High Prevalence of Supplement Intake with a Concomitant Low Information Quality among Swiss Fitness Center Users


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Ethics
2.2. Inclusion and Exclusion Criteria
2.3. Questionnaire
2.4. Statistics
3. Results
3.1. Subjects
3.2. Supplement Intake
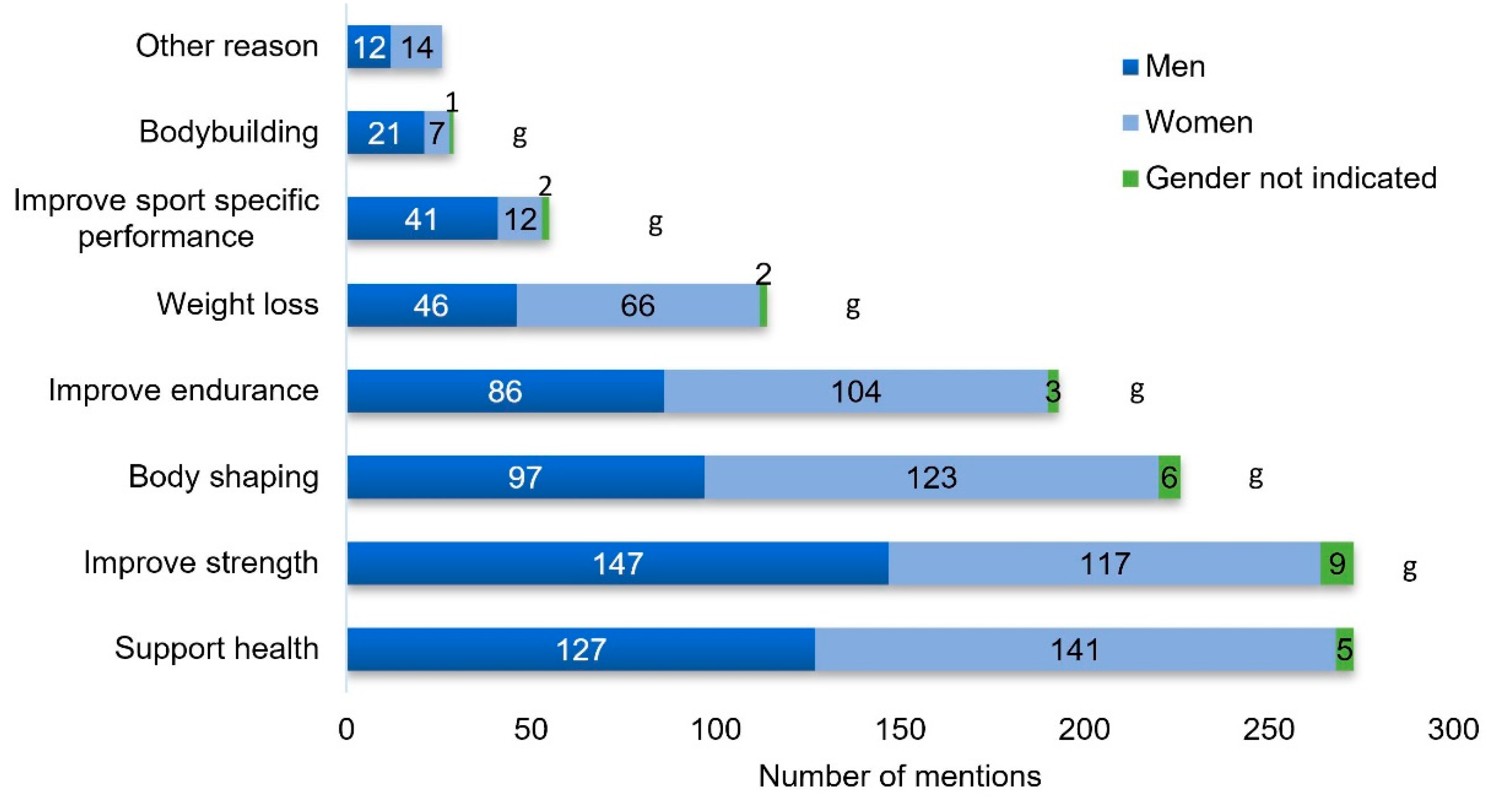
3.3. Training Goals
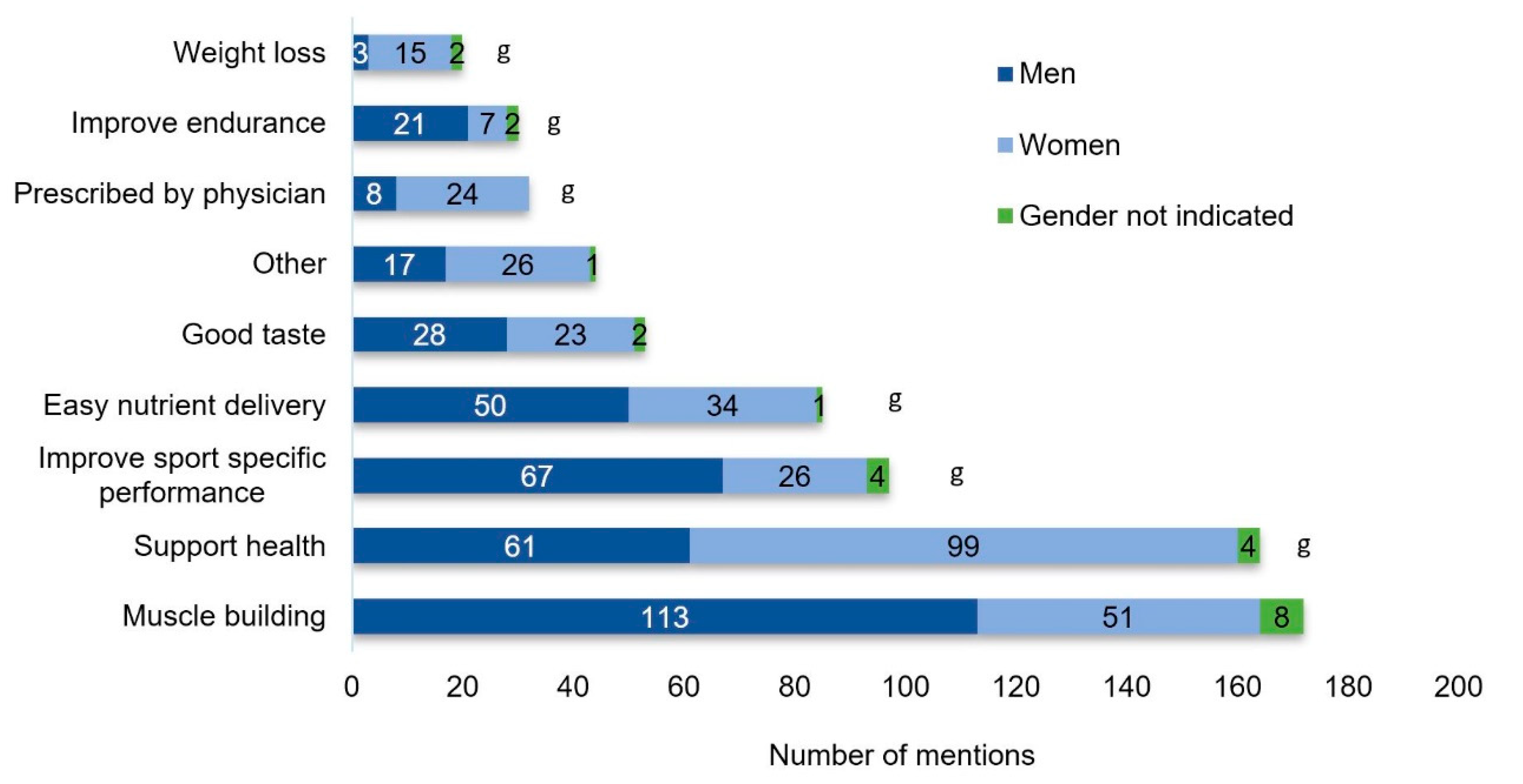
3.4. Reasons for Supplement Intake
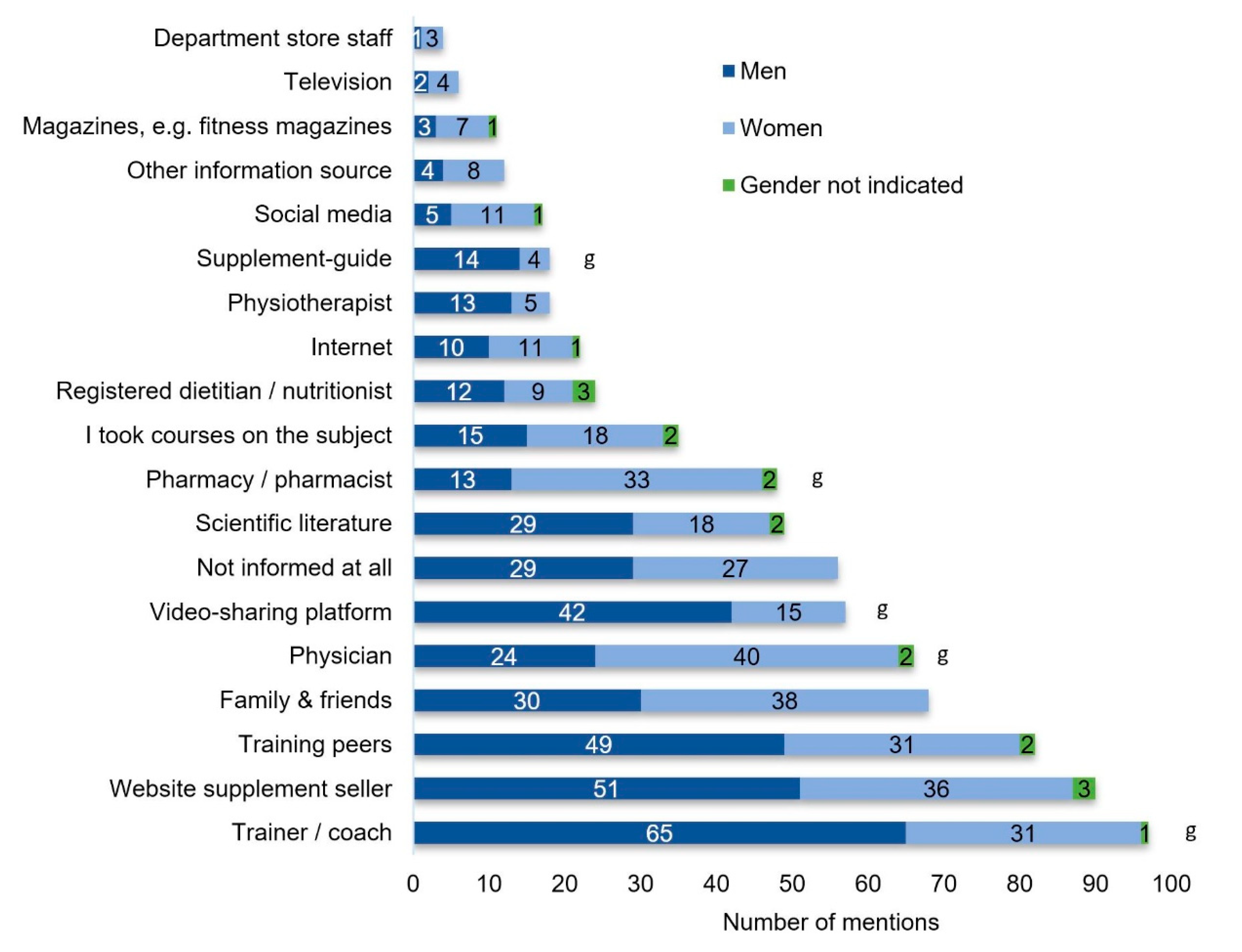
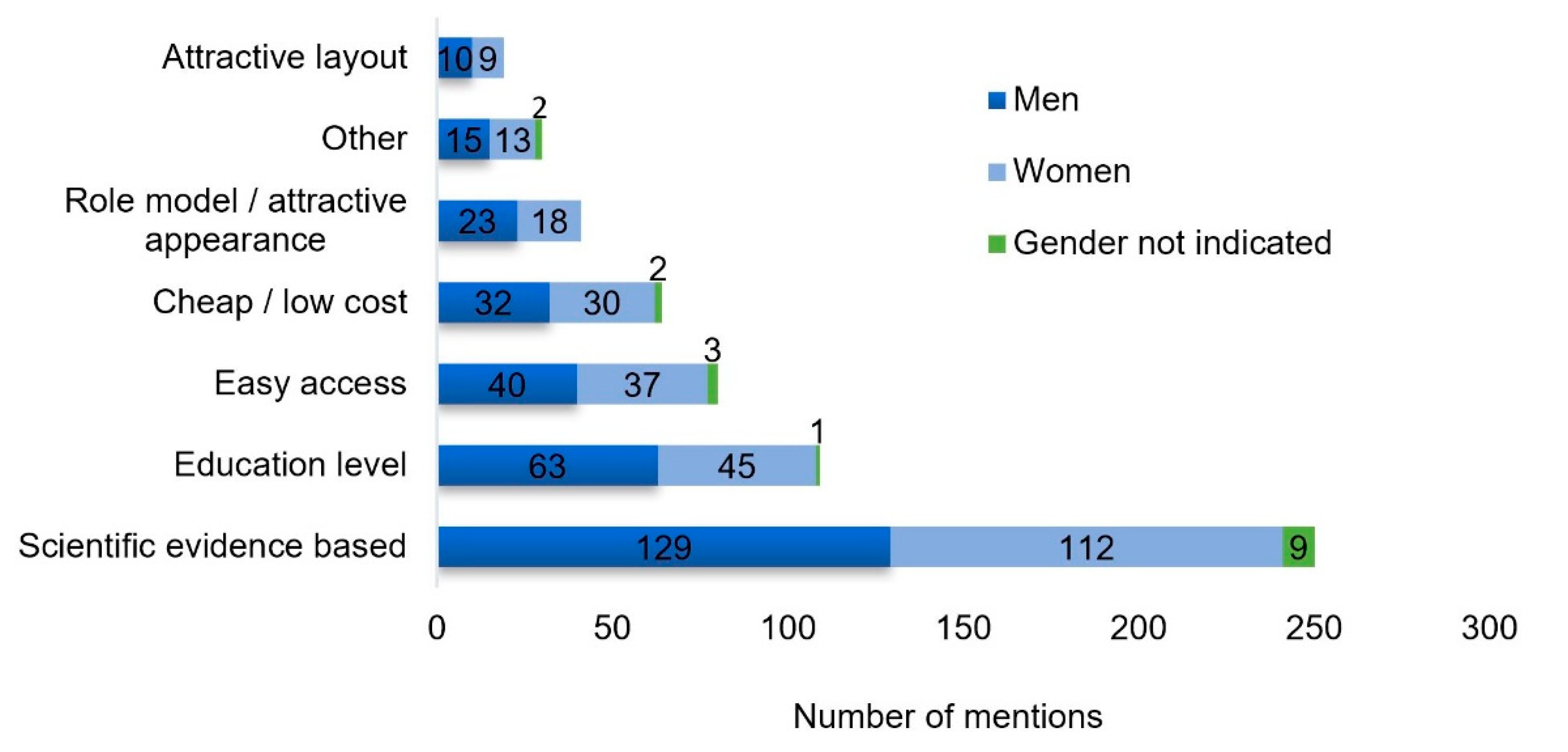
3.5. Information Sources
4. Discussion
4.1. Supplement Intake
4.2. Information Sources
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mettler, S.; Mannhart, C.; Colombani, P.C. Developement and validation of a food pyramid for swiss athletes. Int. J. Sport. Nutr. Exerc. Metab. 2009, 19, 504–518. [Google Scholar] [CrossRef] [PubMed]
- Larson-Meyer, D.E.; Woolf, K.; Burke, L. Assessment of nutrient status in athletes and the need for supplementation. Int. J. Sport. Nutr. Exerc. Metab. 2018, 28, 139–158. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef]
- Knapik, J.J.; Steelman, R.A.; Hoedebecke, S.S.; Austin, K.G.; Farina, E.K.; Lieberman, H.R. Prevalence of dietary supplement use by athletes: Systematic review and meta-analysis. Sports Med. 2016, 46, 103–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garthe, I.; Maughan, R.J. Athletes and supplements: Prevalence and perspectives. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 126–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques-Vidal, P.; Pecoud, A.; Hayoz, D.; Paccaud, F.; Mooser, V.; Waeber, G.; Vollenweider, P. Prevalence and characteristics of vitamin or dietary supplement users in Lausanne, Switzerland: The CoLaus study. Eur. J. Clin. Nutr. 2009, 63, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 104–125. [Google Scholar] [CrossRef] [Green Version]
- Maughan, R.J.; Shirreffs, S.M.; Vernec, A. Making decisions about supplement use. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 52, 439–455. [Google Scholar] [CrossRef]
- Maughan, R.J.; Depiesse, F.; Geyer, H. The use of dietary supplements by athletes. J. Sport. Sci. 2007, 25, S103–S113. [Google Scholar] [CrossRef]
- Maughan, R.J.; Greenhaff, P.L.; Hespel, P. Dietary supplements for athletes: Emerging trends and recurring themes. J. Sport Sci. 2011, 29, S57–S66. [Google Scholar] [CrossRef]
- Geyer, H.; Parr, M.K.; Koehler, K.; Mareck, U.; Schanzer, W.; Thevis, M. Nutritional supplements cross-contaminated and faked with doping substances. J. Mass. Spectrom. 2008, 43, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Bundesministerium für Ernährung, L.u.V. Nationale Verzehrs Studie II, Ergebnisbericht, Teil 1; Max Rubner-Institut: Karlsruhe, Germany, 2008.
- Bailey, R.L.; Gahche, J.J.; Lentino, C.V.; Dwyer, J.T.; Engel, J.S.; Thomas, P.R.; Betz, J.M.; Sempos, C.T.; Picciano, M.F. Dietary supplement use in the United States, 2003–2006. J. Nutr. 2011, 141, 261–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lun, V.; Erdman, K.A.; Fung, T.S.; Reimer, R.A. Dietary supplementation practices in Canadian high-performance athletes. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Braun, H.; Koehler, K.; Geyer, H.; Kleiner, J.; Mester, J.; Schanzer, W. Dietary supplement use among elite young german athletes. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 97–109. [Google Scholar] [CrossRef]
- Lamprecht, M.; Fischer, A.; Stamm, H.P. Sportaktivität und Sportinteresse der Schweizer Bevölkerung; Bundesamt für Sport BASPO: Magglingen, Switzerland, 2014. [Google Scholar]
- Abo Ali, E.A.; Elgamal, H.H. Use of dietary supplements among gym trainees in Tanta city, Egypt. J. Egypt. Public Health Assoc. 2016, 91, 185–191. [Google Scholar]
- El Khoury, D.; Antoine-Jonville, S. Intake of nutritional supplements among people exercising in gyms in Beirut city. J. Nutr. Metab. 2012, 2012, 703490. [Google Scholar] [CrossRef]
- Goston, J.L.; Correia, M.I. Intake of nutritional supplements among people exercising in gyms and influencing factors. Nutrition 2010, 26, 604–611. [Google Scholar] [CrossRef]
- Wardenaar, F.C.; Ceelen, I.J.; Van Dijk, J.W.; Hangelbroek, R.W.; Van Roy, L.; Van der Pouw, B.; De Vries, J.H.; Mensink, M.; Witkamp, R.F. Nutritional supplement use by dutch elite and sub-elite athletes: Does receiving dietary counseling make a difference? Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 32–42. [Google Scholar] [CrossRef]
- Sanchez-Oliver, A.J.; Grimaldi-Puyana, M.; Dominguez, R. Evaluation and behavior of spanish bodybuilders: Doping and sports supplements. Biomolecules 2019, 9, 122. [Google Scholar] [CrossRef] [Green Version]
- Morrison, L.J.; Gizis, F.; Shorter, B. Prevalent use of dietary supplements among people who exercise at a commercial gym. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Attlee, A.; Haider, A.; Hassan, A.; Alzamil, N.; Hashim, M.; Obaid, R.S. Dietary Supplement Intake and Associated Factors Among Gym Users in a University Community. J. Diet. Suppl. 2018, 15, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Vernec, A.; Stear, S.J.; Burke, L.M.; Castell, L.M. A–Z of nutritional supplements: Dietary supplements, sports nutrition foods and ergogenic aids for health and performance: Part 48. Br. J. Sports Med. 2013, 47, 998–1000. [Google Scholar] [CrossRef] [Green Version]
- Torres-McGehee, T.M.; Pritchett, K.L.; Zippel, D.; Minton, D.M.; Cellamare, A.; Sibilia, M. Sports nutrition knowledge among collegiate athletes, coaches, athletic trainers, and strength and conditioning specialists. J. Athl. Train. 2012, 47, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Trakman, G.L.; Forsyth, A.; Middleton, K.; Hoye, R.; Jenner, S.; Keenan, S.; Belski, R. Australian football athletes lack awareness of current sport nutrition guidelines. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 644–650. [Google Scholar] [CrossRef]
- Kruseman, M.; Miserez, V.; Kayser, B. Knowledge about nutrition and weight loss among fitness instructors: A cross-sectional study in Geneva, Switzerland. Schweiz. Z. Sportmed. Sporttraum. 2008, 56, 156–160. [Google Scholar]
- Kruger, J.; Dunning, D. Unskilled and unaware of it: How difficulties in recognizing one’s own incompetence lead to inflated self-assessments. J. Personal. Soc. Psychol. 1999, 77, 1121–1134. [Google Scholar] [CrossRef]
- Milgram, S. Behavioral study of obedience. J. Abnorm. Psychol. 1963, 67, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Waller, M.C.; Kerr, D.A.; Binnie, M.J.; Eaton, E.; Wood, C.; Stenvers, T.; Gucciardi, D.F.; Goodman, C.; Ducker, K.J. Supplement Use and behaviors of athletes affiliated with an Australian state-based sports institute. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 518–525. [Google Scholar] [CrossRef] [Green Version]
- Trakman, G.L.; Forsyth, A.; Hoye, R.; Belski, R. Australian team sports athletes prefer dietitians, the internet and nutritionists for sports nutrition information. Nutr. Diet. J. Dietit. Assoc. Aust. 2019, 76, 428–437. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % | n | |
|---|---|---|
| Gender | ||
| Male | 49 | 205 |
| Female | 48 | 200 |
| Not given | 3 | 12 |
| Age group [y] | ||
| 18–30 | 47 | 197 |
| 31–45 | 23 | 97 |
| 46–60 | 15 | 61 |
| >60 | 11 | 47 |
| Not given | 4 | 15 |
| Training | ||
| Frequency | ||
| [week−1] | ||
| <1 | 1 | 5 |
| 1–2 | 21 | 89 |
| 3–4 | 50 | 210 |
| 5–6 | 21 | 86 |
| Daily or more | 6 | 25 |
| Not given | 1 | 2 |
| Total (n = 417) 2 % (n) | Men (n = 205) % (n) | Women (n = 200) % (n) | p (Gender) | |
|---|---|---|---|---|
| Consumers 1 | 82.0 (332) | 84.4 (173) | 80.0 (159) | 0.201 |
| Protein powders and drinks | 43.2 (180) | 54.6 (112) | 30.0 (60) | <0.001 |
| Magnesium | 33.7 (141) | 30.2 (62) | 36.5 (73) | 0.182 |
| Multivitamin and multimineral | 31.4 (131) | 32.2 (66) | 29.5 (59) | 0.557 |
| Vitamin D | 24.0 (100) | 21.5 (44) | 25.5 (51) | 0.338 |
| Sports drinks | 22.3 (93) | 30.7 (63) | 13.0 (26) | <0.001 |
| Vitamin C | 20.1 (84) | 23.4 (48) | 16.5 (32) | 0.061 |
| Recovery products | 19.2 (80) | 24.4 (50) | 13.5 (27) | 0.005 |
| Protein bars | 18.0 (73) | 21.0 (43) | 15.0 (30) | 0.118 |
| Amino acids (e.g., BCAA, glutamine) | 17.3 (72) | 22.0 (45) | 12.0 (24) | 0.008 |
| Energy drinks | 14.4 (60) | 14.6 (30) | 14.5 (29) | 0.969 |
| Caffeine (without coffee) | 13.2 (55) | 16.1 (33) | 9.5 (19) | 0.047 |
| Creatine | 12.9 (54) | 22.4 (46) | 3.5 (7) | <0.001 |
| Iron | 11.0 (46) | 10.2 (17) | 14.0 (28) | 0.068 |
| Energy bars | 8.6 (36) | 10.7 (22) | 6.5 (13) | 0.130 |
| Plant extracts | 7.9 (33) | 10.2 (17) | 7.5 (15) | 0.767 |
| L-Carnitine | 7.4 (31) | 9.8 (20) | 5.0 (10) | 0.068 |
| Beta-Alanine | 4.1 (17) | 5.4 (11) | 1.5 (3) | 0.033 |
| Alkalizing mineral products | 3.4 (14) | 2.9 (6) | 3.5 (7) | 0.744 |
| Probiotics | 3.1 (13) | 2.4 (5) | 3.5 (7) | 0.529 |
| Carbohydrate gels | 2.2 (9) | 3.4 (7) | 0.5 (2) | 0.099 |
| Nitrate/Beetroot juice | 1.9 (8) | 1.5 (3) | 2.5 (5) | 0.454 |
| Fat-Burn Products | 1.7 (7) | 2.0 (4) | 1.5 (3) | 0.728 |
| Bicarbonate/Citrate | 0.7 (3) | 0.5 (1) | 0.5 (1) | 0.968 |
| HMB | 0.5 (2) | 0.5 (1) | 0.0 (0) | 0.323 |
| Steroids | 0.2 (1) | 0.0 (0) | 0.0 (0) | - |
| Other | 4.1 (17) | 4.4 (9) | 4.0 (8) | 0.845 |
| 18–30 (n = 197) % (n) | 31–45 (n = 97) % (n) | 46–60 (n = 61) % (n) | >60 (n = 47) % (n) | p (Age) | |
|---|---|---|---|---|---|
| Consumers 1 | 87.3 (172) d | 79.4 (77) | 82.0 (50) | 66.0 (31) a | 0.006 |
| Protein powders and drinks | 55.8 (110) c,d | 45.4 (44) c,d | 19.6(12) a,b | 14.9 (7) a,b | <0.001 |
| Magnesium | 35.0 (69) | 29.9 (29) | 37.7 (23) | 31.9 (15) | 0.733 |
| Multivitamin and multimineral | 33.5 (66) | 27.8 (27) | 31.1 (19) | 31.9 (15) | 0.808 |
| Vitamin D | 23.9 (47) | 21.6 (21) | 21.3 (13) | 25.5 (12) | 0.931 |
| Sports drinks | 24.4 (48) | 18.6 (18) | 32.8 (20) d | 6.4 (3) c | 0.007 |
| Vitamin C | 20.8 (41) | 18.6 (18) | 19.7 (12) | 17.0 (8) | 0.930 |
| Recovery products | 27.4 (54) d | 15.5 (15) | 11.5 (7) | 4.3 (2) a | <0.001 |
| Protein bars | 18.8 (37) | 18.5 (18) | 24.5 (15) | 8.5 (4) | 0.200 |
| Amino acids (e.g., BCAA, glutamine) | 24.8 (49) c | 14.4 (14) | 6.5 (4) a | 8.5 (4) | 0.001 |
| Energy drinks | 22.8 (45) b,c | 8.2 (8) a | 6.5 (4) a | 2.1 (1) | <0.001 |
| Caffeine (without coffee) | 19.8 (39) | 9.3 (9) | 4.9 (3) | 4.3 (2) | 0.001 £ |
| Creatine | 19.8 (39) c | 11.3 (11) | 3.3 (2) a | 4.3 (2) | 0.001 |
| Iron | 15.2 (30) | 9.3 (9) | 8.2 (5) | 2.1 (1) | 0.046 $ |
| Energy bars | 8.6 (17) | 7.2 (7) | 13.1 (8) | 6.4 (3) | 0.555 |
| Plant extracts | 10.7 (21) | 6.1 (6) | 6.6 (4) | 4.3 (2) | 0.349 |
| L-Carnitine | 8.1 (16) | 6.2 (6) | 11.5 (7) | 4.3 (2) | 0.500 |
| Beta-Alanine | 5.1 (10) | 4.1 (4) | 1.6 (1) | 2.1 (1) | 0.589 |
| Alkalizing mineral products | 2.0 (4) | 6.2 (6) | 1.6 (1) | 4.3 (2) | 0.234 |
| Probiotics | 3.0 (6) | 3.1 (3) | 4.9 (3) | 2.1 (1) | 0.858 |
| Carbohydrate gels | 2.0 (4) | 2.1 (2) | 3.3 (2) | 0.0 (0) | 0.687 |
| Nitrate/Beetroot juice | 1.0 (2) | 1.0 (1) | 1.6 (1) | 6.4 (3) | 0.078 |
| Fat-Burn Products | 3.0 (6) | 1.0 (1) | 0.0 (0) | 0.0 (0) | 0.245 |
| Bicarbonate/Citrate | 0.0 (0) | 2.1 (2) | 1.6 (1) | 0.0 (0) | 0.190 |
| HMB | 0.5 (1) | 1.0 (1) | 0.0 (0) | 0.0 (0) | 0.778 |
| Steroids | 0.0 (0) | 1.0 (1) | 0.0 (0) | 0.0 (0) | 0.369 |
| Other | 5.5 (11) | 1.0 (1) | 3.3 (2) | 2.1 (1) | 0.238 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mettler, S.; Bosshard, J.V.; Häring, D.; Morgan, G. High Prevalence of Supplement Intake with a Concomitant Low Information Quality among Swiss Fitness Center Users. Nutrients 2020, 12, 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092595
Mettler S, Bosshard JV, Häring D, Morgan G. High Prevalence of Supplement Intake with a Concomitant Low Information Quality among Swiss Fitness Center Users. Nutrients. 2020; 12(9):2595. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092595
Chicago/Turabian StyleMettler, Samuel, Joëlle Vera Bosshard, Dino Häring, and Gareth Morgan. 2020. "High Prevalence of Supplement Intake with a Concomitant Low Information Quality among Swiss Fitness Center Users" Nutrients 12, no. 9: 2595. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12092595