
Gastrointestinal Microbiome and Multiple Health Outcomes: Umbrella Review
1
West China School of Nursing, Sichuan University/West China Hospital, Sichuan University, 37 Guo Xue Rd., Chengdu 610041, China
2
Department of Organization, West China Hospital, Sichuan University, 37 Guo Xue Rd., Chengdu 610041, China
*
Author to whom correspondence should be addressed.
Nutrients 2022, 14(18), 3726; https://0-doi-org.brum.beds.ac.uk/10.3390/nu14183726
Submission received: 23 July 2022
/
Revised: 29 August 2022
/
Accepted: 8 September 2022
/
Published: 9 September 2022
(This article belongs to the Special Issue Nutrition, Gut Microbiota and Health)
{kind=link}
{kind=link}
{kind=link}
Abstract
:In recent years, there has been growing concern about the impact of the gastrointestinal microbiome on human health outcomes. To clarify the evidence for a link between the gastrointestinal microbiome and a variety of health outcomes in humans, we conducted an all-encompassing review of meta-analyses and systematic reviews that included 195 meta-analyses containing 950 unique health outcomes. The gastrointestinal microbiome is related to mortality, gastrointestinal disease, immune and metabolic outcomes, neurological and psychiatric outcomes, maternal and infant outcomes, and other outcomes. Existing interventions for intestinal microbiota (such as probiotics, fecal microbiota transplant, etc.) are generally safe and beneficial to a variety of human health outcomes, but the quality of evidence is not high, and more detailed and well-designed randomized controlled trials are necessary.
1. Introduction
There are hundreds of millions of microorganisms in the human gut [1]. Collectively known as gut flora, the human gastrointestinal microbiota is more than 10 times the number of cells in the human body, providing metabolic, immune, and protective functions and playing a vital role in human health [2,3,4,5,6]. The gut microbiota produces bioactive metabolites that influence many aspects of host physiology. For example, as a product of intestinal flora, short-chain fatty acids (SCFAs) are playing an increasingly important role. Butyrate can induce the apoptosis of colon cancer cells and activate intestinal gluconeogenesis, which has beneficial effects on glucose and energy homeostasis [7]. Butyrate and propionate appeared to control gut hormones, reducing appetite and food intake in mice [8]. Other specific products of the gut microbiome are directly relevant to human health outcomes. Trimethylamine, for example, is oxidized in the liver to trimethylamine N-oxide, which is positively associated with an increased risk of adverse cardiovascular events [9,10]. The gastrointestinal microbiota is influenced by many factors, including genetics, host physiology (age, disease, stress, etc.), and environmental factors (living conditions, drug use, diet, etc.) [8,11,12,13]. In recent years, the consumption of specific dietary components (such as fiber and prebiotics) and fecal microbiota transplantation have become common ways to regulate the microbiome. In addition, the concept of the brain–gut–microbiota axis has attracted much attention. The central nervous system (CNS) is able to respond directly or indirectly to the microbiota and its metabolites through the network of CNS neurons. Gut microbiota can affect brain function from the bottom up through the microbiota–gut–brain axis, and it can participate in the occurrence and development of psychiatric, neurodevelopmental, age-related, and neurodegenerative disorders. The brain may also affect gut microbiota and its metabolites from the top down through the brain–gut–microbiota axis. The concrete mechanism of two-way communication between the gut and brain is not entirely clear, but communication between the gut microbiome and the brain/central nervous system is closely related to other systems, such as the immune system, the endocrine system, the intestinal barrier and blood–brain barrier, microbial metabolites and gut hormones, as well as the sensory and autonomic nervous systems [14,15,16,17,18].
However, it is important to systematically evaluate and summarize the advanced evidence on the impact of gastrointestinal microbiota on all health outcomes before interventions are undertaken. To date, many epidemiological studies (case controls or cohort) and clinical trials (cross-sectional or randomized control trials) have been widely used to investigate the relationship between gut microbes and a range of health outcomes. However, different studies have come to conflicting conclusions. If carried out and interpreted properly, umbrella reviews can provide evidence of the highest quality. Therefore, we conducted an umbrella review by integrating evidence from multiple meta-analyses to help determine the presence and extent of associations between gastrointestinal microbiota and different health outcomes and to assess any risks that may be associated with changes in gastrointestinal microbiota in existing studies. The research results can provide a basis for policymakers to formulate or update relevant guidelines.
2. Methods
2.1. Umbrella Review Method and Assessment of Methodological Quality
The umbrella review was carried out as previously published in the relevant literature [19,20]. The AMSTAR [21] and GRADE [22] were used to independently evaluate the methodological quality of the selected meta-analyses or systematic reviews and the quality of the original literature by two investigators (Chengting Chang and Xingzhu Yuan). If there was any inconsistency, a third researcher was consulted. There are 16 items in AMSTAR 2 [21] in total, among which 2, 4, 7, 9, 11, 13, and 15 are the key items. The evaluation results of each item are divided into yes (Y) and part of yes (PY) and no (N). If the evaluation result was not, it was considered to be inconsistent. If there was no or only one noncritical item considered as N, the meta-analysis was rated as highly reliable. If more than one noncritical item is rated as nonconformance, the analysis is considered to have medium credibility. If the analysis does not meet one key item regardless of whether it meets any nonkey item, it is rated as low reliability. If more than one key item does not meet the criteria, no matter whether the nonkey item meets the criteria, the credibility is very low. GRADE [23] has four grades, high, mediate, low, and very low, and it evaluates the quality of evidence of outcome indicators through five degrading factors: the risk of bias, imprecision, inconsistency, indirectness, and magnitude of effect.
2.2. Literature Search
We searched meta-analyses of observational or interventional studies, which examined the link between gut microbiota and any health outcomes, published between inception and September 2021 in PubMed, Web of Science, Embase, and the Cochrane Database of Systematic Reviews. We used the following terms/keywords to search: (meta analys* or meta-analys* or systematic review*) and (gastrointestinal microbiome or intestine flora or related free words) using truncated terms for all fields, following the SIGN guidance recommended search terms for systematic reviews and meta-analyses [24]. See Supplementary Materials for detailed retrieval strategies. We also conducted a manual search for references to eligible articles.
2.3. Eligibility Criteria
Two researchers (Chengting Chang and Xingzhu Yuan) independently screened the titles and abstracts and selected articles for full-text review. They then independently reviewed the full-text articles for eligibility. A third researcher, Xinrong Chen, arbitrated any differences that could not be resolved by consensus.
Meta-analyses and/or systematic reviews assessing the link between the human gut microbiota (containing microbial metabolites) and any health outcomes were included, regardless of whether and for what reason the gut microbiota changed. However, considering that antibiotics may have a direct impact on health outcomes such as inflammatory factors or disease recovery, the article on antibiotics as an intervention was excluded. Participants of any age, gender, and race from any country and setting were allowed to be included, and participants could be healthy, have pre-existing conditions, or be pregnant. We did not use language restrictions, but animal or in vitro experiments were excluded. There was no limit to the types of meta-analyses but the network meta-analysis, which means observational (cohort, case-control, and cross-sectional studies with binary outcomes) and interventional studies (randomized controlled trials) can be included. However, at least one of the relative risks, odds ratios, relative rates, hazard ratios, standardized mean difference, weighted mean difference, mean difference, risk difference, or median difference should be reported. If there was more than one meta-analysis and/or systematic review of the same research question, we included the most recent study with the largest number of studies and participants. If an article conducted a separate meta-analysis of more than one health outcome, we included each one separately.
2.4. Data Extraction
Two investigators (Chengting Chang and Xingzhu Yuan) independently extracted the following information from the included literature: the first author, year of publication, populations, number of studies, number of cases/control or total participants, study design (cohort, case-control, randomized controlled trial (RCT)), intervention duration or length of follow-up, outcome(s) of interest (multiple health outcomes), outcome comparison (e.g., highest versus lowest/none), meta-analysis metric (e.g., odds ratio), estimated summary effect with the 95% confidence intervals (95% CIs), type of effect model (fixed or random), heterogeneity and publication bias. Any discrepancies in the data extracted by the two researchers were resolved by consensus.
2.5. Data Analysis
After incorporating appropriate systematic reviews and meta-analyses, we added major trials missing from the largest or the most recent meta-analysis. The estimated summary effect and its 95% confidence interval for each included meta-analysis were then extracted. We used the I2 metric [25] (0% to 25%: might not be necessary; 25% to 50%: might be represented as moderate heterogeneity; 50% to 75%: might be shown as substantial heterogeneity; 75% to 100%: considerable heterogeneity). Heterogeneity was assessed using p values generated by the Egger test [26] (p < 0.05) to assess publication bias. We did not reanalyze the other data or primary studies included in the meta-analysis.
3. Results
3.1. Characteristics of Included Articles
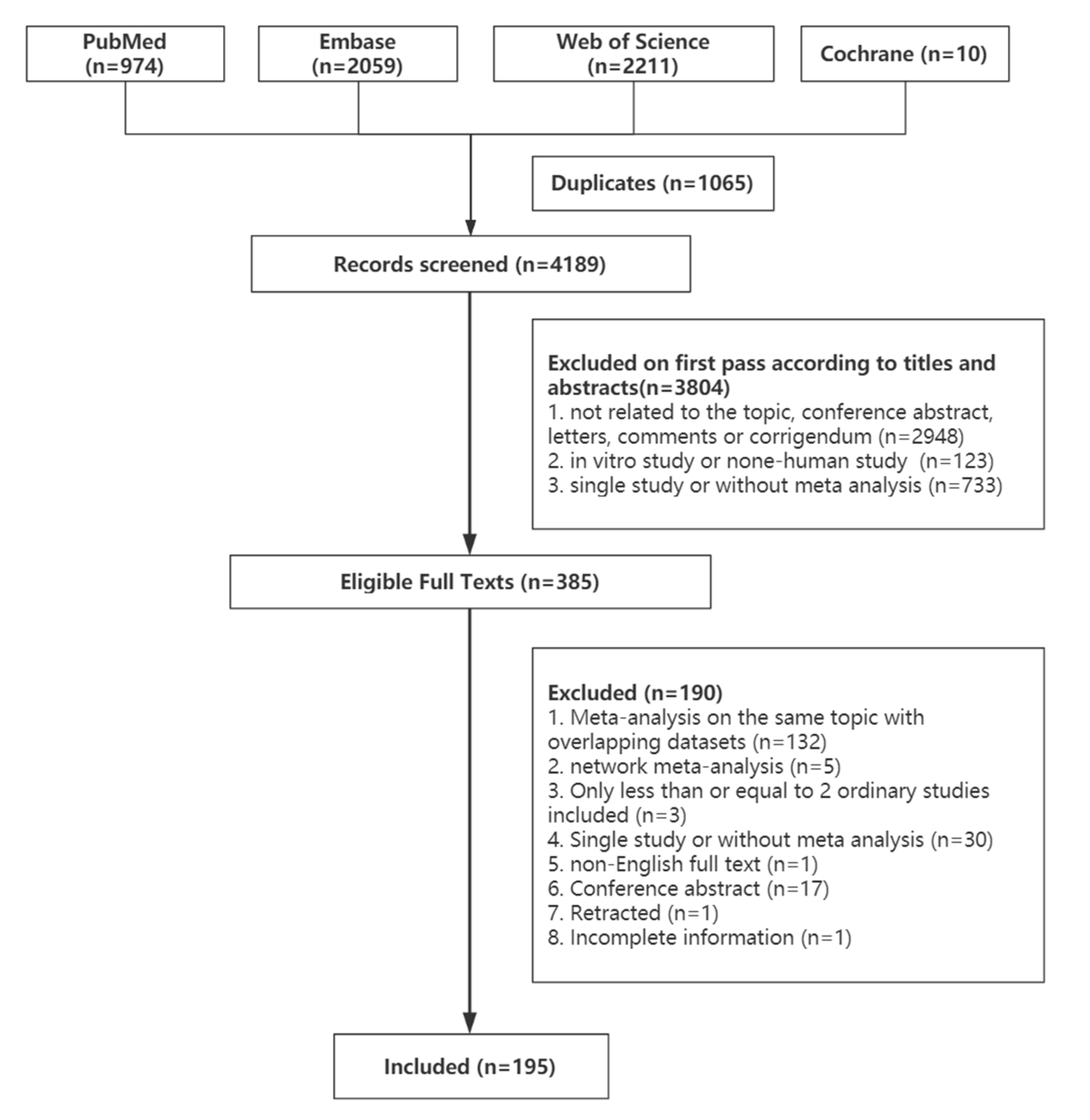
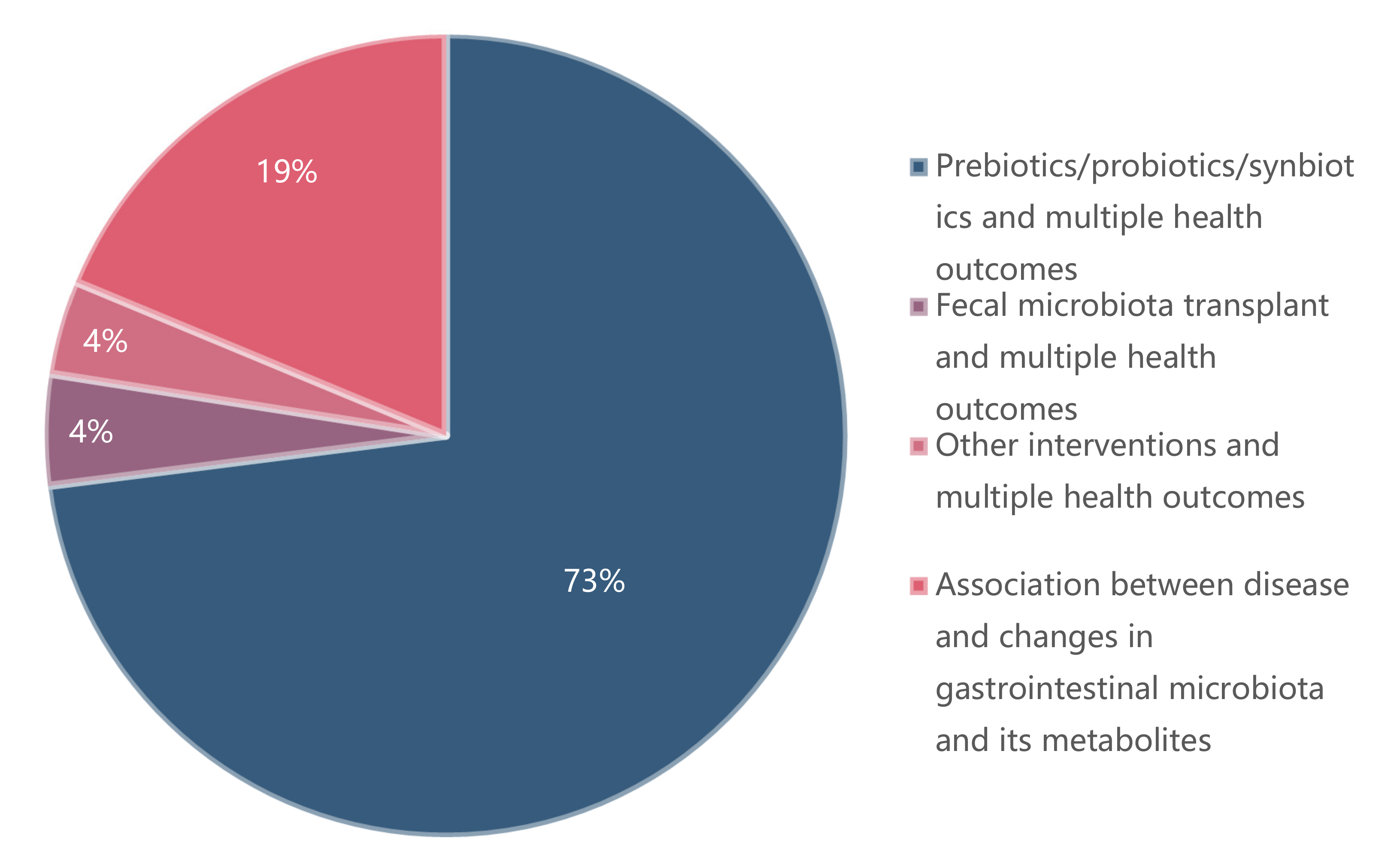
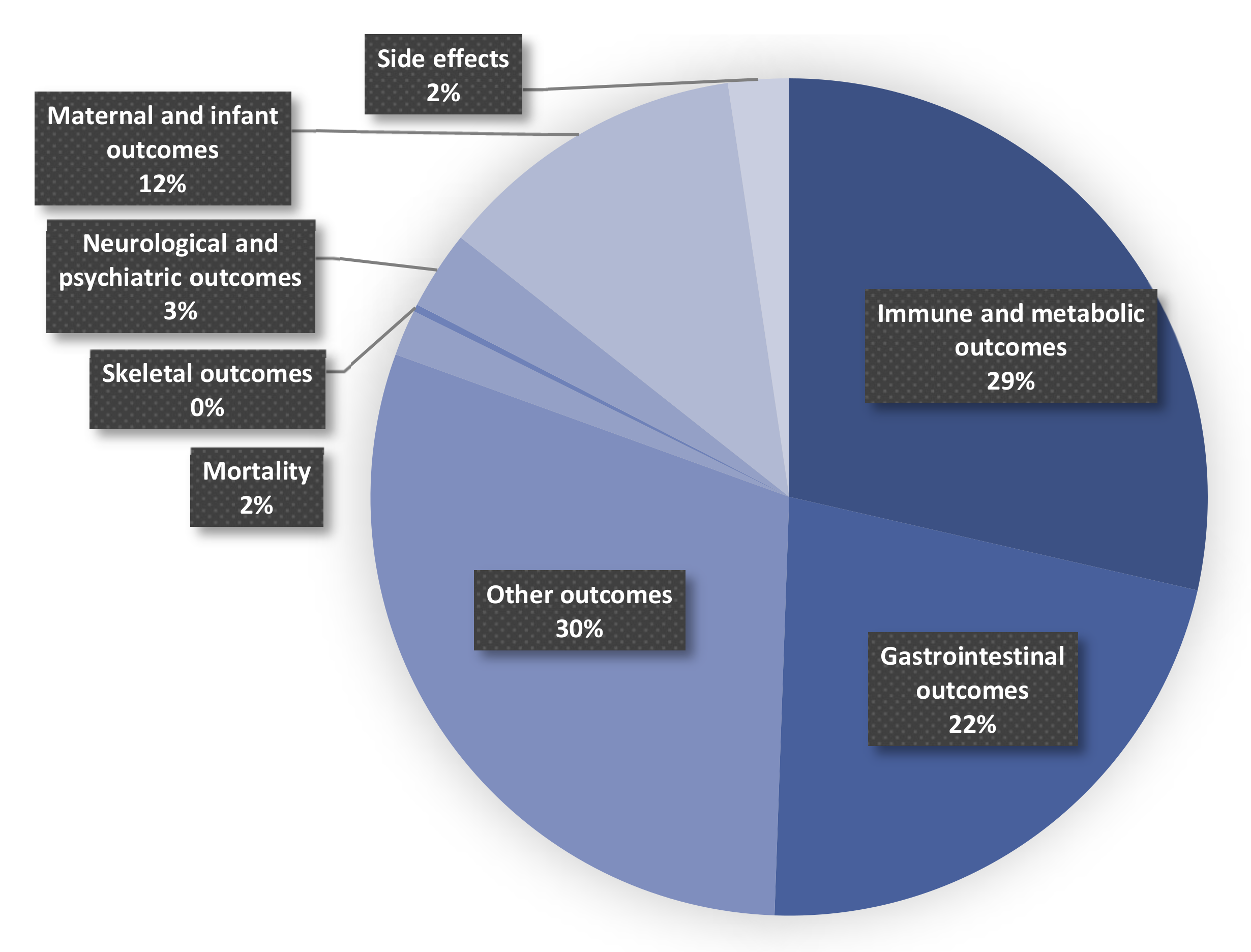
Figure 1 shows the process of the systematic search and selection of eligible studies. A total of 5254 records were retrieved, 385 of which were eligible for the stage of full-text review. Finally, 195 recent meta-analyses spanning 2009–2021 with 970 unique results were included in our umbrella review (Figure 2). Outcomes related to prebiotics/probiotics/synbiotics are shown in Figure 3.
The number of meta-analyses of single outcomes ranged from 3 to 54. The detailed associations between prebiotics/probiotics/synbiotics and multiple health outcomes are shown in Supplementary Table S1. The relationship between fecal microbiota transplantation and multiple health outcomes is presented in Supplementary Table S9. Supplementary Table S10 shows other outcomes related to the gastrointestinal microbiome. The associations between disease and changes in gastrointestinal microbiota and its metabolites are shown in Supplementary Table S11.
3.2. Prebiotics/Probiotics/Synbiotics and Multiple Health Outcomes
3.2.1. Mortality
In very preterm (28–32 week of gestation), preterm infants (<36 or 37 weeks), low birth weight infants (<2500 g), and very low birth weight (<1500 g) infants, prebiotic/probiotic use is associated with reduced mortality [27,28,29,30,31,32,33]. However, in extremely preterm (<28 weeks’ gestation) or extremely low birth weight (<1000 g) infants, surgical patients and people with any grade of acute or chronic hepatic encephalopathy, prebiotic/probiotic use has not been associated with reduced mortality [28,34,35]. Additionally, there was no association between the use of a prebiotic, probiotic, or synbiotic agent and the improvement of the death rate in patients who underwent abdominal surgery [36]. See Supplement Table S2 for a more detailed summary.
3.2.2. Immune and Metabolic Outcomes
A number of meta-analyses have proven that related indicators of liver function (e.g., bilirubin, total cholesterol, low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol (HDL-c), triglycerides, etc.) were associated with prebiotics/probiotics/synbiotics [37,38,39,40,41,42,43]. However, the association was uncertain for patients with liver disease, kidney disease or metabolic syndrome [42,44,45,46].
In addition, immune-related indicators (such as immunoglobulin A, immunoglobulin G, immunoglobulin M, C-reactive protein (CRP), tumor necrosis factor α, etc.) were related to prebiotics/probiotics/synbiotics [47,48,49,50], but in patients with liver disease or rheumatoid disease or human immunodeficiency virus (HIV), adult athletes, kidney disease patients, healthy elderly individuals aged > 60 years, or obese adults (age ≥ 18 years) who had undergone bariatric surgery, correlations are no longer proven [42,44,51,52,53,54,55,56].
Evidence has been shown to link blood sugar control (such as fasting plasma glucose, glucose, fasting insulin, glycated hemoglobin, etc.) [39,40,44,45,48,57,58,59] and enzymes (lidiamine oxidase, gamma-glutamyl transpeptidase, etc.) [41,42,47] to prebiotics/probiotics/synbiotics.
Protein results (albumin, prealbumin, total protein, hemoglobin, etc.) were associated with prebiotics/probiotics/synbiotics [47] but not in adult chronic kidney disease [53]. Meanwhile, prebiotics/probiotics/synbiotics were related to total antioxidant capacity [39,49], nitric oxide (NO) [49], total glutathione [39,49], plasma ammonia [34,60], malondialdehyde [49,61], serum calcium levels, parathyroid hormone, urinary calcium [62], and the rise of butyrate and total SCFAs [35].
However, there was no evidence of the relationship between prebiotics/probiotics/synbiotics and urea, uric acid, and creatinine in adult chronic kidney disease [53,63,64]. See Supplementary Table S3 for a more detailed summary.
3.2.3. Gastrointestinal Disease
Prebiotics/probiotics/synbiotics are correlated with gastrointestinal symptoms and functional level. Prebiotics/probiotics/synbiotics have been linked to a lower risk of diarrhea [47,65,66,67,68,69,70,71,72,73,74,75] but not in adults who received mechanical ventilation (MV) therapy in hospitals [65] and healthy infants or children, aged 0–18 years [76]. In all patients who met the criteria of severe stroke, early enteral nutrition combined with probiotics was associated with many improvements in gastrointestinal function [47]. The use of combination probiotics is associated with the improvement of persistence of symptoms and bloating scores but not flatulence scores in adults (participants aged > 16 years) [77]. However, regarding abdominal pain scores in patients with irritable bowel syndrome, the association with prebiotics/probiotics/synbiotics is still controversial [78,79,80,81]. Whether probiotics are related to stool frequency and consistency varies with the disease and the population [33,80,82,83,84,85]. In addition, the overall symptom response to treatment, integrative symptom score, severity of abdominal pain, bloating, and flatulence in adult patients ≥ 18 and ≤ 64 years with irritable bowel syndrome or other functional bowel disorders were irrelevant to prebiotics/probiotics/synbiotics [86].
There is also evidence of an association between a positive stool Clostridium difficile cytotoxin assay or culture [68,70], a decrease in Eubacterium rectale or Clostridium coccoides [87], the elevation of beneficial bacteria such as bifidobacterial [88], and prebiotics/probiotics/synbiotics. Additionally, the eradication of Helicobacter pylori (H. pylori) in H. pylori-infected patients was related to probiotics [89]. In adults who received mechanical ventilation therapy in hospitals, oropharyngeal colonization, gastric colonization, and the rate of Gram-negative bacterial positivity were associated with prebiotics/probiotics/synbiotics, while a positive rate of Gram-positive bacterial culture and positive fungal culture rates were irrelevant [65].
The reduction in colon endoscopic scores in children or adults with ulcerative colitis was also related to prebiotics/probiotics/synbiotics [90,91] but not only using Escherichia coli Nissle (EcN) 1917 [92]. For people of any age with ulcerative colitis in remission, clinical relapse and maintenance of clinical remission were not associated with probiotics [93]. Prebiotics/probiotics/synbiotics were related to clinical remission and clinical response in adults or children with active ulcerative colitis [94,95,96,97] and inducing/maintaining inflammatory bowel disease (IBD) remission [98], but preventing relapse is irrelevant [97,99]. See Supplementary Table S4 for a more detailed summary.
3.2.4. Neurological and Psychiatric Outcomes
Probiotics are associated with cognitive improvement in adults [100] but not with cognitive function in dementia patients [101]. However, when focusing on patients with a diagnosis of Alzheimer’s disease (AD) or mild cognitive impairment (MCI), a correlation between probiotics and cognitive promotion has been shown [49].
Probiotics are associated with adult healthy volunteers’ preclinical psychological symptoms of anxiety, depression, and stress [102] but not the symptoms of depressive symptoms [103]. For the general population or clinical population, patients with major depressive disorder or other clinical diagnosis populations, probiotics are related to the improvement of depressive symptoms [103]. Probiotics did not show a correlation with schizophrenia symptoms in patients with at least moderately severe psychotic symptoms aged 18–65 years [104]. Probiotics were associated with a reduction in stress levels and stress-related subthreshold anxiety/depression levels in healthy people [105]. When probiotics were associated with the improvement of depression and anxiety in patients with depression or anxiety, prebiotics and anxiety in adult patients with 18 and 64-year irritable bowel syndrome or other functional bowel disorders (FBDs) showed no correlation [86]. Additionally, depression and anxiety in patients with depression or anxiety did not show any relation to prebiotics [106]. See Supplementary Table S5 for a more detailed summary.
3.2.5. Maternal and Infant Outcomes
Prebiotics/probiotics/synbiotics were associated with the duration of crying in infants [107,108,109]. The risk of necrotizing enterocolitis (before hospital discharge), invasive infection (before hospital discharge) in very preterm (<32 weeks’ gestation) or very low birth weight (<1500 g), but not in infants extremely preterm (<28 weeks’ gestation) or extremely low birth weight (<1000 g) infants, was related to prebiotics/probiotics/synbiotics [28]. The duration of birth hospitalization in very preterm (<32 weeks’ gestation) or very low birth weight (<1500 g) was also reduced [28]. Prebiotics/probiotics/synbiotics were associated with preventing necrotizing enterocolitis in preterm neonates [29,30,31,32], decreasing the death rate in preterm infants <37 weeks and/or birth weight < 2500 g [30,31,32], and reducing total cholesterol and triglycerides in pregnant women [110]. A mixture of Lactobacillus and Bifidobacterium was associated with the risk of eczema in children [111], but Lactobacillus rhamnosus GG is irrelevant [112].
The occurrence of new cases of colic [107] in infants, the risk of neurodevelopmental impairment, cerebral palsy, visual impairment, hearing impairment in very preterm (<32 weeks’ gestation) or very low birth weight (<1500 g) [28], sepsis, Hirschsprung-associated enterocolitis (HAEC), and age reaching full feeds in preterm infants [29,31,32,113] have not been found to be related to prebiotics/probiotics/synbiotics. Mean cognitive and motor scores, the risk of cognitive impairment, the risk of motor impairment, the risk of neurodevelopment impairment (NDI), the risk of cerebral palsy, and the risk of hearing impairment in children under 5 years of age in preterm infants (<37 weeks gestation and/or birth weight < 1500 g) [114] have not been proven to be related to prebiotics/probiotics/synbiotics use. Additionally, preterm birth < 37 weeks’ gestation [115], newborn birth weight [116], and HDL-C and LDL-C in pregnant women [110] were irrelevant to prebiotics/probiotics/synbiotics.
It is contradictory whether prebiotics/probiotics/synbiotics are related to preventing gestational diabetes and some related infant outcomes 105], [110 in pregnant women not previously diagnosed with diabetes mellitus. However, in adult pregnant women regardless of weight status (normal, overweight, or obese), who were diagnosed with gestational diabetes mellitus (GDM) according to the oral glucose tolerance test and were not on any hypoglycemic agents, they were related to blood sugar control in pregnant women and some related infant outcomes [117].
There is no evidence that prebiotics/probiotics/synbiotics are associated with adverse effects including parental depression and mental illness, choking, bacterial infection, or apparent life-threatening/serious events (dichotomous outcome) in infants [107]. See Supplementary Table S6 for a more detailed summary.
3.2.6. Other Outcomes
In participants taking antibiotics, there is no evidence to prove that the detection of C. difficile in stool [67] and length of hospital stay [67] are related to probiotics. Overall, prebiotics/probiotics/synbiotics were associated with a reduction in the incidence of infection [36,47,74,87,118,119,120,121], the enteral nutrition target time [47], and the length of hospital stay [33,35,47,119,120]. Parts of the outcomes of respiratory tract infections in healthy children (from birth to 18 years) were also relevant [122]. Prebiotics/probiotics/synbiotics were related to the improvement of polymorphonuclear phagocytic capacity, natural killer (NK) cell tumoricidal activity, and reduction in No-recovery [34,123].
The association between the risk of atopic and food sensitization and prebiotics/probiotics/synbiotics in children varied according to the time of administration [124]. The risk of developing asthma, allergic rhinitis, wheezing, and positive aeroallergen skin-prick test (SPT) results in healthy children were not associated with prebiotics/probiotics/synbiotics [125].
Liver stiffness was measured by the FibroScan in adult patients with nonalcoholic fatty liver disease (NAFLD) or nonalcoholic steatohepatitis (NASH) and BMI in male and female patients of any age who presented at least one of the following: NAFLD, steatosis, liver fibrosis, and steatohepatitis [42,126] were proven to be related to prebiotics/probiotics/synbiotics [44,127].
In surgical patients, prebiotics/probiotics/synbiotics were related to superficial incisional, duration of postoperative pyrexia, fluid diet, hospital stay, and solid diet [35]. There is evidence that prebiotics/probiotics/synbiotics may be useful to improve quality-of-life (QoL) in adults of both sexes and of all ages with irritable bowel syndrome (IBS) [86,128]. In adults who received mechanical ventilation (MV) therapy in hospitals, ventilator-associated pneumonia (VAP) incidence, length of ICU stay, length of hospital stay, days of antibiotics use, the incidence of bacteremia, and rate of multidrug-resistant (MDR) infections were related to prebiotics/probiotics/synbiotics [65]. In addition, improvement in the corresponding score of adults with relapsing–remitting multiple sclerosis [129], physical growth during the first year of life of full-term neonates [130], and reduction in the Severity Scoring of Atopic Dermatitis (SCORAD) values at 8 weeks in patients with atopic dermatitis [131] were associated with prebiotics/probiotics/synbiotics. For the patients with minimal hepatic encephalopathy (MHE), the development of overt HE (week 4 but not 12 weeks), and improvement in MHE (week 12) were also relevant [60].
For adults (≥18 years old) with body mass index (BMI) > 25 kg/m2, prebiotics/probiotics/synbiotics were related to waist circumference [132], fat mass, fat percentage, waist-to-hip ratio [48], total abdominal fat area, and subcutaneous abdominal fat area [57]. Probiotic fermented milk products (PFMPs) were associated with body weight, but BMI, waist circumference, and body fat percentage were irrelevant [133]. The meta-analysis did not prove that waist circumference and hip circumference in women with polycystic ovary syndrome (PCOS) are irrelevant to prebiotics/probiotics/synbiotics [40], but the modified Ferriman–Gallway score is relevant [39].
The blood pressure of adults (18 years or older) with overweight or obesity [48], number of pulmonary exacerbations, and forced expiratory volume (FEV)1 (% predicted) in participants who fulfilled consensus diagnostic criteria for cystic fibrosis (CF) were not associated with prebiotics/probiotics/synbiotics [134]. In the participants who were diagnosed with chronic kidney disease (CKD), weight, BMI and estimated glomerular filtration rate preservation [63,64] were irrelevant to prebiotics/probiotics/synbiotics. Additionally, in adult diabetic patients, BMI is irrelevant [135], but blood pressure is relevant [135]. Probiotics had no significant effect on sleep [136]. Weight, BMI and waist circumference in adults with metabolic syndrome were not associated with prebiotics/probiotics/synbiotics [46], while BMI and blood pressure control in hypertension patients were relevant [59]. Whether probiotics are related to the immune response to influenza in adults differs from the virus strain [137,138]. There was no correlation between probiotic use and spinal bone mineral density and total hip bone mineral density of adults [62]. See Supplementary Table S7 for a more detailed summary.
3.2.7. Side Effects
In hospitalized or outpatients (adult or children) taking antibiotics [66,67,69,70,73], patients with ulcerative colitis (UC) [92], people with any grade of acute or chronic hepatic encephalopathy [34], adults with inflammatory bowel disease [86,99] or patients with celiac disease [88] or with functional dyspepsia [139], there is no evidence that prebiotics/probiotics/synbiotics are associated with adverse events [77,138,140]. See Supplementary Table S8 for a more detailed summary.
3.3. Fecal Microbiota Transplant and Multiple Health Outcomes
Fecal microbiota transplant (FMT) was related to diarrhea in adult human participants with diagnoses of C. difficile diarrhea aged over 19 years old [141] but not in patients with documented recurrent Clostridium difficile infection [142] and adult patients (≥18 years) with IBS [143]. Clinical remission or response of patients with IBD was associated with FMT [144,145,146,147], but it is still controversial whether endoscopic mission/response in adult subjects with endoscopically and clinically active UC is related to FMT [145,146,148]. In adults diagnosed with metabolic syndrome, FMT was relevant to the increase in HDL cholesterol and LDL cholesterol, the reduction in glycated hemoglobin (HbA1c) and total cholesterol, but not fasting glucose, triglycerides, BMI, weight, and homeostasis model assessment of insulin resistance (HOMA-IR) [149]. In addition, FMT was related to achieving antimicrobial resistance remission in adults (>18 years) with achieving antimicrobial resistance colonization [150]. Regarding the serious adverse events, there is no evidence linking them to FMT [95]. See Supplementary Table S9 for a more detailed summary.
3.4. Other Interventions and Multiple Health Outcomes
Chinese herbal compounds, Chinese patent medicine, and single Chinese medical herbs were associated with reductions in fasting blood glucose, HbA1c, 2 h postprandial blood glucose, and HOMA-IR [151] through affecting the gastrointestinal microbiome. Dietary fiber (including fruit and vegetable) was related to the risk of Crohn’s disease (CD) and UC [152] and depression in adults and children [153]. Additionally, the low-FODMAP (fermentable oligo-, di- and monosaccharides, and polyols) diet in adult human subjects with IBS was relevant to the decline in IBS severity [154]. The incidence of gastrointestinal acute graft-versus-host disease but not the incidence of mucositis grade III–IV and overall survival at day + 100 was associated with enteral nutrition with or without the addition of parenteral nutrition [155]. In young children (preferably younger than 5 years of age) with acute diarrhea, postbiotics (bioactive compounds produced during a fermentation process, including microbial cells, cell constituents, and metabolites) that support health and/or wellbeing were related to the duration of diarrhea episodes [156]. In addition, kefir beverages have a certain effect on blood glucose control in type II diabetic patients [157], and starch type 2 in adult CKD patients receiving regular hemodialysis has some benefits [158]. However, treatment of Helicobacter pylori infection was not related to the improvement of rosacea-related skin symptoms [159]. See Supplementary Table S10 for a more detailed summary.
3.5. Association between Disease and Changes in Gastrointestinal Microbiota and Its Metabolites
In patients with chronic pancreatitis [160], chronic liver disease [161], cirrhosis [162], systemic sclerosis [163], or Parkinson’s disease [164], but not participants with obesity, the risk of small intestinal bacterial overgrowth increased [165]. However, the relationship is still controversial in populations with IBS [166,167,168]. Similarly, whether patients have small intestinal bacterial overgrowth (SIBO) is associated with a decrease in the risk of ascites, minimal hepatic encephalopathy, and spontaneous bacterial peritonitis in patients aged ≥ 18 years patients with cirrhosis and nonalcoholic fatty liver disease [162,169]. The risk of prevalence of SIBO on upper gut aspirate culture, and the prevalence of the positive glucose hydrogen breath test but not the positive lactulose hydrogen breath test is related to whether patients have IBS [166].
Whether adult patients are diagnosed with CKD [170] or stroke [171] is associated with high circulating trimethylamine N-oxide (TMAO) concentrations. Additionally, the increase in TMAO concentrations is related to an increase in all-cause mortality [172], the incidence of major adverse cardio and cerebrovascular events (MACCEs) [173,174], major adverse cardiovascular events (MACEs) [10,172,175], hypertension prevalence [176], diabetes [177], cardiovascular events (CVEs) risk [9], heart failure [178] and CRP concentrations [179], but diastolic blood pressure, HDL-cholesterol, LDL-cholesterol, triglycerides, total cholesterol and BMI are irrelevant [180,181]. H. pylori infection is elevated in patients with Guillain–Barre Syndrome or IBD but not IBS [182,183,184]. Similarly, if a patient is infected with H pylori infection, NAFLD increases [185].
In children with autism, patients with NAFLD, IBD, or colorectal cancer, some species change [186,187,188,189,190,191]. For example, the bacterial counts of F. prausnitzii, Clostridium coccoides, Clostridium leptum, Faecalibacterium prausnitzii, and Bifidobacterium decrease in patients with IBD [186]. Some metabolites, such as acetate, valerate, butyrate, and total SCFAs, also change in the population with IBD or IBS [189,192,193].
In addition, the alpha diversity (Simpson index) decreased in men who had sex with men (MSM) or people who were HIV + [194]. Overall, the number of observed species and CHAO1 index, but not the Shannon index and Simpson index, are related to psychiatric diagnosis [195]. However, there is no evidence of the relationship between major depressive disorder and the Shannon index or Simpson index [196]. See Supplementary Table S11 for a more detailed summary.
3.6. Heterogeneity of Included Studies
Of all included outcomes, approximately 16.7% had low heterogeneity (I2 < 25%). About 64.9% of the outcomes had moderate heterogeneity (I2 ranging from 25 to 75%); 13.2% of the outcomes were highly heterogeneous (I2 > 75%). However, heterogeneity was not reported in 5.2% of outcomes, and we could not reanalyze it because the information was not available.
3.7. Publication Bias of Included Studies
Funnel plots and Egger’s test were used in this umbrella review. No publication bias was found in 20.4% of the studies. Other meta-analyses did not report the results of publication bias. However, in many of the included studies, there was a high probability of unreported publication bias.
3.8. GRADE Classification and AMSTAR 2 Score of Included Studies
The studies were classified into four levels, with approximately 4.2% rated high, about 92.7% rated low, and 2.6% rated very low by AMSTAR 2. The reason was that most studies did not report the source of funding for the studies included in the meta-analysis (Item 10). Approximately 25.8% were rated as very low, 38.0% as low, and 36.1% as the medium in terms of GRADE. The detailed results of AMSTAR 2 and GRADE are presented in Supplementary Tables S12 and S13, respectively.
4. Discussion
In this review, we identified a total of 195 meta-analyses and 970 unique results. Based on the available evidence, the gastrointestinal microbiome is more often associated with a range of health-related outcomes than with harm. There has been some research into how gastrointestinal microbes affect health outcomes. In addition to acting as a microbial barrier, the gut microbiota also participates in the composition of other intestinal barriers through various pathways, and it jointly plays an important role in the gut. Studies have shown that the intestinal microbiota has a protective effect on host intestinal epithelial cells, thus further strengthening the role of the intestinal mechanical barrier. On the contrary, the intestinal microbial disorder will lead to an increase in intestinal permeability, the damage of tight junction proteins to a certain extent, and the damage to the intestinal mechanical barrier [197].
Probiotics play a positive role in human health mainly by maintaining microbial balance and inhibiting the growth of harmful bacteria or pathogens. Studies have shown that whether probiotics can inhibit the growth of harmful bacteria through competition mainly depends on the ability of probiotic strain combinations to inhibit, displace, or interfere in the process of adhesion of pathogenic strains [198,199,200]. The inhibition of adhesion of probiotics to pathogens is achieved by steric hindrance at the level of intestinal receptors, competitive exclusion of nutrients and mucosal adhesion sites, and promotion of intestinal mucin changes [201,202]. Specifically, probiotics contribute to the maintenance of intestinal barrier function by promoting mucus secretion (a gel layer that provides protection against harmful bacteria or antigens by acting as a lubricant to improve intestinal movement and binding carbohydrates to the surface of epithelial cells) [203,204]. In addition, probiotics have beneficial effects by producing enzymes and beneficial metabolites, facilitating synthesis, and enhancing the absorption of beneficial substances. Another important mechanism by which probiotics participate in the regulation of gut microbiota is through the production of different antibacterial substances such as bacteriocin, SCFAs, and deconjugated bile acid. SCFAs such as butyric, propionic, lactic and acetic acid are some of the compounds produced by probiotics after they metabolize carbohydrates, which reduce the total pH of the small intestine and inhibit the growth of pathogenic bacteria [205]. The bactericidal action of bacteriocin mainly involves the formation of pores in the membrane, which are harmful to target cells and inhibit cell wall synthesis to achieve the relative stability of intestinal microorganisms [206]. In addition, probiotics may improve intestinal immunity by stimulating secretory IgA production and enhancing gut–brain communication. Recent studies have highlighted the potential of probiotics to stimulate the intestinal immune system by activating the aromatic hydrocarbon receptor (AhR) pathway, which is an important inflammatory regulator [207,208].
Prebiotics are defined as health-beneficial substrates selectively utilized by host microbes that preferentially stimulate the growth of a limited number of health-promoting bacteria in the gut and exert health benefits, including beneficial effects on gastrointestinal cognitive function, cardiometabolic health, and bone strength [205].
Synbiotics refer to the combination of prebiotics and probiotics: a mixture of living microbes and substrates selectively utilized by host microbes that exhibit synergistic effects and have a positive effect on the host [209]. The independence of the synbiotic components has been interpreted differently. One is independent selection, meaning that each ingredient is responsible for its specific effects, in which prebiotics are not necessarily preferentially metabolized by the probiotic strain and can be fermented by the host microbiota. The other is synergistic, in which prebiotics are specifically selected as substrates for particular strains of probiotics to support their growth [210].
Although there is evidence of the effectiveness and mechanisms of various interventions to modify gastrointestinal microbiota, there is still much work that needs to be completed. For example, differences in patient clinical characteristics lead to different responses to the administration of the same prebiotics/probiotics/synbiotics, which means that various factors, such as age, sex, diet, bowel habits, and microbiome composition can influence and help predict the outcome of interventions. At the same time, the effectiveness of various interventions should be evaluated from overall symptom improvement to more specific and overall symptom improvement, such as increased fecal frequency, metabolic protein levels, or reduction in abdominal distention or pain.
In addition, existing studies have focused on probiotics, and the effectiveness of other measures to improve the gut microbiota is not completely clear. There is a lack of reliable prospective studies for repeated validation. For example, existing trials still differed in FMT delivery methods, bacterial dose, fecal filtration methods, and administration frequency, and they failed to control for other donor factors, such as diet. Although original literature on brain-derived neurotrophic factors in Alzheimer’s or cortisol in stress may exist, no meta-analysis on the relationship between gastrointestinal microbiome changes and them was found. This might be a good direction for future research. In addition, many studies have proved that changes in the gastrointestinal microbiome are related to the occurrence of diseases, but no consensus has been reached on the causal relationship between the two. In other words, whether the disease breaks the balance of the gastrointestinal microbiome or the disorder of the gastrointestinal microbiome leads to the disease or whether there is a two-way effect between the two still needs to be confirmed by further reliable studies [167,168,171].
Overall, a number of factors contribute to changes in gut microbiota, which in turn have an impact on health outcomes. However, due to the large heterogeneity, the diversity of intestinal flora detection and the uncontrollability of other influencing factors, rigorous and credible meta-analyses are in short supply. Furthermore, there is still a lack of direct evidence linking specific changes in gut flora to health outcomes.
5. Conclusions
In summary, the gastrointestinal microbiome is closely associated with human health outcomes. Probiotics, prebiotics, synbiotics and FMT commonly used today are generally safe and beneficial to a variety of human health outcomes. Other interventions, such as traditional Chinese medicine, low FODMAP diet, and dietary fiber, have gradually shown positive results. In addition, the gastrointestinal microbiome is associated with the occurrence and development of a variety of diseases, but the causal relationship is still worth further investigation. However, the quality of evidence is still insufficient, so high-quality prospective studies are needed in the future.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/nu14183726/s1, Table S1: Prebiotics/probiotics/synbiotics and multiple health outcomes; Table S2: Prebiotics/probiotics/synbiotics and mortality; Table S3: Prebiotics/probiotics/synbiotics and immune and metabolic outcomes; Table S4: Prebiotics/probiotics/synbiotics and immune and gastrointestinal disease; Table S5: Prebiotics/probiotics/synbiotics neurological and psychiatric outcomes; Table S6: Prebiotics/probiotics/synbiotics and maternal and infant outcomes; Table S7: Prebiotics/probiotics/synbiotics and other outcomes; Table S8: Prebiotics/probiotics/synbiotics and side effects; Table S9: Fecal microbiota transplant and multiple health outcomes; Table S10: Other interventions and multiple health outcomes; Table S11: Association between disease and changes in gastrointestinal microbiota and its metabolites; Table S12: AMSTAR2; Table S13: GRADE.
Author Contributions
K.L. conceived the study. C.C. and X.Y. performed literature retrieval, literature screening, data extraction, analysis and interpretation. C.C. wrote the manuscript under the guidance of K.L., X.Z. and X.C. provided guidance in framing the review. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the key research and development project of Science & Technology Department of Sichuan Province (No. 2021YFS0022).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bull, M.J.; Plummer, N.T. Part 1: The Human Gut Microbiome in Health and Disease. Integr. Med. 2014, 13, 17–22. [Google Scholar]
- Hakansson, A.; Molin, G. Gut microbiota and inflammation. Nutrients 2011, 3, 637–682. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Kolodziejczyk, A.A.; Thaiss, C.A.; Elinav, E. Dysbiosis and the immune system. Nat. Rev. Immunol. 2017, 17, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Sparks, J.B.; Karyala, S.V.; Settlage, R.; Luo, X.M. Host adaptive immunity alters gut microbiota. ISME J. 2015, 9, 770–781. [Google Scholar] [CrossRef]
- Rothschild, D.; Weissbrod, O.; Barkan, E.; Kurilshikov, A.; Korem, T.; Zeevi, D.; Costea, P.I.; Godneva, A.; Kalka, I.N.; Bar, N.; et al. Environment dominates over host genetics in shaping human gut microbiota. Nature 2018, 555, 210–215. [Google Scholar] [CrossRef]
- Valdes, A.M.; Walter, J.; Segal, E.; Spector, T.D. Role of the gut microbiota in nutrition and health. BMJ 2018, 361, k2179. [Google Scholar] [CrossRef]
- Wang, C.; Gao, Z.; Qian, Y.; Li, X.; Wang, J.; Ma, J.; Guo, J.; Fu, F. Effects of Different Concentrations of Ganpu Tea on Fecal Microbiota and Short Chain Fatty Acids in Mice. Nutrients 2021, 13, 3715. [Google Scholar] [CrossRef]
- Lin, H.V.; Frassetto, A.; Kowalik, E.J.J.; Nawrocki, A.R.; Lu, M.M.; Kosinski, J.R.; Hubert, J.A.; Szeto, D.; Yao, X.; Forrest, G.; et al. Butyrate and propionate protect against diet-induced obesity and regulate gut hormones via free fatty acid receptor 3-independent mechanisms. PLoS ONE 2012, 7, e35240. [Google Scholar] [CrossRef]
- Qi, J.; You, T.; Li, J.; Pan, T.; Xiang, L.; Han, Y.; Zhu, L. Circulating trimethylamine N-oxide and the risk of cardiovascular diseases: A systematic review and meta-analysis of 11 prospective cohort studies. J. Cell. Mol. Med. 2018, 22, 185–194. [Google Scholar] [CrossRef]
- Yao, M.; Liao, P.; Zhao, X.; Wang, L. Trimethylamine-N-oxide has prognostic value in coronary heart disease: A meta-analysis and dose-response analysis. BMC Cardiovasc. Disor. 2020, 20. [Google Scholar] [CrossRef]
- Qin, J.; Li, Y.; Cai, Z.; Li, S.; Zhu, J.; Zhang, F.; Liang, S.; Zhang, W.; Guan, Y.; Shen, D.; et al. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature 2012, 490, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Yatsunenko, T.; Rey, F.E.; Manary, M.J.; Trehan, I.; Dominguez-Bello, M.G.; Contreras, M.; Magris, M.; Hidalgo, G.; Baldassano, R.N.; Anokhin, A.P.; et al. Human gut microbiome viewed across age and geography. Nature 2012, 486, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Goodrich, J.K.; Waters, J.L.; Poole, A.C.; Sutter, J.L.; Koren, O.; Blekhman, R.; Beaumont, M.; Van Treuren, W.; Knight, R.; Bell, J.T.; et al. Human genetics shape the gut microbiome. Cell 2014, 159, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.H.; Pothoulakis, C.; Mayer, E.A. Principles and clinical implications of the brain-gut-enteric microbiota axis. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 306–314. [Google Scholar] [CrossRef]
- Agirman, G.; Hsiao, E.Y. SnapShot: The microbiota-gut-brain axis. Cell 2021, 184, 2524. [Google Scholar] [CrossRef]
- Fung, T.C.; Olson, C.A.; Hsiao, E.Y. Interactions between the microbiota, immune and nervous systems in health and disease. Nat. Neurosci. 2017, 20, 145–155. [Google Scholar] [CrossRef]
- Cryan, J.F.; O’Riordan, K.J.; Cowan, C.S.M.; Sandhu, K.V.; Bastiaanssen, T.F.S.; Boehme, M.; Codagnone, M.G.; Cussotto, S.; Fulling, C.; Golubeva, A.V.; et al. The Microbiota-Gut-Brain Axis. Physiol. Rev. 2019, 99, 1877–2013. [Google Scholar] [CrossRef]
- Farzi, A.; Fröhlich, E.E.; Holzer, P. Gut Microbiota and the Neuroendocrine System. Neurotherapeutics. 2018, 15, 5–22. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Integration of evidence from multiple meta-analyses: A primer on umbrella reviews, treatment networks and multiple treatments meta-analyses. CMAJ 2009, 181, 488–493. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schunemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Search filters. Available online: https://www.sign.ac.uk/what-we-do/methodology/search-filters/ (accessed on 31 August 2021).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2019. [Google Scholar]
- Egger, M.; Davey, S.G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Dermyshi, E.; Wang, Y.; Yan, C.; Hong, W.; Qiu, G.; Gong, X.; Zhang, T. The “Golden Age” of Probiotics: A Systematic Review and Meta-Analysis of Randomized and Observational Studies in Preterm Infants. Neonatology 2017, 112, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Sharif, S.; Meader, N.; Oddie, S.J.; Rojas-Reyes, M.X.; Mcguire, W. Probiotics to prevent necrotising enterocolitis in very preterm or very low birth weight infants. Cochrane Database Syst. Rev. 2020, 10, CD5496. [Google Scholar] [CrossRef]
- Yang, Y.; Guo, Y.; Kan, Q.; Zhou, X.G.; Zhou, X.Y.; Li, Y. A meta-analysis of probiotics for preventing necrotizing enterocolitis in preterm neonates. Braz. J. Med. Biol. Res. 2014, 47, 804–810. [Google Scholar] [CrossRef]
- Jiang, T.; Zhang, H.; Xu, X.; Li, H.; Yang, J. Mixed probiotics decrease the incidence of stage II-III necrotizing enterocolitis and death: A systematic review and meta-analysis. Microb. Pathog. 2020, 138, 103794. [Google Scholar] [CrossRef]
- Liu, D.; Shao, L.; Zhang, Y.; Kang, W. Safety and efficacy of Lactobacillus for preventing necrotizing enterocolitis in preterm infants. Int. J. Surg. 2020, 76, 79–87. [Google Scholar] [CrossRef]
- Zhu, X.; Tang, X.; Qu, F.; Zheng, Y.; Zhang, W.; Diao, Y. Bifidobacterium may benefit the prevention of necrotizing enterocolitis in preterm infants: A systematic review and meta-analysis. Int. J. Surg. 2019, 61, 17–25. [Google Scholar] [CrossRef]
- Chi, C.; Buys, N.; Li, C.; Sun, J.; Yin, C. Effects of prebiotics on sepsis, necrotizing enterocolitis, mortality, feeding intolerance, time to full enteral feeding, length of hospital stay, and stool frequency in preterm infants: A meta-analysis. Eur. J. Clin. Nutr. 2019, 73, 657–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalal, R.; Mcgee, R.G.; Riordan, S.M.; Webster, A.C. Probiotics for people with hepatic encephalopathy. Cochrane Database Syst. Rev. 2017, 2, CD8716. [Google Scholar] [CrossRef]
- Skonieczna-żydecka, K.; Kaczmarczyk, M.; łoniewski, I.; Lara, L.; Koulaouzidis, A.; Misera, A.; Maciejewska, D.; Marlicz, W. A Systematic Review, Meta-Analysis, and Meta-Regression Evaluating the Efficacy and Mechanisms of Action of Probiotics and Synbiotics in the Prevention of Surgical Site Infections and Surgery-Related Complications. J. Clin. Med. 2018, 7, 556. [Google Scholar] [CrossRef]
- Kinross, J.M.; Markar, S.; Karthikesalingam, A.; Chow, A.; Penney, N.; Silk, D.; Darzi, A. A Meta-Analysis of Probiotic and Synbiotic Use in Elective Surgery. J. Parenter. Enter. Nutr. 2013, 37, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.M.; Tian, Z.W.; Li, M.; Li, B.; Cui, W.W. Effects of probiotic supplementation on the regulation of blood lipid levels in overweight or obese subjects: A meta-analysis. Food Funct. 2019, 10, 1747–1759. [Google Scholar] [CrossRef]
- Beserra, B.T.S.; Fernandes, R.; Do Rosario, V.A.; Mocellin, M.C.; Kuntz, M.G.F.; Trindade, E.B.S.M. A systematic review and meta-analysis of the prebiotics and synbiotics effects on glycaemia, insulin concentrations and lipid parameters in adult patients with overweight or obesity. Clin. Nutr. 2015, 34, 845–858. [Google Scholar] [CrossRef]
- Cozzolino, M.; Vitagliano, A.; Pellegrini, L.; Chiurazzi, M.; Andriasani, A.; Ambrosini, G.; Garrido, N. Therapy with probiotics and synbiotics for polycystic ovarian syndrome: A systematic review and meta-analysis. Eur. J. Nutr. 2020, 59, 2841–2856. [Google Scholar] [CrossRef]
- Li, Y.; Tan, Y.; Xia, G.; Shuai, J. Effects of probiotics, prebiotics, and synbiotics on polycystic ovary syndrome: A systematic review and meta-analysis. Crit. Rev. Food Sci. 2021, 1–17. [Google Scholar] [CrossRef]
- Khalesi, S.; Johnson, D.W.; Campbell, K.; Williams, S.; Fenning, A.; Saluja, S.; Irwin, C. Effect of probiotics and synbiotics consumption on serum concentrations of liver function test enzymes: A systematic review and meta-analysis. Eur. J. Nutr. 2018, 57, 2037–2053. [Google Scholar] [CrossRef]
- Loman, B.R.; Hernández-Saavedra, D.; An, R.; Rector, R.S. Prebiotic and probiotic treatment of nonalcoholic fatty liver disease: A systematic review and meta-analysis. Nutr. Rev. 2018, 76, 822–839. [Google Scholar] [CrossRef]
- As Habi, A.; Nazari, M.; Hajianfar, H.; Arab, A.; Faghfoori, Z. A systematic review and meta-analysis of probiotic consumption and metabolic status of athletes. Int. J. Food Prop. 2020, 23, 941–954. [Google Scholar] [CrossRef]
- Khan, M.Y.; Mihali, A.B.; Rawala, M.S.; Aslam, A.; Siddiqui, W.J. The promising role of probiotic and synbiotic therapy in aminotransferase levels and inflammatory markers in patients with nonalcoholic fatty liver disease—A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiary, M.; Morvaridzadeh, M.; Agah, S.; Rahimlou, M.; Christopher, E.; Zadro, J.R.; Heshmati, J. Effect of Probiotic, Prebiotic, and Synbiotic Supplementation on Cardiometabolic and Oxidative Stress Parameters in Patients with Chronic Kidney Disease: A Systematic Review and Meta-analysis. Clin. Ther. 2021, 43, e71–e96. [Google Scholar] [CrossRef]
- Hadi, A.; Arab, A.; Khalesi, S.; Rafie, N.; Kafeshani, M.; Kazemi, M. Effects of probiotic supplementation on anthropometric and metabolic characteristics in adults with metabolic syndrome: A systematic review and meta-analysis of randomized clinical trials. Clin. Nutr. 2021, 40, 4662–4673. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hu, Y.; Yuan, X.; Yang, J.; Ka, L. Effect of early enteral nutrition combined with probiotics in patients with stroke: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2022, 76, 592–603. [Google Scholar] [CrossRef] [PubMed]
- Pontes, K.S.D.S.; Guedes, M.R.; Cunha, M.R.D.; Mattos, S.D.S.; Barreto Silva, M.I.; Neves, M.F.; Marques, B.C.A.A.; Klein, M.R.S.T. Effects of probiotics on body adiposity and cardiovascular risk markers in individuals with overweight and obesity: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 4915–4931. [Google Scholar] [CrossRef]
- Den, H.; Dong, X.; Chen, M.; Zou, Z. Efficacy of probiotics on cognition, and biomarkers of inflammation and oxidative stress in adults with Alzheimer’s disease or mild cognitive impairment—A meta-analysis of randomized controlled trials. Aging 2020, 12, 4010–4039. [Google Scholar] [CrossRef]
- Milajerdi, A.; Mousavi, S.M.; Sadeghi, A.; Salari-Moghaddam, A.; Parohan, M.; Larijani, B.; Esmaillzadeh, A. The effect of probiotics on inflammatory biomarkers: A meta-analysis of randomized clinical trials. Eur. J. Nutr. 2020, 59, 633–649. [Google Scholar] [CrossRef]
- Pan, H.; Li, R.; Li, T.; Wang, J.; Liu, L. Whether Probiotic Supplementation Benefits Rheumatoid Arthritis Patients: A Systematic Review and Meta-Analysis. Engineering 2017, 3, 115–121. [Google Scholar] [CrossRef]
- Tavakoly, R.; Hadi, A.; Rafie, N.; Talaei, B.; Marx, W.; Arab, A. Effect of Probiotic Consumption on Immune Response in Athletes: A Meta-analysis. Int. J. Sports Med. 2021, 42, 769–781. [Google Scholar] [CrossRef]
- Jia, L.; Jia, Q.; Yang, J.; Jia, R.; Zhang, H. Efficacy of Probiotics Supplementation On Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Kidney Blood Press. Res. 2018, 43, 1623–1635. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Kaewput, W.; Hatch, S.T.; Bathini, T.; Sharma, K.; Wijarnpreecha, K.; Ungprasert, P.; D’Costa, M.; Mao, M.A.; Cheungpasitporn, W. Effects of Probiotics on Inflammation and Uremic Toxins Among Patients on Dialysis: A Systematic Review and Meta-Analysis. Digest. Dis. Sci. 2019, 64, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.; Zhang, Y.; Chai, H.; Gao, Z.; Shi, D. Effects of microbiota-driven therapy on inflammatory responses in elderly individuals: A systematic review and meta-analysis. PLoS ONE 2019, 14, e211233. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Ren, Z.; Zang, Y.; Hua, H.; Lu, J.; Xu, Q.; Zhu, S. Effects of Microecological Preparations on Obese Patients after Bariatric Surgery: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2020, 2020, 8724546. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xin, S.; Ding, L.; Ding, W.; Hou, Y.; Liu, C.; Zhang, X. The Potential Role of Probiotics in Controlling Overweight/Obesity and Associated Metabolic Parameters in Adults: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2019, 2019, 3862971. [Google Scholar] [CrossRef]
- Bock, P.M.; Telo, G.H.; Ramalho, R.; Sbaraini, M.; Leivas, G.; Martins, A.F.; Schaan, B.D. The effect of probiotics, prebiotics or synbiotics on metabolic outcomes in individuals with diabetes: A systematic review and meta-analysis. Diabetologia 2021, 64, 26–41. [Google Scholar] [CrossRef]
- Chi, C.; Li, C.; Wu, D.; Buys, N.; Wang, W.; Fan, H.; Sun, J. Effects of Probiotics on Patients with Hypertension: A Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2020, 22. [Google Scholar] [CrossRef]
- Cao, Q.; Yu, C.; Yang, S.; Cao, H.; Chen, P.; Deng, M.; Li, L. Effect of probiotic treatment on cirrhotic patients with minimal hepatic encephalopathy: A meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 9–16. [Google Scholar] [CrossRef]
- Askari, G.; Ghavami, A.; Shahdadian, F.; Moravejolahkami, A.R. Effect of synbiotics and probiotics supplementation on autoimmune diseases: A systematic review and meta-analysis of clinical trials. Clin. Nutr. 2021, 40, 3221–3234. [Google Scholar] [CrossRef]
- Malmir, H.; Ejtahed, H.; Soroush, A.; Mortazavian, A.M.; Fahimfar, N.; Ostovar, A.; Esmaillzadeh, A.; Larijani, B.; Hasani-Ranjbar, S. Probiotics as a New Regulator for Bone Health: A Systematic Review and Meta-Analysis. Evid. -Based Complement. Altern. Med. 2021, 2021, 3582989. [Google Scholar] [CrossRef]
- Tao, S.B.; Tao, S.Y.; Cheng, Y.M.; Liu, J.; Ma, L.; Fu, P. Effects of probiotic supplements on the progression of chronic kidney disease: A meta-analysis. Nephrology 2019, 24, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Mcfarlane, C.; Ramos, C.I.; Johnson, D.W.; Campbell, K.L. Prebiotic, Probiotic, and Synbiotic Supplementation in Chronic Kidney Disease: A Systematic Review and Meta-analysis. J. Ren. Nutr. 2019, 29, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Zhu, X.; Shang, F.; Zhang, X. Preventive Effect of Probiotics on Ventilator-Associated Pneumonia: A Meta-analysis of 2428 Patients. Ann. Pharmacother. 2021, 55, 949–962. [Google Scholar] [CrossRef]
- Guo, Q.; Goldenberg, J.Z.; Humphrey, C.; Dib, R.E.; Johnston, B. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Gastroenterology 2019, 156, 220. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, J.Z.; Yap, C.; Lytvyn, L.; Lo, C.K.; Beardsley, J.; Mertz, D.; Johnston, B.C. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst. Rev. 2017, 2017, D6095. [Google Scholar] [CrossRef]
- Wu, Z.J.; Du, X.; Zheng, J. Role of Lactobacillus in the prevention of Clostridium difficile-associated diarrhea: A meta-analysis of randomized controlled trials. Chin. Med. J. 2013, 126, 4154–4161. [Google Scholar] [PubMed]
- Johnston, B.C.; Ma, S.S.Y.; Goldenberg, J.Z.; Thorlund, K.; Vandvik, P.O.; Loeb, M.; Guyatt, G.H. Probiotics for the prevention of clostridium difficile-associated diarrhea. Ann. Intern. Med. 2012, 157, 878. [Google Scholar] [CrossRef]
- Shen, N.T.; Maw, A.; Tmanova, L.L.; Pino, A.; Ancy, K.; Crawford, C.V.; Simon, M.S.; Evans, A.T. Timely Use of Probiotics in Hospitalized Adults Prevents Clostridium difficile Infection: A Systematic Review With Meta-Regression Analysis. Gastroenterology 2017, 152, 1889–1900. [Google Scholar] [CrossRef]
- Goodman, C.; Keating, G.; Georgousopoulou, E.; Hespe, C.; Levett, K. Probiotics for the prevention of antibiotic-associated diarrhoea: A systematic review and meta-analysis. BMJ Open 2021, 11, e43054. [Google Scholar] [CrossRef]
- Jafarnejad, S.; Shab-Bidar, S.; Speakman, J.R.; Parastui, K.; Daneshi-Maskooni, M.; Djafarian, K. Probiotics Reduce the Risk of Antibiotic-Associated Diarrhea in Adults (18–64 Years) but Not the Elderly (>65 Years). Nutr. Clin. Pract. 2016, 31, 502–513. [Google Scholar] [CrossRef] [PubMed]
- Blaabjerg, S.; Artzi, D.; Aabenhus, R. Probiotics for the Prevention of Antibiotic-Associated Diarrhea in Outpatients—A Systematic Review and Meta-Analysis. Antibiotics 2017, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Xu, W.; Liu, M.; Hu, K.; Sun, Y.; Yang, X.; Zhu, G.; Wang, Z.; Huang, W. Efficacy of prophylactic probiotics in combination with antibiotics versus antibiotics alone for colorectal surgery: A meta-analysis of randomized controlled trials. J. Surg. Oncol. 2018, 117, 1394–1404. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, M.; Geng, S.; Yu, J.; Kuang, Y.; Luo, H.; Wang, K. Effects of Probiotics on Diarrhea and CD4 Cell Count in People Living With HIV: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2021, 12, 570520. [Google Scholar] [CrossRef]
- Lohner, S.; Küllenberg, D.; Antes, G.; Decsi, T.; Meerpohl, J.J. Prebiotics in healthy infants and children for prevention of acute infectious diseases: A systematic review and meta-analysis. Nutr. Rev. 2014, 72, 523–531. [Google Scholar] [CrossRef]
- Ford, A.C.; Harris, L.A.; Lacy, B.E.; Quigley, E.M.M.; Moayyedi, P. Systematic review with meta-analysis: The efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2018, 48, 1044–1060. [Google Scholar] [CrossRef] [PubMed]
- Asha, M.Z.; Khalil, S.F.H. Efficacy and Safety of Probiotics, Prebiotics and Synbiotics in the Treatment of Irritable Bowel Syndrome: A systematic review and meta-analysis. Sultan Qaboos Univ. Med. J. SQUMJ 2020, 20, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zou, L.; Chen, M.; Wang, H.; Shen, W.; Zheng, Q.; Cui, W. Efficacy of probiotic adjuvant therapy for irritable bowel syndrome in children: A systematic review and meta-analysis. PLoS ONE 2021, 16, e255160. [Google Scholar] [CrossRef]
- Connell, M.; Shin, A.; James-Stevenson, T.; Xu, H.; Imperiale, T.F.; Herron, J. Systematic review and meta-analysis: Efficacy of patented probiotic, VSL#3, in irritable bowel syndrome. Neurogastroenterol. Motil. 2018, 30, e13427. [Google Scholar] [CrossRef]
- Yuan, F.; Ni, H.; Asche, C.V.; Kim, M.; Walayat, S.; Ren, J. Efficacy ofBifidobacterium infantis 35624 in patients with irritable bowel syndrome: A meta-analysis. Curr. Med. Res. Opin. 2017, 33, 1191–1197. [Google Scholar] [CrossRef]
- Huang, R.; Hu, J. Positive Effect of Probiotics on Constipation in Children: A Systematic Review and Meta-Analysis of Six Randomized Controlled Trials. Front. Cell. Infect. Microbiol. 2017, 7, 153. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Jiang, J.; Tian, F.; Zhao, J.; Zhang, H.; Zhai, Q.; Chen, W. Meta-analysis of randomized controlled trials of the effects of probiotics on functional constipation in adults. Clin. Nutr. 2020, 39, 2960–2969. [Google Scholar] [CrossRef] [PubMed]
- Zhong, C.; Qu, C.; Wang, B.; Liang, S.; Zeng, B. Probiotics for Preventing and Treating Small Intestinal Bacterial Overgrowth. J. Clin. Gastroenterol. 2017, 51, 300–311. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Li, J.; Long, Q.; Yue, C.; He, B.; Tang, X. The efficacy and safety of probiotics for patients with constipation-predominant irritable bowel syndrome: A systematic review and meta-analysis based on seventeen randomized controlled trials. Int. J. Surg. 2020, 79, 111–119. [Google Scholar] [CrossRef]
- Wilson, B.; Rossi, M.; Dimidi, E.; Whelan, K. Prebiotics in irritable bowel syndrome and other functional bowel disorders in adults: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2019, 109, 1098–1111. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, K.; Cawood, A.L.; Gibson, G.R.; Cooke, L.H.; Stratton, R.J. Amino Acid Formula Containing Synbiotics in Infants with Cow’s Milk Protein Allergy: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 935. [Google Scholar] [CrossRef]
- Seiler, C.L.; Kiflen, M.; Stefanolo, J.P.; Bai, J.C.; Bercik, P.; Kelly, C.P.; Verdu, E.F.; Moayyedi, P.; Pinto-Sanchez, M.I. Probiotics for Celiac Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Gastroenterol. 2020, 115, 1584–1595. [Google Scholar] [CrossRef]
- Losurdo, G.; Cubisino, R.; Barone, M.; Principi, M.; Leandro, G.; Ierardi, E.; Leo, A.D. Probiotic monotherapy and Helicobacter pylori eradication: A systematic review with pooled-data analysis. World J. Gastroenterol. 2018, 24, 139–149. [Google Scholar] [CrossRef]
- Rufino, M.N.; Da Costa, A.L.; Jorge, E.N.; Paiano, V.F.; Camparoto, M.L.; Keller, R.; Bremer-Neto, H. Synbiotics improve clinical indicators of ulcerative colitis: Systematic review with meta-analysis. Nutr. Rev. 2022, 80, 157–164. [Google Scholar] [CrossRef]
- Peng, L.; Zhong, Y.; Wang, A.; Jiang, Z. Probiotics combined with aminosalicylic acid affiliates remission of ulcerative colitis: A meta-analysis of randomized controlled trial. Biosci. Rep. 2019, 39, BSR20180943. [Google Scholar] [CrossRef]
- Losurdo, G.; Iannone, A.; Contaldo, A.; Ierardi, E.; Di Leo, A.; Principi, M. Escherichia coli Nissle 1917 in Ulcerative Colitis Treatment: Systematic Review and Meta-analysis. J. Gastrointest. Liver Dis. 2020, 24, 499–505. [Google Scholar] [CrossRef]
- Iheozor-Ejiofor, Z.; Kaur, L.; Gordon, M.; Baines, P.A.; Sinopoulou, V.; Akobeng, A.K. Probiotics for maintenance of remission in ulcerative colitis. Cochrane Database Syst. Rev. 2020, 3, D7443. [Google Scholar] [CrossRef]
- Astó, E.; Méndez, I.; Audivert, S.; Farran-Codina, A.; Espadaler, J. The Efficacy of Probiotics, Prebiotic Inulin-Type Fructans, and Synbiotics in Human Ulcerative Colitis: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 293. [Google Scholar] [CrossRef] [PubMed]
- Dang, X.; Xu, M.; Liu, D.; Zhou, D.; Yang, W. Assessing the efficacy and safety of fecal microbiota transplantation and probiotic VSL#3 for active ulcerative colitis: A systematic review and meta-analysis. PLoS ONE 2020, 15, e228846. [Google Scholar] [CrossRef]
- Kaur, L.; Gordon, M.; Baines, P.A.; Iheozor-Ejiofor, Z.; Sinopoulou, V.; Akobeng, A.K. Probiotics for induction of remission in ulcerative colitis. Cochrane Database Syst. Rev. 2020, 2020, D5573. [Google Scholar] [CrossRef]
- Pabón-Carrasco, M.; Ramirez-Baena, L.; Vilar-Palomo, S.; Castro-Méndez, A.; Martos-García, R.; Rodríguez-Gallego, I. Probiotics as a Coadjuvant Factor in Active or Quiescent Inflammatory Bowel Disease of Adults—A Meta-Analytical Study. Nutrients 2020, 12, 2628. [Google Scholar] [CrossRef]
- Zhang, X.; Guan, X.; Tang, Y.; Sun, J.; Wang, X.; Wang, W.; Fan, J. Clinical effects and gut microbiota changes of using probiotics, prebiotics or synbiotics in inflammatory bowel disease: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 2855–2875. [Google Scholar] [CrossRef]
- Derwa, Y.; Gracie, D.J.; Hamlin, P.J.; Ford, A.C. Systematic review with meta-analysis: The efficacy of probiotics in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 46, 389–400. [Google Scholar] [CrossRef]
- Lv, T.; Ye, M.; Luo, F.; Hu, B.; Wang, A.; Chen, J.; Yan, J.; He, Z.; Chen, F.; Qian, C.; et al. Probiotics treatment improves cognitive impairment in patients and animals: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 120, 159–172. [Google Scholar] [CrossRef]
- Krüger, J.F.; Hillesheim, E.; Pereira, A.C.S.N.; Camargo, C.Q.; Rabito, E.I. Probiotics for dementia: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2021, 79, 160–170. [Google Scholar] [CrossRef]
- Mckean, J.; Naug, H.; Nikbakht, E.; Amiet, B.; Colson, N. Probiotics and Subclinical Psychological Symptoms in Healthy Participants: A Systematic Review and Meta-Analysis. J. Altern. Complementary Med. 2017, 23, 249–258. [Google Scholar] [CrossRef]
- Goh, K.K.; Liu, Y.; Kuo, P.; Chung, Y.E.; Lu, M.; Chen, C. Effect of probiotics on depressive symptoms: A meta-analysis of human studies. Psychiatry Res. 2019, 282, 112568. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Venkatanarayanan, N.; Ho, C.Y.X.; Lim, D.Y.; Yeo, W. A Systematic Review of the Effect of Probiotic Supplementation on Schizophrenia Symptoms. Neuropsychobiology 2019, 78, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Davidson, S.J.; Barrett, H.L.; Price, S.A.; Callaway, L.K.; Dekker Nitert, M. Probiotics for preventing gestational diabetes. Cochrane Database Syst. Rev. 2021, 2021, D9951. [Google Scholar] [CrossRef]
- Liu, R.T.; Walsh, R.F.L.; Sheehan, A.E. Prebiotics and probiotics for depression and anxiety: A systematic review and meta-analysis of controlled clinical trials. Neurosci. Biobehav. Rev. 2019, 102, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Ong, T.G.; Gordon, M.; Banks, S.S.; Thomas, M.R.; Akobeng, A.K. Probiotics to prevent infantile colic. Cochrane Database Syst. Rev. 2019, 3, CD012473. [Google Scholar] [CrossRef] [PubMed]
- Skonieczna-żydecka, K.; Janda, K.; Kaczmarczyk, M.; Marlicz, W.; łoniewski, I.; łoniewska, B. The Effect of Probiotics on Symptoms, Gut Microbiota and Inflammatory Markers in Infantile Colic: A Systematic Review, Meta-Analysis and Meta-Regression of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 999. [Google Scholar] [CrossRef]
- Sung, V.; Collett, S.; de Gooyer, T.; Hiscock, H.; Tang, M.; Wake, M. Probiotics to Prevent or Treat Excessive Infant Crying. JAMA Pediatr. 2013, 167, 1150. [Google Scholar] [CrossRef]
- Han, M.; Sun, J.; Su, X.; Peng, Y.; Goyal, H.; Wu, C.; Zhu, X.; Li, L. Probiotics improve glucose and lipid metabolism in pregnant women: A meta-analysis. Ann. Transl. Med. 2019, 7, 99. [Google Scholar] [CrossRef]
- Sun, M.; Luo, J.; Liu, H.; Xi, Y.; Lin, Q. Can Mixed Strains of Lactobacillus and Bifidobacterium Reduce Eczema in Infants under Three Years of Age? A Meta-Analysis. Nutrients 2021, 13, 1461. [Google Scholar] [CrossRef]
- Szajewska, H.; Horvath, A. Lactobacillus rhamnosus GG in the Primary Prevention of Eczema in Children: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1319. [Google Scholar] [CrossRef]
- Nakamura, H.; Lim, T.; Puri, P. Probiotics for the prevention of Hirschsprung-associated enterocolitis: A systematic review and meta-analysis. Pediatr. Surg. Int. 2018, 34, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, R.P.; Taneja, S.; Chowdhury, R.; Strand, T.A.; Bhandari, N. Effect of prebiotic and probiotic supplementation on neurodevelopment in preterm very low birth weight infants: Findings from a meta-analysis. Pediatr. Res. 2020, 87, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Grev, J.; Berg, M.; Soll, R. Maternal probiotic supplementation for prevention of morbidity and mortality in preterm infants. Cochrane Database Syst. Rev. 2018, 2018, D12519. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Tung, Y.; Chang, H.; Lin, C.; Chen, Y. Effect of Probiotic Supplementation on Newborn Birth Weight for Mother with Gestational Diabetes Mellitus or Overweight/Obesity: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3477. [Google Scholar] [CrossRef] [PubMed]
- Hasain, Z.; Che Roos, N.A.; Rahmat, F.; Mustapa, M.; Raja Ali, R.A.; Mokhtar, N.M. Diet and Pre-Intervention Washout Modifies the Effects of Probiotics on Gestational Diabetes Mellitus: A Comprehensive Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 3045. [Google Scholar] [CrossRef]
- Kahn, J.; Pregartner, G.; Schemmer, P. Effects of both Pro- and Synbiotics in Liver Surgery and Transplantation with Special Focus on the Gut–Liver Axis—A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2461. [Google Scholar] [CrossRef] [PubMed]
- Sawas, T.; Al Halabi, S.; Hernaez, R.; Carey, W.D.; Cho, W.K. Patients Receiving Prebiotics and Probiotics Before Liver Transplantation Develop Fewer Infections Than Controls: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2015, 13, 1567–1574. [Google Scholar] [CrossRef]
- Yang, Z.; Wu, Q.; Liu, Y.; Fan, D. Effect of Perioperative Probiotics and Synbiotics on Postoperative Infections After Gastrointestinal Surgery: A Systematic Review with Meta-Analysis. J. Parenter. Enter. Nutr. 2017, 41, 1051–1062. [Google Scholar] [CrossRef]
- Chan, C.K.Y.; Tao, J.; Chan, O.S.; Li, H.; Pang, H. Preventing Respiratory Tract Infections by Synbiotic Interventions: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. Int. Rev. J. 2020, 11, 979–988. [Google Scholar] [CrossRef]
- Wang, Y.; Li, X.; Ge, T.; Xiao, Y.; Liao, Y.; Cui, Y.; Zhang, Y.; Ho, W.; Yu, G.; Zhang, T. Probiotics for prevention and treatment of respiratory tract infections in children. Medicine 2016, 95, e4509. [Google Scholar] [CrossRef]
- Miller, L.E.; Lehtoranta, L.; Lehtinen, M.J. Short-term probiotic supplementation enhances cellular immune function in healthy elderly: Systematic review and meta-analysis of controlled studies. Nutr. Res. 2019, 64, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Hu, H.; Liu, C.; Zhang, Q.; Shakya, S.; Li, Z. Probiotics for Prevention of Atopy and Food Hypersensitivity in Early Childhood. Medicine 2016, 95, e2562. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Wang, L.; Wu, S.; Yuan, L.; Tang, S.; Xiang, Y.; Qu, X.; Liu, H.; Qin, X.; Liu, C. Efficacy of probiotic supplementary therapy for asthma, allergic rhinitis, and wheeze: A meta-analysis of randomized controlled trials. Allergy Asthma Proc. 2019, 40, 250–260. [Google Scholar] [CrossRef]
- Stachowska, E.; Portincasa, P.; Jamioł-Milc, D.; Maciejewska-Markiewicz, D.; Skonieczna-żydecka, K. The Relationship between Prebiotic Supplementation and Anthropometric and Biochemical Parameters in Patients with NAFLD—A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 3460. [Google Scholar] [CrossRef] [PubMed]
- Sharpton, S.R.; Maraj, B.; Harding-Theobald, E.; Vittinghoff, E.; Terrault, N.A. Gut microbiome–targeted therapies in nonalcoholic fatty liver disease: A systematic review, meta-analysis, and meta-regression. Am. J. Clin. Nutr. 2019, 110, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Le Morvan De Sequeira, C.; Kaeber, M.; Cekin, S.E.; Enck, P.; Mack, I. The Effect of Probiotics on Quality of Life, Depression and Anxiety in Patients with Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3497. [Google Scholar] [CrossRef]
- Jiang, J.; Chu, C.; Wu, C.; Wang, C.; Zhang, C.; Li, T.; Zhai, Q.; Yu, L.; Tian, F.; Chen, W. Efficacy of probiotics in multiple sclerosis: A systematic review of preclinical trials and meta-analysis of randomized controlled trials. Food Funct. 2021, 12, 2354–2377. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Srinivasjois, R.; Patole, S. Prebiotic Supplementation in Full-term Neonates. Arch. Pediatr. Adolesc. Med. 2009, 163, 755–764. [Google Scholar] [CrossRef]
- Chang, Y.; Trivedi, M.K.; Jha, A.; Lin, Y.; Dimaano, L.; García-Romero, M.T. Synbiotics for Prevention and Treatment of Atopic Dermatitis. JAMA Pediatr. 2016, 170, 236. [Google Scholar] [CrossRef]
- Suzumura, E.A.; Bersch-Ferreira, Â.C.; Torreglosa, C.R.; Da Silva, J.T.; Coqueiro, A.Y.; Kuntz, M.G.F.; Chrispim, P.P.; Weber, B.; Cavalcanti, A.B. Effects of oral supplementation with probiotics or synbiotics in overweight and obese adults: A systematic review and meta-analyses of randomized trials. Nutr. Rev. 2019, 77, 430–450. [Google Scholar] [CrossRef]
- Mohammadi, H.; Ghavami, A.; Faghihimani, Z.; Sharifi, S.; Nattagh-Eshtivani, E.; Ziaei, R.; Miraghajani, M. Effects of probiotics fermented milk products on obesity measure among adults: A systematic review and meta-analysis of clinical trials. J. Funct. Foods 2021, 82, 104494. [Google Scholar] [CrossRef]
- Coffey, M.J.; Garg, M.; Homaira, N.; Jaffe, A.; Ooi, C.Y. Probiotics for people with cystic fibrosis. Cochrane Database Syst. Rev. 2020, 1, CD012949. [Google Scholar] [CrossRef] [PubMed]
- Hendijani, F.; Akbari, V. Probiotic supplementation for management of cardiovascular risk factors in adults with type II diabetes: A systematic review and meta-analysis. Clin. Nutr. 2018, 37, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Irwin, C.; Mccartney, D.; Ben, D.; Khalesi, S. Effects of probiotics and paraprobiotics on subjective and objective sleep metrics: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2020, 74, 1536–1549. [Google Scholar] [CrossRef]
- Lei, W.; Shih, P.; Liu, S.; Lin, C.; Yeh, T. Effect of Probiotics and Prebiotics on Immune Response to Influenza Vaccination in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2017, 9, 1175. [Google Scholar] [CrossRef]
- Yeh, T.; Shih, P.; Liu, S.; Lin, C.; Liu, J.; Lei, W.; Lin, C. The influence of prebiotic or probiotic supplementation on antibody titers after influenza vaccination: A systematic review and meta-analysis of randomized controlled trials. Drug Des. Dev. Ther. 2018, Volume 12, 217–230. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, H.M.; Wang, X.; Xie, J.; Li, X.; Ma, J.; Wang, F.; Tang, X. Efficacy of prebiotics and probiotics for functional dyspepsia. Medicine 2020, 99, e19107. [Google Scholar] [CrossRef]
- Sohail, G.; Xu, X.; Christman, M.C.; Tompkins, T.A. Probiotic Medilac-S® forthe induction of clinical remission in a Chinese population with ulcerative colitis: A systematic review and meta-analysis. World J. Clin. Cases 2018, 6, 961–984. [Google Scholar] [CrossRef]
- Pomares Bascuñana, R.Á.; Veses, V.; Sheth, C.C. Effectiveness of fecal microbiota transplant for the treatment ofClostridioides difficile diarrhea: A systematic review and meta-analysis. Lett. Appl. Microbiol. 2021, 73, 149–158. [Google Scholar] [CrossRef]
- Khan, M.Y.; Dirweesh, A.; Khurshid, T.; Siddiqui, W.J. Comparing fecal microbiota transplantation to standard-of-care treatment for recurrent Clostridium difficile infection: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1309–1317. [Google Scholar] [CrossRef]
- Ianiro, G.; Eusebi, L.H.; Black, C.J.; Gasbarrini, A.; Cammarota, G.; Ford, A.C. Systematic review with meta-analysis: Efficacy of faecal microbiota transplantation for the treatment of irritable bowel syndrome. Aliment. Pharmacol. Ther. 2019, 50, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldeira, L.D.F.; Borba, H.H.; Tonin, F.S.; Wiens, A.; Fernandez-Llimos, F.; Pontarolo, R. Fecal microbiota transplantation in inflammatory bowel disease patients: A systematic review and meta-analysis. PLoS ONE 2020, 15, e238910. [Google Scholar] [CrossRef] [PubMed]
- Cold, F.; Baunwall, S.M.D.; Dahlerup, J.F.; Petersen, A.M.; Hvas, C.L.; Hansen, L.H. Systematic review with meta-analysis: Encapsulated faecal microbiota transplantation—Evidence for clinical efficacy. Ther. Adv. Gastroenterol. 2021, 14, 1320557622. [Google Scholar] [CrossRef] [PubMed]
- Narula, N.; Kassam, Z.; Yuan, Y.; Colombel, J.; Ponsioen, C.; Reinisch, W.; Moayyedi, P. Systematic Review and Meta-analysis. Inflamm. Bowel Dis. 2017, 23, 1702–1709. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Dong, Y.; Huang, W.; Zhu, D.; Mao, H.; Su, P. Fecal Microbiota Transplantation for Ulcerative Colitis: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e157259. [Google Scholar] [CrossRef]
- Liu, X.; Li, Y.; Wu, K.; Shi, Y.; Chen, M. Fecal Microbiota Transplantation as Therapy for Treatment of Active Ulcerative Colitis: A Systematic Review and Meta-Analysis. Gastroenterol. Res. Pract. 2021, 2021, 6612970. [Google Scholar] [CrossRef]
- Proença, I.M.; Allegretti, J.R.; Bernardo, W.M.; de Moura, D.T.H.; Ponte Neto, A.M.; Matsubayashi, C.O.; Flor, M.M.; Kotinda, A.P.S.T.; de Moura, E.G.H. Fecal microbiota transplantation improves metabolic syndrome parameters: Systematic review with meta-analysis based on randomized clinical trials. Nutr. Res. 2020, 83, 1–14. [Google Scholar] [CrossRef]
- Tariq, R.; Furqan, F.; Pardi, D.; Khanna, S. 201 Efficacy of Fecal Microbiota Transplantation for Acute Graft Versus Host Disease in the Gut: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2019, 114, S123. [Google Scholar] [CrossRef]
- Zheng, Y.; Ding, Q.; Wei, Y.; Gou, X.; Tian, J.; Li, M.; Tong, X. Effect of traditional Chinese medicine on gut microbiota in adults with type 2 diabetes: A systematic review and meta-analysis. Phytomedicine 2021, 88, 153455. [Google Scholar] [CrossRef]
- Milajerdi, A.; Ebrahimi-Daryani, N.; Dieleman, L.A.; Larijani, B.; Esmaillzadeh, A. Association of Dietary Fiber, Fruit, and Vegetable Consumption with Risk of Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Adv. Nutr. Int. Rev. J. 2021, 12, 735–743. [Google Scholar] [CrossRef]
- Fatahi, S.; Matin, S.S.; Sohouli, M.H.; Găman, M.; Raee, P.; Olang, B.; Kathirgamathamby, V.; Santos, H.O.; Guimarães, N.S.; Shidfar, F. Association of dietary fiber and depression symptom: A systematic review and meta-analysis of observational studies. Complement. Ther. Med. 2021, 56, 102621. [Google Scholar] [CrossRef] [PubMed]
- van Lanen, A.; de Bree, A.; Greyling, A. Efficacy of a low-FODMAP diet in adult irritable bowel syndrome: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 3505–3522. [Google Scholar] [CrossRef] [PubMed]
- Zama, D.; Gori, D.; Muratore, E.; Leardini, D.; Rallo, F.; Turroni, S.; Prete, A.; Brigidi, P.; Pession, A.; Masetti, R. Enteral versus Parenteral Nutrition as Nutritional Support after Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis. Transplant. Cell. Ther. 2021, 27, 180–181. [Google Scholar] [CrossRef] [PubMed]
- Malagón-Rojas, J.N.; Mantziari, A.; Salminen, S.; Szajewska, H. Postbiotics for Preventing and Treating Common Infectious Diseases in Children: A Systematic Review. Nutrients 2020, 12, 389. [Google Scholar] [CrossRef]
- Salari, A.; Ghodrat, S.; Gheflati, A.; Jarahi, L.; Hashemi, M.; Afshari, A. Effect of kefir beverage consumption on glycemic control: A systematic review and meta-analysis of randomized controlled clinical trials. Complementary Ther. Clin. Pract. 2021, 44, 101443. [Google Scholar] [CrossRef]
- Jia, L.; Dong, X.; Li, X.; Jia, R.; Zhang, H. Benefits of resistant starch type 2 for patients with end-stage renal disease under maintenance hemodialysis: A systematic review and meta-analysis. Int. J. Med. Sci. 2021, 18, 811–820. [Google Scholar] [CrossRef]
- Jørgensen, A.R.; Egeberg, A.; Gideonsson, R.; Weinstock, L.B.; Thyssen, E.P.; Thyssen, J.P. Rosacea is associated with Helicobacter pylori: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. 2017, 31, 2010–2015. [Google Scholar] [CrossRef]
- Capurso, G.; Signoretti, M.; Archibugi, L.; Stigliano, S.; Delle Fave, G. Systematic review and meta-analysis: Small intestinal bacterial overgrowth in chronic pancreatitis. United Eur. Gastroenterol. J. 2016, 4, 697–705. [Google Scholar] [CrossRef]
- Shah, A.; Shanahan, E.; Macdonald, G.; Fletcher, L.; Ghasemi, P.; Morrison, M.; Jones, M.; Holtmann, G. Systematic Review and Meta-Analysis: Prevalence of Small Intestinal Bacterial Overgrowth in Chronic Liver Disease. Semin. Liver Dis. 2017, 37, 388–400. [Google Scholar] [CrossRef]
- Maslennikov, R.; Pavlov, C.; Ivashkin, V. Small intestinal bacterial overgrowth in cirrhosis: Systematic review and meta-analysis. Hepatol. Int. 2018, 12, 567–576. [Google Scholar] [CrossRef]
- Feng, X.; Li, X.; Jiang, Z. Prevalence and predictors of small intestinal bacterial overgrowth in systemic sclerosis: A systematic review and meta-analysis. Clin. Rheumatol. 2021, 40, 3039–3051. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Feng, X.; Jiang, Z.; Jiang, Z. Association of small intestinal bacterial overgrowth with Parkinson’s disease: A systematic review and meta-analysis. Gut Pathog. 2021, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Werlang, M.E.; Watthanasuntorn, K.; Panjawatanan, P.; Cheungpasitporn, W.; Gomez, V.; Lukens, F.J.; Ungprasert, P. Obesity and Risk of Small Intestine Bacterial Overgrowth: A Systematic Review and Meta-Analysis. Am. J. Dig. Dis. 2020, 65, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.C.; Nehra, A.; Mathur, A.; Rai, S. A meta-analysis on small intestinal bacterial overgrowth in patients with different subtypes of irritable bowel syndrome. J. Gastroenterol. Hepatol. 2020, 35, 922–931. [Google Scholar] [CrossRef]
- Chen, B.; Kim, J.J.; Zhang, Y.; Du, L.; Dai, N. Prevalence and predictors of small intestinal bacterial overgrowth in irritable bowel syndrome: A systematic review and meta-analysis. J. Gastroenterol. 2018, 53, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, A.; Shah, A.; Jones, M.P.; Koloski, N.; Talley, N.J.; Morrison, M.; Holtmann, G. Methane positive small intestinal bacterial overgrowth in inflammatory bowel disease and irritable bowel syndrome: A systematic review and meta-analysis. Gut Microbes 2021, 13, 1933313. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Lou, S.; Watthanasuntorn, K.; Kroner, P.T.; Cheungpasitporn, W.; Lukens, F.J.; Pungpapong, S.; Keaveny, A.P.; Ungprasert, P. Small intestinal bacterial overgrowth and nonalcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 601–608. [Google Scholar] [CrossRef]
- Zeng, Y.; Guo, M.; Fang, X.; Teng, F.; Tan, X.; Li, X.; Wang, M.; Long, Y.; Xu, Y. Gut Microbiota-Derived Trimethylamine N-Oxide and Kidney Function: A Systematic Review and Meta-Analysis. Adv. Nutr. Int. Rev. J. 2021, 12, 1286–1304. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Vajdi, M.; Asghari-Jafarabadi, M. Gut microbiota-associated metabolite trimethylamine N-Oxide and the risk of stroke: A systematic review and dose–response meta-analysis. Nutr. J. 2020, 19, 76. [Google Scholar] [CrossRef]
- Guasti, L.; Galliazzo, S.; Molaro, M.; Visconti, E.; Pennella, B.; Gaudio, G.V.; Lupi, A.; Grandi, A.M.; Squizzato, A. TMAO as a biomarker of cardiovascular events: A systematic review and meta-analysis. Intern. Emerg. Med. 2021, 16, 201–207. [Google Scholar] [CrossRef]
- Schiattarela, G.G.; Sannino, A.; Toscano, E.; Giugliano, G.; Gargiulo, G.; Franzone, A.; Avvedimento, M.; Trimarco, B.; Esposito, G.; Perrino, C. P1482Gut microbe-generated metabolite trimethylamine-N-oxide and cardiovascular risk: A systematic review and meta-analysis of mortality outcome. Eur. Heart J. 2017, 38, 304. [Google Scholar] [CrossRef]
- Farhangi, M.A. Gut microbiota-dependent trimethylamine N-oxide and all-cause mortality: Findings from an updated systematic review and meta-analysis. Nutrition 2020, 78, 110856. [Google Scholar] [CrossRef] [PubMed]
- Heianza, Y.; Ma, W.; Manson, J.E.; Rexrode, K.M.; Qi, L. Gut Microbiota Metabolites and Risk of Major Adverse Cardiovascular Disease Events and Death: A Systematic Review and Meta-Analysis of Prospective Studies. J. Am. Heart Assoc. 2017, 6, e4947. [Google Scholar] [CrossRef] [PubMed]
- Ge, X.; Zheng, L.; Zhuang, R.; Yu, P.; Xu, Z.; Liu, G.; Xi, X.; Zhou, X.; Fan, H. The Gut Microbial Metabolite Trimethylamine N-Oxide and Hypertension Risk: A Systematic Review and Dose–Response Meta-analysis. Adv. Nutr. Int. Rev. J. 2019, 11, 66–76. [Google Scholar] [CrossRef]
- Zhuang, R.; Ge, X.; Han, L.; Yu, P.; Gong, X.; Meng, Q.; Zhang, Y.; Fan, H.; Zheng, L.; Liu, Z.; et al. Gut microbe–generated metabolite trimethylamineN-oxide and the risk of diabetes: A systematic review and dose-response meta-analysis. Obes. Rev. 2019, 20, 883–894. [Google Scholar] [CrossRef]
- Li, W.; Huang, A.; Zhu, H.; Liu, X.; Huang, X.; Huang, Y.; Cai, X.; Lu, J.; Huang, Y. Gut microbiota-derived trimethylamineN-oxide is associated with poor prognosis in patients with heart failure. Med. J. Aust. 2020, 213, 374–379. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Vajdi, M. Novel findings of the association between gut microbiota–derived metabolite trimethylamine N-oxide and inflammation: Results from a systematic review and dose-response meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 60, 2801–2823. [Google Scholar] [CrossRef]
- Abbasalizad Farhangi, M.; Vajdi, M. Gut microbiota–associated trimethylamineN-oxide and increased cardiometabolic risk in adults: A systematic review and dose-response meta-analysis. Nutr. Rev. 2021, 79, 1022–1042. [Google Scholar] [CrossRef]
- Dehghan, P.; Farhangi, M.A.; Nikniaz, L.; Nikniaz, Z.; Asghari Jafarabadi, M. Gut microbiota-derived metabolite trimethylamine N-oxide (TMAO) potentially increases the risk of obesity in adults: An exploratory systematic review and dose-response meta- analysis. Obes. Rev. 2020, 21, e12993. [Google Scholar] [CrossRef]
- Dardiotis, E.; Sokratous, M.; Tsouris, Z.; Siokas, V.; Mentis, A.F.A.; Aloizou, A.M.; Michalopoulou, A.; Bogdanos, D.P.; Xiromerisiou, G.; Deretzi, G.; et al. Association betweenHelicobacter pylori infection and Guillain-Barré Syndrome: A meta-analysis. Eur. J. Clin. Investig. 2020, 50. [Google Scholar] [CrossRef]
- Luther, J.; Dave, M.; Higgins, P.D.R.; Kao, J.Y. Association between Helicobacter pylori infection and inflammatory bowel disease. Inflamm. Bowel Dis. 2010, 16, 1077–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Q.X.; Foo, N.X.; Loke, W.; Koh, Y.Q.; Seah, V.J.M.; Soh, A.Y.S.; Yeo, W.S. Is there an association betweenHelicobacter pylori infection and irritable bowel syndrome? A meta-analysis. World J. Gastroenterol. 2019, 25, 5702–5710. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Liu, Q.; He, Y.; Shi, W.; Xu, Q.; Yuan, Q.; Lin, Q.; Li, B.; Ye, L.; Min, Y.; et al. Association between Helicobacter pylori infection and nonalcoholic fatty liver. Medicine 2019, 98, e17781. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Shen, J.; Ran, Z.H. Association between Faecalibacterium prausnitzii Reduction and Inflammatory Bowel Disease: A Meta-Analysis and Systematic Review of the Literature. Gastroenterol. Res. Pract. 2014, 2014, 872725. [Google Scholar] [CrossRef]
- Wang, L.; Alammar, N.; Singh, R.; Nanavati, J.; Song, Y.; Chaudhary, R.; Mullin, G.E. Gut Microbial Dysbiosis in the Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Case-Control Studies. J. Acad. Nutr. Diet. 2020, 120, 565–586. [Google Scholar] [CrossRef]
- Liu, H.; Wu, H.; Bilegsaikhan, E.; Liu, T.; Lu, E.X.; Shen, X. Differential expression of intestinal microbiota in colorectal cancer compared with healthy controls: A systematic review and meta-analysis. Int. J. Clin. Exp. Med. 2016, 9, 10923–10930. [Google Scholar]
- Sun, Q.; Jia, Q.; Song, L.; Duan, L. Alterations in fecal short-chain fatty acids in patients with irritable bowel syndrome. Medicine 2019, 98, e14513. [Google Scholar] [CrossRef]
- Andreo-Martínez, P.; Rubio-Aparicio, M.; Sánchez-Meca, J.; Veas, A.; Martínez-González, A.E. A Meta-analysis of Gut Microbiota in Children with Autism. J. Autism Dev. Disord. 2022, 52, 1374–1387. [Google Scholar] [CrossRef]
- Shen, T.; Yue, Y.; He, T.; Huang, C.; Qu, B.; Lv, W.; Lai, H. The Association Between the Gut Microbiota and Parkinson’s Disease, a Meta-Analysis. Front. Aging Neurosci. 2021, 13, 636545. [Google Scholar] [CrossRef]
- Zhuang, X.; Li, T.; Li, M.; Huang, S.; Qiu, Y.; Feng, R.; Zhang, S.; Chen, M.; Xiong, L.; Zeng, Z. Systematic Review and Meta-analysis: Short-Chain Fatty Acid Characterization in Patients With Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 1751–1763. [Google Scholar] [CrossRef]
- Kim, K.N.; Yao, Y.; Ju, S.Y. Short Chain Fatty Acids and Fecal Microbiota Abundance in Humans with Obesity: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 2512. [Google Scholar] [CrossRef]
- Zhou, J.; Zhang, Y.; Cui, P.; Luo, L.; Chen, H.; Liang, B.; Jiang, J.; Ning, C.; Tian, L.; Zhong, X.; et al. Gut Microbiome Changes Associated With HIV Infection and Sexual Orientation. Front. Cell. Infect. Microbiol. 2020, 10, 434. [Google Scholar] [CrossRef]
- Nikolova, V.L.; Hall, M.R.B.; Hall, L.J.; Cleare, A.J.; Stone, J.M.; Young, A.H. Perturbations in Gut Microbiota Composition in Psychiatric Disorders. JAMA Psychiatry 2021, 78, 1343. [Google Scholar] [CrossRef] [PubMed]
- Sanada, K.; Nakajima, S.; Kurokawa, S.; Barceló-Soler, A.; Ikuse, D.; Hirata, A.; Yoshizawa, A.; Tomizawa, Y.; Salas-Valero, M.; Noda, Y.; et al. Gut microbiota and major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2020, 266, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, S.R.; Britton, G.J.; Contijoch, E.J.; Vennaro, O.H.; Mortha, A.; Colombel, J.; Grinspan, A.; Clemente, J.C.; Merad, M.; Faith, J.J. Interactions Between Diet and the Intestinal Microbiota Alter Intestinal Permeability and Colitis Severity in Mice. Gastroenterology 2018, 154, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Nova, E.; Wärnberg, J.; Gómez-Martínez, S.; Díaz, L.E.; Romeo, J.; Marcos, A. Immunomodulatory effects of probiotics in different stages of life. Br. J. Nutr. 2007, 98, S90–S95. [Google Scholar] [CrossRef] [PubMed]
- Gueimonde, M.; Noriega, L.; Margolles, A.; de Los Reyes-Gavilan, C.G.; Salminen, S. Ability of Bifidobacterium strains with acquired resistance to bile to adhere to human intestinal mucus. Int. J. Food Microbiol. 2005, 101, 341–346. [Google Scholar] [CrossRef]
- Lee, Y.; Yu, W.; Heo, T. Identification and screening for antimicrobial activity against Clostridium difficile of Bifidobacterium and Lactobacillus species isolated from healthy infant faeces. Int. J. Antimicrob. Agents 2003, 21, 340–346. [Google Scholar] [CrossRef]
- Bermudez-Brito, M.; Plaza-Díaz, J.; Muñoz-Quezada, S.; Gómez-Llorente, C.; Gil, A. Probiotic mechanisms of action. Ann. Nutr. Metab. 2012, 61, 160–174. [Google Scholar] [CrossRef]
- González-Rodríguez, I.; Sánchez, B.; Ruiz, L.; Turroni, F.; Ventura, M.; Ruas-Madiedo, P.; Gueimonde, M.; Margolles, A. Role of extracellular transaldolase from Bifidobacterium bifidum in mucin adhesion and aggregation. Appl. Environ. Microbiol. 2012, 78, 3992–3998. [Google Scholar] [CrossRef]
- Robbe-Masselot, C.; Herrmann, A.; Carlstedt, I.; Michalski, J.; Capon, C. Glycosylation of the two O-glycosylated domains of human MUC2 mucin in patients transposed with artificial urinary bladders constructed from proximal colonic tissue. Glycoconj. J. 2008, 25, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Liévin-Le Moal, V.; Amsellem, R.; Servin, A.L.; Coconnier, M. Lactobacillus acidophilus (strain LB) from the resident adult human gastrointestinal microflora exerts activity against brush border damage promoted by a diarrhoeagenic Escherichia coli in human enterocyte-like cells. Gut 2002, 50, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Kjos, M.; Nes, I.F.; Diep, D.B.; Lotfipour, F. Natural antimicrobial peptides from bacteria: Characteristics and potential applications to fight against antibiotic resistance. J. Appl. Microbiol. 2012, 113, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Rothhammer, V.; Quintana, F.J. The aryl hydrocarbon receptor: An environmental sensor integrating immune responses in health and disease. Nat. Reviews. Immunol. 2019, 19, 184–197. [Google Scholar] [CrossRef]
- Fukumoto, S.; Toshimitsu, T.; Matsuoka, S.; Maruyama, A.; Oh-Oka, K.; Takamura, T.; Nakamura, Y.; Ishimaru, K.; Fujii-Kuriyama, Y.; Ikegami, S.; et al. Identification of a probiotic bacteria-derived activator of the aryl hydrocarbon receptor that inhibits colitis. Immunol. Cell Biol. 2014, 92, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Swanson, K.S.; Gibson, G.R.; Hutkins, R.; Reimer, R.A.; Reid, G.; Verbeke, K.; Scott, K.P.; Holscher, H.D.; Azad, M.B.; Delzenne, N.M.; et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of synbiotics. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 687–701. [Google Scholar] [CrossRef]
- Kolida, S.; Gibson, G.R. Synbiotics in health and disease. Annu. Rev. Food Sci. Technol. 2011, 2, 373–393. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flowchart of the selection of studies for inclusion in the umbrella review on gastrointestinal microbiome and multiple health outcomes.
Figure 1.
Flowchart of the selection of studies for inclusion in the umbrella review on gastrointestinal microbiome and multiple health outcomes.

Figure 2.
Map of outcomes related to the gastrointestinal microbiome.

Figure 3.
Map of outcomes related to prebiotics/probiotics/synbiotics.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chang, C.; Yuan, X.; Zhang, X.; Chen, X.; Li, K. Gastrointestinal Microbiome and Multiple Health Outcomes: Umbrella Review. Nutrients 2022, 14, 3726. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14183726
AMA Style
Chang C, Yuan X, Zhang X, Chen X, Li K. Gastrointestinal Microbiome and Multiple Health Outcomes: Umbrella Review. Nutrients. 2022; 14(18):3726. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14183726
Chicago/Turabian StyleChang, Chengting, Xingzhu Yuan, Xingxia Zhang, Xinrong Chen, and Ka Li. 2022. "Gastrointestinal Microbiome and Multiple Health Outcomes: Umbrella Review" Nutrients 14, no. 18: 3726. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14183726
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.