The Integration of qSOFA with Clinical Variables and Serum Biomarkers Improves the Prognostic Value of qSOFA Alone in Patients with Suspected or Confirmed Sepsis at ED Admission

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Biomarker Measurements
2.2. Statistical Analysis
3. Results
3.1. Group 1: Undifferentiated Patients with Suspected Sepsis at ED Admission.
3.2. Group 2: Patients with Suspected Sepsis at ED Admission who Received a Definitive Diagnosis of Sepsis at the end of Clinical Work-Up.
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Serafim, R.; Gomes, J.A.; Salluh, J.; Póvoa, P. A Comparison of the Quick-SOFA and Systemic Inflammatory Response Syndrome Criteria for the Diagnosis of Sepsis and Prediction of Mortality: A Systematic Review and Meta-Analysis. Chest 2018, 153, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.; Snyder, A.; Han, X.; Sokol, S.; Pettit, N.; Howell, M.D.; Edelson, D.P. Quick Sepsis-related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores for Detecting Clinical Deterioration in Infected Patients outside the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2017, 195, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moskowitz, A.; Patel, P.V.; Grossestreuer, A.V.; Chase, M.; Shapiro, N.I.; Berg, K.; Cocchi, M.N.; Holmberg, M.J.; Donnino, M.W. Quick Sequential Organ Failure Assessment and Systemic Inflammatory Response Syndrome Criteria as Predictors of Critical Care Intervention Among Patients With Suspected Infection. Crit. Care Med. 2017, 45, 1813–1819. [Google Scholar] [CrossRef]
- Yu, H.; Nie, L.; Liu, A.; Wu, K.; Hsein, Y.-C.; Yen, D.W.; Lee, M.-T.G.; Lee, C.-C. Combining procalcitonin with the qSOFA and sepsis mortality prediction. Med. Baltimore 2019, 98, e15981. [Google Scholar] [CrossRef]
- Saeed, K.; Wilson, D.C.; Bloos, F.; Schuetz, P.; van der Does, Y.; Melander, O.; Hausfater, P.; Legramante, J.M.; Claessens, Y.E.; Amin, D.; et al. The early identification of disease progression in patients with suspected infection presenting to the emergency department: A multi-centre derivation and validation study. Crit Care 2019, 23, 40. [Google Scholar] [CrossRef] [Green Version]
- Henning, D.J.; Puskarich, M.A.; Self, W.H.; Howell, M.D.; Donnino, M.W.; Yealy, N.M.; Jones, A.E.; Shapiro, N.I. An Emergency Department Validation of the SEP-3 Sepsis and Septic Shock Definitions and Comparison with 1992 Consensus Definitions. Ann. Emerg. Med. 2017, 70, 544–552. [Google Scholar] [CrossRef]
- Ho, K.M.; Lan, N.S. Combining quick Sequential Organ Failure Assessment with plasma lactate concentration is comparable to standard Sequential Organ Failure Assessment score in predicting mortality of patients with and without suspected infection. J. Crit. Care 2017, 38, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Baumann, B.M.; Greenwood, J.C.; Lewis, K.; Nuckton, T.J.; Darger, B.; Shofer, F.; Troeger, D.; Jung, S.Y.; Kilgannon, J.H.; Rodriguez, R.M. Combining qSOFA criteria with initial lactate levels: Improved screening of septic patients for critical illness. Am. J. Emerg. Med. 2019. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Onal, U.; Valenzuela-Sánchez, F.; Vandana, K.; Rello, J. Mid-Regional Pro-Adrenomedullin (MR-proADM) as a Biomarker for Sepsis and Septic Shock: Narrative Review. Healthcare 2018, 6, 110. [Google Scholar] [CrossRef] [Green Version]
- Mat-Nor, M.B.; Ralib, A.M.; Abdulah, N.Z.; Pickering, J.W. The diagnostic ability of procalcitonin and interleukin-6 to differentiate infectious from noninfectious systemic inflammatory response syndrome and to predict mortality. J. Crit. Care 2016, 33, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.R.; Lindsell, C.J.; Pettilä, V.; Meyer, N.J.; Thair, S.A.; Karlsson, S.; Russell, J.A.; Fjell, C.; Boyd, J.H.; Ruokonen, E.; et al. A multibiomarker-based outcome risk stratification model for adult septic shock. Crit. Care Med. 2014, 42, 781–789. [Google Scholar] [CrossRef] [Green Version]
- De Pablo, R.; Monserrat, J.; Reyes, E.; Diaz-Martin, D.; Zapata, M.R.; Carballo, F.; De La Hera, A.; Prieto, A.; Alvarez-Mon, M. Mortality in patients with septic shock correlates with anti-inflammatory but not proinflammatory immunomodulatory molecules. J. Intensiv. Care Med. 2011, 26, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Ware, L.B.; Koyama, T.; Zhao, Z.; Janz, D.R.; Wickersham, N.E.; Bernard, G.R.; May, A.K.; Calfee, C.S.; Matthay, M.A. Biomarkers of lung epithelial injury and inflammation distinguish severe sepsis patients with acute respiratory distress syndrome. Crit. Care 2013, 17, R253. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.R.; Cvijanovich, N.Z.; Anas, N.; Allen, G.L.; Thomas, N.J.; Bigham, M.T.; Weiss, S.L.; Fitzgerald, J.C.; Checchia, P.A.; Meyer, K.; et al. A Multibiomarker-Based Model for Estimating the Risk of Septic Acute Kidney Injury. Crit. Care Med. 2015, 43, 1646–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikacenic, C.; Price, B.L.; Harju-Baker, S.; O’Mahony, D.S.; Robinson-Cohen, C.; Radella, F.; Hahn, W.O.; Katz, R.; Christiani, D.C.; Himmelfarb, J.; et al. A Two-Biomarker Model Predicts Mortality in the Critically Ill with Sepsis. Am. J. Respir. Crit. Care Med. 2017, 196, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Liu, D.; Chai, W.; Liu, D.; Long, Y. Role of sTREM-1 in predicting mortality of infection: A systematic review and meta-analysis. BMJ Open 2016, 6, e010314. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.S.; Hur, M.; Yi, A.; Kim, H.; Lee, S.; Kim, S.-N. Prognostic value of presepsin in adult patients with sepsis: Systematic review and meta-analysis. PLoS ONE 2018, 13, e0191486. [Google Scholar] [CrossRef] [PubMed]
- Zeiher, B.G.; Steingrub, J.; Laterre, P.F.; Dmitrienko, A.; Fukiishi, Y.; Abraham, E.; EZZI Study Group. LY315920NA/S-5920, a selective inhibitor of group IIA secretory phospholipase A2, fails to improve clinical outcome for patients with severe sepsis. Crit. Care Med. 2005, 33, 1741–1748. [Google Scholar] [CrossRef] [Green Version]
- Matera, G.; Puccio, R.; Giancotti, A.; Quirino, A.; Pulicari, M.C.; Zicca, E.; Caroleo, S.; Renzulli, A.; Liberto, M.C.; Focà, A. Impact of interleukin-10, soluble CD25 and interferon-γ on the prognosis and early diagnosis of bacteremic systemic inflammatory response syndrome: A prospective observational study. Crit. Care 2013, 17, R64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mearelli, F.; Fiotti, N.; Giansante, C.; Casarsa, C.; Orso, D.; De Helmersen, M.; Altamura, N.; Ruscio, M.; Castello, L.M.; Colonetti, E.; et al. Derivation and Validation of a Biomarker-Based Clinical Algorithm to Rule Out Sepsis From Noninfectious Systemic Inflammatory Response Syndrome at Emergency Department Admission: A Multicenter Prospective Study. Crit. Care Med. 2018, 46, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Leisenring, W.; Alono, T.; Pepe, M.S. Comparisons of predictive values of binary medical diagnostic tests for paired designs. Biometrics 2000, 56, 345–351. [Google Scholar] [CrossRef]
- Freund, Y.; Lemachatti, N.; Krastinova, E.; Van Laer, M.; Claessens, Y.-E.; Avondo, A.; Occelli, C.; Feral-Pierssens, A.-L.; Truchot, J.; Ortega, M.; et al. Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients With Suspected Infection Presenting to the Emergency Department. JAMA 2017, 317, 301–308. [Google Scholar] [CrossRef]
- Llewelyn, M.J.; Berger, M.; Gregory, M.; Ramaiah, R.; Taylor, A.L.; Curdt, I.; Lajaunias, F.; Graf, R.; Blincko, S.J.; Drage, S.; et al. Sepsis biomarkers in unselected patients on admission to intensive or high-dependency care. Crit. Care 2013, 17, R60. [Google Scholar] [CrossRef] [Green Version]
- Heffner, A.; Horton, J.M.; Marchick, M.R.; Jones, A.E. Etiology of illness in patients with severe sepsis admitted to the hospital from the emergency department. Clin. Infect. Dis. 2010, 50, 814–820. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.M.; Artigas, A.; Phillips, G.S.; Rhodes, A.; Beale, R.; Osborn, T.; Vincent, J.-L.; Townsend, S.; Lemeshow, S.; Dellinger, R.P. Outcomes of the Surviving Sepsis Campaign in intensive care units in the USA and Europe: A prospective cohort study. Lancet Infect. Dis. 2012, 12, 919–924. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Survivor n = 680 | Non Survivor n = 148 | p | OR | |
|---|---|---|---|---|
| Male | 368 | 67 | 0.051 | 1.426 (0.998–2.038) |
| Median age (IQR) | 78 (69–86) | 85 (79–90) | <0.001 | 1.051 (1.032–1.070) |
| Median Charlson Index (IQR) | 2 (1–4) | 3 (2–5) | <0.001 | 1.164 (1.085–1.250) |
| Medain SOFA (IQR) | 2 (1–4) | 4 (2–6) | <0.001 | 1.337 (1.238–1.444) |
| Median qSOFA (IQR) | 1 (0–1) | 1 (1–2) | <0.001 | 2.419 (1.919–3.050) |
| Clinical variables | ||||
| Body temperature | ||||
| >38°C | 301 (44) | 41 (28) | <0.001 | |
| <36°C | 12 (2) | 18 (12) | <0.001 | 7.708 (3.636–16.386) |
| White blood cell count | ||||
| >12,000/mm3 | 370 (54) | 101 (68) | 0.002 | 1.800 (1.234–2.626) |
| <4000/mm3 | 30 (4) | 4 (3) | 0.342 | |
| RR > 20/min or pCO2 < 32 mmHg | 508 (75) | 128 (86) | 0.002 | 2.167 (1.312–3.580) |
| Heart rate > 90/min | 509 (75) | 122 (82) | 0.05 | 1.576 (0.998–2.491) |
| Median BM (IQR)^ | ||||
| C–reactive protein (mg/dL) | 73 (20–160) | 117 (52–205) | <0.001 | 1.441 (1.231–1.687) |
| Lactate (mg/dL) | 13 (9–19) | 17 (12–26) | <0.001 | 2.491 (1.788–3.471) |
| Procalcitonin (ng/mL) | 0.33 (0.13–2.22) | 0.9 (0.24–3.7) | <0.001 | 1.178 (1.025–1.354) |
| sIL2Rα (pg/mL) | 13234 (8026–22158) | 20028 (12555–3269 | <0.001 | 1.908 (1.508–2.414) |
| sTREM–1 (pg/mL) | 375 (260–590) | 633 (409–1001) | <0.001 | 3.102 (2.332–4.126) |
| sPLA2GIIA (ng/mL) | 31 (21–35) | 31 (26–35) | 0.041 | 1.638 (1.149–2.334) |
| Presepsin (pg/mL) | 443 (280–908) | 802(476–1450) | <0.001 | 1.746 (1.446–2.107) |
| MR–proADM (nmol/L) | 1.6 (1.1–2.5) | 2.8 (1.9–4.7) | <0.001 | 4.361 (3.033–6.269) |
| Etiology of SIRS | ||||
| ni-SIRS | 81(93) | 6 (7) | 0.05 | |
| Infections | ||||
| Localized infections | 95 (99) | 1 (1) | <0.001 | |
| Sepsis | 400 (81) | 96 (19) | 0.096 | |
| Septic shock | 23 (47) | 26 (53) | <0.001 | |
| d-SIRS | 81 (81) | 19 (19) | 0.754 |
| AUROC | Sensitivity | Specificity | NPV | PPV | LR- | LR+ | |
|---|---|---|---|---|---|---|---|
| SOFA | 0.65 | 0.70 | 0.53 | 0.83 | 0.25 | 0.51 | 1.57 |
| (cut-off 3) | (0.61–0.69) | (0.61–0.78) | (0.50–0.58) | (0.81–0.91) | (0.23–0.33) | (0.39–0.67) | (1.36–1.79) |
| qSOFA | 0.67 | 0.46 | 0.82 | 0.84 | 0.36 | 0.66 | 2.58 |
| (cut-off 2) | (0.62–0.72) | (0.38–0.54) | (0.79–0.85) | (0.82–0.90) | (0.32–0.44) | (0.56–0.77) | (2.03–3.28) |
| eqSOFA1a | 0.79 | 0.79 | 0.68 | 0.94 | 0.35 | 0.31 | 2.43 |
| (cut-off* 0.16) | (0.75–0.83) | (0.72–0.86) | (0.63–0.71) | (0.91–0.97) | (0.31–0.45) | (0.23-0.43) | (2.12–2.79) |
| eqSOFA1+CRP+lactateb | 0.81 | 0.81 | 0.67 | 0.94 | 0.36 | 0.24 | 2.55 |
| (cut-off* 0.15) | (0.78–0.85) | (0.77–0.89) | (0.64–0.71) | (0.90–0.96) | (0.32–0.47) | (0.17–0.35) | (2.25–2.91) |
| eqSOFA1+CRP+lactate+MR-proADMc | 0.83 | 0.82 | 0.75 | 0.94 | 0.40 | 0.30 | 3.09 |
| (cut-off* 0.18) | (0.80–0.87) | (0.70–0.84) | (0.71–0.78) | (0.92–0.96) | (0.36–0.51) | (0.22–0.40) | (2.64–3.61) |
| Survivor n = 423 (%) | Non Survivor n = 122 (%) | p | OR | |
|---|---|---|---|---|
| Male | 242 (42) | 56 (53) | 0.027 | 0.635 (0.423–0.951) |
| Median age | 80 (73–86) | 85 (79–90) | <0.001 | 1.043 (1.021–1.065) |
| Median Charlson index | 3 (1–4) | 3 (2–5) | 0.142 | 1.072 (0.984–1.169) |
| Median SOFA (IQR) | 3 (2–4) | 4 (3–6) | <0.001 | 1.27 (1.16–1.38) |
| Median qSOFA | 1 (1–1) | 2 (1–2) | <0.001 | 2.776 (1.838–4.193) |
| Clinical variable | ||||
| Body Temperature | ||||
| >38°C | 204 (52) | 39 (31) | 0.001 | |
| <36°C | 9 (2) | 16 (13) | <0.001 | 6.943 (2.985–16.149) |
| White blood cell count | ||||
| >12,000/mm3 | 241 (60) | 82 (65) | 0.043 | 1.800 (1234–2626) |
| <4000/mm3 | 18 (4) | 4 (4) | 0.629 | |
| Heart rate>90 bpm | 311 (73) | 109 (80) | 0.095 | 2.167 (1.312–3.580) |
| RR>20/min or pCO2<32 mmHg | 328 (x) | 108 (x) | 0.008 | 2.234 (1.224–4.078) |
| Median biomarker (IQR) | ||||
| C-reactive protein (mg/dl) | 129 (73-209) | 130 (74-209) | 0.039 | 1.369 (1.123–1.644) |
| Lactate (mg/dl) | 14.4 (9.9-20) | 18.3 (12.2-27.2) | 0.007 | 1.863 (1.296–2.680) |
| Procalcitonin (ng/mL) | 1.14 (0.36–5.09) | 0.74 (0.26–5.47) | 0.061 | 1.087 (0.934–1.266) |
| MR-proADM (nmol/L) | 1.9 (1.3–3.2) | 3.02 (1.96–5.04) | <0.001 | 3.411 (2.275–5.113) |
| sIL2Rα (pg/ml) | 15130 (9741–25220) | 19446 (12596–31520) | 0.014 | 1.630 (1.246–2.133) |
| Presepsin (pg/mL) | 546 (341–1047) | 781 (446–1423) | 0.023 | 1.545 (1.239–1.926) |
| sTREM-1 (pg/mL) | 418 (280–711) | 619 (405–989) | <0.001 | 2.359 (1.727–3.223) |
| sPLA2GIIA (ng/mL) | 32.3 (27.4–36.3) | 32.2 (28.8–36.5) | 0.692 | 1.187 (0.768–1.834) |
| sTNFR-1 (pg/ml) | 423.5 (320.4–634.0) | 560.61 (388.2–712.6) | <0.001 | 3.164 (1.946–5.143) |
| Source of infection | ||||
| Single source | 399 (94) | 98 (80) | 0.001 | |
| LRTI | 240 (56) | 71 (58) | 0.024 | |
| Non LRTI | 159 (38) | 27 (22) | 0.092 | |
| Multiple source | 24 (6) | 24 (20) | <0.001 | |
| Etiology of infection | ||||
| Clinically documented | 261 (61) | 80 (66) | 0.345 | |
| Microbiologically documented | 174 (41) | 51 (41) | 0.932 | |
| Monomicrobial | 144 (34) | 39 (31) | 0.669 | |
| Bacterial | 133 (31) | 41 (34) | 0.814 | |
| Gram positive | 44 (10) | 19 (15) | 0.002 | |
| Gram negative | 77 (18) | 11 (15) | 0.037 | |
| Non bacterial | 10 (2) | 1 (0) | 0.307 | |
| Polymicrobial | 30 (7) | 12 (1) | 0.317 | |
| BSI | 70 (16) | 29 (24) | 0.365 | |
| Non BSI | 106 (25) | 25 (20) | 0.298 |
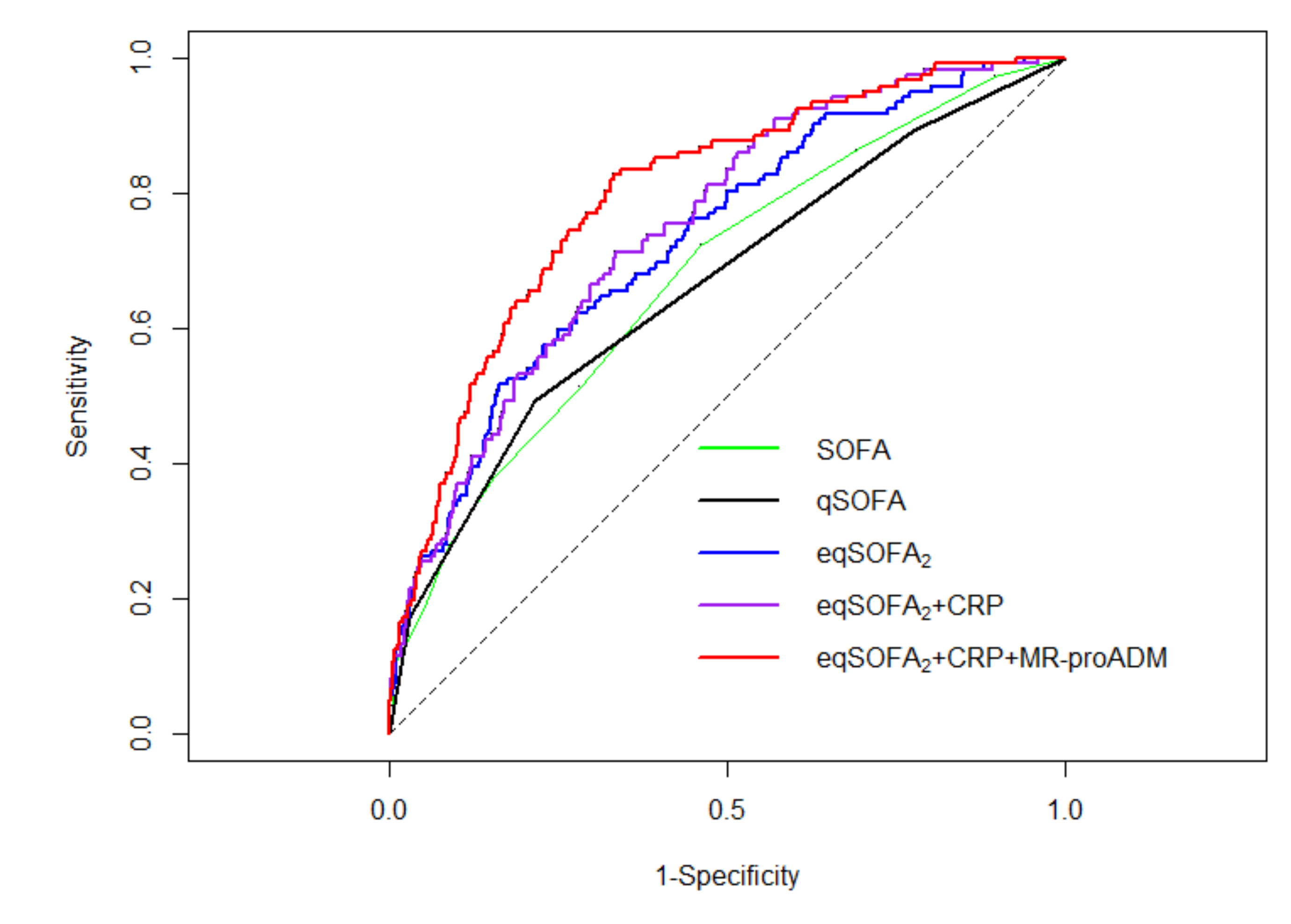
| AUROC | Sensitivity | Specificity | NPV | PPV | LR- | LR+ | |
|---|---|---|---|---|---|---|---|
| SOFA | 0.65 | 0.75 | 0.45 | 0.83 | 0.28 | 0.52 | 1.39 |
| (cut-off 3) | (0.59–0.69) | (0.67–0.80) | (0.40–0.50) | (0.81–0.88) | (0.24–0.38) | (0.37–0.70) | (1.21–1.59) |
| qSOFA | 0.66 | 0.49 | 0.78 | 0.80 | 0.40 | 0.65 | 2.29 |
| (cut-off 2) | (0.61–0.71) | (0.40–0.58) | (0.74–0.82) | (0.79–0.87) | (0.34–0.49) | (0.54–0.77) | (1.77–2.95) |
| eqSOFA2a | 0.73 | 0.52 | 0.84 | 0.85 | 0.48 | 0.58 | 3.21 |
| (cut-off* 0.30) | (0.68–0.78) | (0.42–0.61) | (0.80–0.87) | (0.81–0.89) | (0.42–0.57) | (0.48–0.70) | (2.43–4.24) |
| eqSOFA2+CRPb | 0.75 | 0.71 | 0.67 | 0.88 | 0.38 | 0.43 | 2.14 |
| (cut-off* 0.22) | (0.70–0.79) | (0.62–0.79) | (0.62–0.71) | (0.84–0.91) | (0.33–0.48) | (0.32–0.57) | (1.79–2.55) |
| eqSOFA2+CRP+MR-proADMc | 0.80 | 0.83 | 0.67 | 0.93 | 0.42 | 0.26 | 2.50 |
| (cut-off* 0.18) | (0.76–0.84) | (0.75–0.89 | (0.62–0.71) | (0.89–0.94) | (0.37–0.55) | (0.17–0.38) | (2.14–2.93) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mearelli, F.; Barbati, G.; Casarsa, C.; Giansante, C.; Breglia, A.; Spica, A.; Moras, C.; Olivieri, G.; Occhipinti, A.A.; De Nardo, M.; et al. The Integration of qSOFA with Clinical Variables and Serum Biomarkers Improves the Prognostic Value of qSOFA Alone in Patients with Suspected or Confirmed Sepsis at ED Admission. J. Clin. Med. 2020, 9, 1205. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041205
Mearelli F, Barbati G, Casarsa C, Giansante C, Breglia A, Spica A, Moras C, Olivieri G, Occhipinti AA, De Nardo M, et al. The Integration of qSOFA with Clinical Variables and Serum Biomarkers Improves the Prognostic Value of qSOFA Alone in Patients with Suspected or Confirmed Sepsis at ED Admission. Journal of Clinical Medicine. 2020; 9(4):1205. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041205
Chicago/Turabian StyleMearelli, Filippo, Giulia Barbati, Chiara Casarsa, Carlo Giansante, Andrea Breglia, Andrea Spica, Cristina Moras, Gaia Olivieri, Alessandro Agostino Occhipinti, Margherita De Nardo, and et al. 2020. "The Integration of qSOFA with Clinical Variables and Serum Biomarkers Improves the Prognostic Value of qSOFA Alone in Patients with Suspected or Confirmed Sepsis at ED Admission" Journal of Clinical Medicine 9, no. 4: 1205. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041205