A Literature Review of GP Knowledge and Understanding of ME/CFS: A Report from the Socioeconomic Working Group of the European Network on ME/CFS (EUROMENE)

 , , , , , ,
, , , , , ,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
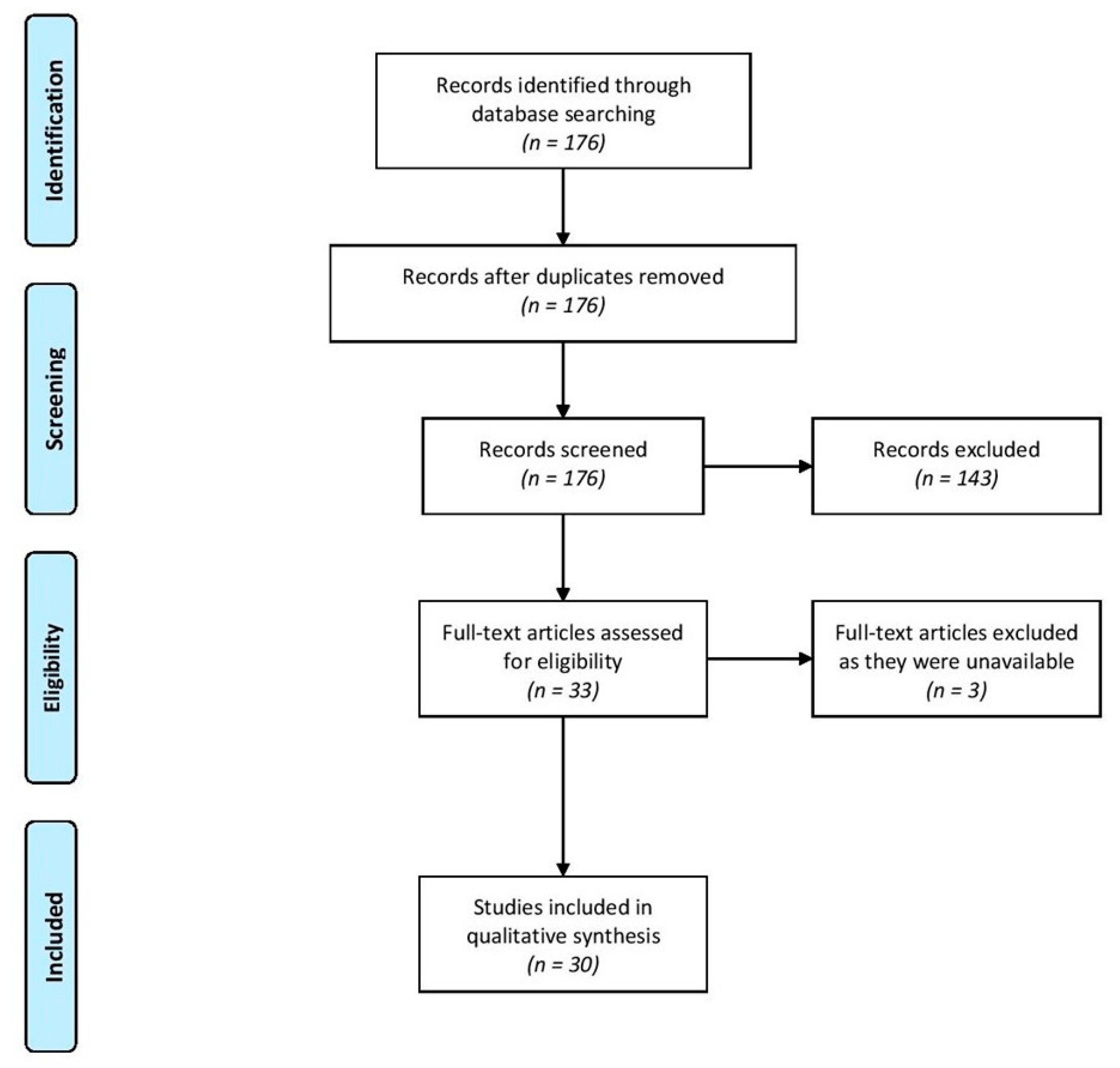
3.1. Search Strategy
3.1.1. Implementation
3.1.2. Papers Identified
3.2. Quantitative Studies
3.2.1. Surveys of GPs
3.2.2. Surveys of ME/CFS Patients
3.2.3. Other Quantitative Studies
3.3. Qualitative Studies
3.3.1. Studies of GPs
3.3.2. Studies of Patients
3.4. Overview Papers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lindan, R. Benign Myalgic Encephalomyelitis. Can. Med. Assoc. J. 1956, 75, 596–597. [Google Scholar]
- Acheson, E.D. The clinical syndrome variously called myalgic encephalomyelitis, Iceland disease and epidemic neuromyasthenis. Am. Med. 1959, 26, 589–595. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.M.; Sherkey, J.A. Myalgic encephalomyelitis/chronic fatigue syndrome: Clinical working case definition, diagnostic and treatment protocols. J. Chronic Fatigue Syndr. 2003, 11, 7–116. [Google Scholar] [CrossRef]
- Johnstone, S.C.; Staines, D.R.; Marshall-Gradisnik, S.M. Epidemiological characteristics of chronic fatigue syndrome/myalgic encephalomyelitis in Australian patients. Clin. Epidemiol. 2016, 8, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Pheby, D.; Lacerda, E.; Nacul, L.; de Lourdes Drachler, M.; Campion, P.; Howe, A.; Sakellariou, D. A disease register for ME/CFS: Report of a pilot study. BMC Res. Notes 2011, 4, 139–146. [Google Scholar] [CrossRef]
- Lloyd, A.R.; Hickie, I.; Boughton, C.R.; Wakefield, D.; Spencer, O. Prevalence of chronic fatigue syndrome in an Australian population. Med. J. Aust. 1990, 153, 522–528. [Google Scholar] [CrossRef]
- Action for ME. Available online: https://actionforme.org.uk/what-is-me/introduction/. (accessed on 6 January 2020).
- EUROMENE. Available online: http://euromene.eu/ (accessed on 13 October 2020).
- Pheby, D.F.; Arāja, D.; Berkis, U.; Brenna, E.; Cullinan, J.; De Korwin, J.-D.; Gitto, L.; Hughes, D.; Hunter, R.; Trepel, D.; et al. The development of a consistent Europe-wide approach to investigating the economic impact of myalgic encephalomyelitis (ME/CFS): A report from the European Network on ME/CFS (EUROMENE). Healthcare 2020, 8, 88. [Google Scholar] [CrossRef] [Green Version]
- COST Action 15111—EUROMENE (European ME/CFS Research Network), Working Group 3: Socio-Economics. Deliverable 10—Common consensus protocol for economic loss calculation due to ME/CFS. Brussels. September 2019. Available online: http://euromene.eu/workinggroups/deliverables/deliverable.html (accessed on 14 October 2020).
- Bayliss, K.; Goodall, M.; Chisholm, A.; Fordham, B.; Chew-Graham, C.; Riste, L.; Fisher, L.; Lovell, K.; Peters, S.; Wearden, A.J. Overcoming the barriers to the diagnosis and management of chronic fatigue syndrome/ME in primary care: A meta synthesis of qualitative studies. BMC Fam. Pract. 2014, 15, 44. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [Green Version]
- Saidi, G.; Haines, L. The management of children with chronic fatigue syndrome-like illness in primary care: A cross-sectional study. Brit. J. Gen. Pract. 2006, 56, 43–47. [Google Scholar]
- Thomas, M.; Smith, A.P. Primary healthcare provision and Chronic Fatigue Syndrome: A survey of patients’ and General Practitioners’ beliefs. BMC Fam. Pract. 2005, 6, 49. [Google Scholar] [CrossRef] [Green Version]
- Ho-Yen, D.O.; McNamara, I. General practitioners’ experience of the chronic fatigue syndrome. Brit. J. Gen. Pract. 1991, 41, 324–326. [Google Scholar]
- Bowen, J.; Pheby, D.; Charlett, A.; McNulty, C. Chronic Fatigue Syndrome: A survey of GPs’ attitudes and knowledge. Fam. Pract. 2005, 22, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Steven, I.D.; McGrath, B.; Qureshi, F.; Wong, C.; Chern, I.; Pearn-Rowe, B. General practitioners’ beliefs, attitudes and reported actions towards chronic fatigue syndrome. Aust. Fam. Physician 2000, 29, 80–85. [Google Scholar]
- Bazelmans, E.; Vercoulen, J.; Swanink, C.; Fennis, J.; Galama, J.; Van Weel, C.; Van Der Meer, J.; Bleijenberg, G. Chronic Fatigue Syndrome and Primary Fibromyalgia Syndrome as recognized by GPs. Fam. Pract. 1999, 16, 602–604. [Google Scholar] [CrossRef] [Green Version]
- FitzGibbon, E.J.; Murphy, D.; O’Shea, K.; Kelleher, C. Chronic debilitating fatigue in Irish general practice: A survey of general practitioners’ experience. Br. J. Gen. Pract. 1997, 47, 618–622. [Google Scholar]
- Van Hoof, E. The doctor-patient relationship in chronic fatigue syndrome: Survey of patient perspectives. Qual. Prim. Care 2009, 17, 263–270. [Google Scholar]
- Vandenbergen, J.; Vanheule, S.; Desmet, M.; Verhaeghe, P. Unexplained chronic fatigue and interpersonal problems: A study in a primary care population. Int. J. Psychiatry Med. 2009, 39, 325–340. [Google Scholar] [CrossRef]
- Cathébras, P.; Jacquin, L.; Le Gal, M.; Fayol, C.; Bouchou, K.; Rousset, H. Correlates of somatic causal attributions in primary care patients with fatigue. Psychother. Psychosom. 1995, 63, 174–180. [Google Scholar] [CrossRef]
- Hansen, A.H.; Lian, O.S. Experiences of general practitioner continuity among women with chronic fatigue syndrome/myalgic encephalomyelitis: A cross-sectional study. BMC Health Serv. Res. 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.H.; Lian, O.S. How do women with chronic fatigue syndrome/myalgic encephalomyelitis rate quality and coordination of healthcare services? A cross-sectional study. BMJ Open 2016, 6, e010277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, O.S.; Hansen, A.H. Factors facilitating patient satisfaction among women with medically unexplained long-term fatigue: A relational perspective. Health Interdiscip. J. Soc. Study Health Illn. Med. 2015, 20, 308–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jason, L.A.; Ferrari, J.R.; Taylor, R.R.; Slavich, S.P.; Stenzel, C.L. A national assessment of the service, support, and housing preferences by persons with chronic fatigue syndrome. Toward a comprehensive rehabilitation program. Eval. Health Prof. 1996, 19, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.M.; Thomas, J.M.; Hamilton, W.T.; White, P.D. Incidence of fatigue symptoms and diagnoses presenting in UK primary care from 1990 to 2001. JRSM 2004, 97, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Bakken, I.J.; Tveito, K.; Aaberg, K.M.; Ghaderi, S.; Gunnes, N.; Trogstad, L.; Magnus, P.; Stoltenberg, C.; Håberg, S.E. Comorbidities treated in primary care in children with chronic fatigue syndrome / myalgic encephalomyelitis: A nationwide registry linkage study from Norway. BMC Fam. Pract. 2016, 17, 128. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.J.; Menezes, P.R.; Hotopf, M.; Bhugra, D.; Wessely, S. Comparative epidemiology of chronic fatigue syndrome in Brazilian and British primary care: Prevalence and recognition. Br. J. Psychiatry 2009, 194, 117–122. [Google Scholar] [CrossRef]
- Brimmer, D.J.; McCleary, K.K.; A Lupton, T.; Faryna, K.M.; Hynes, K.; Reeves, W.C. A train-the-trainer education and promotion program: Chronic fatigue syndrome-a diagnostic and management challenge. BMC Med. Educ. 2008, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Denz-Pe nhey, H.; Murdoch, J.C. Service delivery for people with chronic fatigue syndrome: A pilot action research study. Fam. Pract. 1993, 10, 14–18. [Google Scholar] [CrossRef]
- Bayliss, K.; Riste, L.; Band, R.; Peters, S.; Wearden, A.; Lovell, K.; Fisher, L.; A Chew-Graham, C. Implementing resources to support the diagnosis and management of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME) in primary care: A qualitative study. BMC Fam. Pract. 2016, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Chew-Graham, C.; Dowrick, C.; Wearden, A.; Richardson, V.; Peters, S. Making the diagnosis of Chronic Fatigue Syndrome/Myalgic Encephalitis in primary care: A qualitative study. BMC Fam. Pract. 2010, 11, 16. [Google Scholar] [CrossRef] [Green Version]
- Hannon, K.L.; Peters, S.; Fisher, L.; Riste, L.; Wearden, A.J.; Lovell, K.; Turner, P.; Leech, Y.; Chew-Graham, C. Developing resources to support the diagnosis and management of Chronic Fatigue Syndrome/Myalgic Encephalitis (CFS/ME) in primary care: A qualitative study. BMC Fam. Pract. 2012, 13, 93. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, K.; Riste, L.; Fisher, L.; Wearden, A.; Peters, S.; Lovell, K.; Chew-Graham, C. Diagnosis and management of chronic fatigue syndrome/myalgic encephalitis in black and minority ethnic people: A qualitative study. Prim. Health Care Res. Dev. 2013, 15, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Raine, R.; Carter, S.; Sensky, T.; Black, N. General practitioners’ perceptions of chronic fatigue syndrome and beliefs about its management, compared with irritable bowel syndrome: Qualitative study. BMJ 2004, 328, 1354–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, A.S. Investigating unexplained fatigue in general practice with a particular focus on CFS/ME. BMC Fam. Pract. 2016, 17, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wearden, A.J.; Chew-Graham, C. Managing chronic fatigue syndrome in U.K. primary care: Challenges and opportunities. Chronic Illn. 2006, 2, 143–153. [Google Scholar] [CrossRef]
- Murdoch, J.C. Chronic fatigue syndrome. The patient centred clinical method--a guide for the perplexed. Aust. Fam. Physician 2003, 32, 883–887. [Google Scholar]
- Campion, P. Chronic fatigue syndrome: Is the biopsychosocial model responsible for patient dissatisfaction and harm? (letter). Br. J. Gen. Pract. 2016, 66, 511. [Google Scholar] [CrossRef] [Green Version]
- Ax, S.; Gregg, V.H.; Jones, D. Chronic Fatigue Syndrome: Sufferers’ Evaluation of Medical Support. J. R. Soc. Med. 1997, 90, 250–254. [Google Scholar] [CrossRef] [Green Version]
- Saltzstein, B.J.; Wyshak, G.; Hubbuch, J.T.; Perry, J.C. A naturalistic study of the chronic fatigue syndrome among women in primary care. Gen. Hosp. Psychiatry 1998, 20, 307–316. [Google Scholar] [CrossRef]
- Chew-Graham, C.A.; Cahill, G.; Dowrick, C.; Wearden, A.; Peters, S. Using Multiple Sources of Knowledge to Reach Clinical Understanding of Chronic Fatigue Syndrome. Ann. Fam. Med. 2008, 6, 340–348. [Google Scholar] [CrossRef] [Green Version]
- Chew-Graham, C.; Brooks, J.; Wearden, A.; Dowrick, C.; Peters, S. Factors influencing engagement of patients in a novel intervention for CFS/ME: A qualitative study. Prim. Health Care Res. Dev. 2010, 12, 112–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilje, A.M.; Söderlund, A.; Malterud, K. Obstructions for quality care experienced by patients with chronic fatigue syndrome (CFS)—A case study. Patient Educ. Couns. 2008, 73, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Blease, C.; Carel, H.; Geraghty, K. Epistemic injustice in healthcare encounters: Evidence from chronic fatigue syndrome. J. Med. Ethics. 2017, 43, 549–557. [Google Scholar] [CrossRef]
- Huibers, M.J.H.; Kant, I.J.; Swaen, G.M.H.; Kasl, S.V. Prevalence of chronic fatigue syndrome-like caseness in the working population: Results from the Maastricht cohort study. Occup. Environ. Med. 2004, 61, 464–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Dowd, H.; Beasant, L.; Ingram, J.; A Montgomery, A.; Hollingworth, W.W.; Gaunt, D.; Collin, S.M.; Horne, S.; Jones, B.; Crawley, E. The feasibility and acceptability of an early intervention in primary care to prevent chronic fatigue syndrome (CFS) in adults: Randomised controlled trial. Pilot Feasibility Stud. 2020, 6, 65. [Google Scholar] [CrossRef] [PubMed]
- Kermack, W.O.; McKendrick, A.G. Contribution to the mathematical theory of epidemics. Proc. R. Soc. London 1927, 772, 701–721. [Google Scholar]
- Waters, F.G.; McDonald, G.J.; Banks, S.; Waters, R.A. Myalgic Encephalomyelitis (ME) outbreaks can be modelled as an infectious disease: A mathematical reconsideration of the Royal Free Epidemic of 1955. Fatigue: Biomed. Health Behav. 2020, 8, 70–83. [Google Scholar] [CrossRef]
- McEvedy, C.P.; Beard, A.W. Royal Free Epidemic of 1955: A Reconsideration. BMJ 1970, 1, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Horton, S.; Poland, F.; Kale, S.; Drachler, M.D.L.; Leite, J.C.D.C.; McArthur, M.; Campion, P.; Pheby, D.; Nacul, L. Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) in adults: A qualitative study of perspectives from professional practice. BMC Fam. Pract. 2010, 11, 89. [Google Scholar] [CrossRef] [Green Version]
- Nacul, L.; Lacerda, E.M.; Kingdon, C.C.; Curran, H.; Bowman, E.W. How have selection bias and disease misclassification undermined the validity of myalgic encephalomyelitis/chronic fatigue syndrome studies? J. Health Psychol. 2019, 24, 1765–1769. [Google Scholar] [CrossRef] [Green Version]
- Speight, N. Severe ME in Children. Healthcare 2020, 8, 211. [Google Scholar] [CrossRef]
- Stadje, R.; Dornieden, K.; Baum, E.; Becker, A.; Biroga, T.; Bösner, S.; Haasenritter, J.; Keunecke, C.; Viniol, A.; Donner-Banzhoff, N. The differential diagnosis of tiredness: A systematic review. BMC Fam. Pract. 2016, 17, 147. [Google Scholar] [CrossRef] [Green Version]
- Pheby, D.; Saffron, L. Risk factors for severe ME/CFS. Biol. Med. 2009, 1, 50–74. [Google Scholar]
- Fossey, M.; Libman, E.; Bailes, S.; Baltzan, M.; Schondorf, R.; Amsel, R.; Fichten, C.S. Sleep quality and psychological adjustment in chronic fatigue syndrome. J. Behav. Med. 2004, 27, 581–605. [Google Scholar] [CrossRef] [Green Version]
- Oxfordshire ME Group for Action (OMEGA). OMEGA Membership Survey on Local NHS Services for ME/CFS (April 2013). Available online: http://omegaoxon.org/publications (accessed on 22 July 2020).
- Hng, K.N. Doctors’ Knowledge and Understanding of Myalgic Encephalomyelitis—United Kingdom. 2018. Available online: https://bit.ly/2yFAtY8 or https://bit.ly/3byfwga (accessed on 14 October 2020).
- European Federation of Neurological Associations [EFNA--] 2020—Survey on Stigma and Neurological Disorder. Available online: https://www.efna.net/survey2020/ (accessed on 22 July 2020).
- Anon. Lifelong Lockdown: Lessons Learned from the Health and Wellbeing Survey of Australians Living with ME/CFS 2019. Emerge Australia, October 2020. Available online: https://www.emerge.org.au/health-and-wellbeing-survey-2019 (accessed on 14 October 2020).
- CFS/ME Working Group. Report to the Chief Medical Officer of an Independent Working Group; Department of Health: London, UK, 2001. [Google Scholar]


{kind=link}
| Step | Description | No. Records |
|---|---|---|
| 1 | General Practice or family practice | 75,004 |
| 2 | limit 1 to abstracts | 35,740 |
| 3 | Primary care, or primary health care | 133,124 |
| 4 | limit 3 to abstracts | 104,892 |
| 5 | 2 or 4 | 129,775 |
| 6 | Myalgic encephalomyelitis, or fatigue syndrome, chronic | 5606 |
| 7 | limit 6 to abstracts | 3936 |
| 8 | 5 and 7 | 176 |
| 9 | After exclusions (because not conforming to inclusion criteria) | 33 |
| 10 | After exclusions (because of unavailability of full texts) | 30 |
| Type of Study | No. Papers Identified * |
|---|---|
| Reviews | 1 |
| GP surveys—quantitative | 7 |
| Patient surveys—quantitative | 7 |
| Database studies—quantitative | 2 |
| Medical record review—quantitative | 1 |
| Evaluation of training programme—quantitative | 1 |
| GP studies—qualitative | 6 |
| Patient studies—qualitative | 9 |
| Overview papers on myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) | 4 |
| Authors | Year of Publication | Location | Sample Size | Principal Finding: % Respondents Accepting Existence of ME/CFS as a Genuine Clinical Entity | Definition of Outcome |
|---|---|---|---|---|---|
| Ho-Yen DO, McNamara I. [15] | 1991 | Scotland | 178 | 71 | Response to question as to whether respondent accepted the existence of chronic fatigue syndrome, requiring ‘yes’, ‘no’ or ‘undecided’ response. |
| Fitzgibbon EJ, Murphy D, O’Shea K et al. [19] | 1997 | Ireland | 118 | 58 | Response to question: ‘Do you accept CFS as a distinct clinical entity?’, requiring ‘accept’, ‘do not accept’ or ‘undecided’ response. |
| Bazelmans E, Vercoulen JH, Swanink CM et al. [18] | 1999 | Netherlands | 3881 | 99 | Inferred from number of invitees who cited disbelief in the syndrome as their reason for non-response |
| Thomas MA, Smith AP. [14] | 2005 | South Wales | 45 | 56 | Proportion of respondents agreeing that the syndrome actually exists (specific question not reported) |
| Bowen J, Pheby D, Charlett A, McNulty C. [16] | 2005 | South-west England | 811 | 72 | Responses agreeing or strongly agreeing to proposition via a 5-point Likert scale |
| Reference | Respondents Accepting ME/CFS as Genuine Diagnosis | 95% Confidence Interval | |
|---|---|---|---|
| No./Sample Size | % | ||
| Ho-Yen and McNamara [15] | 127/178 | 71.0 | 33.0–47.2 |
| Fitzgibbon et al. [19] | 68/118 | 58.0 | 48.6–66.2 |
| Thomas and Smith [14] | 25/45 | 56.0 | 41.1–69.1 |
| Bowen et al. [16] | 584/811 | 72.0 | 68.8–75.0 |
| TOTAL | 804/1152 | 69.8 | 67.1–72.4 |
| Authors | Year of Publication | Location | Sample Size | Source of Recruitment | Principal Relevant Outcome Measure | |
|---|---|---|---|---|---|---|
| Description | Numerical Value | |||||
| Jason LA; Ferrari JR; Taylor RR; Slavich SP; Stenzel CL [26] | 1996 | U.S.A. | 1073 | Self-selected respondents to a survey published in the CFIDS Chronicle. | % respondents reporting a need for better education of health care professionals (including in primary care) about ME/CFS | 65 |
| Hansen AH; Lian OS [23] | 2016 | Norway | 488 | Norwegian ME Association (cross-sectional survey) | % respondents reporting poor continuity of GP care:
| 35 35 33 |
| Hansen AH; Lian OS [24]. | 2016 | Norway | 431 | Norwegian ME Association (cross-sectional survey) | % assessing overall quality of primary care to be poor or very poor | 61 |
| Lian OS; Hansen AH [25]. | 2016 | Norway | 431 | Norwegian ME Association (cross-sectional survey) | % reporting satisfaction (to a large extent or to some extent) with GP support during initial phase of illness | 46 |
| Authors | Year of Publication | Location | Methodology | GP Sample Size | Relevant Outcome Measures | Findings |
|---|---|---|---|---|---|---|
| Denz-Penhey H, Murdoch JC [31] | 1993 | New Zealand | Action research in a general practice | 10 | Identification of GP tasks (illness acknowledgement, symptom control, recommendation of health behaviours, relapse prevention), and service and delivery mechanisms | The authors concluded that medical models of illness were unhelpful, and patients suffered as failure to legitimate their conditions led to denial of access to medical care. They wrote: “Doctors … have a weighty bias towards the biomedical model even when it has manifestly failed to meet the needs of our patients.” |
| Raine R; Carter S; Sensky T [32] | 2004 | England | Focus group discussions of clinical scenarios | 46 | Thematic analysis of focus group transcripts, examined against field notes. | Findings support research indicating that outcomes are poorer where doctors and patients disagree. Doctors’ beliefs could result in negative stereotyping of patients with CFS, which constituted a barrier to effective clinical management. |
| Chew-Graham C; Dowrick C; Wearden A; Richardson V; Peters S [33] | 2010 | NW England | Semi-structured interviews with patients participating in a primary care-based randomised controlled trial (the FINE Trial) | 22 | Five themes were identified: defining CFS/ME, excluding physical causes, potential harm from the label, the role of referral and moving on from making the diagnosis. | There was lack of confidence among GPs about making the diagnosis and uncertainty about CFS/ME as a medical condition. Hence, GPs were reluctant to make the diagnosis of CFS/ME, with resultant diagnostic delays and lack of appropriate primary care. |
| Hannon K, Peters S, Fisher L, Riste L, Wearden A, Lovell K, Turner P, Leech Y, Chew-Graham C [34] | 2012 | NW England | Semi-structured interviews with patients, carers, practice nurses, ME/CFS specialists and GPs | 9 | Acquisition of information with the intention of developing a training resource on ME/CFS for primary care. | The GPs had varying degrees of understanding of ME/CFS; some questioned whether ME/CFS was a legitimate illness, and were unaware of the evidence base. There was concern about difficulties of referral to secondary care due to fragmented services and lack of collaboration. |
| Bayliss K; Riste L; Fisher L; Wearden A; Peters S; Lovell K; Chew-Graham C [35] | 2014 | NW England | Semi-structured interviews with key stakeholders (11 BME patients, 2 carers, 9 GPs, 5 practice nurses, 4 ME/CFS specialists, 5 BME community leaders) | 9 | Key themes identified were: models of illness, access to care, language and understanding, family and community, religion and culture, stereotypes and racism. | Patients tended to be unwilling to consult GPs for fatigue, and also encountered impediments to accessing primary care. The high turnover of inner-city GPs may constitute a barrier to accessing care. |
| Bayliss K, Riste L, Band R, Peters S, Wearden A, Lovell K, Fisher L, Chew-Graham CA [36] | 2016 | NW England | Semi-structured interviews with GPs taking part in an ME/CFS training programme | 28 | GPs’ experience of managing people with CFS/ME before participating in the study, and their opinions on the training programme. | There was difficulty recruiting GP practices, for reasons including scepticism about ME/CFS, the complexity of managing the condition, lack of time in a 10 min consultation, and limited specialist referral options. |
| Authors | Year of Publication | Location | Methodology | Patient Sample Size | Relevant Outcome Measures | Findings |
|---|---|---|---|---|---|---|
| Denz-Penhey H, Murdoch JC [31] | 1993 | New Zealand | Action research in a general practice | 10 | What patients expected of their GPs. | Patients primarily sought legitimation, and acknowledgement of the illness (i.e., acceptance, diagnosis, support), symptom control, recommendations regarding health behaviours, and relapse prevention. There was much dissatisfaction with GPs’ perceived failure to meet patients’ needs. |
| Ax S; Gregg VH; Jones D. [41] | 1997 | London, U.K. | Semi-structured interviews | 18 | Illness beliefs, meaning of the diagnosis and satisfaction with medical support. | Most participants found that GP emotional and informational support was inadequate, and they felt unsupported. This was coupled with the rejection of medical and health professionals and an increased sense of self-reliance. |
| Saltzstein BJ, Wyshak G, Hubbuch JT, Perry JC [42] | 1998 | U.S.A. | Semi-structured interviews | 15 | Self-report v. perception of physician’s prognosis | Improvement in health appeared associated with early diagnosis and a physician optimistic about prognosis |
| Chew-Graham CA; Cahill G; Dowrick C; Wearden A; Peters S [43] | 2008 | NW England | Semi-structured interviews with patients participating in a primary care-based randomised controlled trial (the FINE Trial) | 24 | Key emergent themes: (1) understanding CFS/ME and management, and (2) accessing alternative sources of evidence. | Patients were aware of the risk to their credibility from GPs who may not have accepted that ME/CFS even existed as a genuine diagnosis, and were also aware of the limitations of many GPs’ knowledge of the condition. |
| Chew-Graham C; Brooks J; Wearden A; Dowrick C; Peters S [44]. | 2011 | NW England | Semi-structured interviews with patients participating in a primary care–based randomised controlled trial (the FINE Trial) | 19 | Emergent themes: feeling accepted and believed by the therapist, their own acceptance of the diagnosis, and accepting the model of illness presented by the therapist. | Engagement of patients with pragmatic rehabilitation in primary care depends on whether they feel accepted and believed, accept the diagnosis, and have an illness model consistent with the treatment. |
| Gilje AM; Soderlund A; Malterud K. [45]. | 2008 | Norway | Questionnaire and follow-up meeting | 12 | Exploration of patients’ views about the impact of negative opinions held by doctors. | Lack of GP belief in or acknowledgement of the reality of the illness can be worse for patients than the illness itself. Participants wanted doctors to question, listen and take them seriously. GPs were perceived as knowing little about ME/CFS, and therefore unable to give advice. |
| Hannon K, Peters S, Fisher L, Riste L, Wearden A, Lovell K, Turner P, Leech Y, Chew-Graham C [34] | 2012 | NW England | Semi-structured interviews with patients, 9 of whom were from BME communities. | 16 | Key themes identified were the need to be believed, the importance of a positively framed diagnosis, defining, prioritising, and managing symptoms, maximising the benefit of consultation, and the role of carers. | Patients expressed frustration when GPs challenged the legitimacy of the condition, and failed to recognise its seriousness, or how it can affect articulateness and memory. Patients felt a need for signposting, but GPs lacked knowledge of the condition and relevant contacts. |
| Bayliss K; Riste L; Fisher L; Wearden A; Peters S; Lovell K; Chew-Graham C [35] | 2014 | NW England | Semi-structured interviews with key stakeholders (11 BME patients, 2 carers, 9 GPs, 5 practice nurses, 4 ME/CFS specialists, 5 BME community leaders) | 11 | Themes raised by patients included: GPs’ perceptions; patients’ lack of awareness of ME/CFS; community pressures. | Patients perceived a lack of focus by GPs on non-specific symptoms, lack of continuity among city-centre GPs, negative experiences with GPs (e.g., seeing some BME people as ‘work shy’). BME GPs seen as less likely to diagnose ME/CFS. Community pressures include language barriers; family pressures, e.g., to be a high achiever; the influence of religion, so that some would turn to religion or spiritual healers rather than primary care. GPs considered unaware of this. |
| Bayliss K, Riste L, Band R, Peters S, Wearden A, Lovell K, Fisher L, Chew-Graham CA [36] | 2016 | NW England | Semi-structured interviews with GPs taking part in an ME/CFS training programme | 57 | The enquiry centres on the extent of agreement between patients and GPs about how and by whom ME/CFS should be managed in primary care, what is needed to be done to achieve collaboration between patients and GPs, and how the training programme should be assessed. | Patients felt that ME/CFS should be managed within primary care, but wanted to be believed and to receive a positive diagnosis. Where this did not happen, patients disengaged from primary care, illustrating the tension between their needs and barriers to care perceived by GPs, including the inadequacy of a ten-minute consultation for such a complex illness. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pheby, D.F.H.; Araja, D.; Berkis, U.; Brenna, E.; Cullinan, J.; de Korwin, J.-D.; Gitto, L.; Hughes, D.A.; Hunter, R.M.; Trepel, D.; et al. A Literature Review of GP Knowledge and Understanding of ME/CFS: A Report from the Socioeconomic Working Group of the European Network on ME/CFS (EUROMENE). Medicina 2021, 57, 7. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010007
Pheby DFH, Araja D, Berkis U, Brenna E, Cullinan J, de Korwin J-D, Gitto L, Hughes DA, Hunter RM, Trepel D, et al. A Literature Review of GP Knowledge and Understanding of ME/CFS: A Report from the Socioeconomic Working Group of the European Network on ME/CFS (EUROMENE). Medicina. 2021; 57(1):7. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010007
Chicago/Turabian StylePheby, Derek F. H., Diana Araja, Uldis Berkis, Elenka Brenna, John Cullinan, Jean-Dominique de Korwin, Lara Gitto, Dyfrig A. Hughes, Rachael M. Hunter, Dominic Trepel, and et al. 2021. "A Literature Review of GP Knowledge and Understanding of ME/CFS: A Report from the Socioeconomic Working Group of the European Network on ME/CFS (EUROMENE)" Medicina 57, no. 1: 7. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010007