Effects of Physical Exercises and Verbal Stimulation on the Functional Efficiency and Use of Free Time in an Older Population under Institutional Care: A Randomized Controlled Trial

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
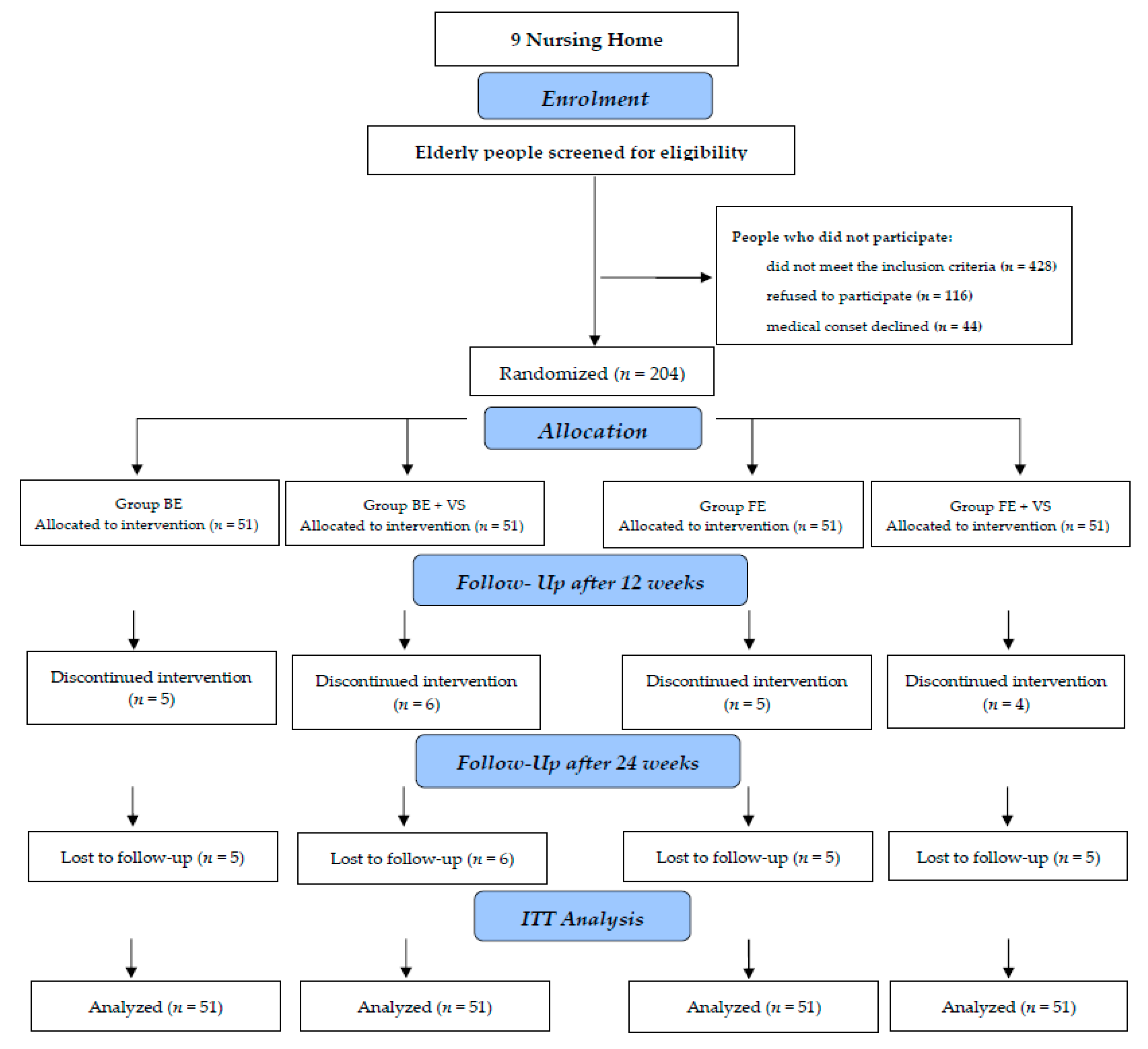
2.1. Trial Design
2.2. Participants
2.3. Interventions
Exercise Program
- Generating extrinsic motivation: the participants were informed about a small reward at the end of the program. Seniors were involved in a given activity to achieve extrinsic consequences. After performing physical exercises, a meeting was organized, at which diplomas for participation in the exercises and commemorative photos were handed out.
- Generating intrinsic motivation: a model for class management was developed, which assumed that the participants would achieve the set goals (challenges). The subjective feelings associated with performing physical exercises and independent steps towards a goal were strengthened. In accordance with the assumptions of the theory of competence-based models of intrinsic motivation [20], the examined person best estimates, depending on individual beliefs based on the significance of the goals established by them, the possibilities of motivation
- Explanation of the importance of physical activity in order to maintain independence and health;
- illustrations of exercises that older people could perform on their own after completing the program;
- description of fears and barriers appearing while physical activity is undertaken by older people and a description of the necessary ways to overcome them.
2.4. Outcome Measures
2.4.1. Main Outcome
2.4.2. Secondary Outcomes
Physical Activity Assessment
Functional Assessment
Muscular Strength Assessments
Mobility Assessment
Flexibility Assessment
Body Balance Assessment
2.5. Other Outcomes
2.5.1. Postural Stability Assessment
2.5.2. Quality of Life Assessment
2.6. Sample Size
2.7. Randomization and Blinding
2.8. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ministry of Family, Labour and Social Policy of the Republic of Poland. Available online: http://senior.gov.pl/materialy_i_badania/pokaz/399 (accessed on 25 November 2019).
- Statistics Poland. Available online: https://stat.gov.pl/obszary-tematyczne/warunki-zycia/ubostwo-pomoc-spoleczna/zaklady-stacjonarne-pomocy-spolecznej-w-2017-roku,18,2.html (accessed on 25 November 2019).
- Forder, J.; Fernandez, J.-L. Length of stay in care homes. Report commissioned by Bupa Care Services, PSSRU Discussion Paper 2769, Canterbury: PSSRU. Available online: https://eprints.lse.ac.uk/33895/1/dp2769.pdf (accessed on 25 November 2019).
- Centers for Disease Control and Prevention. Reporting System (WISQARS) National Center for Injury Prevention and Control. Available online: https://www.cdc.gov/injury/wisqars/index.html. (accessed on 25 November 2019).
- Llamas-Velasco, S.; Villarejo-Galende, A.; Contador, I.; Lora Pablos, D.; Hernández-Gallego, J.; Bermejo-Pareja, F. Physical activity and long-term mortality risk in older adults: A prospective population based study (NEDICES). Prev. Med. Rep. 2016, 4, 546–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekelund, U.; Ward, H.A.; Norat, T.; Luan, J.; May, A.M.; Weiderpass, E.; Sharp, S.J.; Overvad, K.; Østergaard, J.N.; Tjønneland, A.; et al. Physical activity and all-cause mortality across levels of overall and abdominal adiposity in European men and women: The European Prospective Investigation into Cancer and Nutrition Study (EPIC). Am. J. Clin. Nutr. 2015, 101, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Horton, R. Rethinking our approach to physical activity. Lancet 2012, 380, 189–190. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. U.S. Physical activity statistics. Available online: https://www.cdc.gov/physicalactivity/data/index.html (accessed on 25 November 2019).
- Kozdroń, E. Program Rekreacji Ruchowej Osób Starszych; Akademia Wychowania Fizycznego: Warszawa, Poland, 2008; pp. 73–75. [Google Scholar]
- Douma, J.G.; Volkers, K.M.; Engels, G.; Sonneveld, M.H.; Goossens, R.; Scherder, E. Setting-related influences on physical inactivity of older adults in residential care settings: A review. BMC Geriatrics 2017, 17, 97. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Zhao, Y.; Wang, G.; Zhang, H.; Ren, Y.; Wang, B.; Zhang, L.; Yang, X.; Han, C.; Pang, C.; et al. Body mass index and waist circumference combined predicts obesity-related hypertension better than either alone in a rural Chinese population. Sci. Rep. 2016, 6, 31935. [Google Scholar] [CrossRef] [Green Version]
- Resnick, B.; Spellbring, A.M. Understanding what motivates older adults to exercise. J. Gerontol. Nurs. 2000, 26, 34–42. [Google Scholar] [CrossRef]
- Resnick, B. Geriatric rehabilitation: The influence of efficacy beliefs and motivation. Rehabil. Nurs. 2002, 27, 152–159. [Google Scholar] [CrossRef]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gomez, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age (Dordr) 2014, 36, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Marcos-Pardo, P.J.; Martínez-Rodríguez, A.; Gil-Arias, A. Impact of a motivational resistance-training programme on adherence and body composition in the elderly. Sci. Rep. 2018, 8, 1370. [Google Scholar] [CrossRef] [Green Version]
- Farrance, C.; Tsofliou, F.; Clark, C. Adherence to community based group exercise interventions for older people: A mixed-methods systematic review. Prev. Med. 2016, 87, 155–166. [Google Scholar] [CrossRef] [Green Version]
- de Souto Barreto, P.; Morley, J.E.; Chodzko-Zajko, W.; Pitkala, K.H.; Weening-Djiksterhuis, E.; Rodriguez-Mañas, L.; Barbagallo, M.; Rosendahl, E.; Sinclair, A.; Landi, F.; et al. Recommendations on Physical Activity and Exercise for Older Adults Living in Long-Term Care Facilities: A Taskforce Report. J. Am. Med. Dir. Assoc. 2016, 17, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.H.; Elavsky, S.; Koo, K.M. Factors influencing physical activity in older adults. J. Exerc. Rehab. 2014, 10, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Losier, G.F.; Bourque, P.E.; Vallerand, R.J. A Motivational Model of Leisure Participation in the Elderly. J. Psychol. 1993, 127, 153–170. [Google Scholar] [CrossRef]
- Locke, E.A. Motivation through conscious goal setting. Appl. Prev. Psychol. 1996, 5, 117–124. [Google Scholar] [CrossRef]
- Fryderyk-Łukasik, M. Comprehensive Geriatric Assessment in everyday geriatric and caring practice. Geriatr. Opieka Długoter. 2015, 1, 1–6. [Google Scholar]
- Albiński, R.; Kleszczewska-Albińska, A.; Bedyńska, S. Geriatric Depression Scale (GDS). Validity and reliability of different versions of the scale-review. Psychiatr. Pol. 2018, 45, 555–562. [Google Scholar]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, 85–94. [Google Scholar] [CrossRef]
- Washburn, R.A.; Smith, K.W.; Jette, A.M.; Janney, C.A. The physical activity scale for the elderly (PASE): Development and evaluation. J. Clin. Epidemiol. 1993, 46, 153–162. [Google Scholar] [CrossRef]
- Rubenstein, L.V.; Calkins, D.R.; Greenfield, S.; Jette, A.M.; Meenan, R.F.; Nevins, M.A.; Rubenstein, L.Z.; Wasson, J.H.; Williams, M.E. Health status assessment for elderly patients. Report of the Society of General Internal Medicine Task Force on Health Assessment. J. Am. Geriatr. Soc. 1989, 37, 562–569. [Google Scholar] [CrossRef]
- Trampisch, U.S.; Franke, J.; Jedamzik, N.; Hinrichs, T.; Platen, P. Optimal Jamar dynamometer handle position to assess maximal isometric hand grip strength in epidemiological studies. J. Hand Surg. Am. 2012, 37, 2368–2373. [Google Scholar] [CrossRef] [PubMed]
- Schaubert, K.L.; Bohannon, R.W. Reliability and validity of three strength measures obtained from community dwelling elderly persons. J. Strength Cond. Res. 2005, 19, 717–720. [Google Scholar] [PubMed]
- Giladi, N.; Herman, T.; Reider-Groswasser, I.I.; Gurevich, T.; Hausdorff, J.M. Clinical characteristics of elderly patients with a cautious gait of unknown origin. J. Neurol. 2005, 252, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Catlin, P.A.; Gage, K.; Gurucharri, K.; Robertson, R.; Stephen, K. Establishing the reliability and validity of measurements of walking time using the Emory Functional Ambulation Profile. Phys. Ther. 1999, 79, 1122–1133. [Google Scholar] [CrossRef]
- Konopack, J.F.; Marquez, D.X.; Hu, L.; Elavsky, S.; McAuley, E.; Kramer, A.F. Correlates of functional fitness in older adults. Int. J. Behav. Med. 2008, 15, 311–318. [Google Scholar] [CrossRef]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiotherapy Canada 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Drzal-Grabiec, J.; Rachwał, M.; Trzaskoma, Z.; Rykała, J.; Podgórska-Bednarz, J.; Cichocka, I.; Truszczyńska, A.; Rąpała, K. The foot deformity versus postural control in females aged over 65 years. Acta. Bioeng. Biomech. 2014, 16, 73–80. [Google Scholar]
- Maruish, M.E. User’s manual for the SF-36v2 Health Survey, 3rd ed.; QualityMetric Incorporated: Lincoln, RI, USA, 2009; pp. 55–56. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods. 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Wiśniowska-Szurlej, A.; Ćwirlej-Sozańska, A.; Wilmowska-Pietruszyńska, A.; Milewska, N.; Sozański, B. The influence of 3 months of physical exercises and verbal stimulation on functional efficiency and use of free time in an older population under institutional care: Study protocol for a randomized controlled trial. Trials 2017, 18, 376. [Google Scholar]
- Sackley, C.M.; Levin, S.; Cardoso, K.; Hoppitt, T.J. Observations of activity levels and social interaction in a residential care setting. Int. J. Ther. Rehabil. 2006, 13, 370–373. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence, Occupational Therapy Interventions and Physical Activity Interventions to Promote the Mental Wellbeing of Older People in Primary Care and Residential Care, London: NICE, 2008. Available online: https://www.nice.org.uk/guidance/ph16/documents/occupational-therapy-and-physical-activity-interventions-to-promote-the-mental-wellbeing-of-older-people-in-primary-care-and-residential-care-review-proposal-consultation-document2 (accessed on 1 December 2019).
- Wilson, J.J.; Blackburn, N.E.; O’Reilly, R.; Kee, F.; Caserotti, P.; Tully, M.A. Association of objective sedentary behaviour and self-rated health in English older adults. BMC Res. Notes 2019, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J.; Blackwell, J.; Boraxbekk, C.J.; Caserotti, P.; Dela, F.; Evans, A.B.; Jespersen, A.P.; Gliemann, L.; Kramer, A.F.; Lundbye-Jensen, J.; et al. Copenhagen Consensus statement 2019: Physical activity and ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, B.; Smith, L.; Lorencatto, F.; Hamer, M.; Biddle, S.J. How to reduce sitting time? A review of behaviour change strategies used in sedentary behaviour reduction interventions among adults. Health. Psychol. Rev. 2016, 10, 89–112. [Google Scholar] [CrossRef] [Green Version]
- Fitzsimons, C.F.; Kirk, A.; Baker, G.; Michie, F.; Kane, C.; Mutrie, N. Using an individualised consultation and activPAL™ feedback to reduce sedentary time in older Scottish adults: Results of a feasibility and pilot study. Prev. Med. 2013, 57, 718–720. [Google Scholar] [CrossRef] [PubMed]
- Orrow, G.; Kinmonth, A.L.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillsdon, M.; Foster, C.; Thorogood, M. Interventions for promoting physical activity. Cochrane Database Syst. Rev. 2005, 1, CD003180. [Google Scholar]
- Chou, C.H.; Hwang, C.L.; Wu, Y.T. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: A meta-analysis. Arch. Phys. Med. Rehabil 2012, 93, 237–244. [Google Scholar] [CrossRef]
- de Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Silva, R.B.; Aldoradin-Cabeza, H.; Eslick, G.D.; Phu, S.; Duque, G. The Effect of Physical Exercise on Frail Older Persons: A Systematic Review. J. Frailty. Aging 2017, 6, 91–96. [Google Scholar]
- Crocker, T.; Forster, A.; Young, J.; Brown, L.; Ozer, S.; Smith, J.; Green, J.; Hardy, J.; Burns, E.; Glidewell, E.; et al. Physical rehabilitation for older people in long-term care. Cochrane Database Syst. Rev. 2013, CD004294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira, M.R.; da Silva, R.A.; Dascal, J.B.; Teixeira, D.C. Effect of different types of exercise on postural balance in elderly women: A randomized controlled trial. Arch. Gerontol. Geriatr. 2014, 59, 506–514. [Google Scholar] [CrossRef] [PubMed]
- de Vreede, P.L.; Samson, M.M.; van Meeteren, N.L.; Duursma, S.A.; Verhaar, H.J. Functional-task exercise versus resistance strength exercise to improve daily function in older women: A randomized, controlled trial. J. Am. Geriatr. Soc. 2005, 53, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Donoghue, D. Physiotherapy Research and Older People (PROP) group, Stokes EK. How much change is true change? The minimum detectable change of the Berg Balance Scale in elderly people. J. Rehabil. Med. 2009, 41, 343–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchamp, M.K.; Jette, A.M.; Ward, R.E.; Kurlinski, L.A.; Kiely, D.; Latham, N.K.; Bean, J.F. Predictive validity and responsiveness of patient-reported and performance-based measures of function in the Boston RISE study. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 616–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forster, A.; Lambley, R.; Hardy, J.; Young, J.; Smith, J.; Green, J.; Burns, E. Rehabilitation for older people in long-term care. Cochrane Database Syst. Rev. 2009, 1, CD004294. [Google Scholar]
- Prata, M.G.; Scheicher, M.E. Correlation between balance and the level of functional independence among elderly people. Sao Paulo M. J. 2012, 130, 97–101. [Google Scholar] [CrossRef]
- Weeks, L.E.; Profit, S.; Campbell, B.; Graham, H.; Chircop, A.; Sheppard-LeMoine, D. Participation in physical activity: Influences reported by seniors in the community and in long-term care facilities. J. Gerontol. Nurs. 2008, 34, 36–43. [Google Scholar] [CrossRef]


{kind=link}
| BE (n = 51) | BE + VS (n = 51) | FET (n = 51) | FET+VS (n = 51) | p-Value | ||
|---|---|---|---|---|---|---|
| Number (%) Mean (SD) | ||||||
| Sociodemographic | ||||||
| Sex | Female | 32 (62.75) | 29 (56.86) | 29 (56.86) | 28 (54.90) | p = 0.868 |
| Male | 19 (37.25) | 22 (43.14) | 22 (43.14) | 23 (45.10) | ||
| BMI (kg/m2) | Underweight | 1 (1.96) | 3 (5.88) | 0 (0.00) | 1 (1.96) | p = 0.266 |
| Normal body weight | 22 (43.14) | 20 (39.22) | 19 (37.25) | 20 (39.22) | ||
| Overweight | 19 (37.25) | 11 (21.57) | 18 (35.29) | 21 (41.18) | ||
| Obesity | 9 (17.65) | 17 (33.33) | 14 (27.45) | 9 (17.65) | ||
| Marital status | Married | 6 (11.76) | 6 (11.76) | 6 (11.76) | 3 (5.88) | p = 0.570 |
| Widow/widower | 21 (41.18) | 13 (25.49) | 22 (43.14) | 22 (43.14) | ||
| Divorced | 7 (13.73) | 6 (11.76) | 5 (9.80) | 8 (15.69) | ||
| Single | 17 (33.33) | 26 (50.98) | 18 (35.29) | 18 (35.29) | ||
| Education | Basic | 23 (45.10) | 16 (31.37) | 18 (35.29) | 21 (41.18) | p = 0.411 |
| Vocational | 11 (21.57) | 22 (43.14) | 17 (33.33) | 15 (29.41) | ||
| Secondary | 14 (27.45) | 13 (25.49) | 15 (29.41) | 14 (27.45) | ||
| Higher | 3 (5.88) | 0 (0.00) | 1 (1.96) | 1 (1.96) | ||
| Chronic disease | Cardiovascular | 45 (88.24) | 42 (82.35) | 47 (92.16) | 42 (82.35) | p = 0.395 |
| Musculoskeletal | 31 (60.78) | 32 (62.75) | 33 (64.71) | 28 (54.90) | p = 0.765 | |
| Neurological | 10 (19.61) | 11 (21.57) | 16 (31.37) | 9 (17.65) | p = 0.354 | |
| Pulmonary | 25 (49.02) | 24 (47.06) | 25 (49.02) | 27 (52.94) | p = 0.946 | |
| Urinary system | 6 (11.76) | 8 (15.69) | 8 (15.69) | 14 (27.45) | p = 0.183 | |
| GDS | No depression | 36 (70.59) | 33 (64.71) | 35 (68.63) | 34 (66.67) | p = 0.930 |
| Moderate depression | 15 (29.41) | 18 (35.29) | 16 (31.37) | 17 (33.33) | ||
| MMSE | No cognitive impairment | 16 (31.37) | 22 (43.14) | 18 (35.29) | 17 (33.33) | p = 0.805 |
| Cognitive impairment without dementia | 13 (25.49) | 12 (23.53) | 14 (27.45) | 17 (33.33) | ||
| Mild dementia | 22 (43.14) | 17 (33.33) | 19 (37.25) | 17 (33.33) | ||
| Age (years) | 74.37 (8.36) | 73.22 (7.33) | 74.88 (7.54) | 73.76 (7.58) | p = 0.717 | |
| Body mass (kg) | 70.59 (16.5) | 71.81 (20.74) | 71.81 (16.15) | 71.56 (16.00) | p = 0.982 | |
| Height (cm) | 163.2 (10.11) | 163.24 (11.61) | 161.82 (11.19) | 164.67 (9.02) | p = 0.603 | |
| Years in nursing home | 4.18 (3.51) | 4.43 (4.11) | 3.92 (4.66) | 4.10 (3.90) | p = 0.937 | |
| Number of drugs | 4.16 (1.50) | 4.27 (1.73) | 4.27 (1.56) | 4.25 (1.49) | p = 0.978 | |
| Number of falls | 0.71 (1.27) | 0.88 (1.14) | 0.88 (1.42) | 0.76 (1.27) | p = 0.867 | |
| Main Outcome | ||||||
| SPPB | 9.00 (2.20) | 9.25 (2.06) | 9.22 (2.09) | 9.04 (2.24) | p = 0.912 | |
| Secondary Outcomes | ||||||
| Physical Activity Assessment | Total PASE | 23.35 (13.61) | 23.91 (13.56) | 22.92 (13.69) | 23.49 (13.07) | p = 0.987 |
| Leisure time activity | 6.19 (3.68) | 6.26 (3.42) | 6.25 (3.68) | 6.33 (3.31) | p = 0.998 | |
| Household activity | 17.16 (11.72) | 17.65 (11.50) | 16.67 (11.9) | 17.16 (11.72) | p = 0.981 | |
| Functional Assessment | ADL | 5.29 (0.86) | 5.18 (0.89) | 5.25 (0.93) | 5.35 (0.84) | p = 0.782 |
| IADL | 8.61 (2.07) | 8.59 (2.5) | 8.67 (2.45) | 8.78 (2.28) | p = 0.974 | |
| Muscular Strength Assessments | HGS P (kg) | 18 (8.77) | 19.12 (9.77) | 19.96 (10.88) | 18.65 (9.04) | p = 0.773 |
| HGS L (kg) | 15.82 (9.25) | 17.99 (9.06) | 17.03 (9.03) | 17.93 (8.71) | p = 0.584 | |
| 5× STS (s) | 22.83 (10.54) | 23.87 (8.5) | 23.80 (10.90) | 23.96 (11.17) | p = 0.940 | |
| Mobility Assessment | TUG (s) | 21.07 (9.88) | 20.2 (9.87) | 21.32 (10.72) | 20.99 (10.72) | p = 0.952 |
| TUG cog (s) | 25.17 (11.58) | 24.33 (11.19) | 25.00 (11.08) | 24.88 (12.25) | p = 0.985 | |
| Gait speed (m/s) | 0.59 (0.27) | 0.62 (0.32) | 0.57 (0.27) | 0.60 (0.27) | p = 0.828 | |
| Flexibility Assessment | BS R (cm) | −32.82 (16.74) | −31.59 (16.31) | −33.57 (13.46) | −31.39 (13.40) | p = 0.868 |
| BS L (cm) | −34.18 (17.41) | −34.22 (16.79) | −34.9 (13.41) | −31.20 (18.47) | p = 0.681 | |
| CSR R (cm) | −14.06 (14.8) | −13.98 (16.04) | −11.29 (12.69) | −11.59 (13.82) | p = 0.649 | |
| CSR L (cm) | −14.59 (15.2) | −14.88 (15.21) | −11.59 (12.5) | −12.53 (13.83) | p = 0.589 | |
| Body Balance Assessment | BBS | 33.96 (13.15) | 33.10 (13.20) | 32.67 (14.40) | 33.00 (13.94) | p = 0.969 |
| Other Outcomes | ||||||
| Quality of Life Assessment | Physical Component Summary | 52.01 (15.74) | 51.61 (14.80) | 54.06 (15.44) | 54.51 (3.34) | p = 0.693 |
| Mental Health Component Summary | 58.09 (15.42) | 59.24 (19.07) | 61.48 (14.71) | 62.75 (14.89) | p = 0.456 | |
| BE | BE + VS | FET | FET+ VS | BE | BE + VS | FE | FE + VS | ||
|---|---|---|---|---|---|---|---|---|---|
| Baseline—12 weeks | Baseline—24 weeks | ||||||||
| Main Outcome | Mean change from baseline (95% CI) | ||||||||
| SPPB | 0.25 | 0.51 | 0.73 | 1.27 | −0.04 | 0.41 | 0.53 | 1.31 | |
| (0.10–0.41) * | (0.27–0.75) * | (0.47–0.98) * | (0.88–1.67) * | (−0.23–0.15) | (0.17–0.66) * | (0.28–0.78) * | (0.93–1.70) * | ||
| Secondary Outcomes | |||||||||
| Physical Activity Assessment | Total PASE | 5.50 | 4.83 | 4.02 | 5.46 | 1.44 | 5.59 | 4.14 | 6.91 |
| (4.85–6.14) * | (3.33–6.32) * | (1.78–6.27) * | (4.89–6.02) * | (0.70–2.19) * | (2.98–8.20) * | (0.94–7.34) * | (4.58–9.24) * | ||
| Leisure time activity | 5.50 | 5.42 | 5.40 | 5.50 | 1.44 | 3.73 | 2.57 | 5.77 | |
| (4.85–6.14) * | (4.84–5.99) * | (4.84–5.95) * | (4.98–6.02) * | (0.70–2.19) * | (2.77–4.68) * | (1.64–3.51) * | (4.32–7.22) * | ||
| Household activity | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 2.45 | 2.94 | 1.18 | |
| (0.00–0.00) | (0.00–0.00) | (0.00–0.00) | (0.00–0.00) | (0.00–0.00) | (0.34–4.56) * | (0.65–5.23) * | (−0.50–2.85) | ||
| Functional Assessment | ADL | 0.06 | 0.04 | 0.25 | 0.31 | −0.16 | −0.08 | 0.10 | 0.29 |
| (−0.07–0.19) | (−0.13–0.21) | (0.10–0.41) * | (0.13–0.50) * | (−0.27–−0.04) * | (−0.20–0.05) | (0.01–0.18) * | (0.09–0.50) * | ||
| IADL | 0.73 | 0.80 | 0.94 | 1.51 | 0.16 | 0.37 | 0.53 | 1.33 | |
| (0.34–1.12) * | (0.39–1.22) * | (0.52–1.36) * | (1.08–1.94) * | (0.03–0.29) * | (0.13–0.62) * | (0.24–0.82) * | (0.87–1.80) * | ||
| Muscular Strength Assessments | HGS P (kg) | 0.65 | 2.51 | 3.08 | 3.63 | −0.13 | 2.14 | 2.07 | 3.73 |
| (−0.30–1.60) | (1.18–3.83) * | (0.98–5.18) * | (2.21–5.06) * | (−1.08–0.81) | (0.86–3.42) * | (0.43–3.70) * | (2.51–4.95) * | ||
| HGS L (kg) | 0.71 | 1.77 | 2.85 | 3.27 | 0.16 | 1.10 | 2.17 | 3.41 | |
| (−0.04–1.46) | (0.63–2.91) * | (1.29–4.40) * | (1.92–4.63) * | (−0.87–1.18) | (0.02–2.19) * | (0.58–3.76) * | (2.20–4.62) * | ||
| 5× STS (s) | −2.55 | −3.98 | −4.46 | −6.36 | −0.73 | −2.86 | −3.75 | −6.30 | |
| (−3.80–−1.30) * | (−5.72–−2.23) * | (−6.20–−2.71) * | (−8.43–−4.29) * | (−1.83–0.36) | (−4.35–−1.38) * | (−5.47–−2.03) * | (−8.40–−4.19) * | ||
| Mobility Assessment | TUG (s) | −0.91 | −1.63 | −3.32 | −3.89 | 0.25 | −0.24 | −0.71 | −4.13 |
| (−1.60–−0.23) * | (−2.93–−0.33) * | (−5.16–−1.48) * | (−5.82–−1.97) * | (−0.72–1.23) | (−1.37–0.88) | (−2.04–0.62) | (−6.09–−2.18) * | ||
| TUG cog (s) | −1.29 | −1.85 | −2.79 | −3.61 | 0.08 | −0.10 | −0.70 | −3.88 | |
| (−2.42–−0.16) * | (−3.18–−0.51) * | (−3.87–−1.72) * | (−5.87–−1.36) * | (−1.30–1.47) | (−1.45–1.26) | (−2.21–0.80) | (−6.66–−1.10) * | ||
| Gait speed (m/s) | 0.07 | 0.09 | 0.09 | 0.17 | −0.02 | 0.01 | 0.04 | 0.17 | |
| (0.04–0.09) * | (0.05–0.13) * | (0.05–0.14) * | (0.13–0.21) * | (−0.04–0.01) | (−0.02–0.05) | (0.01–0.07) * | (0.13–0.22) * | ||
| Flexibility Assessment | BS R (cm) | 1.57 | 7.16 | 6.41 | 9.27 | 0.82 | 5.14 | 5.31 | 9.24 |
| (−0.74–3.88) | (4.49–9.82) * | (4.76–8.06) * | (5.94–12.61) * | (−1.45–3.10) | (2.53–7.75) * | (3.20–7.42) * | (5.82–12.65) * | ||
| BS L (cm) | 1.63 | 7.18 | 8.31 | 7.53 | 0.59 | 4.49 | 6.41 | 8.80 | |
| (−0.44–3.70) | (4.57–9.78) * | (5.67–10.96) * | (3.00–12.06) * | (−1.49–2.66) | (1.98–7.00) * | (4.24–8.58) * | (4.01–13.59) * | ||
| CSR R (cm) | 4.16 | 7.90 | 10.02 | 11.43 | 2.22 | 5.55 | 6.78 | 10.86 | |
| (2.18–6.14) * | (3.96–11.85) * | (6.94–13.10) * | (7.96–14.90) * | (0.29–4.14) * | (2.16–8.94) * | (3.93–9.64) * | (7.67–14.06) * | ||
| CSR L (cm) | 3.90 | 8.76 | 10.73 | 10.94 | 2.10 | 6.80 | 8.41 | 10.84 | |
| (1.52–6.29) * | (6.18–11.35) * | (7.75–13.70) * | (7.99–13.89) * | (0.49–3.70) * | (4.21–9.40) * | (5.60–11.23) * | (7.82–13.87) * | ||
| Body Balance Assessment | BBS | 1.18 | 4.27 | 5.82 | 7.27 | 0.20 | 2.78 | 4.39 | 7.31 |
| (−0.47–2.83) | (2.82–5.73) * | (3.65–8.00) * | (5.27–9.28) * | (−1.64–2.03) | (1.67–3.90) * | (2.29–6.49) * | (5.40–9.23) * | ||
| Other Outcomes | |||||||||
| Quality of Life Assessment | Physical Component Summary | 0.97 | 6.46 | 5.46 | 12.10 | −0.21 | 4.80 | 2.78 | 11.79 |
| (−1.94–3.87) | (3.24–9.67) * | (3.00–7.92) * | (9.33–14.86) * | (−2.22–1.80) | (2.04–7.56) * | (0.23–5.32) * | (8.64–14.95) * | ||
| Mental Health Component Summary | 2.28 | 7.88 | 5.18 | 7.28 | 0.04 | 6.34 | 4.27 | 5.01 | |
| (−1.44–5.99) | (3.30–12.45) * | (2.35–8.01) * | (3.50–11.07) * | (−2.43–2.50) | (2.04–10.63) * | (1.55–6.99) * | (1.22–8.79) * | ||
| Post hoc (Bonferroni) Analysis | ANOVA p Value | |||||||
|---|---|---|---|---|---|---|---|---|
| BE vs. BE + VS | BE vs. FET | BE vs. FET + VS | FET vs. BE + VS | BE + VS vs. FET + VS | FET vs. FET+ VS | |||
| Main Outcome | ||||||||
| SPPB | p = 0.387 | p = 0.051 | p < 0.001 * | p = 0.387 | p = 0.001 * | p = 0.022 * | p < 0.001 * | |
| Secondary Outcomes | ||||||||
| Functional Assessment | ADL | p = 1.000 | p = 0.255 | p = 0.127 | p = 0.233 | p = 0.097 | p = 1.000 | p = 0.033 * |
| IADL | p = 1.000 | p = 1.000 | p = 0.047 * | p = 1.000 | p = 0.082 | p = 0.210 | p = 0.034 * | |
| Muscular Strength Assessments | HGS P (kg) | p = 0.330 | p = 0.116 | p = 0.033 * | p = 1.000 | p = 0.871 | p = 1.000 | p = 0.033 * |
| HGS L (kg) | p = 0.657 | p = 0.075 | p = 0.022 * | p = 0.657 | p = 0.346 | p = 0.657 | p = 0.017 * | |
| 5× STS (s) | p = 0.483 | p = 0.474 | p = 0.012 * | p = 0.695 | p = 0.257 | p = 0.474 | p = 0.020 * | |
| Mobility Assessment | TUG (s) | p = 1.000 | p = 0.129 | p = 0.036 * | p = 0.349 | p = 0.144 | p = 1.000 | p = 0.018 * |
| TUG cog (s) | p = 1.000 | p = 0.655 | p = 0.191 | p = 1.000 | p = 0.509 | p = 1.000 | p = 0.144 | |
| Gait speed (m/s) | p = 0.935 | p = 0.935 | p = 0.001 * | p = 0.935 | p = 0.021 * | p = 0.027 * | p = 0.002 * | |
| Flexibility Assessment | BS R (cm) | p = 0.011 * | p = 0.032 * | p < 0.001 * | p = 0.680 | p = 0.484 | p = 0.343 | p < 0.001 * |
| BS L (cm) | p = 0.048 * | p = 0.015 * | p = 0.038 * | p = 1.000 | p = 1.000 | p = 1.000 | p = 0.010 * | |
| CSR R (cm) | p = 0.393 | p = 0.050 * | p = 0.009 * | p = 0.697 | p = 0.393 | p = 0.697 | p = 0.009 * | |
| CSR L (cm) | p = 0.050 * | p = 0.002 * | p = 0.002 * | p = 0.780 | p = 0.780 | p = 0.911 | p = 0.001 * | |
| Body Balance Assessment | BBS | p = 0.071 | p = 0.002 * | p < 0.001 * | p = 0.468 | p = 0.071 | p = 0.468 | p < 0.001 * |
| Other Outcomes | ||||||||
| Quality of Life Assessment | Physical Component Summary | p = 0.022 * | p = 0.052 | p < 0.001 * | p = 0.620 | p = 0.022 * | p = 0.006 * | p < 0.001 * |
| Mental Health Component Summary | p = 0.218 | p = 1.000 | p = 0.306 | p = 1.000 | p = 1.000 | p = 1.000 | p = 0.146 | |
| Post hoc (Bonferroni) Analysis | ANOVA p Value | |||||||
|---|---|---|---|---|---|---|---|---|
| BE vs. BE + VS | BE vs. FET | BE vs. FET + VS | FET vs. BE + VS | BE + VS vs. FET + VS | FET vs. FET + VS | |||
| Main Outcome | ||||||||
| SPPB | p = 0.044 * | p = 0.012 * | p < 0.001 * | p = 0.547 | p < 0.001 * | p < 0.001 * | p < 0.001 * | |
| Secondary Outcomes | ||||||||
| Physical Activity Assessment | Total PASE | p = 0.075 | p = 0.413 | p = 0.009 * | p = 0.787 | p = 0.787 | p = 0.413 | p = 0.010 * |
| Leisure time activity | p = 0.010 * | p = 0.245 | p <0.001 * | p = 0.245 | p = 0.019 * | p < 0.001 * | p < 0.001 * | |
| Household activity | p = 0.252 | p = 0.115 | p = 0.922 | p = 0.922 | p = 0.922 | p = 0.632 | p = 0.083 | |
| Functional Assessment | ADL | p = 0.427 | p = 0.042 * | p <0.001 * | p = 0.150 | p = 0.001 * | p = 0.144 | p < 0.001 * |
| IADL | p = 0.640 | p = 0.260 | p <0.001 * | p = 0.640 | p<0.001 * | p = 0.001 * | p < 0.001 * | |
| Muscular Strength Assessments | HGS P (kg) | p = 0.066 | p = 0.066 | p <0.001 * | p = 0.933 | p = 0.208 | p = 0.208 | p = 0.001 * |
| HGS L (kg) | p = 0.479 | p = 0.092 | p = 0.002 * | p = 0.479 | p = 0.047 * | p = 0.479 | p = 0.002 * | |
| 5× STS (s) | p = 0.134 | p = 0.039 * | p < 0.001 * | p = 0.444 | p = 0.017 * | p = 0.087 | p < 0.001 * | |
| Mobility Assessment | TUG (s) | p = 1.000 | p = 0.989 | p < 0.001 * | p = 1.000 | p = 0.001 * | p = 0.002 * | p < 0.001 * |
| TUG cog (s) | p = 1.000 | p = 1.000 | p = 0.016 * | p = 1.000 | p = 0.021 * | p = 0.063 | p = 0.008 * | |
| Gait speed (m/s) | p = 0.366 | p = 0.045 * | p < 0.001 * | p = 0.366 | p < 0.001 * | p <0.001 * | p < 0.001 * | |
| Flexibility Assessment | BS R (cm) | p = 0.087 | p = 0.085 | p< 0.001 * | p = 0.925 | p = 0.088 | p = 0.088 | p < 0.001 * |
| BS L (cm) | p = 0.224 | p = 0.040 * | p = 0.001 * | p = 0.546 | p = 0.196 | p = 0.546 | p = 0.002 * | |
| CSR R (cm) | p = 0.208 | p = 0.105 | p < 0.001 * | p = 0.546 | p = 0.049 * | p = 0.141 | p = 0.001 * | |
| CSR L (cm) | p = 0.04 * | p = 0.003 * | p < 0.001 * | p = 0.375 | p = 0.080 | p = 0.360 | p < 0.001 * | |
| Body Balance Assessment | BBS | p = 0.080 | p = 0.004 * | p < 0.001 * | p = 0.201 | p = 0.002 * | p = 0.062 | p <0.001 * |
| Other Outcomes | ||||||||
| Quality of Life Assessment | Physical Component Summary | p = 0.024 * | p = 0.222 | p < 0.001 * | p = 0.280 | p = 0.001 * | p <0.001 * | p <0.001 * |
| Mental Health Component Summary | p = 0.055 | p = 0.313 | p = 0.195 | p = 1.000 | p = 1.000 | p = 1.000 | p = 0.054 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiśniowska-Szurlej, A.; Ćwirlej-Sozańska, A.; Wołoszyn, N.; Sozański, B.; Wilmowska-Pietruszyńska, A. Effects of Physical Exercises and Verbal Stimulation on the Functional Efficiency and Use of Free Time in an Older Population under Institutional Care: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 477. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9020477
Wiśniowska-Szurlej A, Ćwirlej-Sozańska A, Wołoszyn N, Sozański B, Wilmowska-Pietruszyńska A. Effects of Physical Exercises and Verbal Stimulation on the Functional Efficiency and Use of Free Time in an Older Population under Institutional Care: A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(2):477. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9020477
Chicago/Turabian StyleWiśniowska-Szurlej, Agnieszka, Agnieszka Ćwirlej-Sozańska, Natalia Wołoszyn, Bernard Sozański, and Anna Wilmowska-Pietruszyńska. 2020. "Effects of Physical Exercises and Verbal Stimulation on the Functional Efficiency and Use of Free Time in an Older Population under Institutional Care: A Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 2: 477. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9020477