Physical Activity and/or High Protein Intake Maintains Fat-Free Mass in Older People with Mild Disability; the Fukuoka Island City Study: A Cross-Sectional Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
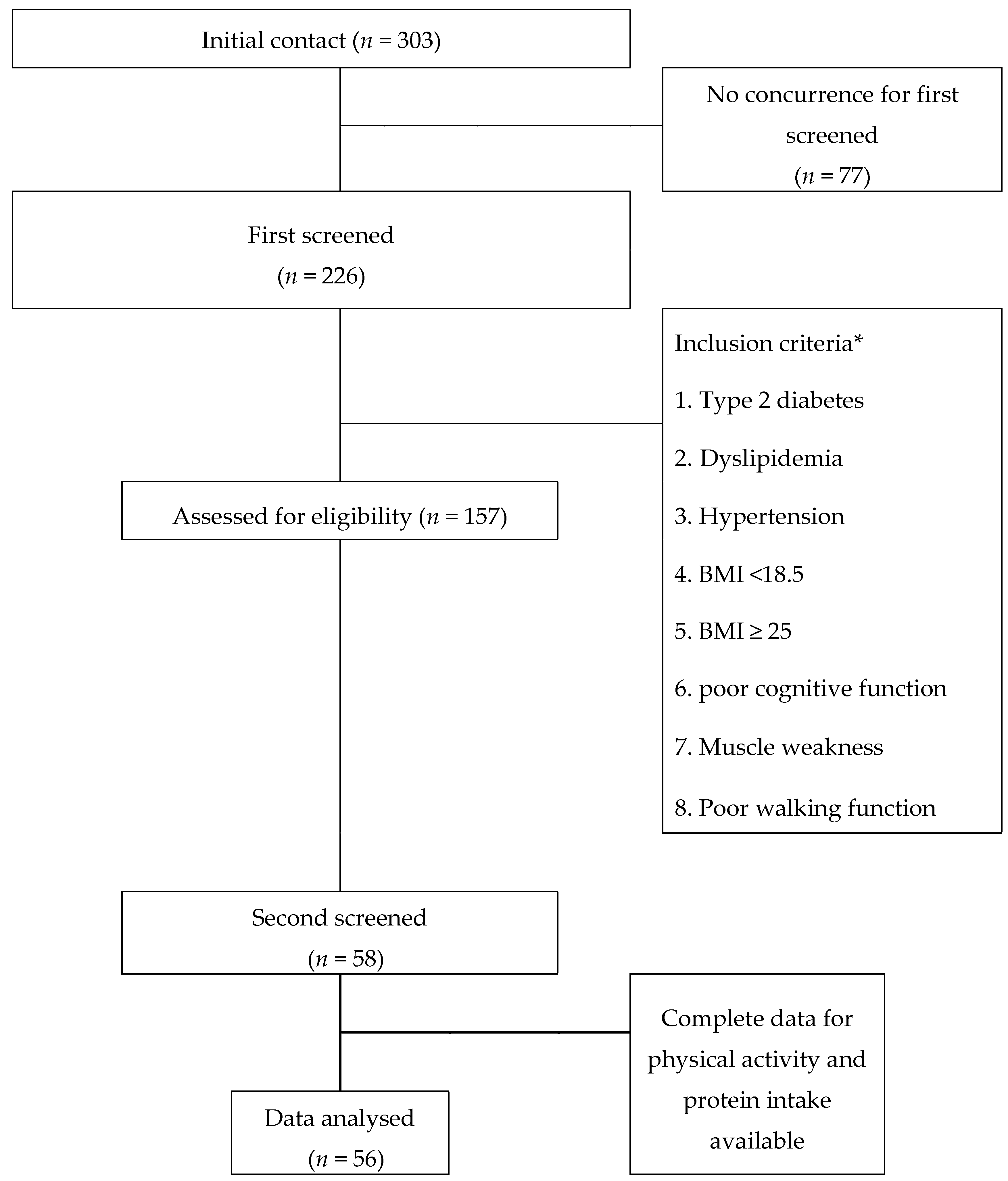
2.1. Participants
2.2. Anthropometric and Body Composition Measurements
2.3. Energy Expenditure and PA
2.4. Dietary Assessment
2.5. Inclusion and Exclusion from the Participants
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Levels of Physical Activity and Protein Intake by Participants
4.2. The Relationship between FFM and Physical Activity
4.3. The Relationship between FFM and Protein Intake
4.4. The Relationship between FFM and a Combination of Protein Intake and Physical Activity
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Janssen, I.; Heymsfield, S.B.; Wang, Z.M.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. (1985) 2000, 89, 81–88. [Google Scholar] [CrossRef]
- Hirani, V.; Blyth, F.; Naganathan, V.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Sarcopenia is associated with incident disability, institutionalization, and mortality in community-dwelling older men: The concord health and ageing in men project. J. Am. Med. Dir. Assoc. 2015, 16, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: Results from ilSIRENTE study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, L.M.; Lepkowski, J.M.; Imanaka, Y. Comorbidity and its impact on disability. Milbank Q. 1989, 67, 450–484. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, R.E.; Lang, I.A.; Llewellyn, D.J.; Rockwood, K. Frailty, body mass index, and abdominal obesity in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 65, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef] [PubMed]
- St-Jean-Pelletier, F.; Pion, C.H.; Leduc-Gaudet, J.P.; Sgarioto, N.; Zovile, I.; Barbat-Artigas, S.; Reynaud, O.; Alkaterji, F.; Lemieux, F.C.; Grenon, A.; et al. The impact of ageing, physical activity, and pre-frailty on skeletal muscle phenotype, mitochondrial content, and intramyocellular lipids in men. J. Cachexia Sarcopenia Muscle 2017, 8, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Rennie, M.J. Anabolic resistance: The effects of aging, sexual dimorphism, and immobilization on human muscle protein turnover. Appl. Physiol. Nutr. Metab. 2009, 34, 377–381. [Google Scholar] [CrossRef]
- Cuthbertson, D.; Smith, K.; Babraj, J.; Leese, G.; Waddell, T.; Atherton, P.; Wackerhage, H.; Taylor, P.M.; Rennie, M.J. Anabolic signaling deficits underlie amino acid resistance of wasting, aging muscle. FASEB J. 2005, 19, 422–424. [Google Scholar] [CrossRef]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Ministry of Health Labour Welfare. Dietary Reference Intakes for Japanese; Ministry of Health Labour Welfare: Tokyo, Japan, 2015. [Google Scholar]
- Phillips, S.M.; Chevalier, S.; Leidy, H.J. Protein “requirements” beyond the RDA: Implications for optimizing health. Appl. Physiol. Nutr. Metab. 2016, 41, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Houston, D.K.; Tooze, J.A.; Garcia, K.; Visser, M.; Rubin, S.; Harris, T.B.; Newman, A.B.; Kritchevsky, S.B.; Health, A.B.C.S. Protein intake and mobility limitation in community-dwelling older adults: The health ABC study. J. Am. Geriatr. Soc. 2017, 65, 1705–1711. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cermak, N.M.; Res, P.T.; de Groot, L.C.; Saris, W.H.; van Loon, L.J. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: A meta-analysis. Am. J. Clin. Nutr. 2012, 96, 1454–1464. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Otobe, Y.; Tanaka, T.; Ohji, S.; Koyama, S.; Sato, A.; Suzuki, M.; et al. Synergistic effect of bodyweight resistance exercise and protein supplementation on skeletal muscle in sarcopenic or dynapenic older adults. Geriatr. Gerontol. Int. 2019, 19, 429–437. [Google Scholar] [CrossRef]
- Morris, M.S.; Jacques, P.F. Total protein, animal protein and physical activity in relation to muscle mass in middle-aged and older Americans. Br. J. Nutr. 2013, 109, 1294–1303. [Google Scholar] [CrossRef]
- Kato, S. Development of the revised version of Hasegawa’s Dementia Scale (HDS-R). Jpn. Geriatr. Psychiatr. Med. 1991, 2, 1339–1347. [Google Scholar]
- Inoue, M.; Jinbo, D.; Nakamura, Y.; Taniguchi, M.; Urakami, K. Development and evaluation of a computerized test battery for Alzheimer’s disease screening in community-based settings. Am. J. Alzheimers Dis. Other Demen. 2009, 24, 129–135. [Google Scholar] [CrossRef]
- Urakami, K. Diagnostic biomarker for early stage of Alzheimer’s disease: Current state and view in the future. Psychogeriatrics 2010, 10, 49–52. [Google Scholar] [CrossRef]
- Shimokata, H.; Ando, F. Association of daily physical performance with muscle volume and strength. Geriatr. Gerontol. Int. 2012, 49, 195–198. (In Japanese) [Google Scholar] [Green Version]
- Hewitt, M.J.; Going, S.B.; Williams, D.P.; Lohman, T.G. Hydration of the fat-free body mass in children and adults: Implications for body composition assessment. Am. J. Physiol. 1993, 265, E88–E95. [Google Scholar] [CrossRef]
- Yamada, Y.; Yokoyama, K.; Noriyasu, R.; Osaki, T.; Adachi, T.; Itoi, A.; Naito, Y.; Morimoto, T.; Kimura, M.; Oda, S. Light-intensity activities are important for estimating physical activity energy expenditure using uniaxial and triaxial accelerometers. Eur. J. Appl. Physiol. 2009, 105, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, M.; Normand, S.; Pachiaudi, C.; Lacour, J.R.; Laville, M.; Kostka, T. Simultaneous validation of ten physical activity questionnaires in older men: A doubly labeled water study. J. Am. Geriatr. Soc. 2001, 49, 28–35. [Google Scholar] [CrossRef] [PubMed]
- DeLany, J.P.; Schoeller, D.A.; Hoyt, R.W.; Askew, E.W.; Sharp, M.A. Field use of D2 18O to measure energy expenditure of soldiers at different energy intakes. J. Appl. Physiol. (1985) 1989, 67, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Hashii-Arishima, Y.; Yokoyama, K.; Itoi, A.; Adachi, T.; Kimura, M. Validity of a triaxial accelerometer and simplified physical activity record in older adults aged 64–96 years: A doubly labeled water study. Eur. J. Appl. Physiol. 2018, 118, 2133–2146. [Google Scholar] [CrossRef]
- Ikenaga, M.; Yamada, Y.; Takeda, N.; Kimura, M.; Higaki, Y.; Tanaka, H.; Kiyonaga, A.; Nakagawa Study, G. Dynapenia, gait speed and daily physical activity measured using triaxial accelerometer in older Japanese men. J. Phys. Fit. Sports Med. 2014, 3, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Michishita, R.; Fukae, C.; Mihara, R.; Ikenaga, M.; Morimura, K.; Takeda, N.; Yamada, Y.; Higaki, Y.; Tanaka, H.; Kiyonaga, A.; et al. Association between the physical activity and heart rate corrected-QT interval in older adults. Geriatr. Gerontol. Int. 2015, 15, 895–901. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- Maeda, K.; Higashimoto, Y.; Honda, N.; Shiraishi, M.; Hirohata, T.; Minami, K.; Iwasaki, T.; Chiba, Y.; Yamagata, T.; Terada, K. Effect of a postoperative outpatient pulmonary rehabilitation program on physical activity in patients who underwent pulmonary resection for lung cancer. Geriatr. Gerontol. Int. 2016, 16, 550–555. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Nyström, C.D.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Ganpule, A.A.; Tanaka, S.; Ishikawa-Takata, K.; Tabata, I. Interindividual variability in sleeping metabolic rate in Japanese subjects. Eur. J. Clin. Nutr. 2007, 61, 1256–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, Y.; Oshikata, R.; Miyamoto, N.; Kishida, R.; Nagata, A.; Terazawa, Y.; Hirakawa, F.; Yoshimura, Y.; Imamura, H. Validity of 1-, 2-, 3-, and 4-day dietary records in comparison with 7-day weighed dietary records. Health Eval. Promot. 2010, 37, 405–413. [Google Scholar]
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-administered diet history questionnaire developed for health education: A relative validation of the test-version by comparison with 3-day diet record in women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Rhee, J.J.; Sampson, L.; Cho, E.; Hughes, M.D.; Hu, F.B.; Willett, W.C. Comparison of methods to account for implausible reporting of energy intake in epidemiologic studies. Am. J. Epidemiol. 2015, 181, 225–233. [Google Scholar] [CrossRef]
- Gibson, R.; Eriksen, R.; Lamb, K.; McMeel, Y.; Vergnaud, A.-C.; Spear, J.; Aresu, M.; Chan, Q.; Elliott, P.; Frost, G. Dietary assessment of British police force employees: A description of diet record coding procedures and cross-sectional evaluation of dietary energy intake reporting (the airwave health monitoring study). BMJ Open 2017, 7, e012927. [Google Scholar] [CrossRef]
- Ishikawa-Takata, K.; Naito, Y.; Tanaka, S.; Ebine, N.; Tabata, I. Use of doubly labeled water to validate a physical activity questionnaire developed for the Japanese population. J. Epidemiol. 2011, 21, 114–121. [Google Scholar] [CrossRef]
- Kobayashi, S.; Asakura, K.; Suga, H.; Sasaki, S. High protein intake is associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr. J. 2013, 12, 164. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; D’Angelo, E.; Sisto, A.; Marzetti, E. Protein intake and muscle health in old age: From biological plausibility to clinical evidence. Nutrients 2016, 8, 295. [Google Scholar] [CrossRef]
- Hernandez-Alonso, P.; Salas-Salvado, J.; Ruiz-Canela, M.; Corella, D.; Estruch, R.; Fito, M.; Aros, F.; Gomez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. High dietary protein intake is associated with an increased body weight and total death risk. Clin. Nutr. 2016, 35, 496–506. [Google Scholar] [CrossRef]
- Nilsson, A.; Montiel Rojas, D.; Kadi, F. Impact of meeting different guidelines for protein intake on muscle mass and physical function in physically active older women. Nutrients 2018, 10, 1156. [Google Scholar] [CrossRef]
- Isanejad, M.; Mursu, J.; Sirola, J.; Kroger, H.; Rikkonen, T.; Tuppurainen, M.; Erkkila, A.T. Dietary protein intake is associated with better physical function and muscle strength among elderly women. Br. J. Nutr. 2016, 115, 1281–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmerman, K.L.; Dhanani, S.; Glynn, E.L.; Fry, C.S.; Drummond, M.J.; Jennings, K.; Rasmussen, B.B.; Volpi, E. A moderate acute increase in physical activity enhances nutritive flow and the muscle protein anabolic response to mixed nutrient intake in older adults. Am. J. Clin. Nutr. 2012, 95, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Russo, A.; Cesari, M.; Pahor, M.; Liperoti, R.; Danese, P.; Bernabei, R.; Onder, G. Walking one hour or more per day prevented mortality among older persons: Results from ilSIRENTE study. Prev. Med. 2008, 47, 422–426. [Google Scholar] [CrossRef]
- Speakman, J.R.; Westerterp, K.R. Associations between energy demands, physical activity, and body composition in adult humans between 18 and 96 y of age. Am. J. Clin. Nutr. 2010, 92, 826–834. [Google Scholar] [CrossRef] [Green Version]
- Foong, Y.C.; Chherawala, N.; Aitken, D.; Scott, D.; Winzenberg, T.; Jones, G. Accelerometer-determined physical activity, muscle mass, and leg strength in community-dwelling older adults. J. Cachexia Sarcopenia Muscle 2016, 7, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Park, S.; Shephard, R.J.; Aoyagi, Y. Yearlong physical activity and sarcopenia in older adults: The Nakanojo Study. Eur. J. Appl. Physiol. 2010, 109, 953–961. [Google Scholar] [CrossRef]
- Raguso, C.A.; Kyle, U.; Kossovsky, M.P.; Roynette, C.; Paoloni-Giacobino, A.; Hans, D.; Genton, L.; Pichard, C. A 3-year longitudinal study on body composition changes in the elderly: Role of physical exercise. Clin. Nutr. 2006, 25, 573–580. [Google Scholar] [CrossRef]
- Pannemans, D.L.; Westerterp, K.R. Energy expenditure, physical activity and basal metabolic rate of elderly subjects. Br. J. Nutr. 1995, 73, 571–581. [Google Scholar] [CrossRef]
- Roberts, S.B.; Dallal, G.E. Energy requirements and aging. Public Health Nutr. 2005, 8, 1028–1036. [Google Scholar] [CrossRef] [Green Version]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef]
- Houston, D.K.; Nicklas, B.J.; Ding, J.; Harris, T.B.; Tylavsky, F.A.; Newman, A.B.; Lee, J.S.; Sahyoun, N.R.; Visser, M.; Kritchevsky, S.B. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: The Health, Aging, and Body Composition (Health ABC) Study. Am. J. Clin. Nutr. 2008, 87, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Martone, A.M.; Marzetti, E.; Calvani, R.; Picca, A.; Tosato, M.; Santoro, L.; Di Giorgio, A.; Nesci, A.; Sisto, A.; Santoliquido, A.; et al. Exercise and protein intake: A synergistic approach against sarcopenia. Biomed. Res. Int. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Verreijen, A.M.; Engberink, M.F.; Memelink, R.G.; van der Plas, S.E.; Visser, M.; Weijs, P.J. Effect of a high protein diet and/or resistance exercise on the preservation of fat free mass during weight loss in overweight and obese older adults: A randomized controlled trial. Nutr. J. 2017, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Breen, L.; Stokes, K.A.; Churchward-Venne, T.A.; Moore, D.R.; Baker, S.K.; Smith, K.; Atherton, P.J.; Phillips, S.M. Two weeks of reduced activity decreases leg lean mass and induces “anabolic resistance” of myofibrillar protein synthesis in healthy elderly. J. Clin. Endocrinol. Metab. 2013, 98, 2604–2612. [Google Scholar] [CrossRef] [PubMed]
- Pace, N.; Rathbun, E.N. Studies on body composition. 3. The body water and chemically combined nitrogen content in relation to fat content. J. Biol. Chem. 1945, 158, 685–691. [Google Scholar]
- Park, J.; Ishikawa-Takata, K.; Tanaka, S.; Hikihara, Y.; Ohkawara, K.; Watanabe, S.; Miyachi, M.; Morita, A.; Aiba, N.; Tabata, I. The relationship of body composition to daily physical activity in free-living Japanese adult men. Br. J. Nutr. 2014, 111, 182–188. [Google Scholar] [CrossRef]
- Miyake, M.; Kirisako, T.; Kokubo, T.; Miura, Y.; Morishita, K.; Okamura, H.; Tsuda, A. Randomised controlled trial of the effects of L-ornithine on stress markers and sleep quality in healthy workers. Nutr. J. 2014, 13, 53. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | All n = 56 | Men n = 17 | Women n = 39 | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age, years | 71.8 | 6.9 | 71.1 | 6.6 | 72.1 | 6.9 |
| Height, cm | 154 | 9 | 162.9 | 6.3 | 149.4 | 5.6 |
| Body weight, kg | 54.5 | 12.2 | 63.8 | 12.3 | 50.5 | 9.4 |
| Body mass index, kg/m2 | 23.0 | 3.8 | 23.9 | 3.3 | 22.6 | 3.9 |
| Fat-free mass, kg | 36.9 | 8.2 | 46.2 | 7.7 | 32.8 | 3.8 |
| Fat-free mass, % | 68.1 | 7.5 | 73.0 | 7.3 | 65.9 | 6.4 |
| Energy intake, kcal/day | 1814 | 327 | 2066 | 349 | 1704 | 240 |
| Energy expenditure, kcal/day | 1853 | 375 | 2126 | 440 | 1734 | 260 |
| Energy expenditure, kcal/kg/day | 34.5 | 5.3 | 33.5 | 4.5 | 34.9 | 5.5 |
| Nutritional parameter | ||||||
| Protein intake, g/day | 71.5 | 14.0 | 79.9 | 13.4 | 67.9 | 12.3 |
| Protein intake, g/kg BW/day | 1.28 | 0.32 | 1.25 | 0.28 | 1.29 | 0.33 |
| Protein intake, g/kg FFM/day | 1.99 | 0.40 | 1.75 | 0.29 | 2.09 | 0.40 |
| Fat intake, g/day | 57.4 | 15.6 | 62.6 | 13.1 | 55.1 | 15.8 |
| Carbohydrate intake, g/day | 239 | 41 | 271 | 40 | 225 | 32 |
| Protein source | ||||||
| Soy protein, g/day | 9.4 | 7.9 | 9.6 | 6.1 | 9.3 | 8.5 |
| Fish and shellfish protein, g/day | 12.4 | 6.9 | 14.0 | 5.3 | 11.7 | 6.4 |
| Meat protein, g/day | 12.2 | 6.9 | 14.4 | 7.3 | 11.2 | 6.4 |
| Egg protein, g/day | 4.8 | 3.0 | 5.5 | 2.9 | 4.5 | 2.9 |
| Milk protein, g/day | 19.5 | 14.5 | 21.1 | 17.8 | 18.8 | 12.5 |
| Other protein, g/day | 13.2 | 12.3 | 15.3 | 11.7 | 12.4 | 12.3 |
| Distribution of protein intake across eating occasions | ||||||
| Breakfast protein, g/meal | 16.5 | 6.2 | 17.5 | 6.7 | 16.0 | 5.8 |
| Lunch protein, g/meal | 21.3 | 6.6 | 22.2 | 7.2 | 21.0 | 6.2 |
| Supper protein, g/meal | 30.0 | 7.7 | 34.5 | 6.9 | 28.0 | 7.1 |
| Snack protein, g/meal | 3.8 | 5.5 | 5.8 | 6.7 | 2.9 | 4.5 |
| Physical activity parameter | ||||||
| PAL | 1.77 | 0.24 | 1.62 | 0.20 | 1.84 | 0.22 |
| Steps, counts/day | 6199 | 2747 | 6535 | 2903 | 6053 | 2626 |
| Sedentary, min/day | 200 | 46 | 167 | 39 | 214 | 40 |
| LPA, min/day | 332 | 87 | 259 | 53 | 364 | 78 |
| MVPA, min/day | 30 | 20 | 32 | 22 | 28 | 19 |
| Crude Values | Values Adjusted for Age and Sex | |||
|---|---|---|---|---|
| Parameter | r | p | r | p |
| Physical parameter | ||||
| Age, years | −0.198 | 0.144 | ||
| Height, cm | 0.236 | 0.080 | −0.191 | 0.167 |
| Body weight, kg | −0.321 | 0.016 | −0.719 | <0.001 |
| BMI, kg/m2 | −0.604 | <0.001 | −0.753 | <0.001 |
| Nutritional parameter | ||||
| Energy intake, kcal/day | 0.207 | 0.126 | -0.054 | 0.700 |
| Protein intake, g/day | 0.295 | 0.027 | 0.142 | 0.305 |
| Protein intake, g/kg/day | 0.541 | <0.001 | 0.652 | <0.001 |
| Fat intake, g/day | −0.026 | 0.853 | −0.192 | 0.163 |
| Carbohydrate intake, g/day | 0.215 | 0.111 | −0.042 | 0.765 |
| Physical activity parameter | ||||
| PAL | 0.122 | 0.372 | 0.345 | 0.011 |
| Steps, counts/day | 0.234 | 0.083 | 0.161 | 0.246 |
| Sedentary, min/day | −0.163 | 0.231 | 0.076 | 0.586 |
| LPA, min/day | −0.117 | 0.403 | 0.137 | 0.321 |
| MVPA, min/day | 0.389 | 0.003 | 0.350 | 0.009 |
| R2 | p Value | Included Independent Variables | Standardized Coefficient (β) | p Value | |
|---|---|---|---|---|---|
| Model 1 | 0.221 | <0.001 | Age | −0.167 | 0.176 |
| Sex | −0.428 | 0.001 | |||
| Model 2 | 0.314 | <0.001 | Age | −0.059 | 0.632 |
| Sex | −0.588 | <0.001 | |||
| PAL | 0.357 | 0.011 | |||
| Model 3 | 0.317 | <0.001 | Age | −0.020 | 0.879 |
| Sex | −0.407 | <0.001 | |||
| MVPA | 0.344 | 0.009 | |||
| Model 4 | 0.552 | <0.001 | Age | −0.175 | 0.066 |
| Sex | −0.467 | <0.001 | |||
| Protein intake | 0.576 | <0.001 | |||
| Model 5 | 0.611 | <0.001 | Age | −0.088 | 0.348 |
| Sex | −0.593 | <0.001 | |||
| PAL | 0.287 | 0.008 | |||
| Protein intake | 0.550 | <0.001 | |||
| Model 6 | 0.599 | <0.001 | Age | −0.070 | 0.485 |
| Sex | −0.450 | < 0.001 | |||
| MVPA | 0.245 | 0.018 | |||
| Protein intake | 0.540 | < 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takae, R.; Hatamoto, Y.; Yasukata, J.; Kose, Y.; Komiyama, T.; Ikenaga, M.; Yoshimura, E.; Yamada, Y.; Ebine, N.; Higaki, Y.; et al. Physical Activity and/or High Protein Intake Maintains Fat-Free Mass in Older People with Mild Disability; the Fukuoka Island City Study: A Cross-Sectional Study. Nutrients 2019, 11, 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112595
Takae R, Hatamoto Y, Yasukata J, Kose Y, Komiyama T, Ikenaga M, Yoshimura E, Yamada Y, Ebine N, Higaki Y, et al. Physical Activity and/or High Protein Intake Maintains Fat-Free Mass in Older People with Mild Disability; the Fukuoka Island City Study: A Cross-Sectional Study. Nutrients. 2019; 11(11):2595. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112595
Chicago/Turabian StyleTakae, Rie, Yoichi Hatamoto, Jun Yasukata, Yujiro Kose, Takaaki Komiyama, Masahiro Ikenaga, Eiichi Yoshimura, Yosuke Yamada, Naoyuki Ebine, Yasuki Higaki, and et al. 2019. "Physical Activity and/or High Protein Intake Maintains Fat-Free Mass in Older People with Mild Disability; the Fukuoka Island City Study: A Cross-Sectional Study" Nutrients 11, no. 11: 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11112595