Estimating Vitamin C Status in Critically Ill Patients with a Novel Point-of-Care Oxidation-Reduction Potential Measurement

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Cohorts
2.2.1. Vitamin C Status Study
2.2.2. Pharmacokinetic Study
2.3. Vitamin C Measurements
2.3.1. Vitamin C Status Study
2.3.2. Pharmacokinetic Study
2.4. Defining Vitamin C Deficiency
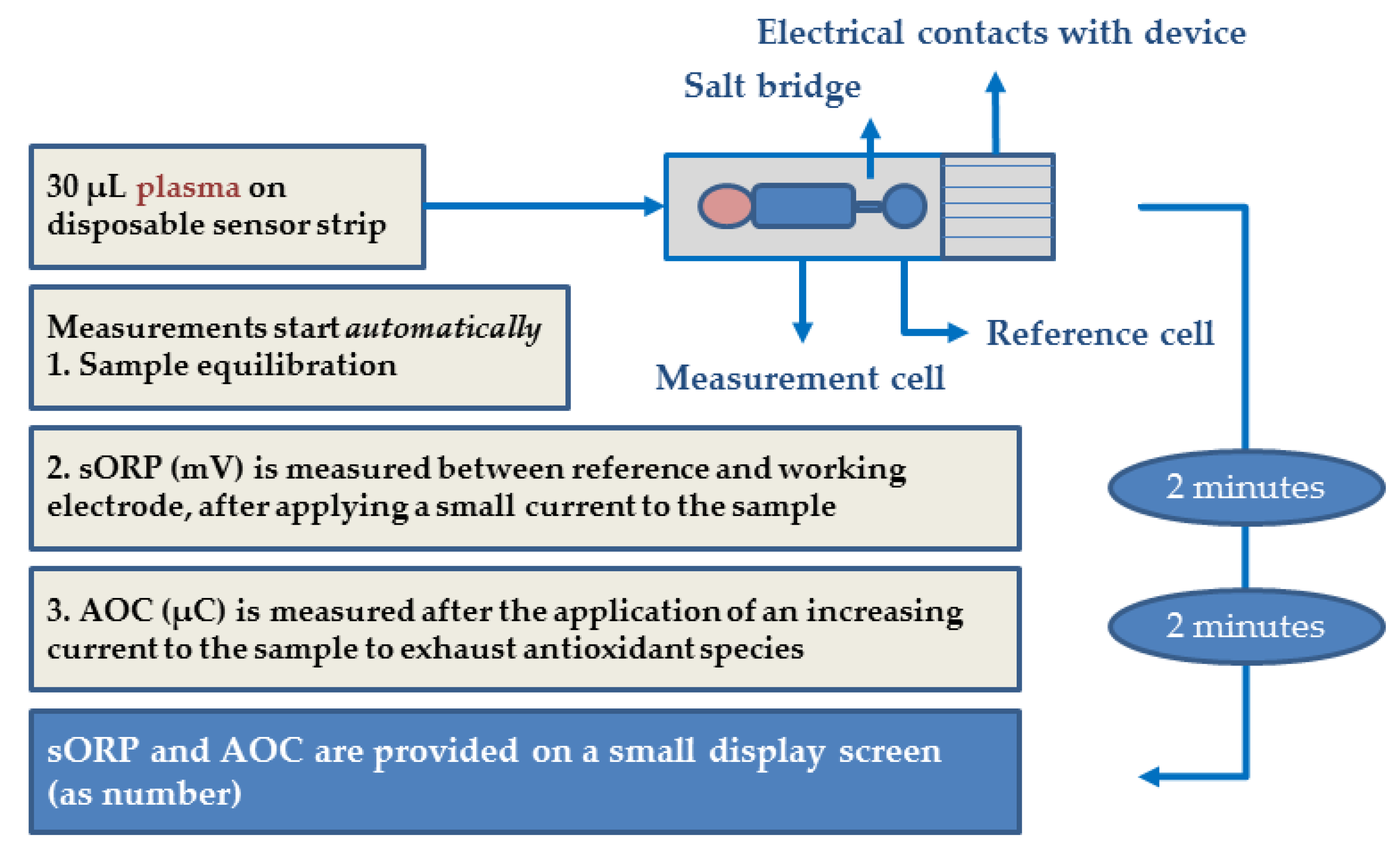
2.5. sORP and AOC Measurements
2.6. Sample Collecting and Processing
2.7. Statistics
3. Results
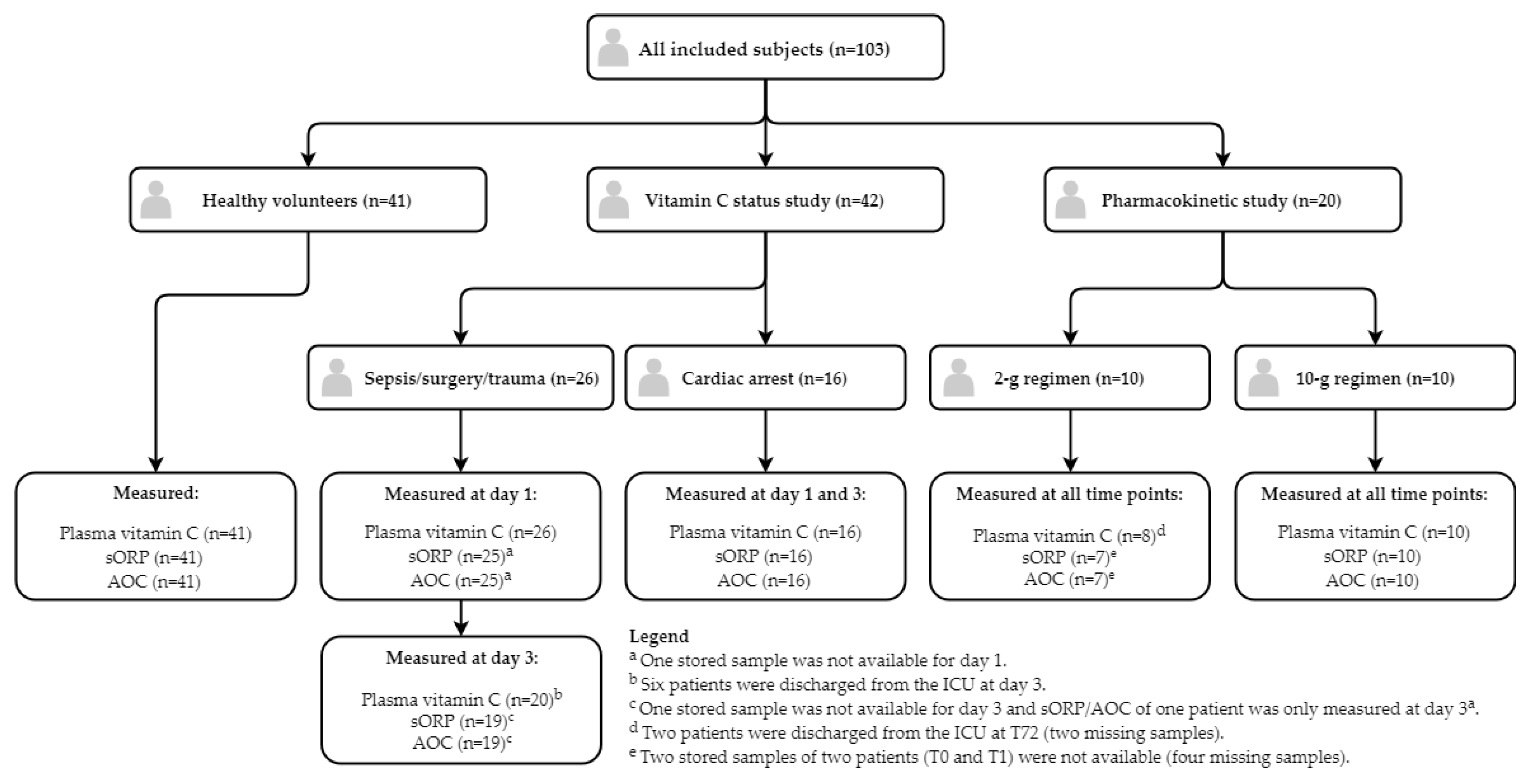
3.1. Study Measurements
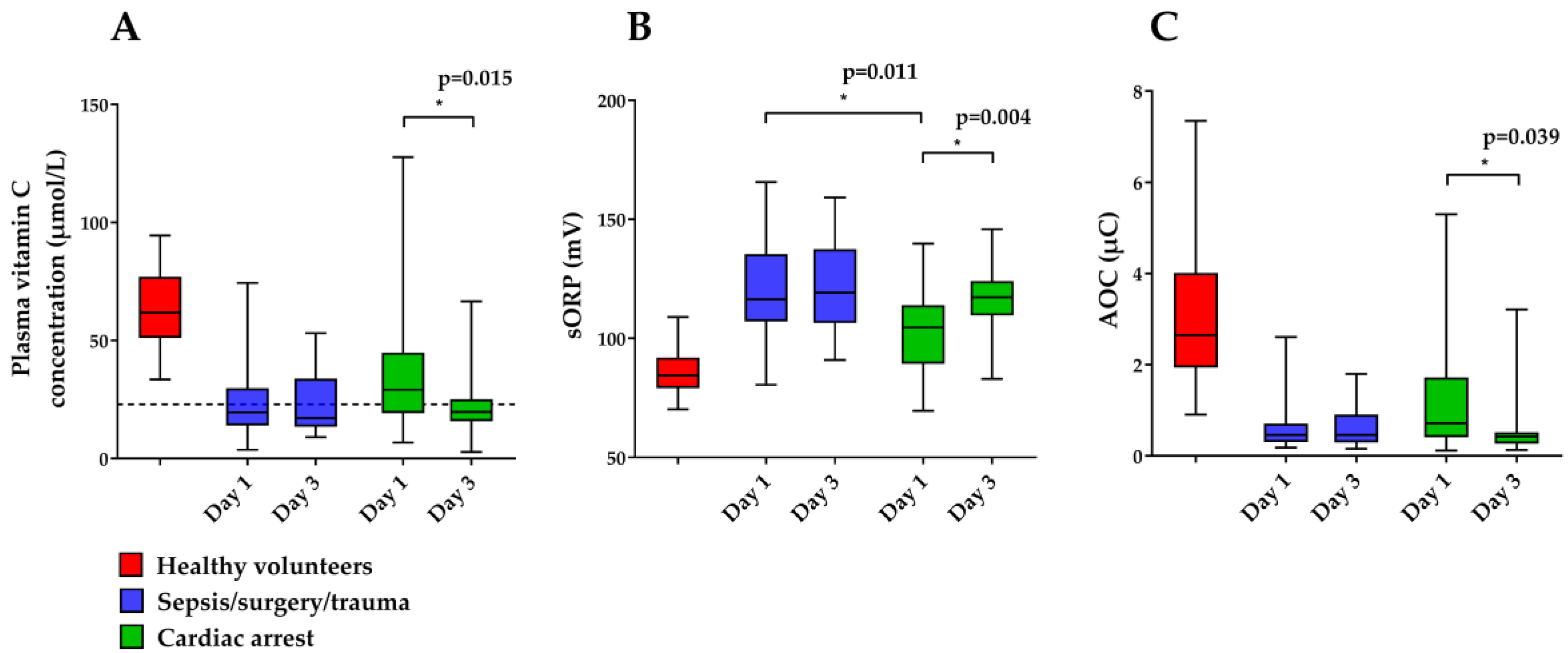
3.1.1. Vitamin C Status Study
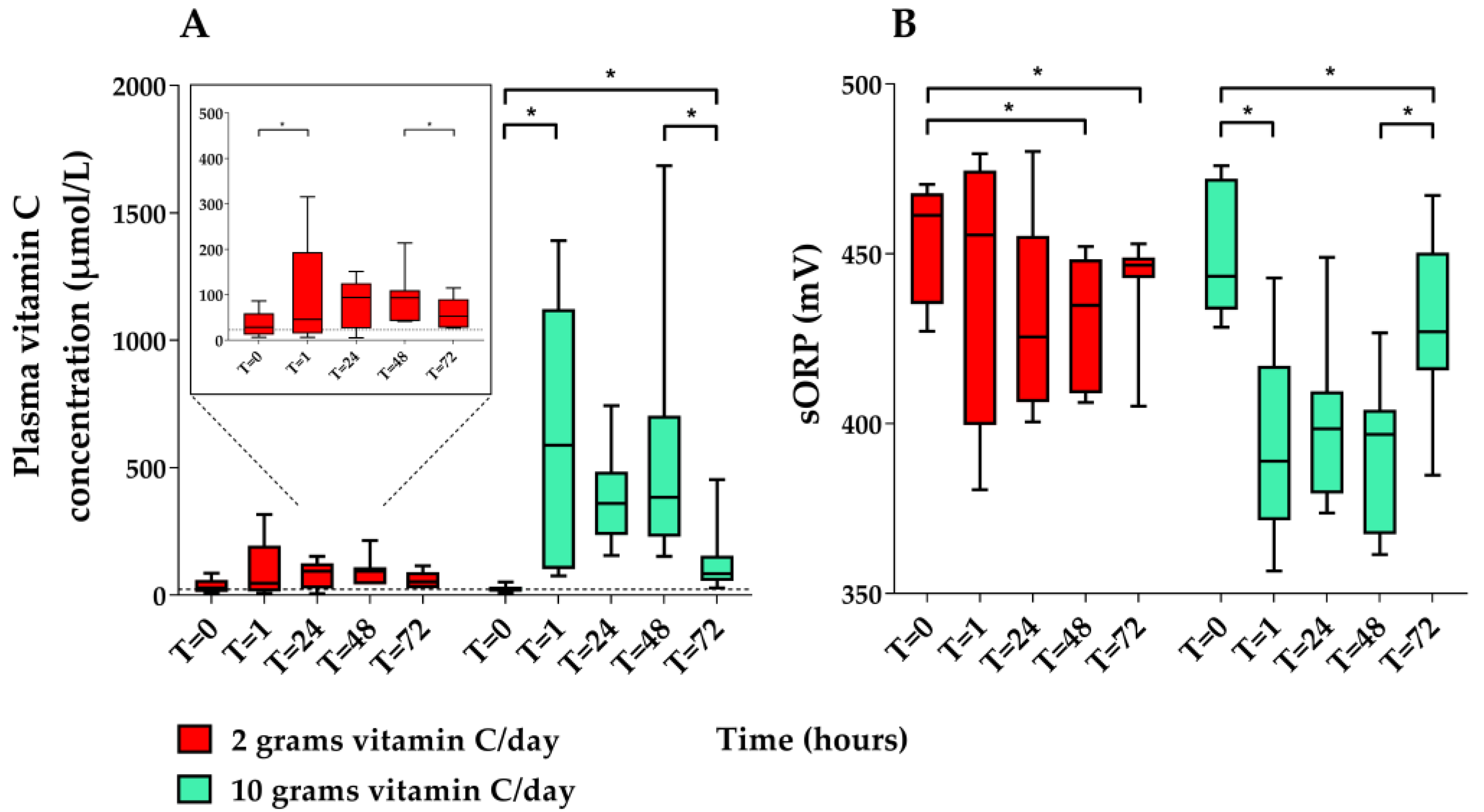
3.1.2. Pharmacokinetic study
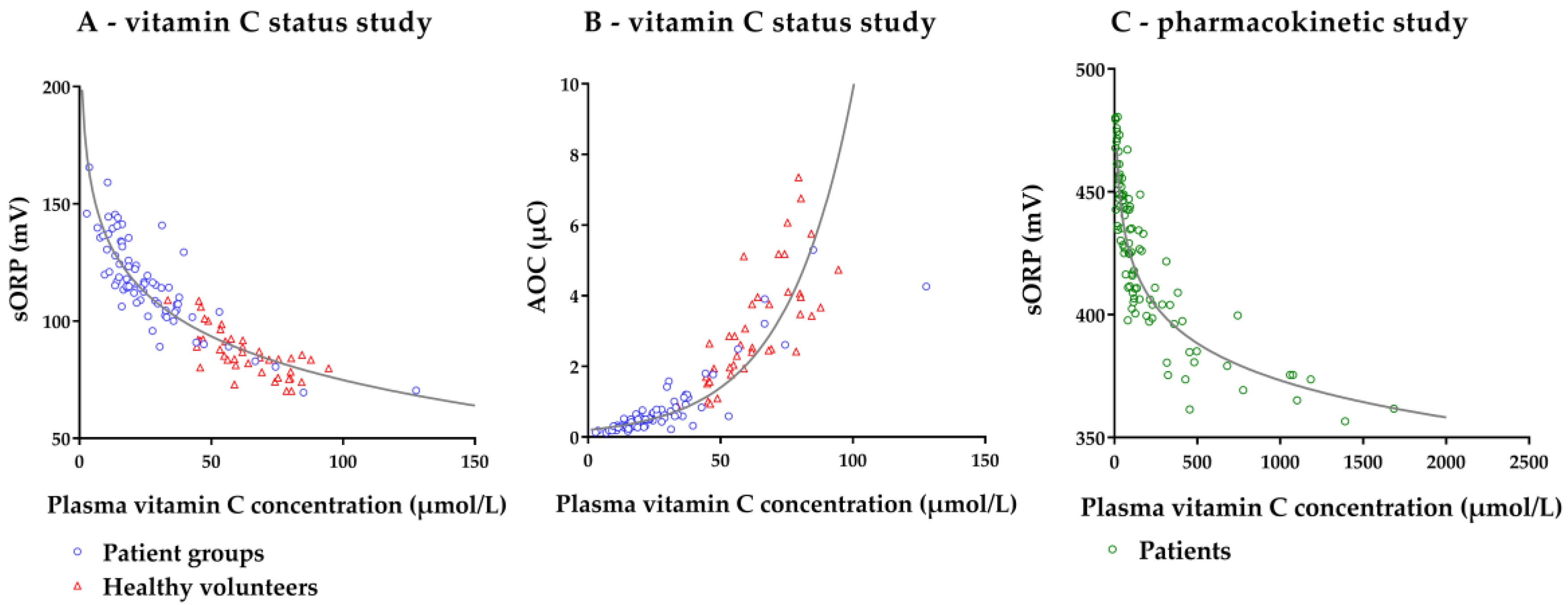
3.2. Association between Plasma Vitamin C Concentration and sORP/AOC
3.2.1. Vitamin C Status Study
3.2.2. Pharmacokinetic Study
3.3. Concordance between Changes in Plasma Vitamin C Concentration and Changes in ORP/AOC
3.3.1. Vitamin C Status Study
3.3.2. Pharmacokinetic Study
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Borrelli, E.; Roux-Lombard, P.; Grau, G.E.; Girardin, E.; Ricou, B.; Dayer, J.; Suter, P.M. Plasma concentrations of cytokines, their soluble receptors, and antioxidant vitamins can predict the development of multiple organ failure in patients at risk. Crit. Care Med. 1996, 24, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Grooth, H.J.; Spoelstra-de Man, A.M.E.; Oudemans-van Straaten, H.M. Early plasma vitamin c concentration, organ dysfunction and icu mortality. Intensive Care Med. 2014, 40 (Suppl. 1), S199. [Google Scholar]
- May, J.M.; Harrison, F.E. Role of vitamin c in the function of the vascular endothelium. Antioxid. Redox Signal. 2013, 19, 2068–2083. [Google Scholar] [CrossRef] [PubMed]
- Frei, B.; England, L.; Ames, B.N. Ascorbate is an outstanding antioxidant in human blood plasma. Proc. Natl. Acad. Sci. USA 1989, 86, 6377–6381. [Google Scholar] [CrossRef]
- Frei, B.; Stocker, R.; England, L.; Ames, B.N. Ascorbate: The most effective antioxidant in human plasma. Adv. Exp. Med. Biol. 1990, 264, 155–163. [Google Scholar] [PubMed]
- May, J.M. Vitamin c transport and its role in the central nervous system. Subcell Biochem. 2012, 56, 85–103. [Google Scholar] [PubMed]
- Carr, A.C.; Maggini, S. Vitamin c and immune function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef]
- Padayatty, S.J.; Levine, M. Vitamin C: The known and the unknown and goldilocks. Oral. Dis. 2016, 22, 463–493. [Google Scholar] [CrossRef]
- Oudemans-van Straaten, H.M.; Spoelstra-de Man, A.M.; de Waard, M.C. Vitamin c revisited. Crit. Care 2014, 18, 460. [Google Scholar] [CrossRef]
- Carr, A.C.; Rosengrave, P.C.; Bayer, S.; Chambers, S.; Mehrtens, J.; Shaw, G.M. Hypovitaminosis c and vitamin c deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care 2017, 21, 300. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Hooper, M.H. Doctor-your septic patients have scurvy! Crit. Care 2018, 22, 23. [Google Scholar] [CrossRef] [PubMed]
- Spoelstra-de Man, A.M.E.; Elbers, P.W.G.; Oudemans-van Straaten, H.M. Making sense of early high-dose intravenous vitamin c in ischemia/reperfusion injury. Crit. Care 2018, 22, 70. [Google Scholar] [CrossRef]
- Spoelstra-de Man, A.M.E.; Elbers, P.W.G.; Oudemans-Van Straaten, H.M. Vitamin C: Should we supplement? Curr. Opin. Crit. Care 2018, 24, 248–255. [Google Scholar] [CrossRef]
- Rael, L.T.; Bar-Or, R.; Kelly, M.T.; Carrick, M.M.; Bar-Or, D. Assessment of oxidative stress in patients with an isolated traumatic brain injury using disposable electrochemical test strips. Electroanalysis 2015, 27, 2567–2573. [Google Scholar] [CrossRef]
- Polson, D.; Villalba, N.; Freeman, K. Optimization of a diagnostic platform for oxidation-reduction potential (orp) measurement in human plasma. Redox. Rep. 2018, 23, 125–129. [Google Scholar] [CrossRef]
- Rael, L.T. Redoxsys™ Orp Scientific Data Synopsis; Luoxis Diagnostics, Inc.: Englewood, CO, USA, 2014. [Google Scholar]
- Bobe, G.; Cobb, T.J.; Leonard, S.W.; Aponso, S.; Bahro, C.B.; Koley, D.; Mah, E.; Bruno, R.S.; Traber, M.G. Increased static and decreased capacity oxidation-reduction potentials in plasma are predictive of metabolic syndrome. Redox. Biol. 2017, 12, 121–128. [Google Scholar] [CrossRef]
- Heldmaier, K.; Stoppe, C.; Goetzenich, A.; Foldenauer, A.C.; Zayat, R.; Breuer, T.; Schalte, G. Oxidation-reduction potential in patients undergoing transcatheter or surgical aortic valve replacement. Biomed. Res. Int. 2018, 2018, 8469383. [Google Scholar] [CrossRef] [PubMed]
- Rael, L.T.; Bar-Or, R.; Salottolo, K.; Mains, C.W.; Slone, D.S.; Offner, P.J.; Bar-Or, D. Injury severity and serum amyloid a correlate with plasma oxidation-reduction potential in multi-trauma patients: A retrospective analysis. Scand. J. Trauma Resusc. Emerg. Med. 2009, 17, 57. [Google Scholar] [CrossRef]
- Bjugstad, K.B.; Rael, L.T.; Levy, S.; Carrick, M.; Mains, C.W.; Slone, D.S.; Bar-Or, D. Oxidation-reduction potential as a biomarker for severity and acute outcome in traumatic brain injury. Oxid. Med. Cell. Longev. 2016, 6974257. [Google Scholar] [CrossRef]
- Bjugstad, K.B.; Lalama, J.; Rael, L.T.; Salottolo, K.; Dauber, I.; Bar-Or, D. Poor acute outcome in congestive heart failure is associated with increases in the plasma static oxidation-reduction potentials (sorp) in men but not in women. Redox. Rep. 2017, 22, 534–541. [Google Scholar] [CrossRef]
- Rael, L.T.; Bar-Or, R.; Mains, C.W.; Slone, D.S.; Levy, A.S.; Bar-Or, D. Plasma oxidation-reduction potential and protein oxidation in traumatic brain injury. J. Neurotrauma 2009, 26, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Bar-Or, D.; Bar-Or, R.; Rael, L.T.; Brody, E.N. Oxidative stress in severe acute illness. Redox. Biol. 2015, 4, 340–345. [Google Scholar] [CrossRef] [Green Version]
- Rael, L.T.; Bar-Or, R.; Aumann, R.M.; Slone, D.S.; Mains, C.W.; Bar-Or, D. Oxidation-reduction potential and paraoxonase-arylesterase activity in trauma patients. Biochem. Biophys. Res. Commun. 2007, 361, 561–565. [Google Scholar] [CrossRef]
- Spanidis, Y.; Goutzourelas, N.; Stagos, D.; Kolyva, A.S.; Gogos, C.A.; Bar-Or, D.; Kouretas, D. Assessment of oxidative stress in septic and obese patients using markers of oxidation-reduction potential. Athens Greece 2015, 29, 595–600. [Google Scholar]
- De Grooth, H.J.; Manubulu-Choo, W.P.; Zandvliet, A.S.; Spoelstra-de Man, A.M.E.; Girbes, A.R.; Swart, E.L.; Oudemans-van Straaten, H.M. Vitamin-c pharmacokinetics in critically ill patients: A randomized trial of four intravenous regimens. Chest 2018, 153, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Zhi, L.; Liang, J.; Hu, X.; Xu, J.; Yu, C.; Shao, H.; Pan, X.; Han, C. The reliability of clinical dynamic monitoring of redox status using a new redox potential (orp) determination method. Redox. Rep. 2013, 18, 63–70. [Google Scholar] [CrossRef]
- Winkler, B.S. Unequivocal evidence in support of the nonenzymatic redox coupling between glutathione/glutathione disulfide and ascorbic acid/dehydroascorbic acid. Biochim. Biophys. Acta BBA Gen. Subj. 1992, 1117, 287–290. [Google Scholar] [CrossRef]
- Buettner, G.R.; Jurkiewicz, B.A. Catalytic metals, ascorbate and free radicals: Combinations to avoid. Radiat. Res. 1996, 145, 532–541. [Google Scholar] [CrossRef]
- Buettner, G.R. The pecking order of free radicals and antioxidants: Lipid peroxidation, α-tocopherol, and ascorbate. Archives Biochem. Biophysics 1993, 300, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Curhan, G.; Forman, J.P.; Ascherio, A.; Choi, H.K. Vitamin c intake and serum uric acid concentration in men. J. Rheumatol. 2008, 35, 1853–1858. [Google Scholar]
- Evans, R.M.; Currie, L.; Campbell, A. The distribution of ascorbic acid between various cellular components of blood, in normal individuals, and its relation to the plasma concentration. Br. J. Nutr. 1982, 47, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Simcock, J.W.; Vissers, M.C. Human skeletal muscle ascorbate is highly responsive to changes in vitamin c intake and plasma concentrations. Am. J. Clin. Nutr. 2013, 97, 800–807. [Google Scholar] [CrossRef] [PubMed]
- Margolis, S.A.; Duewer, D.L. Measurement of ascorbic acid in human plasma and serum: Stability, intralaboratory repeatability, and interlaboratory reproducibility. Clin. Chem. 1996, 42, 1257–1262. [Google Scholar] [PubMed]
- Comstock, G.W.; Norkus, E.P.; Hoffman, S.C.; Xu, M.W.; Helzlsouer, K.J. Stability of ascorbic acid, carotenoids, retinol, and tocopherols in plasma stored at -70 degrees c for 4 years. Cancer Epidemiol. Biomark. Prev. 1995, 4, 505–507. [Google Scholar]
- Karlsen, A.; Blomhoff, R.; Gundersen, T.E. Stability of whole blood and plasma ascorbic acid. Eur. J. Clin. Nutr. 2007, 61, 1233–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vitamin C Status Study | Pharmacokinetic Study | |
|---|---|---|
| Blood tubes | Heparinized | Heparinized |
| Centrifuging | 10 min 1800 RPM | 10 min 1800 RPM |
| Plasma processing | Not further processed before storage at −80 °C | Acidified before storage at −80 °C |
| Time to sORP/AOC measurements | 5–6 years after storage at −80 °C | 2-3 years after storage at −80 °C |
| Time points sORP/AOC measurements | Once for healthy subjects Day 1 and day 3 for patients | T = 0, 1, 24, 48 and 72 |
| Vitamin C Status Study | |||
| Healthy volunteers | Total (n = 41) | ||
| Age (years) | 42 (27–49) | ||
| Sex, male (%) | 12 (29.3) | ||
| BMI (kg/m2) | 22.0 (20.3–25.6) | ||
| Plasma vitamin C concentration (µmol/L) a | 63.3 ± 14.8 | ||
| Patients | Total (n = 42) | Sepsis/surgery/trauma (n = 26) | Cardiac Arrest (n = 16) |
| Age (years) | 61 (48–76) | 57 (33–76) | 63 (53–77) |
| Sex, male (%) | 27 (64.3) | 15 (57.7) | 12 (75.0) |
| BMI (kg/m2) | 25.3 (22.4–27.6) | 24.9 (22.0–26.7) | 25.8 (23.3–28.2) |
| SOFA day 1 b | 7 ± 3 | 7 ± 4 | 6 ± 2 |
| Lactate day 1 (mmol/L) c | 2.4 (1.7–4.9) | 2.5 (1.4–5.5) | 2.3 (1.7–4.9) |
| Plasma vitamin C concentration (µmol/L) a | 25.3 (16.0–36.0) | 22.4 (13.6–32.9) | 29.2 (19.3–44.9) |
| Pharmacokinetic Study | |||
| Patients | Total (n = 20) | 2 g vitamin C/day (n = 10) | 10 g vitamin C/day (n = 10) |
| Age (years) | 64 (58–78) | 63 (53–78) | 66 (55–77) |
| Sex, male (%) | 13 (65.0) | 6 (60.0) | 7 (70.0) |
| BMI (kg/m2) | 27.4 ± 5.8 | 29.0 ± 6.7 | 25.8 ± 4.7 |
| SOFA at admission b | 7 (7–10) | 8 (7–9) | 7 (7–11) |
| Lactate T = 0 (mmol/L) | 1.5 (1.1–1.8) | 1.5 (1.0–2.2) | 1.5 (1.2–1.7) |
| Plasma vitamin C concentration (µmol/L) a | 22.7 (14.7–39.5) | 26.7 (14.1–47.5) | 19.3 (14.3–33.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozemeijer, S.; Spoelstra-de Man, A.M.E.; Coenen, S.; Smit, B.; Elbers, P.W.G.; de Grooth, H.-J.; Girbes, A.R.J.; Oudemans-van Straaten, H.M. Estimating Vitamin C Status in Critically Ill Patients with a Novel Point-of-Care Oxidation-Reduction Potential Measurement. Nutrients 2019, 11, 1031. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051031
Rozemeijer S, Spoelstra-de Man AME, Coenen S, Smit B, Elbers PWG, de Grooth H-J, Girbes ARJ, Oudemans-van Straaten HM. Estimating Vitamin C Status in Critically Ill Patients with a Novel Point-of-Care Oxidation-Reduction Potential Measurement. Nutrients. 2019; 11(5):1031. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051031
Chicago/Turabian StyleRozemeijer, Sander, Angélique M. E. Spoelstra-de Man, Sophie Coenen, Bob Smit, Paul W. G. Elbers, Harm-Jan de Grooth, Armand R. J. Girbes, and Heleen M. Oudemans-van Straaten. 2019. "Estimating Vitamin C Status in Critically Ill Patients with a Novel Point-of-Care Oxidation-Reduction Potential Measurement" Nutrients 11, no. 5: 1031. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11051031