Laxer Clinical Criteria for Gaming Disorder May Hinder Future Efforts to Devise an Efficient Diagnostic Approach: A Tree-Based Model Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
The Current Study
2. Method
2.1. Participants and Procedures
2.2. Measures
2.2.1. Sociodemographics and Gaming-Related Behaviors
2.2.2. Internet Gaming Disorder Scale–Short-Form (IGDS9-SF)
2.3. Analytic Strategy and Data Management
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics
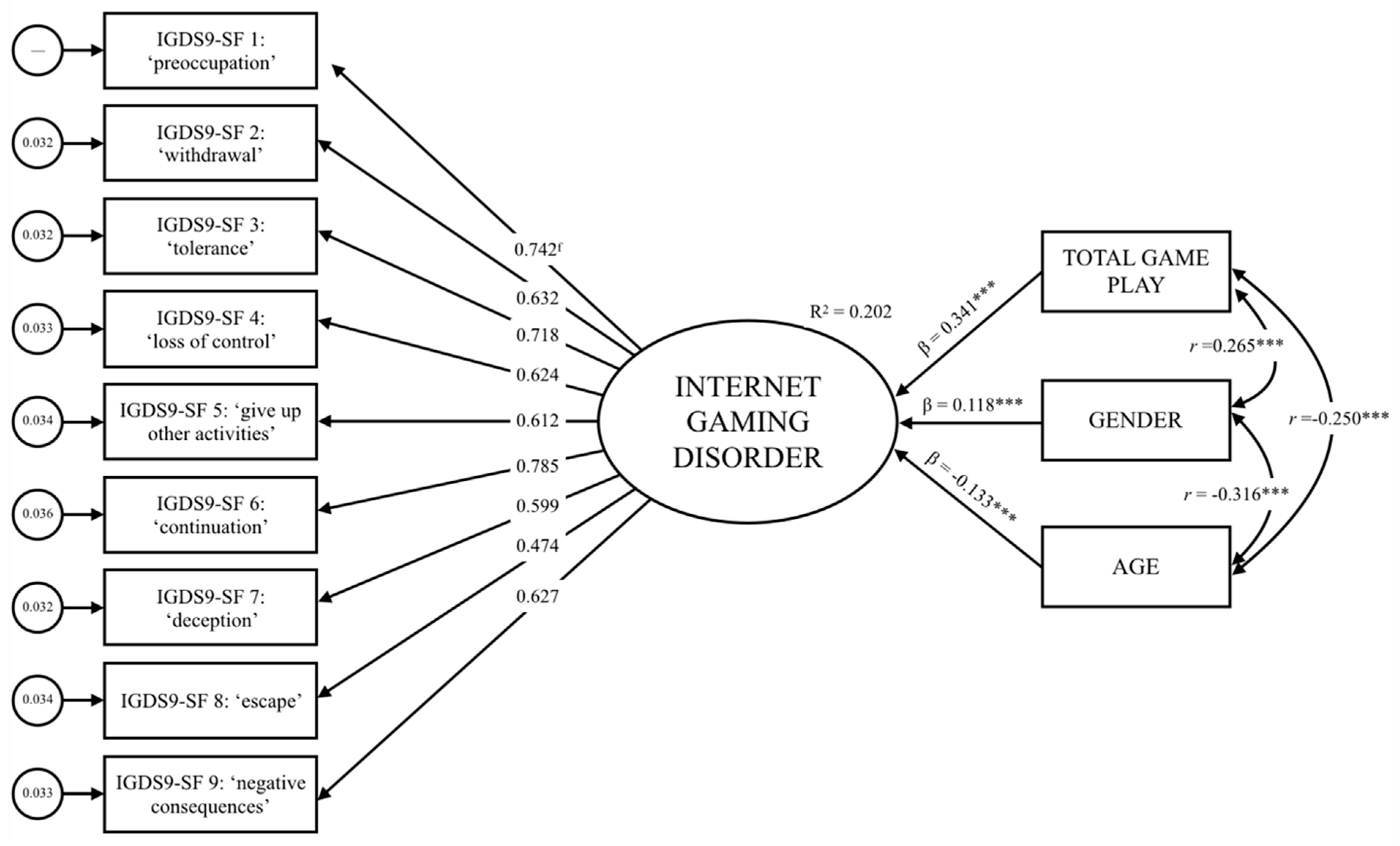
3.2. Construct Unidimensionality and Criterion-Related Validity
3.3. Reliability Analysis
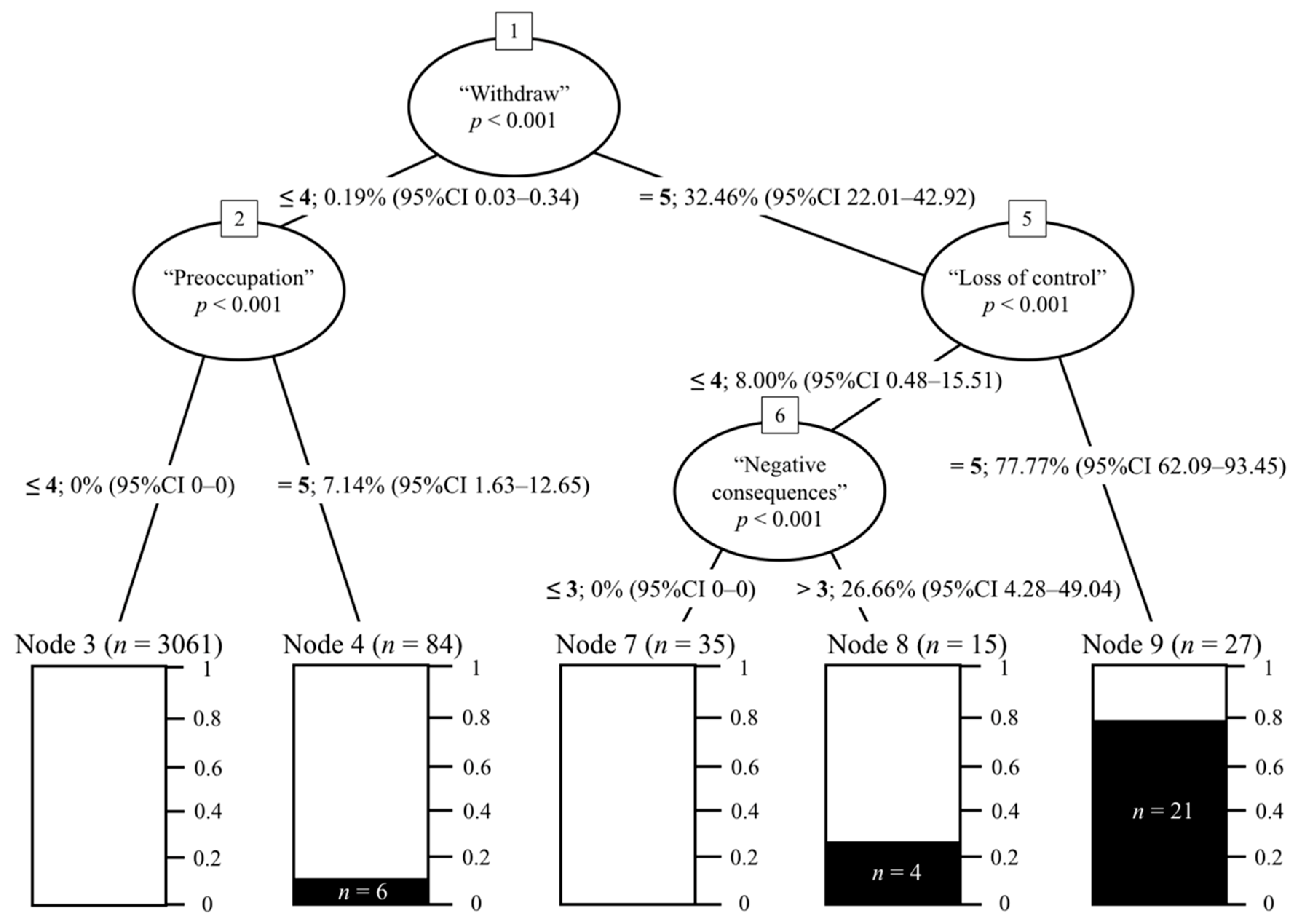
3.4. Conditional Inference Tree Analysis
4. Discussion
5. Conclusions: Implications for Future Research and Diagnostic Practices
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- West, R. Theories of addiction. Addiction 2001, 96, 3–13. [Google Scholar] [CrossRef] [Green Version]
- American Society of Addiction Medicine. Definition of Addiction. Available online: https://www.asam.org/resources/definition-of-addiction (accessed on 20 September 2019).
- Griffiths, M.D. A ‘components’ model of addiction within a biopsychosocial framework. J. Subst. Use 2005, 10, 191–197. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- World Health Organization. ICD-11 Beta Draft: Gaming Disorder. Available online: http://apps.who.int/classifications/icd11/browse/f/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1448597234 (accessed on 21 September 2019).
- Maraz, A.; Király, O.; Demetrovics, Z. Commentary on: Are we overpathologizing everyday life? A tenable blueprint for behavioral addiction research The diagnostic pitfalls of surveys: If you score positive on a test of addiction, you still have a good chance not to be addicted. J. Behav. Addict. 2015, 4, 151–154. [Google Scholar] [CrossRef]
- Rumpf, H.J.; Achab, S.; Billieux, J.; Bowden-Jones, H.; Carragher, N.; Demetrovics, Z.; Higuchi, S.; King, D.L.; Mann, K.; Potenza, M.; et al. Including gaming disorder in the ICD-11: The need to do so from a clinical and public health perspective. J. Behav. Addict. 2018, 7, 556–561. [Google Scholar] [CrossRef]
- Aarseth, E.; Bean, A.M.; Boonen, H.; Colder, C.M.; Coulson, M.; Das, D.; Deleuze, J.; Dunkels, E.; Edman, J.; Ferguson, C.J.; et al. Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. J. Behav. Addict. 2016, 6, 267–270. [Google Scholar] [CrossRef]
- Király, O.; Demetrovics, Z. Inclusion of Gaming Disorder in ICD has more advantages than disadvantages. J. Behav. Addict. 2017, 6, 280–284. [Google Scholar] [CrossRef] [Green Version]
- Kuss, D.J.; Griffiths, M.D.; Pontes, H.M. Chaos and confusion in DSM-5 diagnosis of Internet Gaming Disorder: Issues, concerns, and recommendations for clarity in the field. J. Behav. Addict. 2017, 6, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Van Rooij, A.J.; Kardefelt-Winther, D. Lost in the chaos: Flawed literature should not generate new disorders. J. Behav. Addict. 2017, 6, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Quandt, T. Stepping back to advance: Why IGD needs an intensified debate instead of a consensus. J. Behav. Addict. 2017, 6, 121–123. [Google Scholar] [CrossRef] [Green Version]
- Pontes, H.M. Making the case for video game addiction: Does it exist or not? In Video Game Influences on Aggression, Cognition, and Attention; Ferguson, C.J., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 41–57. [Google Scholar]
- Zhang, J.T.; Brand, M. Editorial: Neural mechanisms underlying internet gaming disorder. Front. Psychiatry 2018, 9, 404. [Google Scholar] [CrossRef]
- Kuss, D.J.; Pontes, H.M.; Griffiths, M.D. Neurobiological correlates in Internet Gaming Disorder: A systematic literature review. Front. Psychiatry 2018, 9, 166. [Google Scholar] [CrossRef]
- Pontes, H.M.; Kuss, D.J.; Griffiths, M.D. Clinical psychology of Internet addiction: A review of its conceptualization, prevalence, neuronal processes, and implications for treatment. Neurosci. Neuroecon. 2015, 4, 11–23. [Google Scholar] [CrossRef]
- Pontes, H.M.; Kuss, D.J.; Griffiths, M.D. Psychometric assessment of Internet Gaming Disorder in neuroimaging studies: A systematic review. In Internet Addiction: Neuroscientific Approaches and Therapeutical Implications Including Smartphone Addiction; Montag, C., Reuter, M., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 181–208. [Google Scholar]
- Park, S.; Jeon, H.J.; Son, J.W.; Kim, H.; Hong, J.P. Correlates, comorbidities, and suicidal tendencies of problematic game use in a national wide sample of Korean adults. Int. J. Ment. Health Syst. 2017, 11, 35. [Google Scholar] [CrossRef]
- Na, E.; Lee, H.; Choi, I.; Kim, D.J. Comorbidity of Internet Gaming Disorder and alcohol use disorder: A focus on clinical characteristics and gaming patterns. Am. J. Addict. 2017, 26, 326–334. [Google Scholar] [CrossRef]
- Wang, H.R.; Cho, H.; Kim, D.J. Prevalence and correlates of comorbid depression in a nonclinical online sample with DSM-5 Internet Gaming Disorder. J. Affect. Disord. 2018, 228, 1–5. [Google Scholar] [CrossRef]
- Pontes, H.M.; Griffiths, M.D. Portuguese validation of the Internet Gaming Disorder Scale–Short-form. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 288–293. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Adams, B.L.M.; Beard, C.L.; Dumble, E.; Trawley, S.; Gomez, R.; Pontes, H.M. Associations between attention deficit hyperactivity and internet gaming disorder symptoms: Is there consistency across types of symptoms, gender and countries? Addict. Behav. Rep. 2019, 9, 100158. [Google Scholar] [CrossRef]
- Sariyska, R.; Reuter, M.; Lachmann, B.; Montag, C. Attention deficit/hyperactivity disorder is a better predictor for problematic Internet use than depression: Evidence from Germany. J. Addict. Res. Ther. 2015, 6, 1–6. [Google Scholar] [CrossRef]
- Pearcy, B.T.D.; McEvoy, P.M.; Roberts, L.D. Internet Gaming Disorder explains unique variance in psychological distress and disability after controlling for comorbid depression, OCD, ADHD, and anxiety. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 126–132. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Gentile, D.A.; Motti-Stefanidi, F. A multilevel longitudinal study of adolescent Internet addiction: The role of obsessive—Compulsive symptoms and classroom openness to experience. Eur. J. Dev. Psychol. 2016, 13, 99–114. [Google Scholar] [CrossRef]
- Wang, C.Y.; Wu, Y.C.; Su, C.H.; Lin, P.C.; Ko, C.H.; Yen, J.Y. Association between Internet gaming disorder and generalized anxiety disorder. J. Behav. Addict. 2017, 6, 564–571. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Gomez, R.; Steen, E.; Beard, C.; Liew, L.; Griffiths, M.D. The longitudinal association between anxiety and Internet addiction in adolescence: The moderating effect of classroom extraversion. J. Behav. Addict. 2017, 6, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Wartberg, L.; Kriston, L.; Zieglmeier, M.; Lincoln, T.; Kammerl, R. A longitudinal study on psychosocial causes and consequences of Internet gaming disorder in adolescence. Psychol. Med. 2018, 49, 287–294. [Google Scholar] [CrossRef]
- Lim, J.A.; Lee, J.Y.; Jung, H.Y.; Sohn, B.K.; Choi, S.W.; Kim, Y.J.; Kim, D.J.; Choi, J.S. Changes of quality of life and cognitive function in individuals with Internet Gaming Disorder: A 6-month follow-up. Medicine 2016, 95, e5695. [Google Scholar] [CrossRef]
- Henchoz, Y.; Studer, J.; Deline, S.; N’Goran, A.A.; Baggio, S.; Gmel, G. Video gaming disorder and sport and exercise in emerging adulthood: A longitudinal study. Behav. Med. 2016, 42, 105–111. [Google Scholar] [CrossRef]
- Schmitt, Z.L.; Livingston, M.G. Video game addiction and college performance among males: Results from a 1 year longitudinal study. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 25–29. [Google Scholar] [CrossRef]
- Pontes, H.M.; Griffiths, M.D.; Patrão, I.M. Internet addiction and loneliness among children and adolescents in the education setting: An empirical pilot study. Aloma 2014, 32, 91–98. [Google Scholar]
- Gentile, D.A.; Choo, H.; Liau, A.; Sim, T.; Li, D.; Fung, D.; Khoo, A. Pathological video game use among youths: A two-year longitudinal study. Pediatrics 2011, 127, e319–e329. [Google Scholar] [CrossRef]
- Männikkö, N.; Ruotsalainen, H.; Jouko Miettunen, J.; Pontes, H.M.; Kääriäinen, M. Problematic gaming behaviour and health-related outcomes: A systematic review and meta-analysis. J. Health Psychol. 2018. [Google Scholar] [CrossRef]
- Brunborg, G.S.; Hanss, D.; Mentzoni, R.A.; Pallesen, S. Core and peripheral criteria of video game addiction in the game addiction scale for adolescents. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 280–285. [Google Scholar] [CrossRef]
- Ustinavičienė, R.; Škėmienė, L.; Lukšienė, D.; Radišauskas, R.; Kalinienė, G.; Vasilavičius, P. Problematic computer game use as expression of Internet addiction and its association with self-rated health in the Lithuanian adolescent population. Medicina 2016, 52, 199–204. [Google Scholar] [CrossRef]
- Wu, A.M.S.; Chen, J.H.; Tong, K.K.; Yu, S.; Lau, J.T.F. Prevalence and associated factors of Internet gaming disorder among community dwelling adults in Macao, China. J. Behav. Addict. 2018, 7, 62–69. [Google Scholar] [CrossRef]
- Myrseth, H.; Notelaers, G. A latent class approach for classifying the problem and disordered gamers in a group of adolescence. Front. Psychol. 2018, 9, 2273. [Google Scholar] [CrossRef]
- Griffiths, M.D.; Van Rooij, A.J.; Kardefelt-Winther, D.; Starcevic, V.; Király, O.; Pallesen, S.; Müller, K.; Dreier, M.; Carras, M.; Prause, N.; et al. Working towards an international consensus on criteria for assessing Internet Gaming Disorder: A critical commentary on Petry et al. (2014). Addiction 2016, 111, 167–175. [Google Scholar] [CrossRef]
- Petry, N.M.; Rehbein, F.; Gentile, D.A.; Lemmens, J.S.; Rumpf, H.J.; Mößle, T.; Bischof, G.; Tao, R.; Fung, D.S.S.; Borges, G.; et al. An international consensus for assessing Internet Gaming Disorder using the new DSM-5 approach. Addiction 2014, 109, 1399–1406. [Google Scholar] [CrossRef]
- Starcevic, V. Tolerance and withdrawal symptoms may not be helpful to enhance understanding of behavioural addictions. Addiction 2016, 111, 1307–1308. [Google Scholar] [CrossRef] [Green Version]
- King, D.L.; Delfabbro, P.H. Defining tolerance in Internet Gaming Disorder: Isn’t it time? Addiction 2016, 111, 2064–2065. [Google Scholar] [CrossRef]
- King, D.L.; Herd, M.C.E.; Delfabbro, P.H. Tolerance in Internet gaming disorder: A need for increasing gaming time or something else? J. Behav. Addict. 2017, 6, 525–533. [Google Scholar] [CrossRef]
- Rehbein, F.; Kliem, S.; Baier, D.; Mößle, T.; Petry, N.M. Prevalence of Internet Gaming Disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction 2015, 110, 842–851. [Google Scholar] [CrossRef]
- Lemmens, J.S.; Valkenburg, P.M.; Gentile, D.A. The Internet Gaming Disorder Scale. Psychol. Assess. 2015, 27, 567–582. [Google Scholar] [CrossRef]
- Ko, C.H.; Yen, J.Y.; Chen, S.H.; Wang, P.W.; Chen, C.S.; Yen, C.F. Evaluation of the diagnostic criteria of Internet Gaming Disorder in the DSM-5 among young adults in Taiwan. J. Psychiatr. Res. 2014, 53, 103–110. [Google Scholar] [CrossRef]
- Gomez, R.; Stavropoulos, V.; Beard, C.; Pontes, H.M. Item Response Theory analysis of the recoded Internet Gaming Disorder Scale-Short-Form (IGDS9-SF). Int. J. Ment. Health Addict. 2019, 17, 859–879. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Gomez, R.; Beard, C.; Pontes, H.M. Item Response Theory Analysis of the Recoded Internet Gaming Disorder Scale 9–Short-Form. In Proceedings of the 5th International Conference on Behavioral Addictions, Cologne, Germany, 23–25 April 2018; pp. 146–147. [Google Scholar] [CrossRef]
- Schivinski, B.; Brzozowska-Woś, M.; Buchanan, E.M.; Griffiths, M.D.; Pontes, H.M. Psychometric assessment of the Internet Gaming Disorder diagnostic criteria: An Item Response Theory study. Addict. Behav. Rep. 2018, 8, 176–184. [Google Scholar] [CrossRef]
- Király, O.; Sleczka, P.; Pontes, H.M.; Urbán, R.; Griffiths, M.D.; Demetrovics, Z. Validation of the ten-item Internet Gaming Disorder Test (IGDT-10) and evaluation of the nine DSM-5 Internet Gaming Disorder criteria. Addict. Behav. 2017, 64, 253–260. [Google Scholar] [CrossRef]
- Pontes, H.M.; Griffiths, M.D. Measuring DSM-5 Internet Gaming Disorder: Development and validation of a short psychometric scale. Comput. Hum. Behav. 2015, 45, 137–143. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Beard, C.; Griffiths, M.D.; Buleigh, T.; Gomez, R.; Pontes, H.M. Measurement invariance of the Internet Gaming Disorder Scale–Short-Form (IGDS9-SF) between Australia, the USA, and the UK. Int. J. Ment. Health Addict. 2018, 16, 377–392. [Google Scholar] [CrossRef]
- de Palo, V.; Monacis, L.; Sinatra, M.; Griffiths, M.D.; Pontes, H.M.; Petro, M.; Miceli, S. Measurement invariance of the nine-item Internet Gaming Disorder Scale (IGDS9-SF) Across Albania, USA, UK, and Italy. Int. J. Ment. Health Addict. 2018. [Google Scholar] [CrossRef]
- Pontes, H.M.; Stavropoulos, V.; Griffiths, M.D. Measurement Invariance of the Internet Gaming Disorder Scale–Short-Form (IGDS9-SF) between the United States of America, India and the United Kingdom. Psychiatry Res. 2017, 257, 472–478. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guildford Press: New York, NY, USA, 2011. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications Ltd.: London, UK, 2013. [Google Scholar]
- Fuster, H.; Carbonell, X.; Pontes, H.M.; Griffiths, M.D. Spanish validation of the Internet Gaming Disorder-20 (IGD-20) Test. Comput. Hum. Behav. 2016, 56, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Lemmens, J.S.; Valkenburg, P.M.; Peter, J. Development and validation of a game addiction scale for adolescents. Media Psychol. 2009, 12, 77–95. [Google Scholar] [CrossRef]
- Pápay, O.; Urbán, R.; Griffiths, M.D.; Nagygyörgy, K.; Farkas, J.; Kökönyei, G.; Felvinczi, K.; Oláh, A.; Elekes, Z.; Demetrovics, Z. Psychometric properties of the problematic online gaming questionnaire short-form and prevalence of problematic online gaming in a national sample of adolescents. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 340–348. [Google Scholar] [CrossRef]
- Pontes, H.M. Investigating the differential effects of social networking site addiction and Internet gaming disorder on psychological health. J. Behav. Addict. 2017, 6, 601–610. [Google Scholar] [CrossRef]
- Berkovits, I.; Hancock, G.R.; Nevitt, J. Bootstrap resampling approaches for repeated measure designs: Relative robustness to sphericity and normality violations. Educ. Psychol. Meas. 2000, 60, 877–892. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Bentler, P.M.; Bonnet, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis. A Global Perspective, 7th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hothorn, T.; Hornik, K.; Zeileis, A. Unbiased recursive partitioning: A conditional inference framework. J. Computat. Graph. Stat. 2006, 15, 651–674. [Google Scholar] [CrossRef]
- Schivinski, B. Eliciting brand-related social media engagement: A conditional inference tree framework. J. Business Res. 2019. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/abs/pii/S0148296319305156?via%3Dihub (accessed on 18 October 2019). [CrossRef]
- Rho, M.J.; Jeong, J.E.; Chun, J.W.; Cho, H.; Jung, D.J.; Choi, I.Y.; Kim, D.J. Predictors and patterns of problematic Internet game use using a decision tree model. J. Behav. Addict. 2016, 5, 500–509. [Google Scholar] [CrossRef] [Green Version]
- Pontes, H.M.; Király, O.; Demetrovics, Z.; Griffiths, M.D. The conceptualisation and measurement of DSM-5 Internet Gaming Disorder: The development of the IGD-20 Test. PLoS ONE 2014, 9, e110137. [Google Scholar] [CrossRef]
- Dufour, M.; Brunelle, N.; Khazaal, Y.; Tremblay, J.; Leclerc, D.; Cousineau, M.M.; Rousseau, M.; Légaré, A.-A.; Berbiche, D. Gender difference in online activities that determine problematic internet use. J. Thér. Comport. Cognit. 2017, 27, 90–98. [Google Scholar] [CrossRef]
- Wu, T.Y.; Lin, C.Y.; Årestedt, K.; Griffiths, M.D.; Broström, A.; Pakpour, A.H. Psychometric validation of the Persian nine-item Internet Gaming Disorder Scale—Short Form: Does gender and hours spent online gaming affect the interpretations of item descriptions? J. Behav. Addict. 2017, 6, 256–263. [Google Scholar] [CrossRef]
- Pontes, H.M.; Macur, M.; Griffiths, M.D. Internet Gaming Disorder among Slovenian primary schoolchildren: Findings from a nationally representative sample of adolescents. J. Behav. Addict. 2016, 5, 304–310. [Google Scholar] [CrossRef]
- Monacis, L.; De Palo, V.; Griffiths, M.D.; Sinatra, M. Validation of the Internet Gaming Disorder Scale—Short-Form (IGDS9-SF) in an Italian-speaking sample. J. Behav. Addict. 2016, 5, 683–690. [Google Scholar] [CrossRef]
- Evren, C.; Dalbudak, E.; Topcu, M.; Kutlu, N.; Evren, B.; Pontes, H.M. Psychometric validation of the Turkish nine-item Internet Gaming Disorder Scale—Short Form (IGDS9-SF). Psychiatry Res. 2018, 265, 349–354. [Google Scholar] [CrossRef]
- Siddiqui, J.A.; Qureshi, S.F.; Alghamdi, A.K. Internet gaming disorder: A case report. J. Behav. Health 2018, 7, 41–44. [Google Scholar] [CrossRef]
- Hadwiger, A.N.; Middleman, A.B.; Pitt, P.D. Case series: Gaming vs. eating—Comorbidity of ARFID and IGD. Eat. Weight Disord. 2019. [Google Scholar] [CrossRef]
- Cai, C.; Yuan, K.; Yin, J.; Feng, D.; Bi, Y.; Li, Y.; Yu, D.; Jin, C.; Qin, W.; Tian, J. Striatum morphometry is associated with cognitive control deficits and symptom severity in internet gaming disorder. Brain Imag. Behav. 2015. [Google Scholar] [CrossRef] [PubMed]
- Khazaal, Y.; Breivik, K.; Billieux, J.; Zullino, D.; Thorens, G.; Achab, S.; Gmel, G.; Chatton, A. Game addiction scale assessment through a nationally representative sample of young adult men: Item response theory graded–response modeling. J. Med. Intern. Res. 2018, 20, e10058. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Zhang, S.; Turel, O.; Bechara, A.; He, Q. A tripartite neurocognitive model of internet gaming disorder. Front. Psychiatry 2017, 8, 285. [Google Scholar] [CrossRef]
- Luijten, M.; Meerkerk, G.J.; Franken, I.H.A.; Van de Wetering, B.J.M.; Schoenmakers, T.M. An fMRI study of cognitive control in problem gamers. Psychiatry Res. 2015, 231, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Korkeila, J.; Kaarlas, S.; Jääskeläinen, M.; Vahlberg, T.; Taiminen, T. Attached to the web—Harmful use of the Internet and its correlates. Eur. Psychiatry 2010, 25, 236–241. [Google Scholar] [CrossRef]
- Charlton, J.P.; Danforth, I.D.W. Distinguishing addiction and high engagement in the context of online game playing. Comput. Hum. Behav. 2007, 23, 1531–1548. [Google Scholar] [CrossRef] [Green Version]
- Charlton, J.P. A factor-analytic investigation of computer ‘addiction’ and engagement. Br. J. Psychol. 2002, 93, 329–344. [Google Scholar] [CrossRef]
- Snodgrass, J.G.; Zhao, W.; Lacy, M.G.; Zhang, S.; Tate, R. Distinguishing core from peripheral psychiatric symptoms: Addictive and problematic internet gaming in North America, Europe, and China. Cult. Med. Psychiatry 2018. [Google Scholar] [CrossRef]
- Iten, G.H.; Bopp, J.A.; Steiner, C.; Opwis, K.; Mekler, E.D. Does a prosocial decision in video games lead to increased prosocial real-life behavior? The impact of reward and reasoning. Comput. Hum. Behav. 2018, 89, 163–172. [Google Scholar] [CrossRef]
- Sundberg, M. Online gaming, loneliness and friendships among adolescents and adults with ASD. Comput. Hum. Behav. 2018, 79, 105–110. [Google Scholar] [CrossRef]
- Petry, N.M.; O’Brien, C.P. Internet Gaming Disorder and the DSM-5. Addiction 2013, 108, 1186–1187. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.M.; Rehbein, F.; Ko, C.H.; O’Brien, C.P. Internet Gaming Disorder in the DSM-5. Curr. Psychiatry Rep. 2015, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Billieux, J.; Schimmenti, A.; Khazaal, Y.; Maurage, P.; Heeren, A. Are we overpathologizing everyday life? A tenable blueprint for behavioral addiction research. J. Behav. Addict. 2015, 4, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Item | IGDS9-SF Item Wording | Clinical Criteria | Included in the ICD-11? |
|---|---|---|---|
| 1 | Do you feel preoccupied with your gaming behavior? (Some examples: Do you think about previous gaming activity or anticipate the next gaming session? Do you think gaming has become the dominant activity in your daily life?) | Preoccupation | No |
| 2 | Do you feel more irritability, anxiety or even sadness when you try to either reduce or stop your gaming activity? | Withdrawal | No |
| 3 | Do you feel the need to spend increasing amount of time engaged gaming in order to achieve satisfaction or pleasure? | Tolerance | No |
| 4 | Do you systematically fail when trying to control or cease your gaming activity? | Loss of control | Yes |
| 5 | Have you lost interests in previous hobbies and other entertainment activities as a result of your engagement with the game? | Giving up other activities | Yes |
| 6 | Have you continued your gaming activity despite knowing it was causing problems between you and other people? | Continuation | Yes |
| 7 | Have you deceived any of your family members, therapists or others because the amount of your gaming activity? | Deception | No |
| 8 | Do you play in order to temporarily escape or relieve a negative mood (e.g., helplessness, guilt, anxiety)? | Escape | No |
| 9 | Have you jeopardized or lost an important relationship, job or an educational or career opportunity because of your gaming activity? | Negative consequences | Yes |
| Rule | IGD Criteria Endorsement Pathways | Gamer Subtype | ||
|---|---|---|---|---|
| 1 | ‘withdrawal’ ≤ 4; 0.19% (95% CI 0.03–0.34) | ‘preoccupation’ ≤ 4; 0% (95% CI 0–0), n = 3061 | ‘Healthy’ | |
| 2 | ‘withdrawal’ ≤ 4; 0.19% (95% CI 0.03–0.34) | ‘preoccupation’ = 5; 7.14% (95% CI 1.63–12.65), n = 84 | ‘Preoccupied’ | |
| 3 | ‘withdrawal’ = 5; 32.46% (95% CI 22.01–42.92) | ‘loss of control’ ≤ 4; 8.00% (95% CI 0.48–15.51) | ‘negative consequences’ ≤ 3; 0% (95% CI 0–0), n = 35 | ‘Low Risk’ |
| 4 | ‘withdrawal’ = 5; 32.46% (95% CI 22.01–42.92) | ‘loss of control’ ≤ 4; 8.00% (95% CI 0.48–15.51) | ‘negative consequences’ > 3; 26.66% (95% CI 4.28–49.04), n = 15 | ‘Harmful’ |
| 5 | ‘withdrawal’ = 5; 32.46% (95% CI 22.01–42.92) | ‘loss of control’ = 5; 77.77% (95% CI 62.09–93.45), n = 27 | ‘Impaired Self-Control’ | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pontes, H.M.; Schivinski, B.; Brzozowska-Woś, M.; Stavropoulos, V. Laxer Clinical Criteria for Gaming Disorder May Hinder Future Efforts to Devise an Efficient Diagnostic Approach: A Tree-Based Model Study. J. Clin. Med. 2019, 8, 1730. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101730
Pontes HM, Schivinski B, Brzozowska-Woś M, Stavropoulos V. Laxer Clinical Criteria for Gaming Disorder May Hinder Future Efforts to Devise an Efficient Diagnostic Approach: A Tree-Based Model Study. Journal of Clinical Medicine. 2019; 8(10):1730. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101730
Chicago/Turabian StylePontes, Halley M., Bruno Schivinski, Magdalena Brzozowska-Woś, and Vasileios Stavropoulos. 2019. "Laxer Clinical Criteria for Gaming Disorder May Hinder Future Efforts to Devise an Efficient Diagnostic Approach: A Tree-Based Model Study" Journal of Clinical Medicine 8, no. 10: 1730. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8101730