Optimal Dietary and Plasma Magnesium Statuses Depend on Dietary Quality for a Reduction in the Risk of All-Cause Mortality in Older Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Information
2.3. Plasma Magnesium and Other Biomarkers
2.4. Outcome Ascertainment
2.5. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| Descriptor | Total | Mean ± SE | Mg intake (mg/day) | ||||
|---|---|---|---|---|---|---|---|
| Q1 (<155) | Q2 (155–<205) | Q3 (205–<265) | Q4 (≥265) | p ‡ | |||
| Total, n | 401 | 336 | 330 | 333 | |||
| Median | 126 | 178 | 230 | 325 | |||
| Plasma Mg (mmol/L), mean ± SE | 0.91 ± 0.01 | 0.90 ± 0.01 | 0.90 ± 0.01 | 0.92 ± 0.01 | 0.91 ± 0.01 | <0.05 | |
| Gender, % | 0.14 | ||||||
| Men | 52.5 | 226 ± 5.99 | 45.4 | 59.1 | 53.6 | 52.1 | |
| Women | 47.5 | 223 ± 7.44 | 54.7 | 40.9 | 46.4 | 47.9 | |
| Age at baseline, % | <0.05 | ||||||
| 65–69 | 30.0 | 228 ± 5.32 | 26.1 | 31.9 | 34.8 | 27.4 | |
| 70–74 | 30.5 | 227 ± 7.92 | 27.9 | 32.9 | 28.1 | 33.1 | |
| 75–97 | 39.5 | 220 ± 9.14 | 46.0 | 35.2 | 37.1 | 39.5 | |
| Education, % | <0.01 | ||||||
| Illiterate | 37.5 | 212 ± 7.55 | 48.7 | 33.1 | 35.9 | 32.0 | |
| Primary school | 39.7 | 218 ± 6.96 | 40.7 | 46.4 | 38.5 | 33.3 | |
| High school and above | 22.8 | 258 ± 9.00 | 10.5 | 20.5 | 25.6 | 34.8 | |
| Ethnicity, % | 0.24 | ||||||
| Non indigenous | 98.2 | 225 ± 6.03 | 97.2 | 98.4 | 98.2 | 99.0 | |
| Indigenous | 1.81 | 194 ± 14.6 | 2.78 | 1.63 | 1.79 | 1.01 | |
| Live alone, % | 0.75 | ||||||
| No | 88.9 | 232 ± 7.31 | 88.2 | 91.2 | 88.6 | 87.7 | |
| Yes | 11.1 | 229 ± 10.6 | 11.8 | 8.83 | 11.4 | 12.3 | |
| Personal income (NTD/month), % | <0.01 | ||||||
| <5000 | 62.2 | 219 ± 7.20 | 69.2 | 57.7 | 65.1 | 56.7 | |
| 5000–19,999 | 28.4 | 224 ± 6.57 | 26.7 | 35.5 | 22.9 | 28.4 | |
| ≥20,000 | 9.42 | 261 ± 14.2 | 4.06 | 6.83 | 12.1 | 14.9 | |
| Smoking more than 6 months, % | <0.01 | ||||||
| No | 63.1 | 230 ± 7.21 | 64.0 | 54.4 | 62.7 | 71.0 | |
| Former smoker | 14.7 | 233 ± 10.3 | 11.7 | 16.5 | 15.0 | 15.7 | |
| Current smoker | 22.2 | 204 ± 7.24 | 24.3 | 29.1 | 22.3 | 13.3 | |
| Alcohol drinker, % | 0.01 | ||||||
| Never drinker | 74.4 | 221 ± 6.39 | 82.0 | 70.8 | 70.3 | 74.6 | |
| Former drinker | 7.10 | 243 ± 17.6 | 5.18 | 7.59 | 6.92 | 8.73 | |
| Current drinker | 18.5 | 233 ± 8.16 | 12.8 | 21.6 | 22.8 | 16.7 | |
| Chewing ability, % | <0.01 | ||||||
| Satisfactory | 65.3 | 230 ± 5.80 | 58.8 | 68.8 | 61.2 | 72.5 | |
| Unsatisfactory | 34.7 | 216 ± 8.62 | 41.2 | 31.2 | 38.8 | 24.5 | |
| Appetite, % | <0.01 | ||||||
| Good | 34.9 | 241 ± 9.44 | 23.1 | 33.9 | 41.0 | 41.6 | |
| Fair | 58.3 | 216 ± 5.65 | 65.6 | 60.5 | 55.1 | 51.8 | |
| Poor | 6.80 | 213 ± 15.8 | 11.2 | 5.58 | 3.90 | 6.56 | |
| Body mass index (kg/m2), % | 0.08 | ||||||
| <18.5 | 7.00 | 225 ± 14.4 | 8.67 | 6.56 | 4.24 | 8.52 | |
| 18.5–23.9 | 49.6 | 222 ± 9.12 | 50.5 | 51.3 | 50.9 | 46.0 | |
| 24.0–26.9 | 27.9 | 234 ± 9.99 | 27.0 | 29.4 | 25.3 | 29.7 | |
| ≥27.0 | 15.5 | 235 ± 10.5 | 13.8 | 12.8 | 19.6 | 15.8 | |
| MET (/day), % | <0.01 | ||||||
| <1.5 | 56.4 | 213 ± 7.35 | 70.6 | 56.2 | 48.7 | 50.0 | |
| 1.5–2.9 | 10.8 | 226 ± 12.3 | 10.3 | 10.1 | 12.1 | 10.7 | |
| ≥3 | 32.8 | 244 ± 5.96 | 19.2 | 33.7 | 39.2 | 39.3 | |
| History of hypertension, % | 0.57 | ||||||
| No | 70.7 | 222 ± 6.13 | 69.7 | 73.7 | 69.3 | 70.0 | |
| Yes | 29.3 | 229 ± 10.3 | 30.3 | 26.3 | 30.7 | 30.0 | |
| Hyperglycemic, % | 0.55 | ||||||
| No (<126 mg/dL) | 91.3 | 229 ± 6.19 | 88.5 | 92.7 | 92.2 | 91.8 | |
| Yes (≥126 mg/dL) | 8.70 | 224 ± 16.2 | 11.5 | 7.32 | 7.78 | 8.25 | |
| Incident diabetes, % | 0.56 | ||||||
| No | 83.2 | 226 ± 6.11 | 80.9 | 83.7 | 81.2 | 86.9 | |
| Yes | 16.8 | 218 ± 11.1 | 19.1 | 16.3 | 18.8 | 13.1 | |
| Plasma glucose (mg/dL), mean ± SE | 106 ± 1.25 | 111 ± 4.23 | 103 ± 1.34 | 104 ± 0.91 | 108 ± 2.37 | 0.24 | |
| Serum C-reactive protein, mean ± SE | 0.45 ± 0.04 | 0.42 ± 0.05 | 0.43 ± 0.05 | 0.44 ± 0.04 | 0.51 ± 0.14 | 0.93 | |
| Serum creatinine (mg/dL), mean ± SE | 1.01 ± 0.02 | 1.03 ± 0.06 | 0.96 ± 0.02 | 1.03 ± 0.03 | 1.00 ± 0.03 | 0.03 | |
| Serum creatinine >1.5 mg/dL, % | 5.85 | 9.12 | 3.26 | 7.01 | 4.17 | 0.09 | |
| Dietary diversity score, mean ± SE | 4.53 ± 0.06 | 3.89 ± 0.08 abc | 4.50 ± 0.08 ad | 4.74 ± 0.07 b | 5.00 ± 0.09 cd | <0.01 | |
| ≤4, % | 46.3 | 194 ± 5.44 | 74.5 | 46.7 | 36.8 | 27.0 | |
| >4, % | 53.7 | 252 ± 7.97 | 25.6 | 53.3 | 63.3 | 73.0 | |
| Dietary intake from SFFQ (serving/day), mean ± SE | |||||||
| Total grain | 11.3 ± 0.22 | 11.1 ± 0.35 | 11.8 ± 0.45 | 11.0 ± 0.30 | 11.3 ± 0.27 | 0.45 | |
| Whole grain | 0.30±0.07 | 0.06 ± 0.03 a | 0.19 ± 0.06 b | 0.20 ± 0.09 c | 0.73 ± 0.17 abc | <0.01 | |
| Dairy product | 0.84 ± 0.05 | 0.58 ± 0.07 ab | 0.76 ± 0.07c | 0.98 ± 0.08 a | 1.04 ± 0.07 bc | <0.01 | |
| Vegetable | 2.55 ± 0.11 | 2.36 ± 0.16 | 2.51 ± 0.17 | 2.57 ± 0.10 | 2.74 ± 0.13 | 0.07 | |
| Fruit | 1.30 ± 0.04 | 1.00 ± 0.08 abc | 1.28 ± 0.07 ad | 1.36 ± 0.07 b | 1.56 ± 0.07 cd | <0.01 | |
| Egg | 0.23 ± 0.01 | 0.17 ± 0.02 a | 0.23 ± 0.03 | 0.23 ± 0.01 | 0.29 ± 0.02 a | <0.01 | |
| Dietary information from 24 h recall, mean ± SE | |||||||
| Total energy intake (kcal/day) | 1633 ± 42.1 | 1490 ± 55.6 a | 1616 ± 57.1 | 1664 ± 59.1 | 1763 ± 59.0 a | <0.01 | |
| Nutrient intakes per 1000 kcal | |||||||
| Fat (g) | 28.7 ± 0.53 | 32.9 ± 1.26 abc | 27.7 ± 1.11 a | 27.6 ± 0.91 b | 26.5 ± 0.74 c | <0.01 | |
| Saturated fatty acid (mg) | 8665 ± 213 | 10,175 ± 448a | 8472 ± 383 | 8494 ± 429 | 7491 ± 297a | <0.01 | |
| Cholesterol (mg) | 129 ± 4.76 | 112 ± 6.59 ab | 133 ± 9.43 | 137 ± 6.70 a | 136 ± 7.70 b | 0.02 | |
| Dietary fiber (g) | 12.5 ± 0.45 | 8.55 ± 0.32 abc | 10.8 ± 0.44 ade | 13.2 ± 0.66 bdf | 17.4 ± 0.91 cef | <0.01 | |
| Potassium (mg) | 1483 ± 34.9 | 932 ± 29.2 abc | 1243 ± 36.0 ade | 1634 ± 60.0 bdf | 2132 ± 52.7 cef | <0.01 | |
| Calcium (mg) | 411 ± 14.9 | 208 ± 12.1 abc | 328 ± 14.9 ade | 456 ± 19.0 bdf | 655 ± 24.9 cef | <0.01 | |
| Mg Intake (mg/day) Hazard Ratio (95% Confidence Intervals) | |||||
|---|---|---|---|---|---|
| Q1 (<155) | Q2 (155–< 205) | Q3 (205–< 265) | Q4 (≥265) | p for trend | |
| Diabetes incidence | |||||
| Person-years | 2096.5 | 1948.3 | 1885.1 | 1964.0 | |
| No of events | 71 | 53 | 64 | 43 | |
| Cumulative incidence rate/1000 person-years | 33.9 | 27.2 | 34.0 | 21.9 | |
| Crude model | 1.00 | 0.75 (0.42–1.32) | 0.88 (0.60–1.30) | 0.61 (0.31–1.19) | 0.14 |
| Model 1 | 1.00 | 0.77 (0.42–1.40) | 0.85 (0.57–1.27) | 0.57 (0.27–1.20) | 0.11 |
| Model 2 | 1.00 | 0.74 (0.42–1.32) | 0.82 (0.56–1.19) | 0.54 (0.26–1.13) | 0.08 |
| Model 3 | 1.00 | 0.77 (0.43–1.38) | 0.86 (0.57–1.31) | 0.59 (0.26–1.33) | 0.20 |
| All-cause mortality | |||||
| Person-years | 2795.7 | 2556.7 | 2568.8 | 2565.2 | |
| No of events/survivals | 173 | 112 | 93 | 97 | |
| Cumulative death rate/1000 person-years | 61.9 | 43.8 | 36.2 | 37.8 | |
| Crude model | 1.00 | 0.65 (0.48–0.87) | 0.57 (0.42–0.78) | 0.64 (0.45–0.90) | 0.01 |
| Model 1 | 1.00 | 0.71 (0.52–0.97) | 0.68 (0.50–0.93) | 0.85 (0.60–1.19) | 0.22 |
| Model 2 | 1.00 | 0.75 (0.55–1.03) | 0.75 (0.56–1.00) | 0.89 (0.62–1.27) | 0.42 |
| Model 3 | 1.00 | 0.79 (0.58–1.08) | 0.81 (0.60–1.09) | 1.05 (0.74–1.49) | 0.94 |
| Cardiovascular mortality | |||||
| Person-years | 2223.0 | 2173.7 | 2223.5 | 2227.2 | |
| No of events/survivals | 40 | 33 | 27 | 24 | |
| Cumulative death rate/1000 person-years | 18.0 | 15.2 | 12.1 | 10.8 | |
| Crude model | 1.00 | 1.04 (0.52–2.09) | 0.77 (0.42–1.43) | 0.77 (0.42–1.40) | 0.26 |
| Model 1 | 1.00 | 1.10 (0.64–1.90) | 1.02 (0.52–2.00) | 1.08 (0.54–2.17) | 0.89 |
| Model 2 | 1.00 | 1.23 (0.71–2.13) | 1.16 (0.63–2.14) | 1.14 (0.55–2.36) | 0.75 |
| Model 3 | 1.00 | 1.25 (0.71–2.18) | 1.21 (0.60–2.45) | 1.24 (0.59–2.60) | 0.61 |

| Descriptor | Total | Plasma Mg (mmol/L) | p ‡ | |||
|---|---|---|---|---|---|---|
| Mean ± SE | Low (<0.75) | Normal (0.75–0.95) | High (>0.95) | |||
| Total, n | 44 | 752 | 190 | |||
| Median | 0.74 | 0.90 | 0.99 | |||
| Mg intake (mg/day), mean ± SE | 227 ± 7.22 | 217 ± 18.4 | 223 ± 7.84 | 241 ± 11.0 | 0.28 | |
| Gender, % | 0.24 | |||||
| Men | 53.5 | 0.91 ± 0.01 | 64.3 | 52.2 | 57.1 | |
| Women | 46.5 | 0.91 ± 0.01 | 35.7 | 47.8 | 42.9 | |
| Age at baseline, % | 0.56 | |||||
| 65–69 | 32.4 | 0.90 ± 0.00 | 27.7 | 33.2 | 30.1 | |
| 70–74 | 30.9 | 0.90 ± 0.01 | 28.4 | 31.6 | 28.8 | |
| 75–97 | 36.7 | 0.91 ± 0.01 | 43.9 | 35.3 | 41.1 | |
| Education, % | 0.03 | |||||
| Illiterate | 35.8 | 0.91 ± 0.01 | 40.6 | 34.7 | 39.0 | |
| Primary school | 41.9 | 0.90 ± 0.01 | 50.5 | 43.8 | 34.0 | |
| High school and above | 22.3 | 0.92 ± 0.01 | 8.91 | 21.5 | 27.0 | |
| Ethnicity, % | <0.01 | |||||
| Non indigenous | 97.8 | 0.91 ± 0.01 | 84.8 | 97.8 | 99.1 | |
| Indigenous | 2.25 | 0.84 ± 0.02 | 15.2 | 2.21 | 0.95 | |
| Live alone, % | 0.66 | |||||
| No | 88.9 | 0.91 ± 0.01 | 85.9 | 88.4 | 91.1 | |
| Yes | 11.1 | 0.90 ± 0.02 | 14.1 | 11.6 | 8.86 | |
| Personal income (NTD/month), % | 0.06 | |||||
| <5000 | 62.8 | 0.91 ± 0.01 | 69.5 | 63.1 | 61.2 | |
| 5000–19,999 | 26.1 | 0.90 ± 0.01 | 30.5 | 26.5 | 24.3 | |
| ≥20,000 | 11.1 | 0.93 ± 0.01 | -- | 10.4 | 14.4 | |
| Smoking more than 6 months, % | 0.55 | |||||
| No | 62.2 | 0.91 ± 0.0 | 59.7 | 63.7 | 57.1 | |
| Former smoker | 14.8 | 0.91 ± 0.01 | 8.71 | 14.3 | 17.6 | |
| Current smoker | 23.0 | 0.90 ± 0.01 | 31.6 | 22.1 | 25.3 | |
| Alcohol drinker, % | 0.12 | |||||
| Never drinker | 73.7 | 0.90 ± 0.01 | 77.8 | 74.7 | 69.6 | |
| Former drinker | 7.54 | 0.92 ± 0.01 | 1.39 | 7.15 | 9.67 | |
| Current drinker | 18.8 | 0.91 ± 0.01 | 20.8 | 18.2 | 20.8 | |
| Chewing ability, % | 0.72 | |||||
| Satisfactory | 66.2 | 0.91±0.01 | 58.1 | 66.1 | 67.2 | |
| Unsatisfactory | 33.9 | 0.90±0.01 | 41.9 | 33.9 | 32.8 | |
| Appetite, % | 0.90 | |||||
| Good | 35.9 | 0.90 ± 0.01 | 35.6 | 36.8 | 33.0 | |
| Fair | 58.3 | 0.91 ± 0.01 | 57.5 | 57.6 | 61.0 | |
| Poor | 5.78 | 0.91 ± 0.01 | 6.87 | 5.69 | 5.99 | |
| Body mass index (kg/m2), % | 0.97 | |||||
| <18.5 | 6.26 | 0.90 ± 0.01 | 9.76 | 6.32 | 5.62 | |
| 18.5–23.9 | 49.5 | 0.90 ± 0.01 | 50.4 | 49.8 | 48.1 | |
| 24.0–26.9 | 28.0 | 0.91 ± 0.01 | 29.1 | 28.0 | 28.3 | |
| ≥27.0 | 16.2 | 0.91 ± 0.01 | 10.7 | 15.9 | 18.0 | |
| MET (/day), % | 0.84 | |||||
| <1.5 | 56.0 | 0.90 ± 0.01 | 57.1 | 56.7 | 53.1 | |
| 1.5–2.9 | 10.3 | 0.90 ± 0.01 | 14.5 | 10.1 | 10.4 | |
| ≥3 | 33.8 | 0.91 ± 0.01 | 28.4 | 33.2 | 36.5 | |
| History of hypertension, % | 0.13 | |||||
| No | 72.3 | 0.90 ± 0.01 | 69.4 | 73.9 | 66.6 | |
| Yes | 27.7 | 0.92 ± 0.01 | 30.6 | 26.1 | 33.5 | |
| Hyperglycemic, % | 0.19 | |||||
| No (<126 mg/dL) | 91.9 | 0.88 ± 0.01 | 81.7 | 91.5 | 94.3 | |
| Yes (≥126 mg/dL) | 8.14 | 0.91 ± 0.01 | 18.3 | 8.49 | 5.71 | |
| Incident diabetes, % | 0.75 | |||||
| No | 84.2 | 0.91 ± 0.01 | 78.6 | 84.0 | 85.6 | |
| Yes | 15.8 | 0.90 ± 0.01 | 21.4 | 16.0 | 14.4 | |
| Plasma glucose (mg/dL), mean ± SE | 106 ± 1.00 | 118 ± 13.6 | 106 ± 1.04 | 104 ± 2.16 | 0.53 | |
| Serum C-reactive protein, mean ± SE | 0.42 ± 0.03 | 0.73 ± 0.26 | 0.42 ± 0.04 | 0.38 ± 0.04 | 0.42 | |
| Serum creatinine (mg/dL), mean ± SE | 1.00 ± 0.02 | 1.01± 0.05 | 0.97 ± 0.02 a | 1.10 ± 0.04 a | 0.02 | |
| Serum creatinine > 1.5 mg/dL, % | 5.75 | 0.94 | 4.35 | 11.5 | 0.01 | |
| Dietary diversity score, mean ± SE | 4.60 ± 0.06 | 3.88 ± 0.19 ab | 4.57 ± 0.06 ac | 4.82 ± 0.09 bc | <0.01 | |
| ≤4, % | 44.0 | 0.89 ± 0.01 | 77.5 | 46.9 | 29.9 | <0.01 |
| > 4, % | 56.0 | 0.92 ± 0.01 | 22.5 | 53.1 | 70.1 | |
| Dietary intake from SFFQ (serving/day), mean ± SE | ||||||
| Total grain | 11.6 ± 0.19 | 11.1 ± 0.96 | 11.7 ± 0.20 | 11.3 ± 0.34 | 0.38 | |
| Whole grain | 0.35 ± 0.09 | 0.10 ± 0.10 | 0.31 ± 0.09 | 0.55 ± 0.18 | 0.15 | |
| Dairy product | 0.84 ± 0.06 | 0.52 ± 0.18 | 0.83 ± 0.08 | 0.90 ± 0.07 | 0.17 | |
| Vegetable | 2.64 ± 0.12 | 2.08 ± 0.22 a | 2.61 ± 0.12 | 2.80 ± 0.16 a | <0.05 | |
| Fruit | 1.33 ± 0.06 | 0.95 ± 0.20 | 1.34 ± 0.07 | 1.34 ± 0.08 | 0.16 | |
| Egg | 0.23 ± 0.02 | 0.12 ± 0.03 ab | 0.23 ± 0.02 a | 0.26 ± 0.02 b | <0.01 | |
| Dietary information from 24 h recall, mean ± SE | ||||||
| Total energy intake (kcal/day) | 1659 ± 50.3 | 1705 ± 132 | 1637 ± 47.9 | 1733 ± 90.3 | 0.38 | |
| Nutrient intakes per 1000 kcal | ||||||
| Fat (g) | 28.7 ± 0.66 | 25.7 ± 2.35 | 29.4 ± 0.79 a | 26.5 ± 0.66 a | <0.01 | |
| Saturated fatty acid (mg) | 8666 ± 243 | 7202 ± 962 | 8850 ± 276 | 8148 ± 373 | 0.04 | |
| Cholesterol (mg) | 130 ± 5.66 | 139 ± 17.9 | 130 ± 5.95 | 125 ± 11.0 | 0.82 | |
| Dietary fiber (g) | 12.7 ± 0.57 | 11.0 ± 1.43 | 12.4 ± 0.70 | 13.8 ± 0.71 | 0.24 | |
| Potassium (mg) | 1498 ± 46.4 | 1297 ± 151 | 1462 ± 42.0 | 1656 ± 89.4 | 0.04 | |
| Calcium (mg) | 411 ± 18.1 | 277 ± 39.7 ab | 402 ± 15.2 a | 462 ± 48.6 b | 0.01 | |
| Plasma Mg (mmol/L) Hazard Ratio (95% Confidence Intervals) | ||||
|---|---|---|---|---|
| Low (<0.75) | Normal (0.75–0.95) | High (>0.95) | p for trend | |
| Incident diabetes | ||||
| Person-years | 198.8 | 4412.4 | 1092.5 | |
| No of events | 8 | 117 | 31 | |
| Cumulative incidence rate/1000 person-years | 40.2 | 26.5 | 28.4 | |
| Crude model | 1.63 (0.56–4.74) | 1.00 | 0.91 (0.58–1.40) | 0.45 |
| Model 1 | 2.00 (0.66–6.08) | 1.00 | 0.95 (0.61–1.47) | 0.44 |
| Model 2 | 2.01 (0.67–6.05) | 1.00 | 0.96 (0.61–1.51) | 0.44 |
| Model 3 | 2.05 (0.68–6.15) | 1.00 | 0.91 (0.58–1.42) | 0.39 |
| All-cause mortality | ||||
| Person-years | 275.2 | 5779.6 | 1468.6 | |
| No of events | 23 | 230 | 54 | |
| Cumulative incidence rate/1000 person-years | 83.6 | 39.8 | 36.8 | |
| Crude model | 1.53 (0.89–2.64) | 1.00 | 0.96 (0.70–1.32) | 0.49 |
| Model 1 | 1.25 (0.83–1.86) | 1.00 | 0.86 (0.61–1.20) | 0.23 |
| Model 2 | 1.24 (0.83–1.86) | 1.00 | 0.86 (0.61–1.21) | 0.24 |
| Model 3 | 1.24 (0.85–1.81) | 1.00 | 0.70 (0.50–0.98) | 0.02 |
| Cardiovascular mortality | ||||
| Person-years | 219.1 | 4958.0 | 1269.6 | |
| No of events | 8 | 63 | 13 | |
| Cumulative incidence rate/1000 person-years | 36.5 | 12.7 | 10.2 | |
| Crude model | 2.76 (0.98–7.79) | 1.00 | 0.84 (0.40–1.75) | 0.37 |
| Model 1 | 2.24 (0.88–5.73) | 1.00 | 0.76 (0.36–1.60) | 0.25 |
| Model 2 | 2.24 (0.88–5.74) | 1.00 | 0.75 (0.36–1.59) | 0.25 |
| Model 3 | 2.28 (0.90–5.75) | 1.00 | 0.51 (0.20–1.26) | <0.05 |

4. Discussion
4.1. Main Findings
4.2. Mg and Diabetes Incidence
4.3. Mg and Mortality
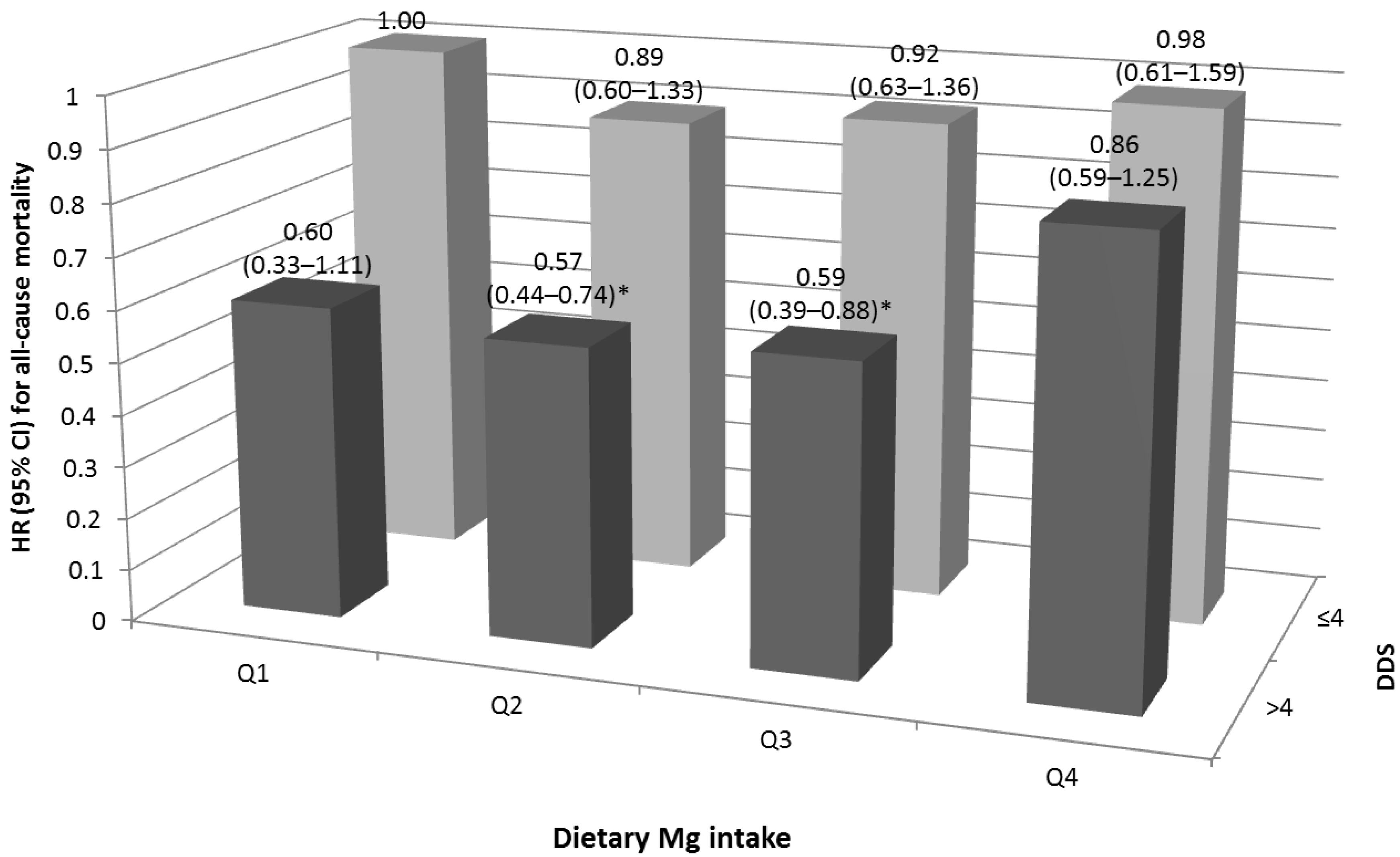
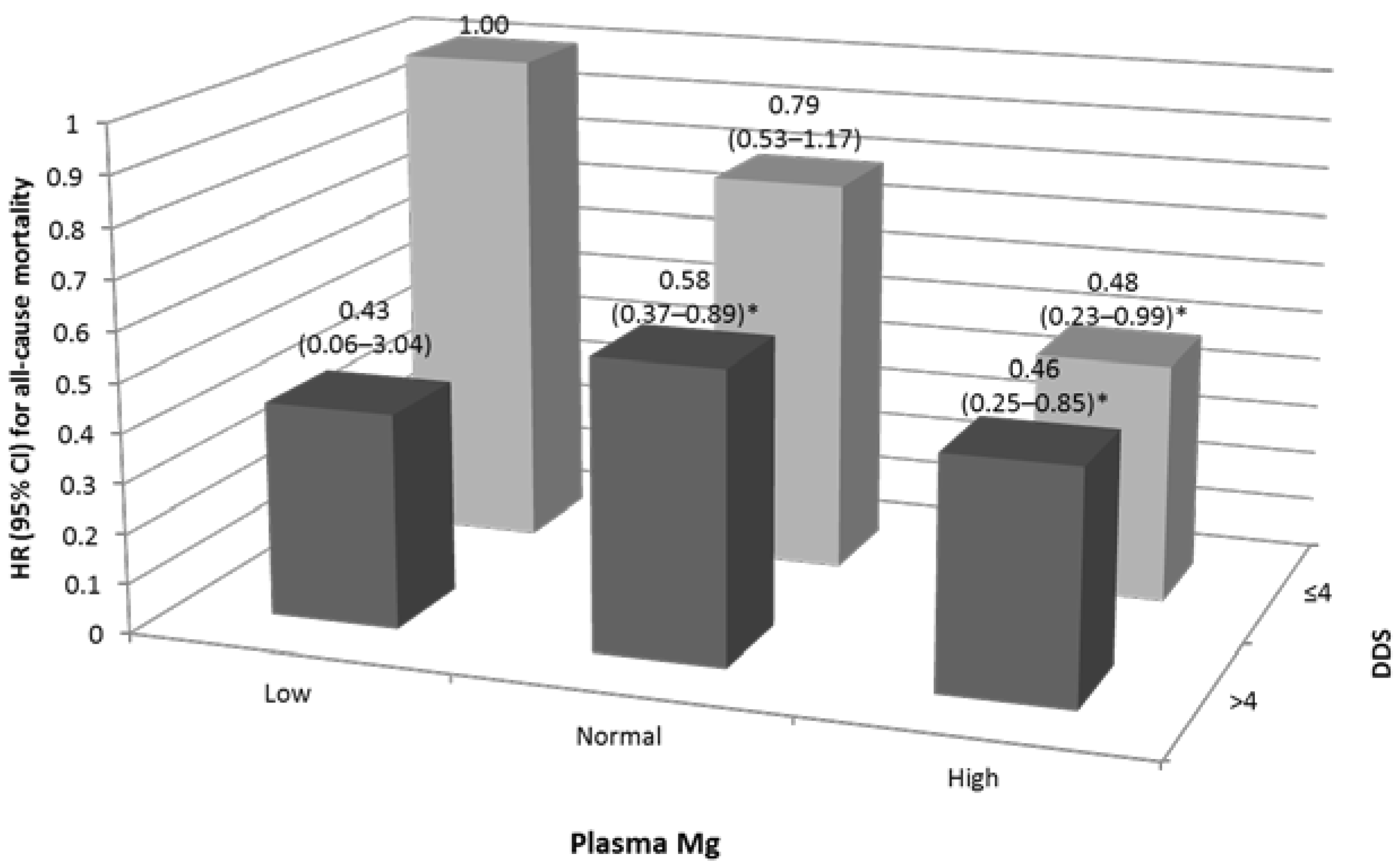
4.4. Joint Effect
4.5. Sensitivity Analyses
4.6. Strengths and Limitations
4.7. Clinical Implications
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix
| Order | ICD-9 Code | Cause-Specific Mortality | N | % |
|---|---|---|---|---|
| 1 | 140–239 | Neoplasms | 136 | 30.33 |
| 2 | 390–459 | Diseases of the circulatory system | 124 | 23.6 |
| 3 | 460–519 | Acute respiratory infections | 66 | 14.3 |
| 4 | 780–799 | Symptoms, signs, and ill-defined conditions | 32 | 8.33 |
| 5 | 580–629 | Diseases of the genitourinary system | 19 | 5.36 |
References
- Topf, J.M.; Murray, P.T. Hypomagnesemia and hypermagnesemia. Rev. Endocr. Metab. Disord. 2003, 4, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Vaquero, M.P. Magnesium and trace elements in the elderly: Intake, status and recommendations. J. Nutr. Health Aging 2002, 6, 147–153. [Google Scholar] [PubMed]
- Song, Y.; Ridker, P.M.; Manson, J.E.; Cook, N.R.; Buring, J.E.; Liu, S. Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older U.S. Women. Diabetes Care 2005, 28, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Sun, Q.; Curhan, G.C.; Taylor, E.N.; Spiegelman, D.; Willett, W.C.; Manson, J.E.; Rexrode, K.M.; Albert, C.M. Dietary and plasma magnesium and risk of coronary heart disease among women. J. Am. Heart Assoc. 2013, 2, e000114. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Ridaura, R.; Willett, W.C.; Rimm, E.B.; Liu, S.; Stampfer, M.J.; Manson, J.E.; Hu, F.B. Magnesium intake and risk of type 2 diabetes in men and women. Diabetes Care 2004, 27, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Sluijs, I.; Czernichow, S.; Beulens, J.W.; Boer, J.M.; van der Schouw, Y.T.; Verschuren, W.M.; Grobbee, D.E. Intakes of potassium, magnesium, and calcium and risk of stroke. Stroke 2014, 45, 1148–1150. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Belvedere, M.; Dominguez, L.J. Magnesium homeostasis and aging. Magnes. Res. 2009, 22, 235–246. [Google Scholar] [PubMed]
- Lee, M.S.; Chen, R.C.Y.; Chang, Y.H.; Huang, Y.C.; Wahlqvist, M.L. Physical function mitigates the adverse effects of being thin on mortality in a freeliving older Taiwanese cohort. J. Nutr. Health Aging 2012, 16, 766–783. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.J.; Chang, Y.H.; Wei, I.L.; Kao, M.D.; Lin, Y.C.; Pan, W.H. Intake levels and major food sources of energy and nutrients in the Taiwanese elderly. Asia Pac. J. Clin. Nutr. 2005, 14, 211–220. [Google Scholar] [PubMed]
- Wood, R.J.; Suter, P.M.; Russell, R.M. Mineral requirements of elderly people. Am. J. Clin. Nutr. 1995, 62, 493–505. [Google Scholar] [PubMed]
- Lee, M.S.; Huang, Y.C.; Wahlqvist, M.L. Chewing ability in conjunction with food intake and energy status in later life affects survival in Taiwanese with the metabolic syndrome. J. Am. Geriatr. Soc. 2010, 58, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Huang, Y.C.; Su, H.H.; Lee, M.Z.; Wahlqvist, M.L. A simple food quality index predicts mortality in elderly Taiwanese. J. Nutr. Health Aging 2011, 15, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.C.; Malik, V.; Jia, W.; Kadowaki, T.; Yajnik, C.S.; Yoon, K.H.; Hu, F.B. Diabetes in asia: Epidemiology, risk factors, and pathophysiology. JAMA 2009, 301, 2129–2140. [Google Scholar] [CrossRef] [PubMed]
- Horner, S.M. Efficacy of intravenous magnesium in acute myocardial infarction in reducing arrhythmias and mortality. Meta-analysis of magnesium in acute myocardial infarction. Circulation 1992, 86, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.H.; Hung, Y.T.; Shaw, N.S.; Lin, W.; Lee, S.D.; Chiu, C.F.; Lin, M.C.; Chen, S.Y.; Hong, C.M.; Huang, T.Y.; et al. Elderly nutrition and health survey in Taiwan (1999–2000): Research design, methodology and content. Asia Pac. J. Clin. Nutr. 2005, 14, 203–210. [Google Scholar] [PubMed]
- Department of Health. Nutrient Composition Data Bank for Foods in Taiwan Area; DOH: Taipei, Taiwan, 1998. [Google Scholar]
- Pan, W.H.; Chang, Y.H.; Chen, J.Y.; Wu, S.J.; Tzeng, M.S.; Kao, M.D. Nutrition and health survey in Taiwan (NAHSIT) 1993~1996: Dietary nutrient intakes assessed by 24h recall. Nutr. Sci. J. 1999, 24, 11–39. [Google Scholar]
- Huang, Y.H.; Lee, M.S.; Pan, W.H.; Wahlqvist, M.L. Validation of a simplified food frequency questionnaire as used in the nutrition and health survey in Taiwan (NAHSIT) for the elderly. Asia Pac. J. Clin. Nutr. 2011, 20, 134–140. [Google Scholar] [PubMed]
- Verhave, J.C.; Fesler, P.; Ribstein, J.; du Cailar, G.; Mimran, A. Estimation of renal function in subjects with normal serum creatinine levels: Influence of age and body mass index. Am. J. Kidney Dis. 2005, 46, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H. Dietary magnesium intake in a national sample of us adults. J. Nutr. 2003, 133, 2879–2882. [Google Scholar] [PubMed]
- Pham, P.C.; Pham, P.M.; Pham, S.V.; Miller, J.M.; Pham, P.T. Hypomagnesemia in patients with type 2 diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Longstreet, D.A.; Heath, D.L.; Panaretto, K.S.; Vink, R. Correlations suggest low magnesium may lead to higher rates of type 2 diabetes in indigenous australians. Rural Remote Health 2007, 7, 843. [Google Scholar] [PubMed]
- Weng, L.C.; Lee, N.J.; Yeh, W.T.; Ho, L.T.; Pan, W.H. Lower intake of magnesium and dietary fiber increases the incidence of type 2 diabetes in Taiwanese. J. Formos. Med. Assoc. 2012, 111, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Shau, W.Y.; Jiang, Y.D.; Li, H.Y.; Chang, T.J.; Sheu, W.H.; Kwok, C.F.; Ho, L.T.; Chuang, L.M. Type 2 diabetes prevalence and incidence among adults in Taiwan during 1999–2004: A national health insurance data set study. Diabet. Med. 2010, 27, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Kamineni, A.; Carnethon, M.; Djousse, L.; Mukamal, K.J.; Siscovick, D. Lifestyle risk factors and new-onset diabetes mellitus in older adults: The cardiovascular health study. Arch. Intern. Med. 2009, 169, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Diabetes in older adults. Diabetes Care 2012, 35, 2650–2664. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferre, M.; Bullo, M.; Estruch, R.; Corella, D.; Martinez-Gonzalez, M.A.; Ros, E.; Covas, M.; Aros, F.; Gomez-Gracia, E.; Fiol, M.; et al. Dietary magnesium intake is inversely associated with mortality in adults at high cardiovascular disease risk. J. Nutr. 2014, 144, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Reffelmann, T.; Ittermann, T.; Dorr, M.; Volzke, H.; Reinthaler, M.; Petersmann, A.; Felix, S.B. Low serum magnesium concentrations predict cardiovascular and all-cause mortality. Atherosclerosis 2011, 219, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine. Magnesium. In Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; National Academy Press: Washington, DC, USA, 1997; pp. 190–249. [Google Scholar]
- Schwartz, R.; Spencer, H.; Welsh, J.J. Magnesium absorption in human subjects from leafy vegetables, intrinsically labeled with sTable 26Mg. Am. J. Clin. Nutr. 1984, 39, 571–576. [Google Scholar] [PubMed]
- Jacques, P.F.; Sulsky, S.I.; Sadowski, J.A.; Phillips, J.C.; Rush, D.; Willett, W.C. Comparison of micronutrient intake measured by a dietary questionnaire and biochemical indicators of micronutrient status. Am. J. Clin. Nutr. 1993, 57, 182–189. [Google Scholar] [PubMed]
- Rock, E.; Astier, C.; Lab, C.; Vignon, X.; Gueux, E.; Motta, C.; Rayssiguier, Y. Dietary magnesium deficiency in rats enhances free radical production in skeletal muscle. J. Nutr. 1995, 125, 1205–1210. [Google Scholar] [PubMed]
- King, D.E.; Mainous, A.G., 3rd; Geesey, M.E.; Woolson, R.F. Dietary magnesium and C-reactive protein levels. J. Am. Coll. Nutr. 2005, 24, 166–171. [Google Scholar] [CrossRef] [PubMed]
- He, M.; van Dam, R.M.; Rimm, E.; Hu, F.B.; Qi, L. Whole-grain, cereal fiber, bran, and germ intake and the risks of all-cause and cardiovascular disease-specific mortality among women with type 2 diabetes mellitus. Circulation 2010, 121, 2162–2168. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.H.; Yeh, W.T.; Svetkey, L.P.; Chuang, S.Y.; Chang, Y.C.; Wang, C.; Pan, W.H. Dietary intakes consistent with the DASH dietary pattern reduce blood pressure increase with age and risk for stroke in a chinese population. Asia Pac. J. Clin. Nutr. 2013, 22, 482–491. [Google Scholar] [PubMed]
- Huang, C.L.; Kuo, E. Mechanism of hypokalemia in magnesium deficiency. J. Am. Soc. Nephrol. 2007, 18, 2649–2652. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.Y.; Hu, Y.W.; Yue, C.S.; Wen, Y.W.; Yeh, W.T.; Hsu, L.S.; Tsai, S.Y.; Pan, W.H. Effect of potassium-enriched salt on cardiovascular mortality and medical expenses of elderly men. Am. J. Clin. Nutr. 2006, 83, 1289–1296. [Google Scholar] [PubMed]
- Bartali, B.; Salvini, S.; Turrini, A.; Lauretani, F.; Russo, C.R.; Corsi, A.M.; Bandinelli, S.; D’Amicis, A.; Palli, D.; Guralnik, J.M.; et al. Age and disability affect dietary intake. J. Nutr. 2003, 133, 2868–2873. [Google Scholar] [PubMed]
- Subar, A.F.; Harlan, L.C.; Mattson, M.E. Food and nutrient intake differences between smokers and non-smokers in the us. Am. J. Public Health 1990, 80, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Wahlqvist, M.L. Ecosystem health disorders—Changing perspectives in clinical medicine and nutrition. Asia Pac. J. Clin. Nutr. 2014, 23, 1–15. [Google Scholar] [PubMed]
- Danziger, J.; William, J.H.; Scott, D.J.; Lee, J.; Lehman, L.W.; Mark, R.G.; Howell, M.D.; Celi, L.A.; Mukamal, K.J. Proton-pump inhibitor use is associated with low serum magnesium concentrations. Kidney Int. 2013, 83, 692–699. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-C.; Wahlqvist, M.L.; Kao, M.-D.; Wang, J.-L.; Lee, M.-S. Optimal Dietary and Plasma Magnesium Statuses Depend on Dietary Quality for a Reduction in the Risk of All-Cause Mortality in Older Adults. Nutrients 2015, 7, 5664-5683. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7075244
Huang Y-C, Wahlqvist ML, Kao M-D, Wang J-L, Lee M-S. Optimal Dietary and Plasma Magnesium Statuses Depend on Dietary Quality for a Reduction in the Risk of All-Cause Mortality in Older Adults. Nutrients. 2015; 7(7):5664-5683. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7075244
Chicago/Turabian StyleHuang, Yi-Chen, Mark L. Wahlqvist, Mei-Ding Kao, Jui-Lien Wang, and Meei-Shyuan Lee. 2015. "Optimal Dietary and Plasma Magnesium Statuses Depend on Dietary Quality for a Reduction in the Risk of All-Cause Mortality in Older Adults" Nutrients 7, no. 7: 5664-5683. https://0-doi-org.brum.beds.ac.uk/10.3390/nu7075244