Serum Follicle-Stimulating Hormone Levels are Associated with Cardiometabolic Risk Factors in Post-Menopausal Korean Women

Abstract
:1. Introduction
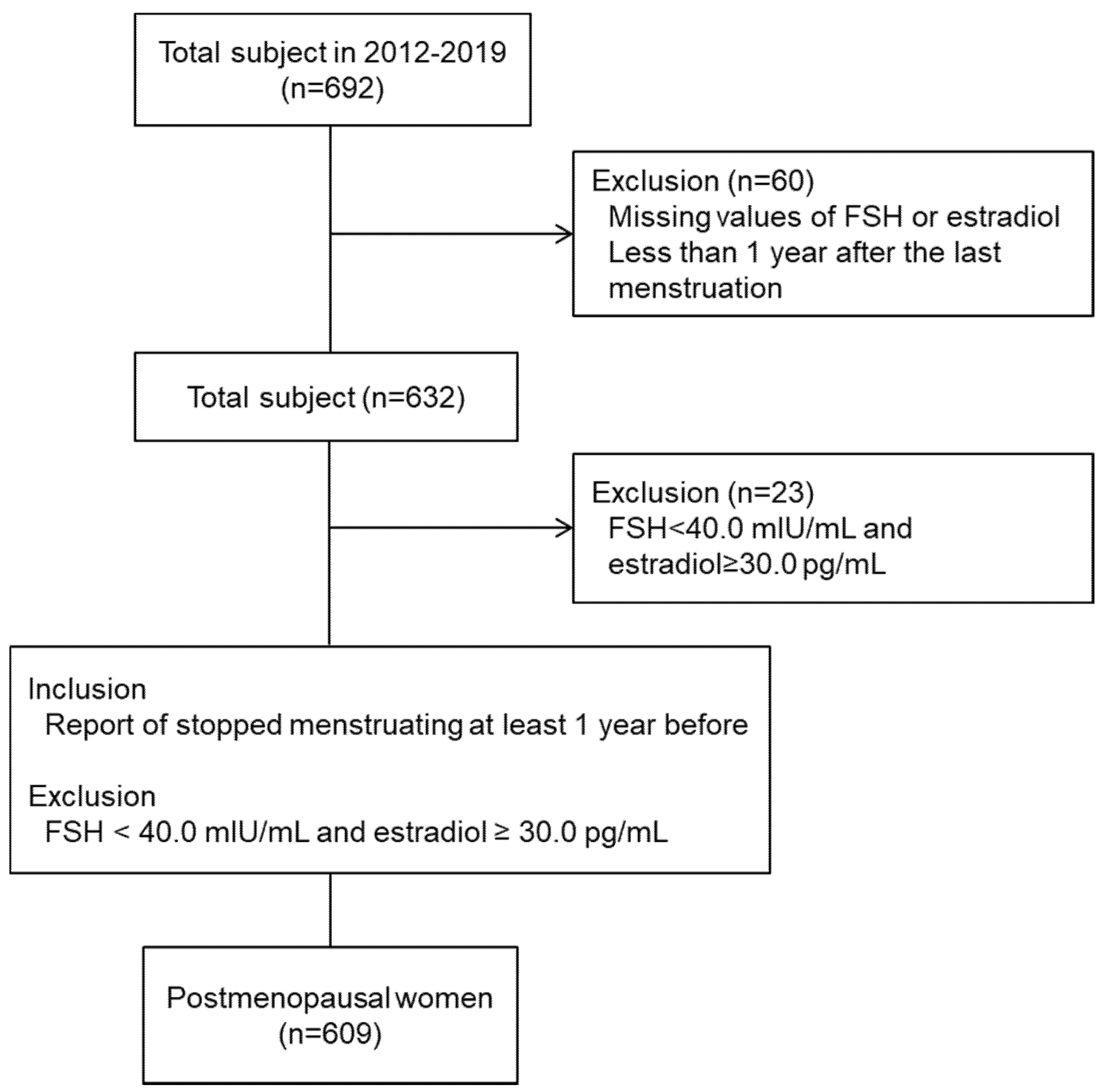
2. Subjects and Methods
2.1. Data Collection
2.2. Biochemical and Hormone Analyses
2.3. Lifestyle Questionnaires
2.4. Definition of Variables
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Participants
3.2. Diet and Physical Activity of the Study Participants
3.3. Cardiometabolic Risk Factors of the Study Participants
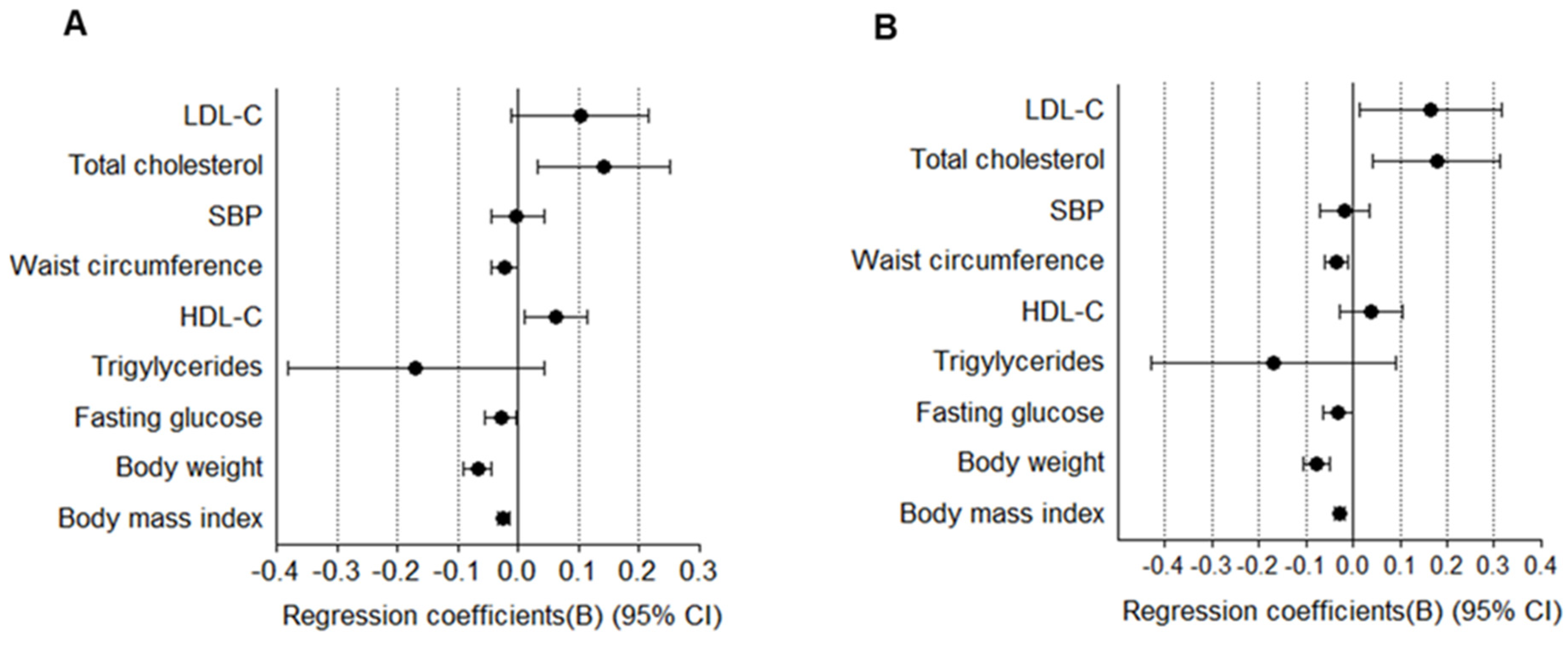
3.4. Association between Follicle-Stimulating Hormone (FSH) Levels and Cardiometabolic Risk Factors
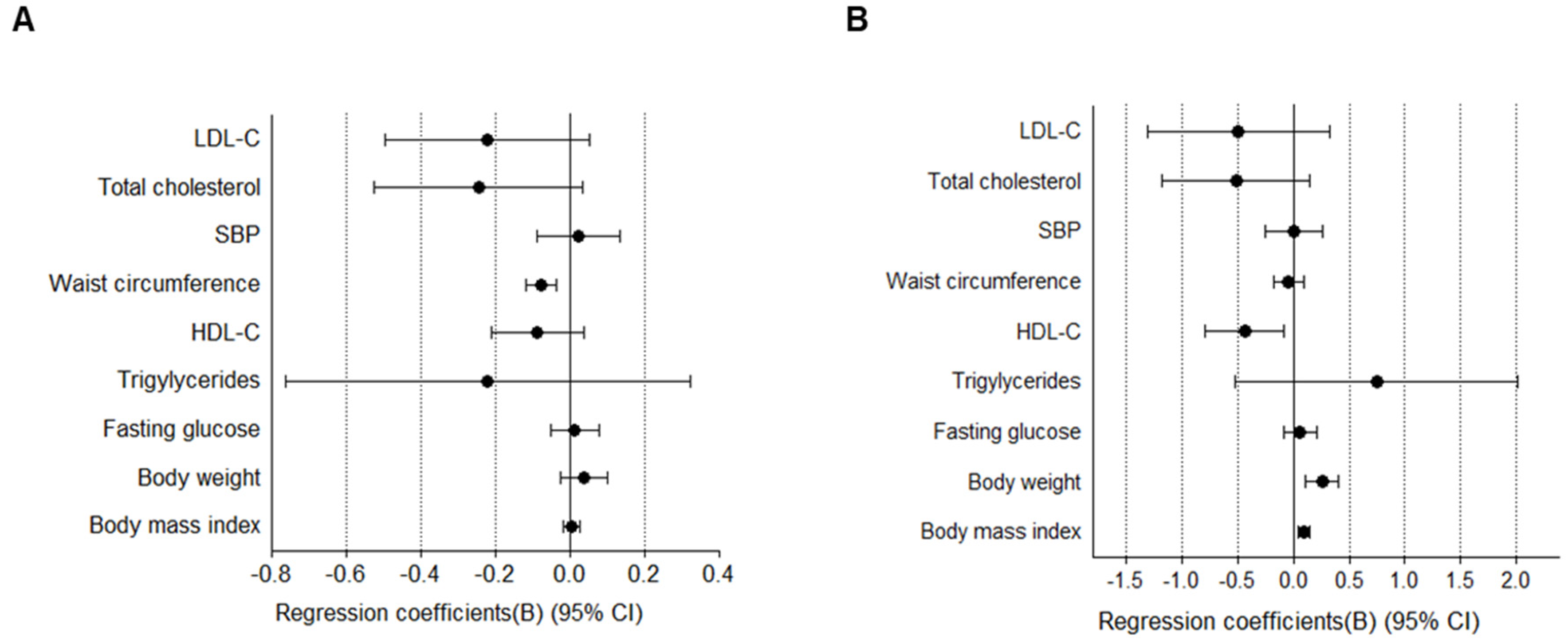
3.5. Association between Estradiol Levels and Cardiometabolic Risk Factors
3.6. Association between FSH Levels and Metabolic Syndrome (MetS)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Despres, J.P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef]
- Eckel, R.H.; Cornier, M.A. Update on the NCEP ATP-III emerging cardiometabolic risk factors. BMC Med. 2014, 12, 115. [Google Scholar] [CrossRef] [Green Version]
- Atsma, F.; Bartelink, M.L.; Grobbee, D.E.; van der Schouw, Y.T. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: A meta-analysis. Menopause 2006, 13, 265–279. [Google Scholar] [CrossRef]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European Guidelines on Cardiovascular Disease Prevention in Clinical Practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar] [PubMed] [Green Version]
- Hallajzadeh, J.; Khoramdad, M.; Izadi, N.; Karamzad, N.; Almasi-Hashiani, A.; Ayubi, E.; Qorbani, M.; Pakzad, R.; Hasanzadeh, A.; Sullman, M.J.M.; et al. Metabolic syndrome and its components in premenopausal and postmenopausal women: A comprehensive systematic review and meta-analysis on observational studies. Menopause 2018, 25, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Marchi, R.; Dell’Agnolo, C.M.; Lopes, T.C.R.; Gravena, A.A.F.; Demitto, M.O.; Brischiliari, S.C.R.; Borghesan, D.H.P.; Carvalho, M.D.B.; Pelloso, S.M. Prevalence of metabolic syndrome in pre- and postmenopausal women. Arch. Endocrinol. Metab. 2017, 61, 160–166. [Google Scholar] [CrossRef]
- Banks, A.D. Women and heart disease: Missed opportunities. J. Midwifery Womens Health 2008, 53, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, M.E.; Manson, J.E.; Buring, J.E.; Cook, N.R.; Seely, E.W.; Ridker, P.M.; Rexrode, K.M. Low sex hormone-binding globulin is associated with the metabolic syndrome in postmenopausal women. Metabolism 2006, 55, 1473–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crandall, C.J.; Barrett-Connor, E. Endogenous sex steroid levels and cardiovascular disease in relation to the menopause: A systematic review. Endocrinol. Metab. Clin. N. Am. 2013, 42, 227–253. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R. Gaps, limitations and new insights on endogenous estrogen and follicle stimulating hormone as related to risk of cardiovascular disease in women traversing the menopause: A narrative review. Maturitas 2017, 104, 44–53. [Google Scholar] [CrossRef]
- Scarabin-Carre, V.; Canonico, M.; Brailly-Tabard, S.; Trabado, S.; Ducimetiere, P.; Giroud, M.; Ryan, J.; Helmer, C.; Plu-Bureau, G.; Guiochon-Mantel, A.; et al. High level of plasma estradiol as a new predictor of ischemic arterial disease in older postmenopausal women: The three-city cohort study. J. Am. Heart Assoc. 2012, 1, e001388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.S.; Yaffe, K.; Lui, L.Y.; Cauley, J.; Taylor, B.; Browner, W.; Cummings, S.; Study of Osteoporotic Fractures Group. Prospective study of endogenous circulating estradiol and risk of stroke in older women. Arch. Neurol. 2010, 67, 195–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, E.L.; Song, Y.; Manson, J.E.; Rifai, N.; Buring, J.E.; Liu, S. Plasma sex steroid hormones and risk of developing type 2 diabetes in women: A prospective study. Diabetologia 2007, 50, 2076–2084. [Google Scholar] [CrossRef] [PubMed]
- Ding, E.L.; Song, Y.; Malik, V.S.; Liu, S. Sex differences of endogenous sex hormones and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2006, 295, 1288–1299. [Google Scholar] [CrossRef]
- Wang, N.; Kuang, L.; Han, B.; Li, Q.; Chen, Y.; Zhu, C.; Chen, Y.; Xia, F.; Cang, Z.; Zhu, C.; et al. Follicle-stimulating hormone associates with prediabetes and diabetes in postmenopausal women. Acta Diabetol. 2016, 53, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanska, A.; Ponikowska, I.; Cwiklinska-Jurkowska, M.; Sypniewska, G. Association of FSH with metabolic syndrome in postmenopausal women: A comparison with CRP, adiponectin and leptin. Biomark. Med. 2014, 8, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Stefanska, A.; Sypniewska, G.; Ponikowska, I.; Cwiklinska-Jurkowska, M. Association of follicle-stimulating hormone and sex hormone binding globulin with the metabolic syndrome in postmenopausal women. Clin. Biochem. 2012, 45, 703–706. [Google Scholar] [CrossRef]
- Wang, N.; Shao, H.; Chen, Y.; Xia, F.; Chi, C.; Li, Q.; Han, B.; Teng, Y.; Lu, Y. Follicle-stimulating hormone, its association with cardiometabolic risk factors, and 10-year risk of cardiovascular disease in postmenopausal women. J. Am. Heart Assoc. 2017, 6, e005918. [Google Scholar] [CrossRef]
- Harlow, S.D.; Gass, M.; Hall, J.E.; Lobo, R.; Maki, P.; Rebar, R.W.; Sherman, S.; Sluss, P.M.; de Villiers, T.J.; STRAW + 10 Collaborative Group. Executive summary of the Stages of Reproductive Aging Workshop + 10: Addressing the unfinished agenda of staging reproductive aging. J. Clin. Endocrinol. Metab. 2012, 97, 1159–1168. [Google Scholar] [CrossRef]
- World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide; World Health Organization: Geneva, The Netherlands, 2012. [Google Scholar]
- Expert Panel on Detection, Evaluation; Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Anuurad, E.; Shiwaku, K.; Nogi, A.; Kitajima, K.; Enkhmaa, B.; Shimono, K.; Yamane, Y. The new BMI criteria for asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. J. Occup. Health 2003, 45, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Enkhmaa, B.; Shiwaku, K.; Anuurad, E.; Nogi, A.; Kitajima, K.; Yamasaki, M.; Oyunsuren, T.; Yamane, Y. Prevalence of the metabolic syndrome using the Third Report of the National Cholesterol Educational Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) and the Modified ATP III Definitions for Japanese and Mongolians. Clin. Chim. Acta 2005, 352, 105–113. [Google Scholar] [PubMed]
- Duggal, J.; Singh, S.; Barsano, C.P.; Arora, R. Cardiovascular risk with subclinical hyperthyroidism and hypothyroidism: Pathophysiology and management. J. Cardiometab. Syndr. 2007, 2, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.Y.; Ima-Nirwana, S.; Mohamed, I.N.; Aminuddin, A.; Johari, M.H.; Ngah, W.Z. The relationships between thyroid hormones and thyroid-stimulating hormone with lipid profile in euthyroid men. Int. J. Med. Sci. 2014, 11, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chon, S.J.; Heo, J.Y.; Yun, B.H.; Jung, Y.S.; Seo, S.K. Serum thyroid stimulating hormone levels are associated with the presence of coronary atherosclerosis in healthy postmenopausal women. J. Menopausal. Med. 2016, 22, 146–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics--2012 update: A report from the American Heart Association. Circulation 2012, 125, e2–e220. [Google Scholar]
- Barrett-Connor, E. Clinical review 162: Cardiovascular endocrinology 3: An epidemiologist looks at hormones and heart disease in women. J. Clin. Endocrinol. Metab. 2003, 88, 4031–4042. [Google Scholar] [CrossRef]
- Gordon, T.; Kannel, W.B.; Hjortland, M.C.; McNamara, P.M. Menopause and coronary heart disease. The Framingham Study. Ann. Intern. Med. 1978, 89, 157–161. [Google Scholar] [CrossRef]
- Colditz, G.A.; Willett, W.C.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Hennekens, C.H. Menopause and the risk of coronary heart disease in women. N. Engl. J. Med. 1987, 316, 1105–1110. [Google Scholar] [CrossRef]
- Tepper, P.G.; Randolph, J.F., Jr.; McConnell, D.S.; Crawford, S.L.; El Khoudary, S.R.; Joffe, H.; Gold, E.B.; Zheng, H.; Bromberger, J.T.; Sutton-Tyrrell, K. Trajectory clustering of estradiol and follicle-stimulating hormone during the menopausal transition among women in the Study of Women’s Health Across the Nation (SWAN). J. Clin. Endocrinol. Metab. 2012, 97, 2872–2880. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Santoro, N.; Chen, H.Y.; Tepper, P.G.; Brooks, M.M.; Thurston, R.C.; Janssen, I.; Harlow, S.D.; Barinas-Mitchell, E.; Selzer, F.; et al. Trajectories of estradiol and follicle-stimulating hormone over the menopause transition and early markers of atherosclerosis after menopause. Eur. J. Prev. Cardiol. 2016, 23, 694–703. [Google Scholar] [CrossRef] [PubMed]
- Munir, J.A.; Wu, H.; Bauer, K.; Bindeman, J.; Byrd, C.; Feuerstein, I.M.; Villines, T.C.; Taylor, A.J. The perimenopausal atherosclerosis transition: Relationships between calcified and noncalcified coronary, aortic, and carotid atherosclerosis and risk factors and hormone levels. Menopause 2012, 19, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.W.; Sammel, M.D.; Lin, H.; Gracia, C.R. Obesity and reproductive hormone levels in the transition to menopause. Menopause 2010, 17, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Randolph, J.F., Jr.; Zheng, H.; Sowers, M.R.; Crandall, C.; Crawford, S.; Gold, E.B.; Vuga, M. Change in follicle-stimulating hormone and estradiol across the menopausal transition: Effect of age at the final menstrual period. J. Clin. Endocrinol. Metab. 2011, 96, 746–754. [Google Scholar] [CrossRef]
- Kim, C.; Randolph, J.F.; Golden, S.H.; Labrie, F.; Kong, S.; Nan, B.; Barrett-Connor, E. Weight loss increases follicle stimulating hormone in overweight postmenopausal women. Obesity (Silver Spring) 2015, 23, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Chu, C.; Xu, B.; Huang, W. A study on expression of FSH and its effects on the secretion of insulin and glucagon in rat pancreas. Tissue Cell 2010, 42, 370–375. [Google Scholar] [CrossRef]
- Ulloa-Aguirre, A.; Zarinan, T. The Follitropin receptor: Matching structure and function. Mol. Pharmacol. 2016, 90, 596–608. [Google Scholar] [CrossRef]
- Stilley, J.A.; Guan, R.; Duffy, D.M.; Segaloff, D.L. Signaling through FSH receptors on human umbilical vein endothelial cells promotes angiogenesis. J. Clin. Endocrinol. Metab. 2014, 99, E813–E820. [Google Scholar] [CrossRef]
- Guo, Y.; Zhao, M.; Bo, T.; Ma, S.; Yuan, Z.; Chen, W.; He, Z.; Hou, X.; Liu, J.; Zhang, Z.; et al. Blocking FSH inhibits hepatic cholesterol biosynthesis and reduces serum cholesterol. Cell Res. 2019, 29, 151–166. [Google Scholar] [CrossRef]
- Christenson, L.K.; Stouffer, R.L. Follicle-stimulating hormone and luteinizing hormone/chorionic gonadotropin stimulation of vascular endothelial growth factor production by macaque granulosa cells from pre- and periovulatory follicles. J. Clin. Endocrinol. Metab. 1997, 82, 2135–2142. [Google Scholar] [CrossRef]
- Huang, Y.; Hua, K.; Zhou, X.; Jin, H.; Chen, X.; Lu, X.; Yu, Y.; Zha, X.; Feng, Y. Activation of the PI3K/AKT pathway mediates FSH-stimulated VEGF expression in ovarian serous cystadenocarcinoma. Cell Res. 2008, 18, 780–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, G.S.; Sosin, M.D.; Patel, J.V.; Grindulis, K.A.; Khattak, F.H.; Davis, R.C.; Lip, G.Y. Plasma indices of angiogenesis in rheumatoid disease: Relationship to cardiovascular risk factors and cardiac function. Int. J. Cardiol. 2010, 145, e105–e108. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Wang, E.S.; Xing, L.L.; Shi, S.; Qu, F.; Zhang, D.; Li, J.Y.; Shu, J.; Meng, Y.; Sheng, J.Z.; et al. Follicle-stimulating hormone induces postmenopausal dyslipidemia through inhibiting hepatic cholesterol metabolism. J. Clin. Endocrinol. Metab. 2016, 101, 254–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, H.; Zhao, G.; Liu, R.; Zheng, M.; Chen, J.; Wen, J. FSH stimulates lipid biosynthesis in chicken adipose tissue by upregulating the expression of its receptor FSHR. J. Lipid Res. 2012, 53, 909–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.M.; Chan, H.C.; Ding, G.L.; Cai, J.; Song, Y.; Wang, T.T.; Zhang, D.; Chen, H.; Yu, M.K.; Wu, Y.T.; et al. FSH regulates fat accumulation and redistribution in aging through the Galphai/Ca2+/CREB pathway. Aging Cell 2015, 14, 409–420. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Research on the menopause in the 1990s: Report of a WHO Scientific Group. World Health Organ. Tech. Rep. Ser. 1996, 866, 1–107. [Google Scholar]
- Politi, M.C.; Schleinitz, M.D.; Col, N.F. Revisiting the duration of vasomotor symptoms of menopause: A meta-analysis. J. Gen. Intern. Med. 2008, 23, 1507–1513. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Follicle-Stimulating Hormone (mIU/mL) | p for Trend 1 | p2 | Adj. p3 | ||||
|---|---|---|---|---|---|---|---|---|
| Q1 (≤62.20) | Q2 (62.21~76.87) | Q3 (76.88~94.00) | Q4 (≥94.01) | |||||
| Number | 153 | 152 | 152 | 152 | - | - | - | |
| Age (years) | 53.86 ± 2.99a | 53.80 ± 3.10ab | 53.41 ± 2.84ab | 52.96 ± 2.77b | 0.0014 | 0.0277 | 0.0104 | |
| Menopausal age (years) | 50.81 ± 2.99 | 50.00 ± 3.40 | 50.23 ± 2.99 | 49.93 ± 3.32 | 0.2500 | 0.4272 | 0.6150 | |
| Alcohol | (N, %) | 48(37.50%) | 57(40.14%) | 52(37.68%) | 55(37.73%) | 0.9574 | 0.9679 | - |
| (g/week) | 16.01 ± 14.22 | 20.98 ± 25.58 | 18.23 ± 22.73 | 20.08 ± 24.89 | 0.6350 | 0.6904 | 0.7788 | |
| Blood pressure–lowering drugs (N, %) | 5(3.27%) | 3(1.97%) | 7(4.61%) | 6(3.95%) | 0.4808 | 0.6297 | - | |
| KI | 35.73 ± 6.68a | 33.77 ± 7.52ab | 33.98 ± 7.16ab | 33.38 ± 7.13b | 0.0157 | 0.0436 | 0.0503 | |
| MRS | 33.16 ± 7.80 | 31.54 ± 8.29 | 32.20 ± 7.60 | 30.66 ± 8.19 | 0.1252 | 0.2088 | 0.3533 | |
| Estradiol (pg/mL) | 10.29 ± 15.64a | 7.02 ± 6.66b | 6.63 ± 4.44b | 7.99 ± 5.98ab | 0.9445 | 0.0117 † | 0.0010 | |
| Height (cm) | 158.01 ± 5.00 | 157.53 ± 4.71 | 156.96 ± 4.86 | 156.97 ± 5.58 | 0.0863 | 0.2066 | 0.9461 | |
| Weight (kg) | 61.01 ± 7.12a | 58.50 ± 7.96b | 56.93 ± 7.22b | 56.83 ± 6.28b | <.0001 | <.0001 | <.0001 | |
| Physical activity (METs/week) | 2438.75 ± 2581.00 | 2184.47 ± 2271.13 | 2768.22 ± 2915.91 | 2778.69 ± 3972.33 | 0.7957 | 0.3987 | 0.4659 | |
| BMI (kg/m2) | 24.45 ± 2.73a | 23.56 ± 2.90b | 23.08 ± 2.46b | 23.08 ± 2.39b | <.0001 | <.0001 | <.0001 | |
| WC (cm) | 85.63 ± 7.79a | 83.26 ± 8.40ab | 82.48 ± 7.16ab | 81.50 ± 6.76b | 0.0010 | 0.0067 | 0.2779 | |
| HC (cm) | 94.24 ± 5.61 | 92.90 ± 3.59 | 92.37 ± 4.23 | 92.53 ± 3.71 | 0.1547 | 0.3051 | 0.8876 | |
| WHR | 0.89 ± 0.05 | 0.88 ± 0.06 | 0.87 ± 0.06 | 0.88 ± 0.05 | 0.3693 | 0.6218 | 0.7451 | |
| SBP (mmHg) | 122.17 ± 13.02a | 118.49 ± 13.11ab | 117.58 ± 12.47b | 119.47 ± 14.25ab | 0.0488 | 0.0167 | 0.2051 | |
| DBP (mmHg) | 77.79 ± 10.46 | 77.67 ± 9.91 | 76.22 ± 10.31 | 77.68 ± 10.17 | 0.4627 | 0.4867 | 0.4921 | |
| Pulse (BPM) | 70.61 ± 8.66 | 70.58 ± 8.66 | 71.30 ± 8.58 | 71.41 ± 7.83 | 0.2007 | 0.7400 | 0.9339 | |
| Glucose (mg/dL) | 89.24 ± 8.06a | 88.39 ± 8.21ab | 88.20 ± 7.77ab | 86.09 ± 7.29b | 0.0004 | 0.0043 | 0.0386 | |
| TC (mg/dL) | 197.32 ± 32.81b | 206.68 ± 32.38ab | 201.93 ± 31.89ab | 209.23 ± 31.50a | 0.0105 | 0.0068 | 0.0042 | |
| TG (mg/dL) | 129.44 ± 80.70b | 110.77 ± 54.57ab | 111.88 ± 58.32ab | 110.41 ± 51.93b | 0.0390 | 0.0191 | 0.0740 | |
| HDL-C (mg/dL) | 52.85 ± 12.14a | 59.08 ± 14.43a | 56.55 ± 13.58ab | 58.65 ± 14.04a | 0.0108 | 0.0009 | 0.0098 | |
| LDL-C (mg/dL) | 118.45 ± 28.16b | 128.56 ± 31.45ab | 123.02 ± 31.69ab | 128.92 ± 28.70a | 0.0367 | 0.0166 | 0.0141 | |
| TC/HDL-C | 3.89 ± 0.91 | 3.73 ± 0.99 | 3.76 ± 0.92 | 3.73 ± 0.93 | 0.2410 | 0.4858 | 0.8169 | |
| LDL-C/HDL-C | 2.35 ± 0.75 | 2.32 ± 0.82 | 2.29 ± 0.77 | 2.33 ± 0.76 | 0.8302 | 0.9406 | 0.9696 | |
| TG/HDL-C | 2.69 ± 1.80a | 2.09 ± 1.39b | 2.20 ± 1.52ab | 2.06 ± 1.38b | 0.0039 | 0.0033 | 0.0213 | |
| Variables | Follicle-Stimulating Hormone (mIU/mL) | p for Trend 1 | p2 | Adj. P3 | |||
|---|---|---|---|---|---|---|---|
| Q1 (≤62.20) | Q2 (62.21~76.87) | Q3 (76.88~94.00) | Q4 (≥94.01) | ||||
| WBC (4.8–10.8 × 103/μL) | 5.12 ± 1.22 | 4.83 ± 1.20 | 4.99 ± 1.16 | 4.87 ± 1.13 | 0.2567 | 0.1164 | 0.2533 |
| RBC (4.2–5.4 × 1003/μL) | 4.38 ± 0.29a | 4.28 ± 0.31b | 4.36 ± 0.32ab | 4.33 ± 0.29ab | 0.5826 | 0.0417 | 0.0629 |
| Hemoglobin (12–16 g/dL) | 13.42 ± 0.82a | 13.16 ± 0.87b | 13.33 ± 0.87ab | 13.23 ± 0.76ab | 0.1552 | 0.0373 | 0.0866 |
| Hematocrit (37–47%) | 39.84 ± 2.16 | 39.26 ± 2.58 | 39.84 ± 2.54 | 39.39 ± 2.06 | 0.3519 | 0.0664 † | 0.0804 |
| Platelet (130–450 × 103/μL) | 249.57 ± 53.80 | 239.80 ± 42.60 | 238.46 ± 49.55 | 245.80 ± 55.65 | 0.6414 | 0.1864 | 0.3450 |
| ALP (45–129 IU/L) | 74.57 ± 18.10 | 74.71 ± 16.13 | 72.43 ± 15.68 | 76.39 ± 17.94 | 0.6073 | 0.2460 | 0.1460 |
| γ-GTP (8–48 IU/L) | 19.95 ± 14.17 | 18.20 ± 12.04 | 19.28 ± 13.67 | 16.84 ± 8.55 | 0.2659 | 0.1341 | 0.2910 |
| AST (12–33 IU/L) | 23.52 ± 5.79 | 23.12 ± 5.64 | 23.45 ± 5.39 | 22.59 ± 4.67 | 0.3413 | 0.4187 | 0.6417 |
| ALT (5–35 IU/L) | 22.68 ± 10.43 | 21.03 ± 8.26 | 21.80 ± 8.69 | 20.36 ± 6.65 | 0.1321 | 0.1042 | 0.3561 |
| Total bilirubin (0.2–1.2 mg/dL) | 0.81 ± 0.30 | 0.84 ± 0.27 | 0.81 ± 0.23 | 0.82 ± 0.26 | 0.6695 | 0.7025 | 0.7281 |
| Total protein (6.7–8.3 g/dL) | 7.35 ± 0.34 | 7.28 ± 0.31 | 7.29 ± 0.35 | 7.29 ± 0.38 | 0.2343 | 0.6317 | 0.6231 |
| Albumin (3.5–5.3 g/dL) | 4.38 ± 0.19 | 4.37 ± 0.18 | 4.39 ± 0.18 | 4.38 ± 0.20 | 0.7952 | 0.3864 | 0.4043 |
| BUN (8–23 mg/dL) | 14.61 ± 3.93 | 14.54 ± 3.25 | 14.98 ± 3.51 | 14.55 ± 3.28 | 0.4111 | 0.6553 | 0.6190 |
| eGFR (90–120 mL/min/1.73 m2) | 114.15 ± 19.67 | 112.44 ± 23.43 | 111.44 ± 22.26 | 110.08 ± 18.76 | 0.1079 | 0.3909 | 0.0970 |
| Uric acid (2.5–6.3 mg/dL) | 4.56 ± 1.13 | 4.36 ± 0.92 | 4.56 ± 0.80 | 4.37 ± 0.99 | 0.8558 | 0.5556 | 0.4102 |
| Total calcium (8.4–10.2 mg/dL) | 9.46 ± 0.33 | 9.55 ± 0.36 | 9.57 ± 0.34 | 9.52 ± 0.32 | 0.2884 | 0.1458 | 0.0689 |
| TSH (0.55–4.78 μIU/mL) | 1.80 ± 0.93 | 1.81 ± 1.01 | 1.94 ± 0.85 | 1.97 ± 1.02 | 0.0514 | 0.4016 | 0.3014 |
| hs-CRP (~5 mg/L) | 0.92 ± 3.63 | 0.50 ± 1.31 | 0.41 ± 0.85 | 1.00 ± 2.46 | 0.2563 | 0.4845 | 0.5692 |
| Urine specific gravity (1.005–1.030) | 1.02 ± 0.01 | 1.02 ± 0.01 | 1.02 ± 0.00 | 1.02 ± 0.01 | 0.7690 | 0.1507 | 0.1298 |
| Urine pH (4.5–9.0) | 6.05 ± 0.85 | 6.16 ± 0.86 | 6.18 ± 0.85 | 6.14 ± 0.86 | 0.2979 | 0.5405 | 0.6468 |
| Variables | Follicle-Stimulating Hormone (mIU/mL) | p for Trend 1 | P2 | Adj. P3 | |||
|---|---|---|---|---|---|---|---|
| Q1 (≤62.20) | Q2 (62.21~76.87) | Q3 (76.88~94.00) | Q4 (≥94.01) | ||||
| MetS (N, %) | 29(33.33%) | 17(18.68%) | 19(24.68%) | 11(15.71%) | 0.0281 | 0.0402 | - |
| Number of the component of MetS | 2.01 ± 1.06a | 1.45 ± 1.20b | 1.51 ± 1.15b | 1.41 ± 1.07b | 0.0015 | 0.0015 | 0.0215 |
| Variables | FSH | Unstandardized Coefficients (B) | Odds Ratio | p-Value | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Metabolic syndrome | Q1 | 0.872 | 2.391 | 0.039 | 1.047 | 5.459 |
| Q2 | 0.228 | 1.256 | 0.606 | 0.528 | 2.991 | |
| Q3 | 0.710 | 2.035 | 0.109 | 0.853 | 4.853 | |
| Q4 | 1.000 | |||||
| Variables | FSH | Unstandardized Coefficients (B) | Odds Ratio | p-Value | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Hypertension | Q1 | 0.436 | 1.546 | 0.123 | 0.888 | 2.690 |
| Q2 | 0.075 | 1.078 | 0.802 | 0.601 | 1.931 | |
| Q3 | 0.057 | 1.058 | 0.849 | 0.591 | 1.896 | |
| Q4 | 1.000 | |||||
| WC (central obesity) | Q1 | 0.958 | 2.606 | 0.024 | 1.136 | 5.975 |
| Q2 | 0.215 | 1.240 | 0.571 | 0.589 | 2.609 | |
| Q3 | 0.175 | 1.191 | 0.650 | 0.560 | 2.535 | |
| Q4 | 1.000 | |||||
| HDL-C | Q1 | 0.466 | 1.593 | 0.095 | 0.921 | 2.754 |
| Q2 | −0.185 | 0.832 | 0.537 | 0.463 | 1.494 | |
| Q3 | 0.160 | 1.173 | 0.578 | 0.668 | 2.060 | |
| Q4 | 1.000 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, E.-S.; Choi, E.-K.; Park, B.-H.; Chae, S.-W. Serum Follicle-Stimulating Hormone Levels are Associated with Cardiometabolic Risk Factors in Post-Menopausal Korean Women. J. Clin. Med. 2020, 9, 1161. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041161
Jung E-S, Choi E-K, Park B-H, Chae S-W. Serum Follicle-Stimulating Hormone Levels are Associated with Cardiometabolic Risk Factors in Post-Menopausal Korean Women. Journal of Clinical Medicine. 2020; 9(4):1161. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041161
Chicago/Turabian StyleJung, Eun-Soo, Eun-Kyung Choi, Byung-Hyun Park, and Soo-Wan Chae. 2020. "Serum Follicle-Stimulating Hormone Levels are Associated with Cardiometabolic Risk Factors in Post-Menopausal Korean Women" Journal of Clinical Medicine 9, no. 4: 1161. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041161