The Effect of the Intelligent Sepsis Management System on Outcomes among Patients with Sepsis and Septic Shock Diagnosed According to the Sepsis-3 Definition in the Emergency Department

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
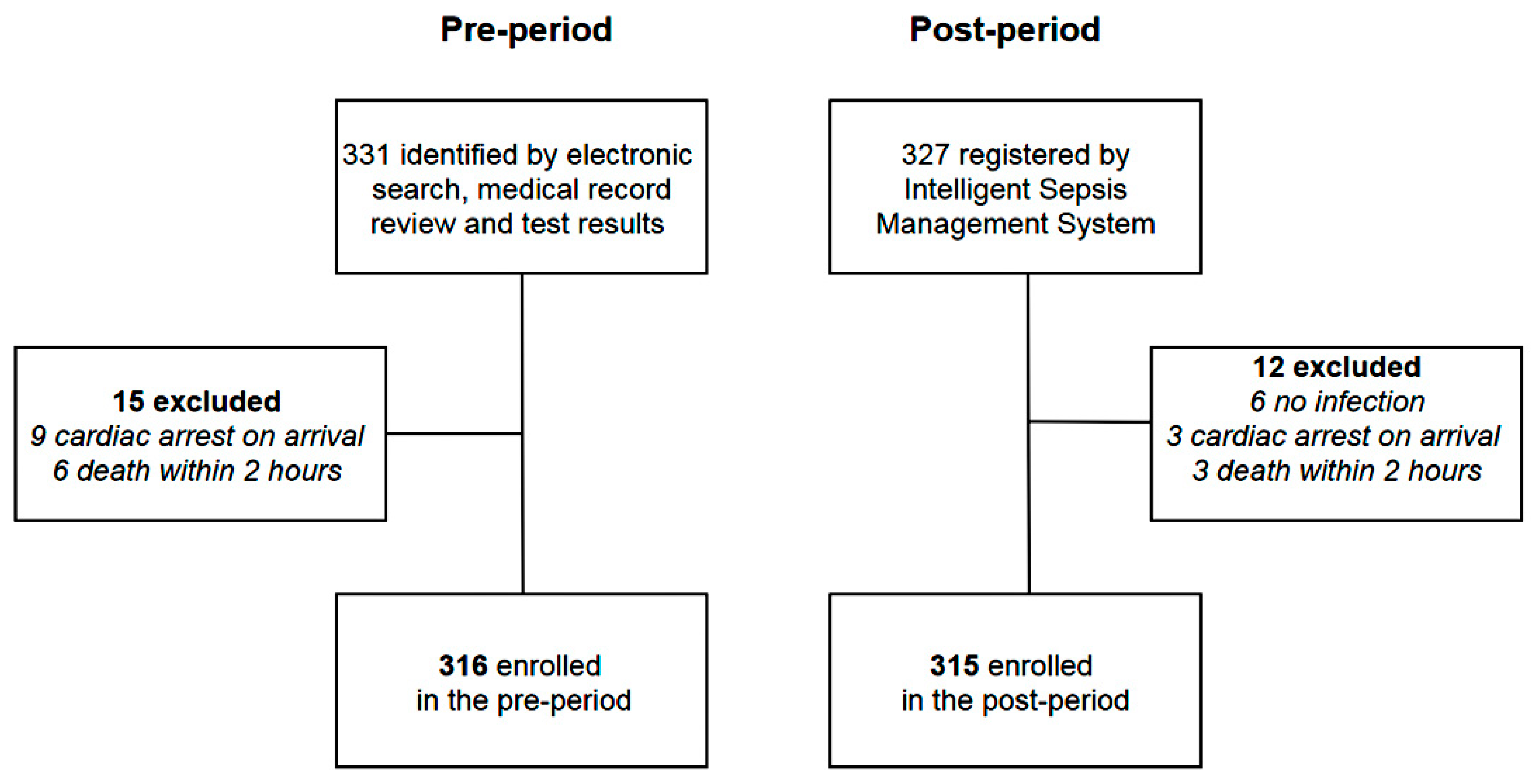
2.2. Study Population
2.3. Intervention
2.4. Definitions
2.5. Data Collection
2.6. Outcomes
2.7. Statistical Analyses
3. Results
3.1. Characteristics of Pre- and Post-Implementation
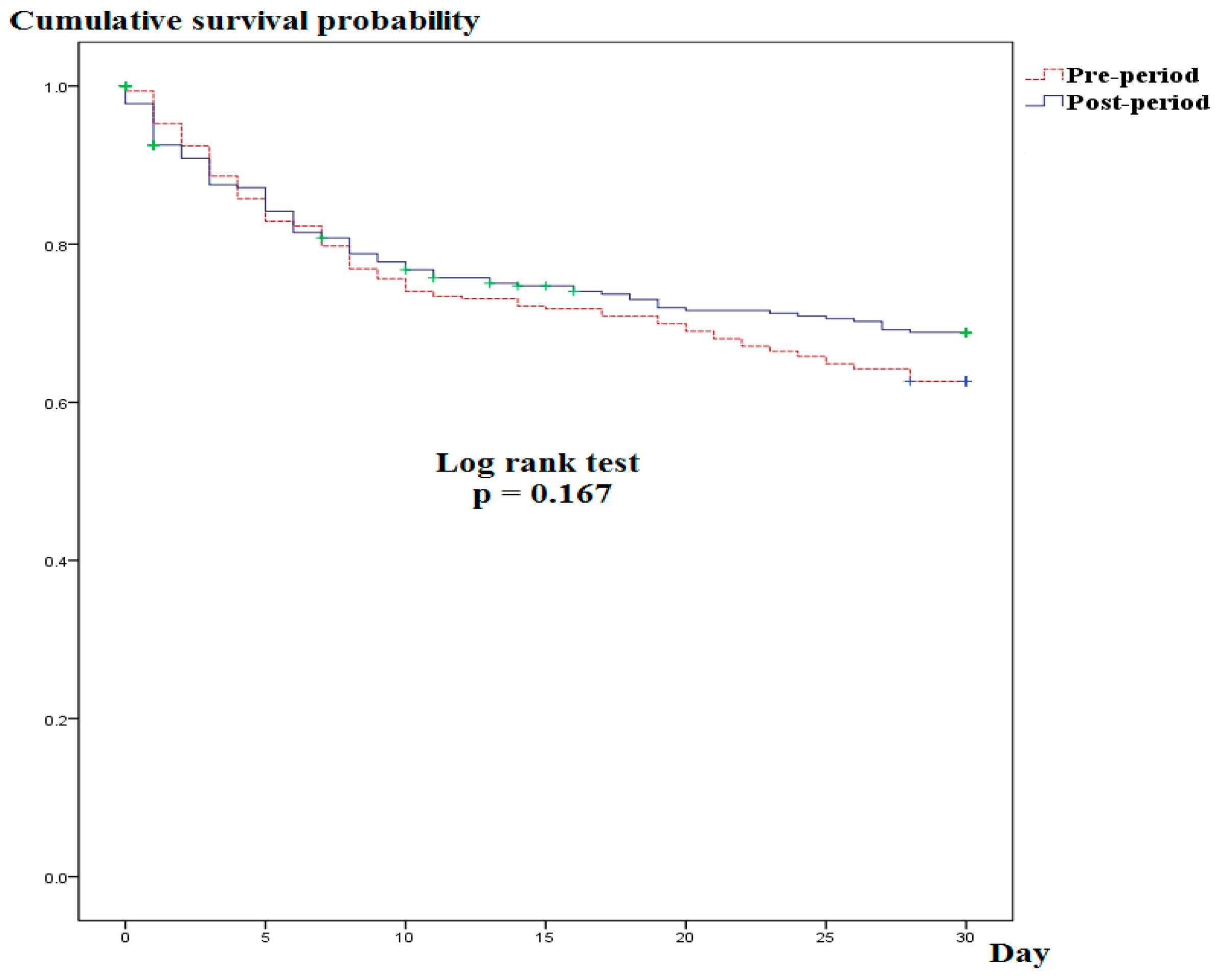
3.2. Outcomes
3.3. Risk Factors For 30-Day Mortality
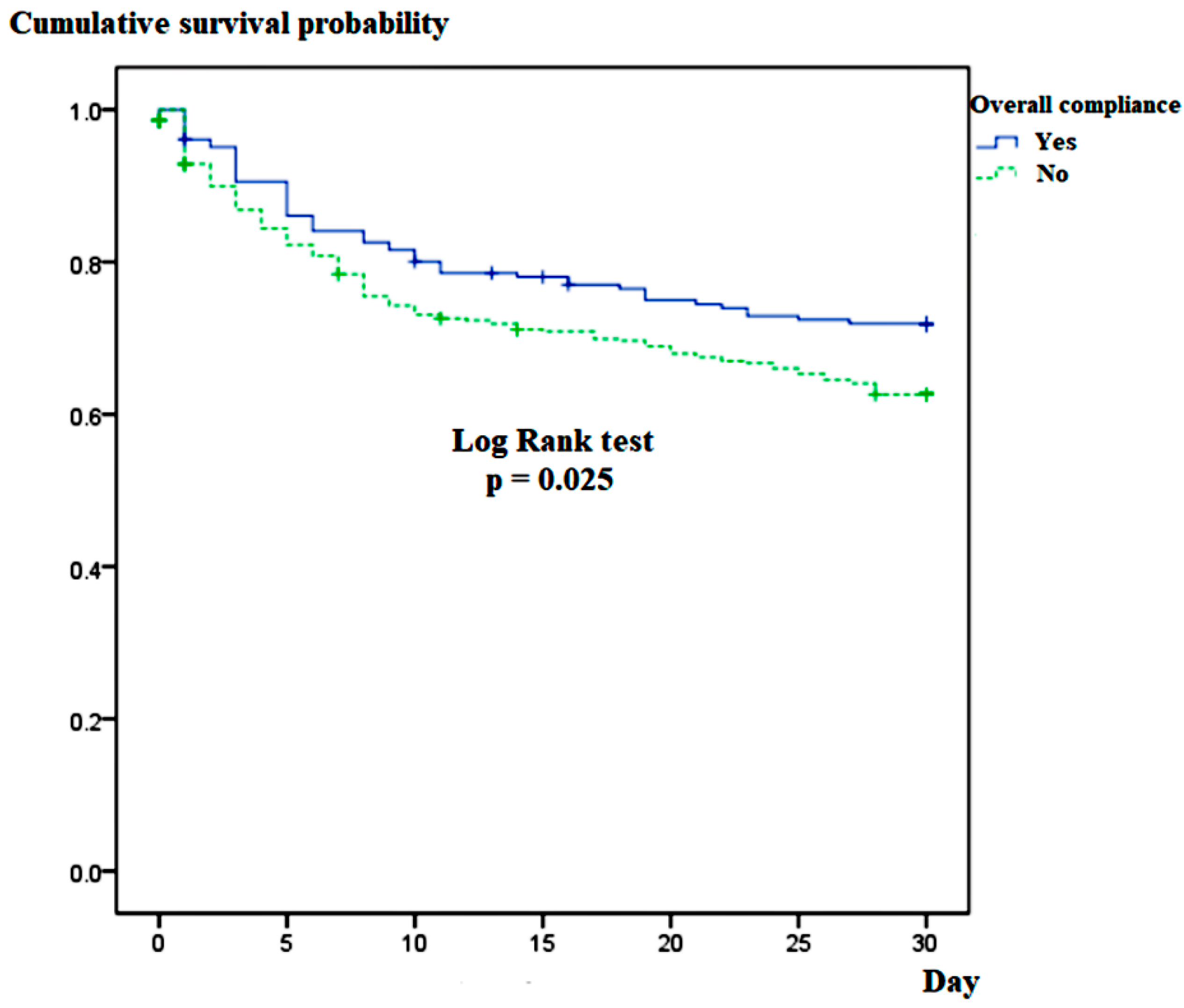
3.4. Comparisons Between the Compliance and Non-Compliance Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vincent, J.L.; Marshall, J.C.; Namendys-Silva, S.A.; François, B.; Martin-Loeches, I.; Lipman, J.; Reinhart, K.; Antonelli, M.; Pickkers, P.; Njimi, H.; et al. Assessment of the worldwide burden of critical illness: The intensive care over nations (ICON) audit. Lancet Respir. Med. 2014, 22, 380–386. [Google Scholar] [CrossRef]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. International Forum of Acute Care Trialists: Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Torio, C.M.; Andrews, R.M. National inpatient hospital costs: The most expensive conditions by payer, 2011: Statistical Brief #160. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013. [Google Scholar]
- Gaieski, D.F.; Edwards, J.M.; Kallan, M.J.; Carr, B.G. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit. Care Med. 2013, 41, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International guidelines for management of sepsis and septic shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Ferrer, R.; Artigas, A.; Levy, M.M.; Blanco, J.; González-Díaz, G.; Garnacho-Montero, J.; Ibáñez, J.; Palencia, E.; Quintana, M.; de la Torre-Prados, M.V.; et al. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA 2008, 299, 2294–2303. [Google Scholar] [CrossRef]
- Burrell, A.R.; McLaws, M.L.; Fullick, M.; Sullivan, R.B.; Sindhusake, D. SEPSIS KILLS: Early intervention saves lives. Med. J. Aust. 2016, 204, 73. [Google Scholar] [CrossRef]
- Castellanos-Ortega, A.; Suberviola, B.; Garcia-Astudillo, L.A.; Holanda, M.S.; Ortiz, F.; Llorca, J.; Delgado-Rodriguez, M. Impact of the Surviving Sepsis Campaign protocols on hospital length of stay and mortality in septic shock patients: Results of a three-year follow-up quasi-experimental study. Crit. Care Med. 2010, 38, 1036–1043. [Google Scholar] [CrossRef]
- Micek, S.T.; Roubinian, N.; Heuring, T.; Bode, M.; Williams, J.; Harrison, C.; Murphy, T.; Prentice, D.; Ruoff, B.E.; Kollef, M.H. Before-after study of a standardized hospital order set for the management of septic shock. Crit. Care Med. 2006, 34, 2707–2713. [Google Scholar] [CrossRef]
- Viale, P.; Tedeschi, S.; Scudeller, L.; Attard, L.; Badia, L.; Bartoletti, M.; Cascavilla, A.; Cristini, F.; Dentale, N.; Fasulo, G.; et al. Infectious diseases team for the early management of severe sepsis and septic shock in the emergency department. Clin. Infect. Dis. 2017, 65, 1253–1259. [Google Scholar] [CrossRef]
- McColl, T.; Gatien, M.; Calder, L.; Yadav, K.; Tam, R.; Ong, M.; Taljaard, M.; Stiell, I. Implementation of an emergency department sepsis bundle and system redesign: A process improvement initiative. CJEM 2017, 19, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Brandt, B.N.; Gartner, A.B.; Moncure, M.; Cannon, C.M.; Carlton, E.; Cleek, C.; Wittkopp, C.; Simpson, S.Q. Identifying severe sepsis via electronic surveillance. Am. J. Med. Qual. 2015, 30, 559–565. [Google Scholar] [CrossRef] [PubMed]
- McRee, L.; Thanavaro, J.L.; Moore, K.; Goldsmith, M.; Pasvogel, A. The impact of an electronic medical record surveillance program on outcomes for patients with sepsis. Heart Lung 2014, 43, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, N.; Gross, A.K.; Pintens, M.; Fee, C.; MacDougall, C. Effect of an electronic medical record alert for severe sepsis among ED patients. Am. J. Emerg. Med. 2016, 34, 185–188. [Google Scholar] [CrossRef]
- Sawyer, A.M.; Deal, E.N.; Labelle, A.J.; Witt, C.; Thiel, S.W.; Heard, K.; Reichley, R.M.; Micek, S.T.; Kollef, M.H. Implementation of a real-time computerized sepsis alert in nonintensive care unit patients. Crit. Care Med. 2011, 39, 469–473. [Google Scholar] [CrossRef]
- Kievlan, D.R.; Zhang, L.A.; Chang, C.H.; Angus, D.C.; Seymour, C.W. Evaluation of repeated Quick Sepsis-Related Organ Failure Assessment Measurements among patients with suspected infection. Crit. Care Med. 2018, 46, 1906–1913. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Sepsis Definitions Task Force: Developing a new definition and assessing new clinical criteria for septic shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]
- Pruinelli, L.; Westra, B.L.; Yadav, P.; Hoff, A.; Steinbach, M.; Kumar, V.; Delaney, C.W.; Simon, G. Delay within the 3-hour Surviving Sepsis Campaign Guideline on mortality for patients with severe sepsis and septic shock. Crit. Care Med. 2018, 46, 500–505. [Google Scholar] [CrossRef]
- Garg, A.X.; Adhikari, N.K.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: A systematic review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef]
- Westra, B.L.; Landman, S.; Yadav, P.; Steinbach, M. Secondary analysis of an electronic surveillance system combined with multi-focal interventions for early detection of sepsis. Appl. Clin. Inform. 2017, 8, 47–66. [Google Scholar] [CrossRef]
- Hooper, M.H.; Weavind, L.; Wheeler, A.P.; Martin, J.B.; Gowda, S.S.; Semler, M.W.; Hayes, R.M.; Albert, D.W.; Deane, N.B.; Nian, H.; et al. Randomized trial of automated, electronic monitoring to facilitate early detection of sepsis in the intensive care unit. Crit. Care Med. 2012, 40, 2096–2101. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Weavind, L.; Hooper, M.H.; Rice, T.W.; Gowda, S.S.; Nadas, A.; Song, Y.; Martin, J.B.; Bernard, G.R.; Wheeler, A.P. An electronic tool for the evaluation and treatment of sepsis in the ICU: A randomized controlled trial. Crit. Care Med. 2015, 43, 1595–1602. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of clinical criteria for sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, R.M.; Greenwood, J.C.; Nuckton, T.J.; Darger, B.; Shofer, F.S.; Troeger, D.; Jung, S.Y.; Speich, K.G.; Valencia, J.; Kilgannon, J.H.; et al. Comparison of qSOFA with current emergency department tools for screening of patients with sepsis for critical illness. Emerg. Med. J. 2018, 35, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Franchini, S.; Duca, A. qSOFA should replace SIRS as the screening tool for sepsis. Crit. Care 2016, 20, 409. [Google Scholar] [CrossRef] [Green Version]
- Haydar, S.; Spanier, M.; Weems, P.; Wood, S.; Strout, T. Comparison of QSOFA score and SIRS criteria as screening mechanisms for emergency department sepsis. Am. J. Emerg. Med. 2017, 35, 1730–1733. [Google Scholar] [CrossRef]
- Yealy, D.M.; Kellum, J.A.; Huang, D.T.; Barnato, A.E.; Weissfeld, L.A.; Pike, F.; Terndrup, T.; Wang, H.E.; Hou, P.C.; ProCESS Investigators; et al. A randomized trial of protocol-based care for early septic shock. N. Engl. J. Med. 2014, 370, 1683–1693. [Google Scholar]
- Peake, S.L.; Delaney, A.; Bailey, M.; Bellomo, R.; Cameron, P.A.; Cooper, D.J.; Higgins, A.M.; Holdgate, A.; ARISE Investigators; ANZICS Clinical Trials Group; et al. Goal-directed resuscitation for patients with early septic shock. N. Engl. J. Med. 2014, 371, 1496–1506. [Google Scholar]
- Mouncey, P.R.; Osborn, T.M.; Power, G.S.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Jahan, R.; Harvey, S.E.; Bell, D.; Bion, J.F.; et al. Trial of early, goal-directed resuscitation for septic shock. N. Engl. J. Med. 2015, 372, 1301–1311. [Google Scholar] [CrossRef]
- Rowan, K.M.; Angus, D.C.; Bailey, M.; Barnato, A.E.; Bellomo, R.; Canter, R.R.; Coats, T.J.; Delaney, A.; Gimbel, E.; PRISM Investigators; et al. Early, goal-directed therapy for septic shock—A patient-level meta-analysis. N. Engl. J. Med. 2017, 376, 2223–2234. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Pre-Period (n = 316) | Post-Period (n = 315) | p-Value |
|---|---|---|---|
| Age (years), median (IQR) | 74 (64–81) | 77 (65–83) | 0.048 |
| Age class (years), n (%) | |||
| <50 | 25 (8) | 24 (8) | |
| 50–59 | 78 (25) | 76 (24) | |
| 60–69 | 103 (33) | 105 (33) | |
| 70–79 | 71 (22) | 72 (23) | |
| ≥80 | 39 (12) | 38 (12) | |
| Male, n (%) | 187 (59.2) | 164 (52.1) | 0.083 |
| Charlson comorbidity index, median (IQR) | 4 (3–6) | 4 (3–5) | 0.546 |
| Korean triage acuity scale, mean (SD) | 2.3 (0.6) | 2.2 (0.6) | 0.627 |
| Quick SOFA criteria, n (%) | |||
| RR ≥ 22/min | 147 (47) | 144 (46) | 0.718 |
| SBP ≤ 100 mmHg | 132 (42) | 137 (43) | 0.752 |
| Altered mental status (GCS < 15) | 159 (50) | 156 (50) | 0.879 |
| Pre-ED antibiotics, n (%) (≤12 h) | 31 (10) | 33 (10) | 0.317 |
| Infection sites, n (%) (multiple selections, if any) | |||
| Respiratory | 198 (63) | 201 (64) | 0.734 |
| Genitourinary | 75 (24) | 71 (23) | 0.697 |
| Gastrointestinal | 36 (11) | 34 (11) | |
| Skin and soft tissue | 11 (3) | 12 (4) | |
| Other sites | 21 (7) | 19 (6) | |
| Biomarkers, median (IQR) | |||
| CRP (mg/dL) | 10.5 (4.6–18.3) | 10.6 (4.7–18.5) | 0.734 |
| Procalcitonin (ng/ml) | 2.4 (1.3–11.8) | 1.2 (0.8–9.7) | 0.028 |
| Lactate (mmol/L) | 2.9 (1.2–5.1) | 2.8 (1.1–4.9) | 0.821 |
| Septic shock, n (%) | 135 (42.7) | 138 (43.8) | 0.779 |
| SOFA score, median (IQR) | 8 (4–11) | 8 (5–11) | 0.343 |
| Length of hospital stay (days), median (IQR) | 10 (3–15) | 9 (3–14) | 0.296 |
| Length of ICU stay (days), median (IQR) | 5 (2–7) | 4 (2–6) | 0.213 |
| Outcomes | Pre-Period (n = 316) | Post-Period (n = 315) | p-Value |
|---|---|---|---|
| Overall compliance with SSC bundle, n (%) | 34 (10.8) | 172 (54.6) | <0.001 |
| Appropriate fluid resuscitation | 245 (77.5) | 281 (89.2) | <0.001 |
| Broad-spectrum antibiotics administered within 3 h of ED presentation | 226 (71.5) | 239 (75.9) | 0.214 |
| Blood culture before antibiotic administration | 255 (80.7) | 304 (96.5) | <0.001 |
| At least two lactate level measurements within 6 h of ED presentation | 37 (11.7) | 265 (84.1) | <0.001 |
| Time to first antibiotic administration (min), median (IQR) | 125 (79–203) | 121 (75–198) | 0.597 |
| All-cause 7-day mortality, n (%) | 64 (20.3) | 58 (18.4) | 0.558 |
| All-cause 14-day mortality, n (%) | 87 (27.5) | 76 (24.1) | 0.329 |
| All-cause 30-day mortality, n (%) | 118 (37.3) | 93 (29.5) | 0.037 |
| Variable | Hazards Ratio (95% CI) | p Value | Adjusted Hazards Ratio (95% CI) | p Value |
|---|---|---|---|---|
| Age | 1.02 (1.01–1.03) | 0.001 | 1.013 (1.002–1.023) | 0.021 |
| Male | 1.08 (0.83–1.42) | 0.564 | ||
| SOFA score | 1.27 (1.22–1.32) | <0.001 | 1.21 (1.15–1.26) | 0.002 |
| Septic shock | 3.45 (2.58–4.60) | <0.001 | 1.83 (0.97–2.76) | 0.18 |
| Overall compliance with SSC bundle | 0.71 (0.52–0.96) | 0.027 | 0.62 (0.44–0.86) | 0.004 |
| CRP | 1.01 (0.997–1.022) | 0.144 | 1.02 (0.995–1.028) | 0.168 |
| Lactate | 1.09 (1.06–1.12) | <0.001 | 1.06 (1.02–1.09) | 0.003 |
| Procalcitonin | 1.004 (1.00–1.01) | 0.053 | 1.001 (0.997–1.006) | 0.779 |
| Time to first antibiotics (min) | 0.999 (0.998–1.000) | 0.041 | 0.998 (0.997–1.000) | 0.059 |
| Post-period | 0.83 (0.63–1.09) | 0.172 | 0.75 (0.55–1.04) | 0.151 |
| Characteristic | Overall Compliance Group (n = 206) | Non-Compliance Group (n = 425) | p-Value |
|---|---|---|---|
| Age (years), median (IQR) | 75 (63–82) | 76 (66–83) | 0.794 |
| Male, n (%) | 107 (51.9) | 244 (57.4) | 0.195 |
| Charlson Comorbidity Index, median (IQR) | 4 (3–5) | 4 (3–6) | 0.631 |
| Biomarkers, median (IQR) | |||
| CRP (mg/dL) | 10.5 (5.3–18.4) | 10.5 (5.4–18.5) | 0.867 |
| Procalcitonin (ng/mL) | 1.0 (0.3–8.5) | 1.8 (0.4–14.7) | 0.148 |
| Lactate (mmol/L) | 2.9 (1.5–5.1) | 2.9 (1.4–4.9) | 0.484 |
| Septic shock, n (%) | 93 (45.1) | 180 (42.4) | 0.507 |
| SOFA score, n (%) | 8 (6–10) | 8 (5–10) | 0.111 |
| Post-period, n (%) | 172 (83.5) | 143 (33.6) | <0.001 |
| 7-day mortality, n (%) | 32 (15.5) | 90 (21.2) | 0.092 |
| 14-day mortality, n (%) | 44 (21.4) | 119 (28.0) | 0.074 |
| 30-day mortality, n (%) | 56 (27.2) | 155 (36.5) | 0.020 |
| Variable | Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Age | 1.23 (0.88–1.60) | 0.472 | ||
| Male | 1.06 (0.88–1.24) | 0.374 | ||
| SOFA score | 0.94 (0.90–1.13) | 0.398 | ||
| Septic shock | 0.89 (0.64–1.25) | 0.507 | ||
| CRP | 1.04 (0.97–1.18) | 0.514 | ||
| Lactate | 0.93 (0.86–1.02) | 0.089 | 0.94 (0.83–1.12) | 0.207 |
| Procalcitonin | 1.04 (0.93–1.13) | 0.495 | ||
| Post-period | 9.98 (6.56–15.17) | <0.001 | 9.51 (6.38–14.03) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.; Cho, H.; Park, D.W.; Ahn, S.; Kim, J.Y.; Seok, H.; Park, J.; Moon, S. The Effect of the Intelligent Sepsis Management System on Outcomes among Patients with Sepsis and Septic Shock Diagnosed According to the Sepsis-3 Definition in the Emergency Department. J. Clin. Med. 2019, 8, 1800. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111800
Song J, Cho H, Park DW, Ahn S, Kim JY, Seok H, Park J, Moon S. The Effect of the Intelligent Sepsis Management System on Outcomes among Patients with Sepsis and Septic Shock Diagnosed According to the Sepsis-3 Definition in the Emergency Department. Journal of Clinical Medicine. 2019; 8(11):1800. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111800
Chicago/Turabian StyleSong, Juhyun, Hanjin Cho, Dae Won Park, Sejoong Ahn, Joo Yeong Kim, Hyeri Seok, Jonghak Park, and Sungwoo Moon. 2019. "The Effect of the Intelligent Sepsis Management System on Outcomes among Patients with Sepsis and Septic Shock Diagnosed According to the Sepsis-3 Definition in the Emergency Department" Journal of Clinical Medicine 8, no. 11: 1800. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8111800