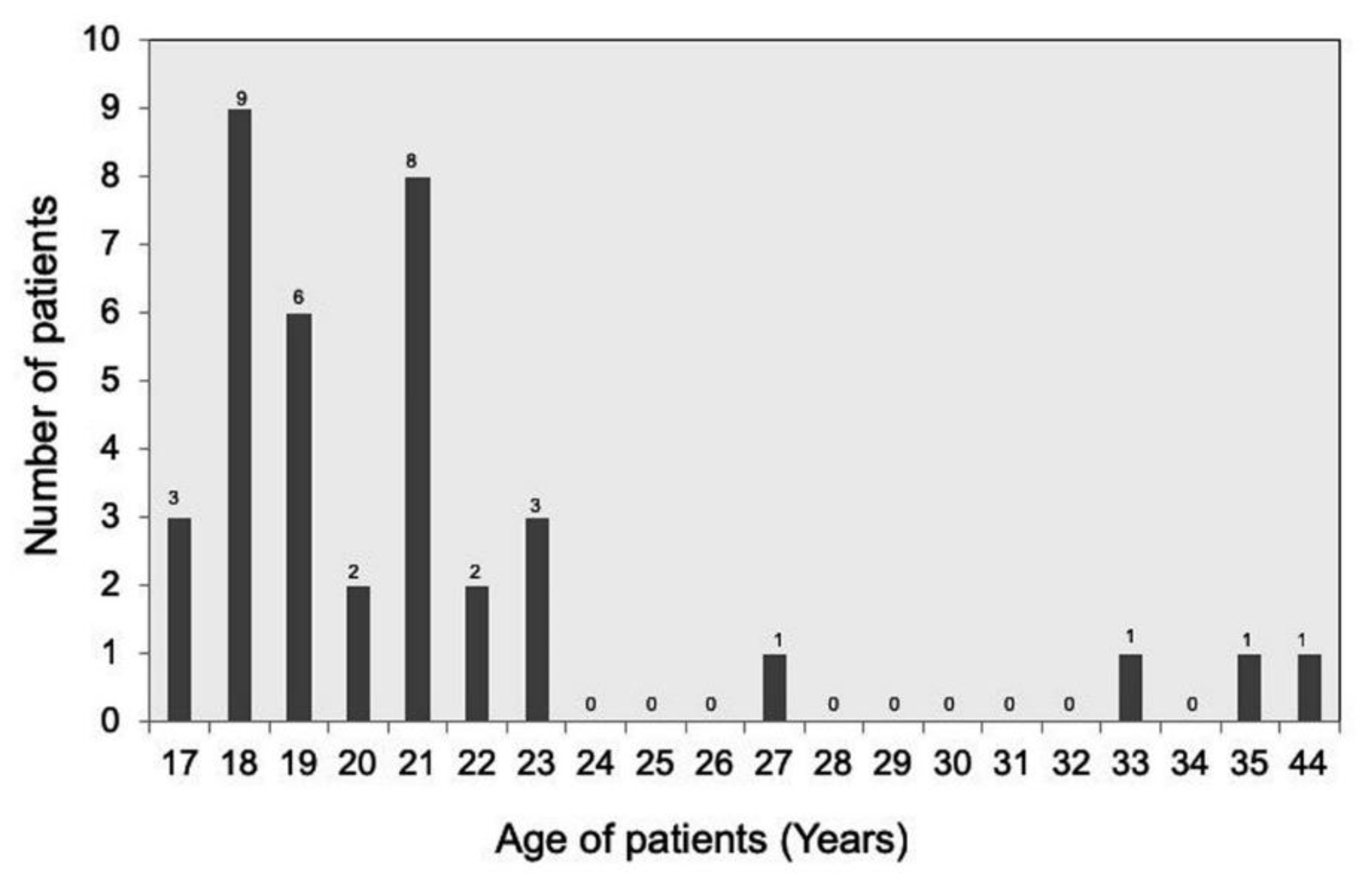
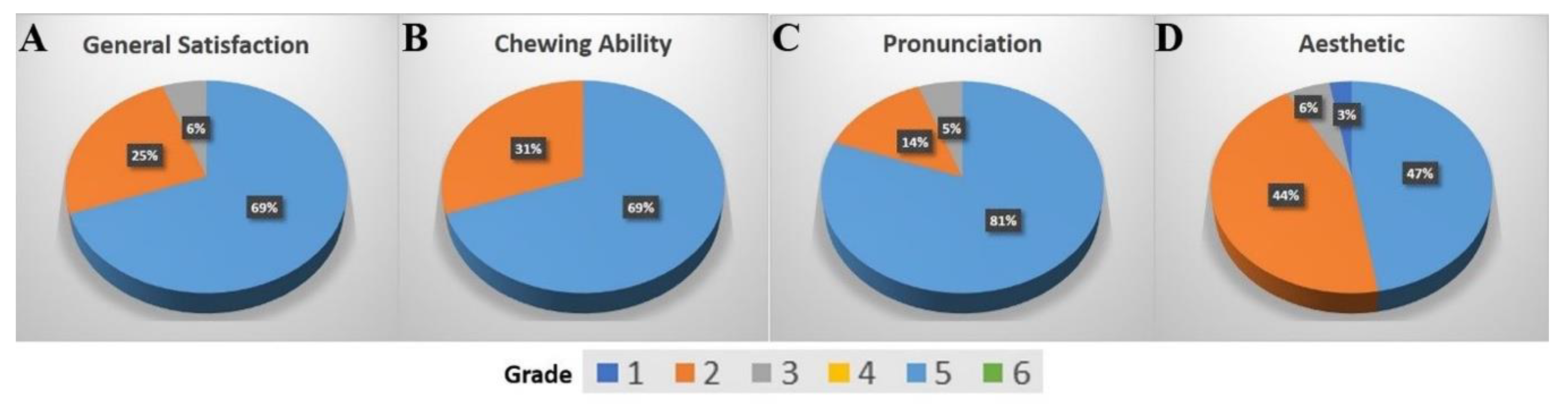
3.1. Patient-Related Parameters
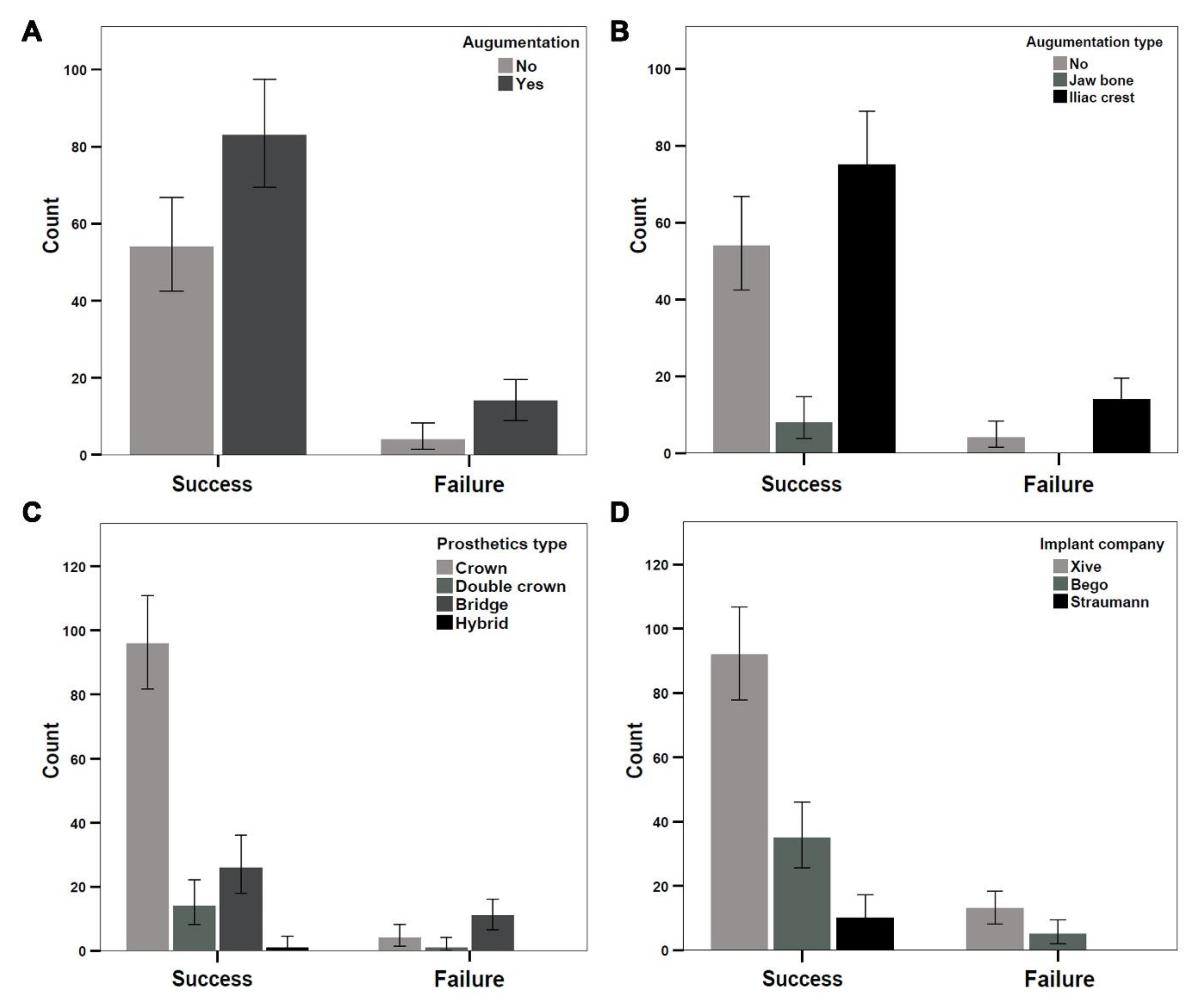
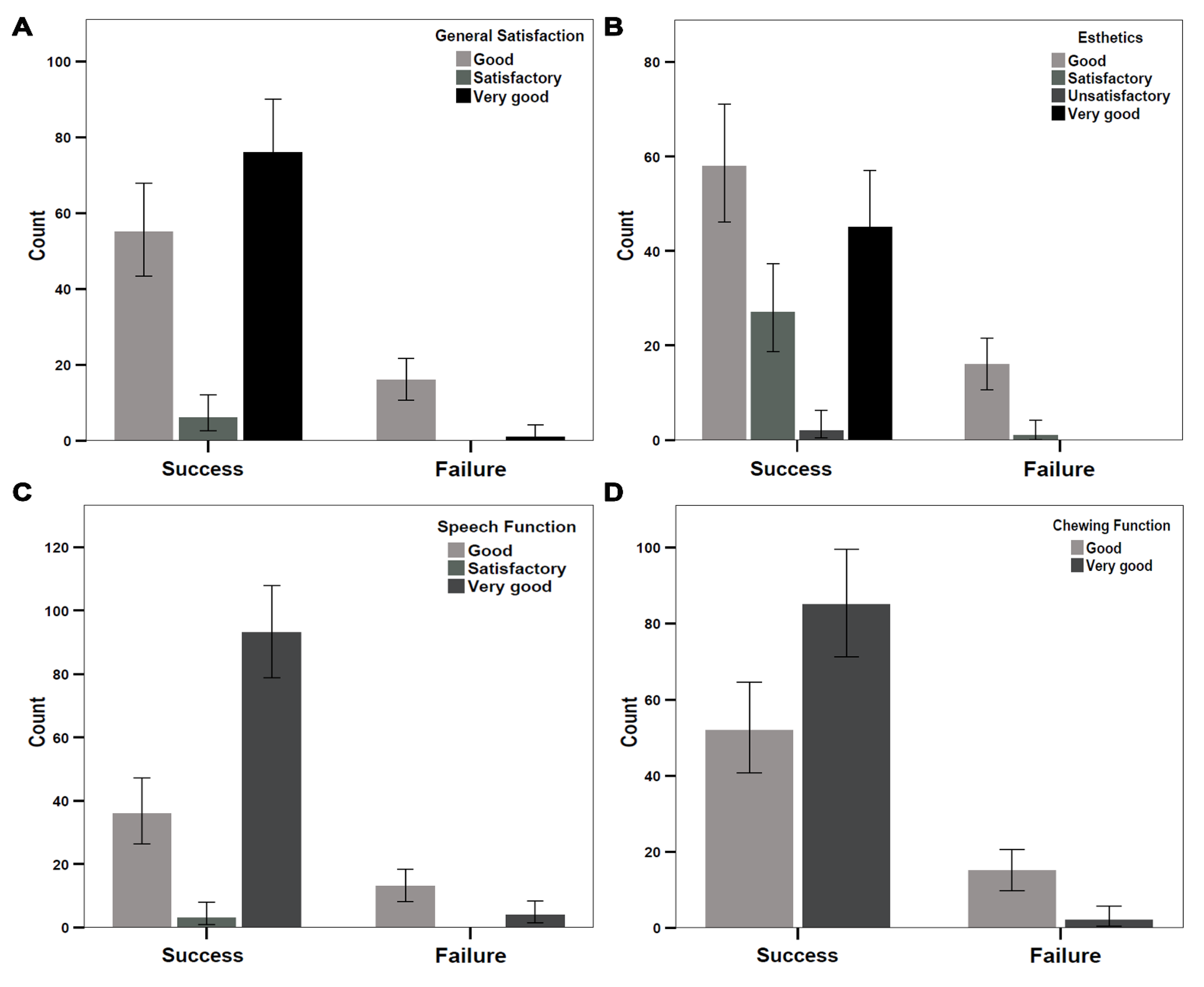
3.2. Analysis of Implant Success Using Albrektsson Criteria
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nunn, J.H.; Carter, N.E.; Gillgrass, T.J.; Hobson, R.S.; Jepson, N.J.; Meechan, J.G.; Nohl, F.S. The interdisciplinary management of hypodontia: Background and role of paediatric dentistry. Br. Dent. J. 2003, 194, 245–251. [Google Scholar] [CrossRef]
- Tan, S.P.; van Wijk, A.J.; Prahl-Andersen, B. Severe hypodontia: Identifying patterns of human tooth agenesis. Eur. J. Orthod. 2011, 33, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Vastardis, H.; Karimbux, N.; Guthua, S.W.; Seidman, J.G.; Seidman, C.E. A human MSX1 homeodomain missense mutation causes selective tooth agenesis. Nat. Genet. 1996, 13, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Créton, M.; Cune, M.; Verhoeven, W.; Muradin, M.; Wismeijer, D.; Meijer, G. Implant treatment in patients with severe hypodontia: A retrospective evaluation. J. Oral Maxillofac. Surg. 2010, 68, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Terheyden, H.; Wusthoff, F. Occlusal rehabilitation in patients with congenitally missing teeth-dental implants, conventional prosthetics, tooth autotransplants, and preservation of deciduous teeth-a systematic review. Int. J. Implant Dent. 2015, 1, 30. [Google Scholar] [CrossRef]
- Polder, B.J.; Van’t Hof, M.A.; Van der Linden, F.P.; Kuijpers-Jagtman, A.M. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent. Oral Epidemiol. 2004, 32, 217–226. [Google Scholar] [CrossRef]
- Gracco, A.L.; Zanatta, S.; Valvecchi, F.F.; Bignotti, D.; Perri, A.; Baciliero, F. Prevalence of dental agenesis in a sample of Italian orthodontic patients: An epidemiological study. Prog. Orthod. 2017, 18, 33. [Google Scholar] [CrossRef]
- Ranta, R.; Stegars, T.; Rintala, A.E. Correlations of hypodontia in children with isolated cleft palate. Cleft Palate J. 1983, 20, 163–165. [Google Scholar]
- Boehn, A. Dental Anomalies in Harelip and Cleft Palate. Acta Odontol. Scand. 1963, 21 (Suppl. S38), 31–109. [Google Scholar]
- Prager, T.M.; Finke, C.; Miethke, R.R. Dental findings in patients with ectodermal dysplasia. J. Orofac. Orthop. 2006, 67, 347–355. [Google Scholar] [CrossRef]
- Kumasaka, S.; Miyagi, A.; Sakai, N.; Shindo, J.; Kashima, I. Oligodontia: A radiographic comparison of subjects with Down syndrome and normal subjects. Spec. Care Dent. 1997, 17, 137–141. [Google Scholar] [CrossRef]
- Kolenc-Fuse, F.J. Tooth agenesis: In search of mutations behind failed dental development. Med. Oral Patol. Oral Cir. Bucal 2004, 9, 385–395. [Google Scholar] [PubMed]
- Hourfar, J.; Lux, C.J.; Ludwig, B. Kieferorthopädische Therapieoptionen von Nichtanlagen permanenter Zähne. Zahnmed. up2date 2014, 8, 167–188. [Google Scholar] [CrossRef]
- Breeze, J.; Dover, M.; Williams, R. Contemporary surgical management of hypodontia. Br. J. Oral Maxillofac. Surg. 2017, 55, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Durey, K.; Carter, L.; Chan, M. The management of severe hypodontia. Part 2: Bone augmentation and the provision of implant supported prostheses. Br. Dent. J. 2014, 216, 63. [Google Scholar] [CrossRef] [PubMed]
- Borzabadi-Farahani, A. Orthodontic considerations in restorative management of hypodontia patients with endosseous implants. J. Oral Implantol. 2012, 38, 779–791. [Google Scholar] [CrossRef]
- Filius, M.; Cune, M.; Raghoebar, G.; Vissink, A.; Visser, A. Prosthetic treatment outcome in patients with severe hypodontia: A systematic review. J. Oral Rehabil. 2016, 43, 373–387. [Google Scholar] [CrossRef]
- Burns, B.; Grieg, V.; Bissell, V.; Savarrio, L. A review of implant provision for hypodontia patients within a Scottish referral centre. Br. Dent. J. 2017, 223, 96. [Google Scholar] [CrossRef]
- Fischer-Brandies, H.; Junker, N. Theory and practice of functional orthodontic treatment in infants and young children with Down’s disease. L’Orthodontie Francaise 1985, 56, 365–369. [Google Scholar]
- Hobkirk, J.; Goodman, J.; Reynolds, I. Component failure in removable partial dentures for patients with severe hypodontia. Int. J. Prosthodont. 1989, 2, 2. [Google Scholar]
- Attia, S.; Wiltfang, J.; Pons-Kuhnemann, J.; Wilbrand, J.F.; Streckbein, P.; Kahling, C.; Howaldt, H.P.; Schaaf, H. Survival of dental implants placed in vascularised fibula free flaps after jaw reconstruction. J. Craniomaxillofac. Surg. 2018, 46, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Attia, S.; Wiltfang, J.; Streckbein, P.; Wilbrand, J.F.; El Khassawna, T.; Mausbach, K.; Howaldt, H.P.; Schaaf, H. Functional and aesthetic treatment outcomes after immediate jaw reconstruction using a fibula flap and dental implants. J. Craniomaxillofac. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Filius, M.A.; Vissink, A.; Cune, M.S.; Raghoebar, G.M.; Visser, A. Long-term implant performance and patients’ satisfaction in oligodontia. J. Dent. 2018, 71, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Bertl, K. A wide mesio-distal gap distance in sites of congenitally missing maxillary lateral incisors is related to a thin bucco-palatal alveolar ridge width. Clin. Oral Implants Res. 2016, 28, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Kokich, V.G.; Kokich, V.O. Congenitally missing mandibular second premolars: Clinical options. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 437–444. [Google Scholar] [CrossRef]
- Fretwurst, T.; Nack, C.; Al-Ghrairi, M.; Raguse, J.; Stricker, A.; Schmelzeisen, R.; Nelson, K.; Nahles, S. Long-term retrospective evaluation of the peri-implant bone level in onlay grafted patients with iliac bone from the anterior superior iliac crest. J. Cranio-Maxillofac. Surg. 2015, 43, 956–960. [Google Scholar] [CrossRef]
- Capelli, M. Autogenous bone graft from the mandibular ramus: A technique for bone augmentation. Int. J. Periodontics Restor. Dent. 2003, 23, 277–286. [Google Scholar]
- Streckbein, P.; Kähling, C.; Wilbrand, J.-F.; Malik, C.-Y.; Schaaf, H.; Howaldt, H.-P.; Streckbein, R. Horizontal alveolar ridge augmentation using autologous press fit bone cylinders and micro-lag-screw fixation: Technical note and initial experience. J. Cranio-Maxillofac. Surg. 2014, 42, 387–391. [Google Scholar] [CrossRef]
- Kumar, P.; Vinitha, B.; Fathima, G. Bone grafts in dentistry. J. Pharm. Bioallied Sci. 2013, 5, S125. [Google Scholar] [CrossRef]
- Attia, S.; Schaper, E.; Schaaf, H.; Pons-Kühnemann, J.; Schlenz, M.A.; Streckbein, P.; Böttger, S.; Howaldt, H.-P.; Wilbrand, J.-F. Evaluation of Implant Success in Patients with Dental Aplasia. BioMed. Res. Int. 2019, 2019, 1680158. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar] [PubMed]
- Chaar, M.S.; Passia, N.; Kern, M. All-ceramic inlay-retained fixed dental prostheses: An update. Quintessence Int. 2015, 46, 46. [Google Scholar]
- Gupta, R.; Weber, K.K. Dental Implants. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Borzabadi-Farahani, A.; Zadeh, H.H. Adjunctive orthodontic applications in dental implantology. J. Oral Implantol. 2015, 41, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Borzabadi-Farahani, A.; Zadeh, H.H. Orthodontic therapy in implant dentistry: Orthodontic implant site development. In Vertical Alveolar Ridge Augmentation in Implant Dentistry: A Surgical Manual; Tolstunov, L., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 2016; pp. 30–37. [Google Scholar]
- Alarifi, A.; AlZubi, A.A. Memetic Search Optimization Along with Genetic Scale Recurrent Neural Network for Predictive Rate of Implant Treatment. J. Med. Syst. 2018, 42, 202. [Google Scholar] [CrossRef]
- Misch, C. Vertical Alveolar Ridge Augmentation in Implant Dentistry: A Surgical Manual; Wiley-Blackwell: Hoboken, NJ, USA, 2017. [Google Scholar]
- Zachrisson, B. Orthodontic tooth movement to regenerate new alveolar tissue and bone for improved single implant aesthetics. Eur. J. Orthod. 2003, 25, 442. [Google Scholar]
- Kokich, V.G. Maxillary lateral incisor implants: Planning with the aid of orthodontics. J. Oral Maxillofac. Surg. 2004, 62, 48–56. [Google Scholar] [CrossRef]
- Lindskog-Stokland, B.; Hansen, K.; Ekestubbe, A.; Wennström, J.L. Orthodontic tooth movement into edentulous ridge areas—A case series. Eur. J. Orthod. 2011, 35, 277–285. [Google Scholar] [CrossRef]
- Vahid-Dastjerdi, E.; Borzabadi-Farahani, A.; Mahdian, M.; Amini, N. Non-syndromic hypodontia in an Iranian orthodontic population. J. Oral Sci. 2010, 52, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Carmichael, R.P.; Sándor, G.K. Dental implants in the management of nonsyndromal oligodontia. Atlas Oral Maxillofac. Surg. Clin. 2008, 16, 11–31. [Google Scholar] [CrossRef]
- Buch, R.S.; Weibrich, G.; Wagner, W. Criteria of success in implantology. Mund. Kiefer Gesichtschir. 2003, 7, 42–46. [Google Scholar] [CrossRef]
- Finnema, K.J.; Raghoebar, G.M.; Meijer, H.J.; Vissink, A. Oral rehabilitation with dental implants in oligodontia patients. Int. J. Prosthodont. 2005, 18, 203–209. [Google Scholar]
- Zou, D.; Wu, Y.; Wang, X.D.; Huang, W.; Zhang, Z.; Zhang, Z. A retrospective 3- to 5-year study of the reconstruction of oral function using implant-supported prostheses in patients with hypohidrotic ectodermal dysplasia. J. Oral. Implantol. 2014, 40, 571–580. [Google Scholar] [CrossRef]
- Iizuka, T.; Hafliger, J.; Seto, I.; Rahal, A.; Mericske-Stern, R.; Smolka, K. Oral rehabilitation after mandibular reconstruction using an osteocutaneous fibula free flap with endosseous implants. Factors affecting the functional outcome in patients with oral cancer. Clin. Oral Implants Res. 2005, 16, 69–79. [Google Scholar] [CrossRef]
- Fu, L.; Khor, K.A.; Lim, J.P. Yttria stabilized zirconia reinforced hydroxyapatite coatings. Surf. Coat. Technol. 2000, 127, 66–75. [Google Scholar] [CrossRef]
- Peng, X.; Mao, C.; Yu, G.-Y.; Guo, C.-B.; Huang, M.-X.; Zhang, Y. Maxillary reconstruction with the free fibula flap. Plast. Reconstr. Surg. 2005, 115, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Takushima, A.; Harii, K.; Asato, H.; Nakatsuka, T.; Kimata, Y. Mandibular reconstruction using microvascular free flaps: A statistical analysis of 178 cases. Plast. Reconstr. Surg. 2001, 108, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Draenert, F.G.; Huetzen, D.; Neff, A.; Mueller, W.E. Vertical bone augmentation procedures: Basics and techniques in dental implantology. J. Biomed. Mater. Res. A 2014, 102, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Keestra, J.A.; Barry, O.; Jong, L.; Wahl, G. Long-term effects of vertical bone augmentation: A systematic review. J. Appl. Oral Sci. 2016, 24, 3–17. [Google Scholar] [CrossRef]
- Åstrand, P.; Nord, P.G.; Brånemark, P.-I. Titanium implants and onlay bone graft to the atrophic edentulous maxilla: A 3-year longitudinal study. Int. J. Oral Maxillofac. Surg. 1996, 25, 25–29. [Google Scholar] [CrossRef]
- Carinci, F.; Farina, A.; Zanetti, U.; Vinci, R.; Negrini, S.; Calura, G.; Laino, G.; Piattelli, A. Alveolar ridge augmentation: A comparative longitudinal study between calvaria and iliac crest bone grafrs. J. Oral Implantol. 2005, 31, 39–45. [Google Scholar] [CrossRef]
- Silness, J.; Gustavsen, F.; Mangersnes, K. The relationship between pontic hygiene and mucosal inflammation in fixed bridge recipients. J. Periodont. Res. 1982, 17, 434–439. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | Number of Implants | |
|---|---|---|
| Total number of patients | 43 | 165 |
| Men | 18 | 97 |
| Women | 25 | 68 |
| Drop-outs | 6 | 10 |
| Investigated patients | 37 * | 155 |
| Removed implants | 2 | 2 |
| Implant failure (Albrektsson) | 7 | 18 |
| General Disorders, Allergies, and Smoking Behavior | No. Patients |
|---|---|
| Cleft lip/palate | 2 |
| Diabetes Type 2 | 2 |
| Bronchial asthma | 1 |
| Blood clotting disorder | 1 |
| Ectodermal dysplasia | 2 |
| Hypothyroidism | 3 |
| Allergy: penicillin | 1 |
| Smoking | 10 |
| No. of Patients (%) | Aesthetics | Orthodontic Treatment Prior to Implant Placement? | |
|---|---|---|---|
| No | Yes | ||
| 17 (47.22%) | Very good | 2 (5.55%) | 15 (41.66%) |
| 16 (44.44%) | Good | 2 (5.55%) | 14 (38.88%) |
| 2 (5.55%) | Satisfactory | 1 (2.77%) | 1 (2.77%) |
| 1 (2.77%) | Unsatisfactory | 0 | 1 (2.77%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attia, S.; Schaaf, H.; El Khassawna, T.; Malhan, D.; Mausbach, K.; Howaldt, H.-P.; Streckbein, P. Oral Rehabilitation of Hypodontia Patients Using an Endosseous Dental Implant: Functional and Aesthetic Results. J. Clin. Med. 2019, 8, 1687. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101687
Attia S, Schaaf H, El Khassawna T, Malhan D, Mausbach K, Howaldt H-P, Streckbein P. Oral Rehabilitation of Hypodontia Patients Using an Endosseous Dental Implant: Functional and Aesthetic Results. Journal of Clinical Medicine. 2019; 8(10):1687. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101687
Chicago/Turabian StyleAttia, Sameh, Heidrun Schaaf, Thaqif El Khassawna, Deeksha Malhan, Katharina Mausbach, Hans-Peter Howaldt, and Philipp Streckbein. 2019. "Oral Rehabilitation of Hypodontia Patients Using an Endosseous Dental Implant: Functional and Aesthetic Results" Journal of Clinical Medicine 8, no. 10: 1687. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101687