Effect of a School-Based Intervention on Nutritional Knowledge and Habits of Low-Socioeconomic School Children in Israel: A Cluster-Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
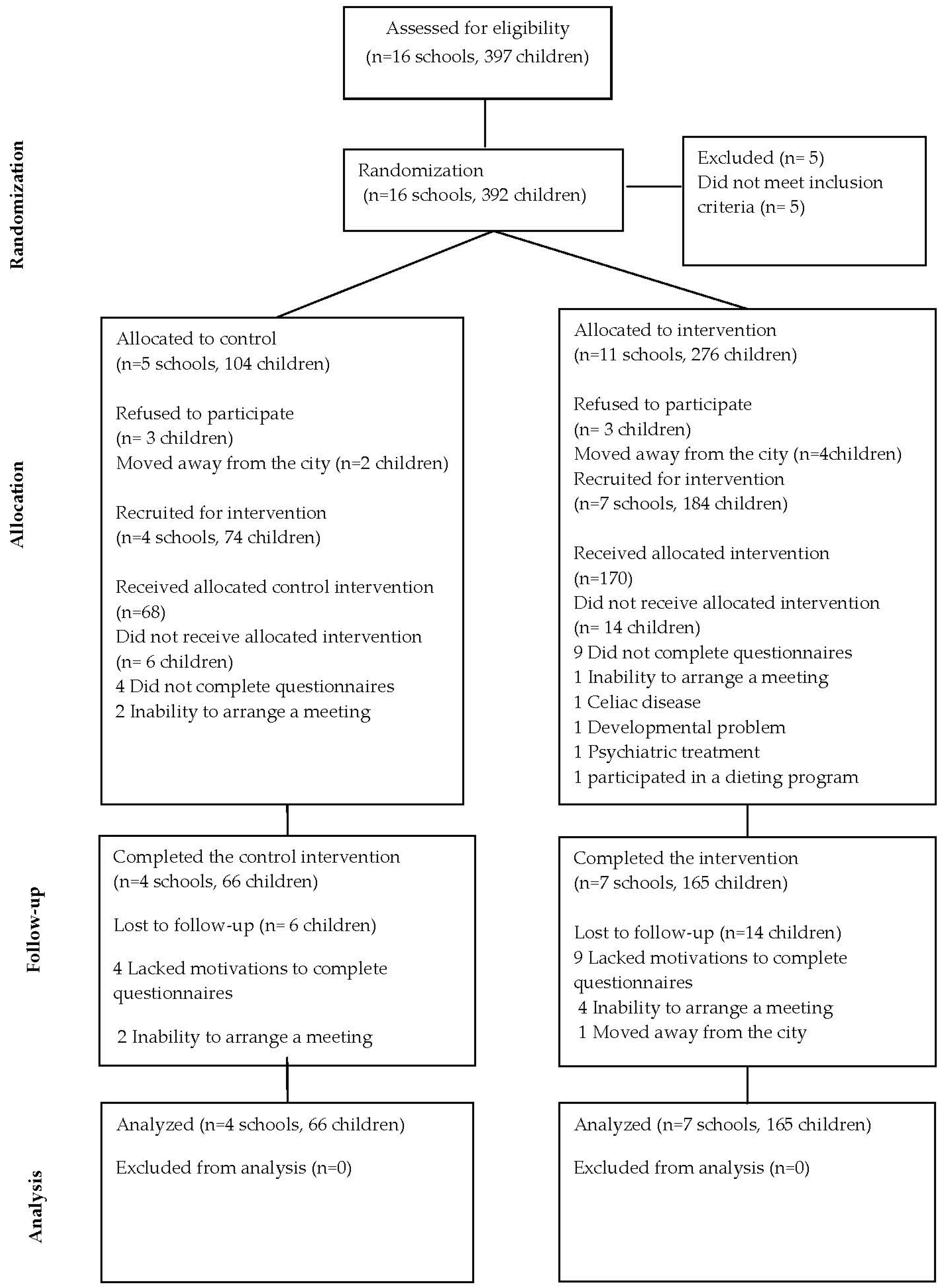
2.1. Study Population and Design
2.2. Sample Size
2.3. Randomization
2.4. Intervention Design
2.5. Data Collection
2.6. Measures
2.6.1. Demographics
2.6.2. Main Outcome Measures
Nutritional Habits
Packed Lunch Score
Physical Activity and Sedentary Behaviors
2.7. Secondary Outcome Measures
2.7.1. Evaluation of Children’s Nutritional Knowledge
2.7.2. Anthropometric Measurements
2.8. Statistical Analysis
3. Results
3.1. Characteristics and Adherence
3.2. Children’s Eating Habits
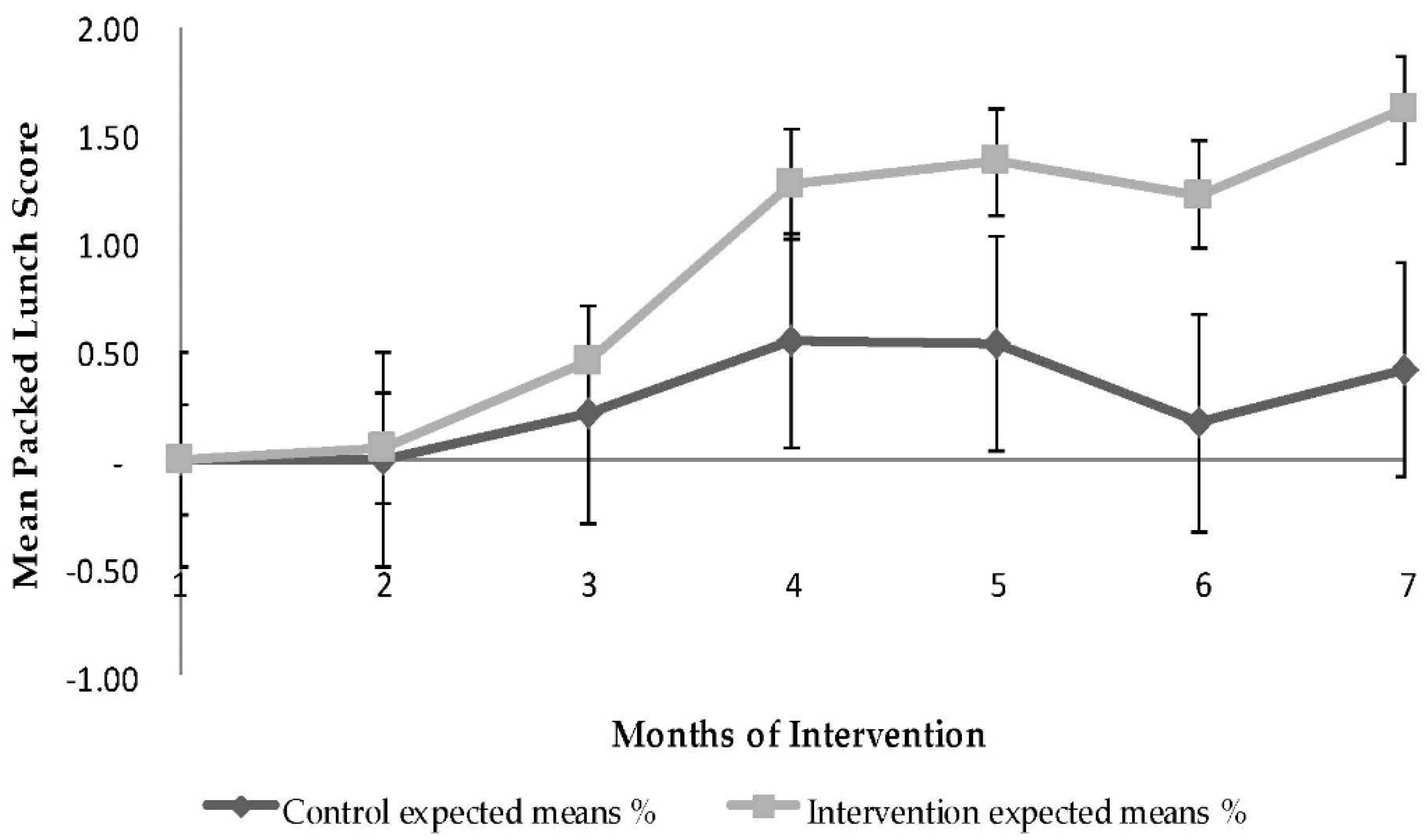
3.3. Quality of Packed Lunch
3.4. Physical Activity
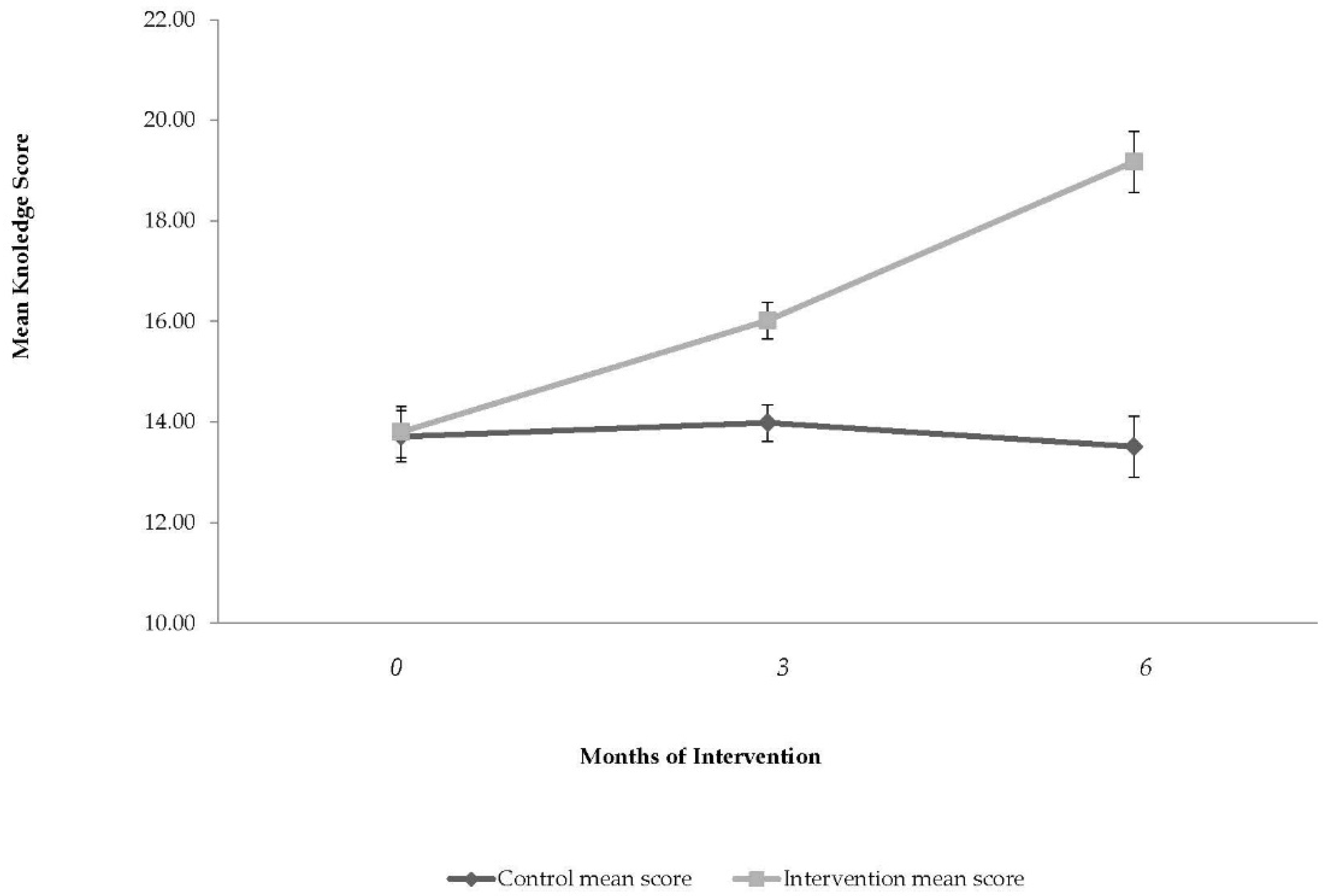
3.5. Children’s Nutritional Knowledge
3.6. Weight
4. Discussion
Limitations and Strengths
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | linear dichroism |
Appendix A: Intervention program

{kind=link}
{kind=link}
{kind=link}
| Week | Objective | Themes | Specific Methods |
|---|---|---|---|
| 1 | Understand how the body works and the importance of healthy food and drinks | The importance of healthy food and drinks and active lifestyle to our health | Food samples (healthy vs. non-healthy). A doll (that the dietitian uses for example themes) |
| 2 | Understand the importance of water to our body | Why do we need water? | A doll (that the dietitian uses for example themes) |
| How do we know we drink enough water? | Water and juice | ||
| 3 | Fruit and vegetables | Vitamins and minerals in fruit and vegetables | Examples of various fruit and vegetables |
| The importance of eating fruit and vegetables of five colors | Preparation of a vegetable salad in five colors | ||
| 4 | Smart choices when eating sweets | What is in the sweets group? | Preparing a carrot cake |
| What is a portion which is reasonable for a child to eat? | Examples of sweets portions | ||
| Celebrating holidays with healthy/yummy food | A doll (that the dietitian uses for example themes) | ||
| 5 | Understand the importance of eating good proteins for growth | What are proteins? | Food samples |
| Why are proteins important for us? | A doll (that the dietitian uses for example themes) | ||
| 6 | Understand the importance of legumes for healthy food choices | Identifying legumes | Cooking lentil soup |
| A doll (that the dietitian uses for example themes) | |||
| 7 | Fats and oils in our food | ||
| 8 | Ability to be make smart food choices | How to help your family prepare a healthy meal | Making smart choices from pictures |
| Preparing a fruit salad | |||
| 9 | How to choose a healthy sandwich | What is a healthy sandwich? | Preparing of sample sandwiches |
| Choosing a sandwich from pictures | |||
| Composing healthy sandwiches from food models | |||
| 10 | Understanding what is a healthy meal | What contains a healthy meal? Food alternatives | Preparing a healthy meal from food models |
| What should my body get during a whole day? | A doll (that the dietitian uses for example themes) |
| Week | Objective | Themes |
|---|---|---|
| 1 | Introduction to health promotion | Health promotion. Health promoting schools |
| 2 | Enhance teachers’ motivation and health leadership | The teacher as a leader of health promoting school |
| 3 | Adopting health promotion strategies to developmental stages in the life of children | Psychological development of school children |
| 4 | Disease prevention | The association between adverse lifestyle habits and future diseases |
| 5 | To understand the importance of breakfast | Breakfast importance |
| 6 | Enhance schoolteacher leadership by supplying behavioral tools | Conflict management with mothers and children |
| 7 | How to aid developing a positive body image among children | The development of body image of children during the early years of life |
| 8 | Supply the teacher with budgetary knowledge on how to prepare healthy snacks, sandwiches, and meals with low budgets in a culturally diverse school | Budget limitations and healthy eating |
| 9 | Introduction to physical activity of young children | Physical activity skills in school aged children |
| 10 | To promote hygiene in the school | Hygiene in the school |
| 11 | Experiencing physical activities adapted to young children | Physical activity skills in school aged children |
| 12 | Create ordinary activities with the teacher to enhance healthy school environment | Every-day life activities to promote healthy school |
| Meeting Number | Children/Mothers | Themes | Specific Methods |
|---|---|---|---|
| 1 | Mothers only | Health food budget management |
|
| 2 | Mothers only | Healthy food budget implementation |
|
| 3 | Children + mothers | Preparing healthy sandwiches with a reasonable budget |
|
Physical Activity Intervention Themes (children’s intervention, both groups)
References
- Wijlaars, L.P.; Johnson, L.; van Jaarsveld, C.H.; Wardle, J. Socioeconomic status and weight gain in early infancy. Int. J. Obes. (Lond.) 2011, 35, 963–970. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, J.A.; Dibley, M.J. Obesity increase among low SES Australian schoolchildren between 2000 and 2006: Time for preventive interventions to target children from low income schools? Int. J. Public Health 2010, 55, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Brauchla, M.; Juan, W.; Story, J.; Kranz, S. Sources of dietary fiber and the association of fiber intake with childhood obesity risk (in 2–18 years old) and diabetes risk of adolescents 12–18 years old: NHANES 2003–2006. J. Nutr. Metab. 2012. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [PubMed]
- Sanchez-Villegas, A.; Pimenta, A.M.; Beunza, J.J.; Guillen-Grima, F.; Toledo, E.; Martinez-Gonzalez, M.A. Childhood and young adult overweight/obesity and incidence of depression in the SUN project. Obesity 2010, 18, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Kalarchian, M.A.; Marcus, M.D. Psychiatric comorbidity of childhood obesity. Int. Rev. Psychiatry 2012, 24, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.K.; Condon, E.; Briefel, R.R.; Reidy, K.C.; Deming, D.M. Food consumption patterns of young preschoolers: Are they starting off on the right path? J. Am. Diet. Assoc. 2010, 110, S52–S59. [Google Scholar] [CrossRef] [PubMed]
- Wanders, A.J.; van den Borne, J.J.; de Graaf, C.; Hulshof, T.; Jonathan, M.C.; Kristensen, M.; Mars, M.; Schols, J.A.; Feskens, E.J.M. Effects of dietary fibre on subjective appetite, energy intake and body weight: A systematic review of randomized controlled trials. Obes. Rev. 2011, 12, 724–739. [Google Scholar] [CrossRef] [PubMed]
- Nyaradi, A.; Li, J.; Hickling, S.; Foster, J.; Oddy, W.H. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front. Hum. Neurosci. 2013, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, G.; Oenema, A.; Kremers, S.P.; van de Mheen, D. Clustering of diet-and activity-related parenting practices: Cross-sectional findings of the INPACT study. Int. J. Behav. Nutr. Phys. Act. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94, 2006S–2011S. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Davison, K.K. Family environmental factors influencing the developing behavioral controls of food intake and childhood overweight. Pediatr. Clin. North Am. 2001, 48, 893–907. [Google Scholar] [CrossRef]
- Vereecken, C.; Maes, L. Young children’s dietary habits and associations with the mothers’ nutritional knowledge and attitudes. Appetite 2010, 54, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 12. [Google Scholar] [CrossRef]
- Hu, C.; Ye, D.; Li, Y.; Huang, Y.; Li, L.; Gao, Y.; Wang, S. Evaluation of a kindergarten-based nutrition education intervention for pre-school children in China. Public Health Nutr. 2010, 13, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Nemet, D.; Geva, D.; Eliakim, A. Health promotion intervention in low socioeconomic kindergarten children. J. Pediatr. 2011, 158, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Ohly, H.; Pealing, J.; Hayter, A.K.; Pettinger, C.; Pikhart, H.; Watt, R.G.; Rees, G. Parental food involvement predicts parent and child intakes of fruits and vegetables. Appetite 2013, 69, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; van Assema, P.; Kremers, S.P. Physical activity, sedentary behavior, and dietary patterns among children. Curr. Nutr. Rep. 2013, 2, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Monasta, L.; Batty, G.D.; Macaluso, A.; Ronfani, L.; Lutje, V.; Bavcar, A.; van Lenthe, F.J.; Brug, J.; Cattaneo, A. Interventions for the prevention of overweight and obesity in preschool children: A systematic review of randomized controlled trials. Obes. Rev. 2011, 12, e107–e118. [Google Scholar] [CrossRef] [PubMed]
- Olsen, N.J.; Mortensen, E.L.; Heitmann, B.L. Predisposition to obesity: Should we target those most susceptible? Curr. Obes. Rep. 2012, 1, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Dennison, B.A.; Russo, T.J.; Burdick, P.A.; Jenkins, P.L. An intervention to reduce television viewing by preschool children. Arch. Pediatr. Adolesc. Med. 2004, 158, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Arcan, C.; Hannan, P.J.; Himes, J.H.; Fulkerson, J.A.; Rock, B.H.; Smyth, M.; Story, M. Intervention effects on kindergarten and first-grade teachers’ classroom food practices and food-related beliefs in American Indian reservation schools. J. Acad. Nutr. Diet. 2013, 113, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, L.; Montgomery, C.; Williamson, A.; Fisher, A.; MCColl, J.H.; lo Conte, R.; Paton, J.Y.; Grant, S. Physical activity to prevent obesity in young children: Cluster randomised controlled trial. BMJ 2006, 333, 1041. [Google Scholar] [CrossRef] [PubMed]
- Annesi, J.J.; Smith, A.E.; Tennant, G.A. Effects of the start for life treatment on physical activity in primarily African American preschool children of ages 3–5 years. Psychol. Health Med. 2013, 18, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Puder, J.J.; Marques-Vidal, P.; Schindler, C.; Zahner, L.; Niederer, I.; Bürgi, F.; Ebenegger, V.; Nydegger, A.; Kriemler, S. Effect of multidimensional lifestyle intervention on fitness and adiposity in predominantly migrant preschool children (Ballabeina): Cluster randomised controlled trial. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Silva-Sanigorski, A.M.; Bell, A.C.; Kremer, P.; Nichols, M.; Crellin, M.; Smith, M.; Sharp, S.; de Groot, F.; Carpenter, L.; Boak, R.; et al. Reducing obesity in early childhood: Results from Romp & Chomp, an Australian community-wide intervention program. Am. J. Clin. Nutr. 2010, 91, 831–840. [Google Scholar] [PubMed]
- Barkali, N.; Endeweld, M.; Fruman, A.; Gottlieb, D. Poverty and Social Gaps Annual Report; National Insurance Institute: Jerusalem, Israel, 2008. [Google Scholar]
- Portes, A. Immigration theory for a new century: Some problems and opportunities. Int. Migr. Rev. 1997, 31, 799–825. [Google Scholar] [CrossRef] [PubMed]
- Kaufman-Shriqui, V.; Entin, A.; Fraser, D.; Novack, Y.; Bilenko, N.; Vardi, H.; Shahar, D.R. Development and validation of food frequency questionnaire for children age 5–6 using multiple methods. Int. J. Child. Health Nutr. 2013, 2, 367–376. [Google Scholar]
- Roodenburg, A.J.; Schlatmann, A.; Dötsch-Klerk, M.; Daamen, R.; Dong, J.; Guarro, M.; Stergiou, M.; Sayed, N.; Ronoh, E.; Lansen, L.; et al. Potential effects of nutrient profiles on nutrient intakes in the Netherlands, Greece, Spain, USA, Israel, China and South-Africa. PLoS ONE 2011, 6, e14721. [Google Scholar] [CrossRef] [PubMed]
- Golan, M.; Weizman, A. Reliability and validity of the family eating and activity habits questionnaire. Eur. J. Clin. Nutr. 1998, 52, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Calfas, K.J.; Sallis, J.F.; Nader, P.R. The development of scales to measure knowledge and preference for diet and physical activity behavior in 4- to 8-year-old children. J. Dev. Behav. Pediatr. 1991, 12, 185–190. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Zeger, S.L.; Liang, K.Y.; Albert, P.S. Models for longitudinal data: A generalized estimating equation approach. Biometrics 1988, 44, 1049–1060. [Google Scholar] [CrossRef] [PubMed]
- Briefel, R.R.; Wilson, A.; Gleason, P.M. Consumption of low-nutrient, energy-dense foods and beverages at school, home, and other locations among school lunch participants and nonparticipants. J. Am. Diet. Assoc. 2009, 109, S79–S90. [Google Scholar] [CrossRef] [PubMed]
- Briley, M.E.; Ranjit, N.; Hoelscher, D.M.; Sweitzer, S.J.; Almansour, F.; Roberts-Gray, C. Unbundling outcomes of a multilevel intervention to increase fruit, vegetables, and whole grains parents pack for their preschool children in sack lunches. Am. J. Health Educ. 2012, 43, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Sweitzer, S.J.; Briley, M.E.; Roberts-Gray, C.; Hoelscher, D.M.; Harrist, R.B.; Staskel, D.M.; Almansour, F.D. Lunch is in the bag: Increasing fruits, vegetables, and whole grains in sack lunches of preschool-aged children. J. Am. Diet. Assoc. 2010, 110, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.; Huybrechts, I.; van Houte, H.; Martens, V.; Wittebroodt, I.; Maes, L. Results from a dietary intervention study in preschools “beastly healthy at school”. Int. J. Public Health 2009, 54, 142–149. [Google Scholar] [CrossRef] [PubMed]
- DeBoer, M.D.; Scharf, R.J.; Demmer, R.T. Sugar-sweetened beverages and weight gain in 2- to 5-year-old children. Pediatrics 2013, 132, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; King, L.; Kelly, B.; Farrell, L.; Howlett, S. Munch and move: Evaluation of a preschool healthy eating and movement skill program. Int. J. Behav. Nutr. Phys. Act. 2010. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Obbagy, J.E.; Altman, J.M.; Essery, E.V.; McGrane, M.M.; Wong, Y.P.; Spahn, J.M.; Williams, C.L. Dietary energy density and body weight in adults and children: A systematic review. J. Acad. Nutr. Diet. 2012, 112, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbon, M.L.; Stolley, M.R.; Schiffer, L.A.; Braunschweig, C.L.; Gomez, S.L.; van Horn, L.; Dyer, A.R. Hip-hop to health Jr. obesity prevention effectiveness trial: Postintervention results. Obesity 2011, 19, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbon, M.L.; Stolley, M.R.; Schiffer, L.; van Horn, L.; KauferChristoffel, K.; Dyer, A. Two-year follow-up results for hip-hop to health Jr.: A randomized controlled trial for overweight prevention in preschool minority children. J. Pediatr. 2005, 146, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Manios, Y.; Kondaki, K.; Kourlaba, G.; Grammatikaki, E.; Birbilis, M.; Ioannou, E. Television viewing and food habits in toddlers and preschoolers in Greece: The GENESIS study. Eur. J. Pediatr. 2009, 168, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.M.; Agaronov, A.; Grytsenko, K.; Yeh, M.C. Intervening to reduce sedentary behaviors and childhood obesity among school-age youth: A systematic review of randomized trials. J. Obes. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]



| Variable Children Preschool Classes | All (n = 238) (n = 11) | Control (n = 68) (n = 4) | Intervention (n = 170) (n = 7) | p Value |
|---|---|---|---|---|
| Age, (mean ± SD), months | 63.4 ± 6.5 | 62.6 ± 6.9 | 63.8 ± 6.4 | 0.12 |
| Gender, (male/female) | 113/125 | 35/33 | 78/92 | 0.48 |
| Weight z-score, (mean ± SD), kg | 0.3 ± 1.3 | 0.5 ± 1.6 | 0.2 ± 1.2 | 0.10 |
| Height z-score, (mean ± SD), cm | −0.1 ± 1.1 | −0.1 ± 1.1 | −0.1 ± 1.0 | 0.89 |
| BMI z-score, (mean ± SD) | 0.5 ± 1.3 | 0.9 ± 1.6 | 0.4 ± 1.1 | 0.01 * |
| BMI, (mean ± SD) | 16.3 ± 2.2 | 16.8 ± 2.8 | 16.0 ± 1.9 | 0.01 * |
| Physical activity, (mean ± SD), h/week | 2.4 ± 1.2 | 2.3 ± 1.2 | 2.5 ± 1.2 | 0.32 |
| Sedentary hours, (mean ± SD), h/day | 2.6 ± 1.4 | 3.0 ± 1.7 | 2.4 ± 1.2 | 0.01 * |
| Sleeping hours, (mean ± SD), h/night | 9.8 ± 1.3 | 10.0 ± 1.3 | 9.8 ± 1.3 | 0.26 |
| Family characteristics | ||||
| Below poverty line (%) | 32.2 | 26.9 | 34.3 | 0.28 |
| Number of siblings (%) | ||||
| 0–1 | 42.9 | 43.5 | 42.7 | 0.92 |
| 2 | 23.5 | 21.7 | 24.2 | |
| 3+ | 36.6 | 34.8 | 33.1 | |
| Religiosity (%) | ||||
| Secular | 33.1 | 34.8 | 32.4 | 0.74 |
| Traditional | 43.3 | 44.9 | 42.6 | |
| Orthodox | 23.7 | 20.3 | 25 | |
| Current parental smoking (%) | 58.2 | 61.2 | 57.0 | 0.56 |
| Single parents (%) | 22.6 | 21.4 | 23.0 | 0.86 |
| Nutritional Habit | Intervention Group | p Value † | |
|---|---|---|---|
| Intervention | Control | ||
| n | 170 | 68 | |
| Eating a variety of foods | |||
| Baseline n (%) | 92 (54.1) | 33 (48.5) | 0.45 |
| 3 months from baseline n (%) | 133 (80.6) | 37 (56.1) | |
| 3 months change from baseline (%) | 48.9 | 15.6 | <0.001 a |
| 6 months from baseline n (%) | 127 (79.4) | 34 (56.6) | |
| 6 months change from baseline (%) | 46.7 | 16.8 | <0.001 a |
| Daily vegetables eating | |||
| Baseline n (%) | 96 (56.5) | 36 (52.9) | 0.41 |
| 3 months from baseline n (%) | 134 (81.2) | 41 (62.1) | |
| 3 months change from baseline (%) | 43.7 | 17.4 | 0.001 a |
| 6 months from baseline n (%) | 126 (78.8) | 37 (61.7) | |
| 6 months change from baseline (%) | 39.4 | 16.5 | 0.001 a |
| Consume sweet and candies on a daily basis | |||
| Baseline n (%) | 91 (53.5) | 33 (48.5) | 0.23 |
| 3 months from baseline n (%) | 59 (35.8) | 20 (30.3) | |
| 3 months change from baseline (%) | −33.2 | −37.5 | 0.08 |
| 6 months from baseline n (%) | 49 (30.6) | 20 (33.3) | |
| 6 months change from baseline (%) | −42.8 | −31.3 | 0.13 |
| Habitual water drinking | |||
| Baseline n (%) | 74 (43.5) | 27 (39.7) | 0.80 |
| 3 months from baseline n (%) | 107 (64.8) | 33 (50.5) | |
| 3 months change from baseline (%) | 49.1 | 25.9 | 0.003 b |
| 6 months from baseline n (%) | 100 (62.5) | 31 (51.6) | |
| 6 months change from baseline (%) | 43.7 | 30.1 | 0.02 |
| Daily consumption of sugar-sweetened beverage | |||
| Baseline n (%) | 79 (46.5) | 34 (50.0) | 0.70 |
| 3 months from baseline n (%) | 45 (27.3) | 24 (36.4) | |
| 3 months change from baseline (%) | −41.3 | −27.2 | 0.02 b |
| 6 months from baseline n (%) | 50 (31.2) | 25 (41.7) | |
| 6 months change from baseline (%) | −32.8 | −16.6 | 0.05 b |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaufman-Shriqui, V.; Fraser, D.; Friger, M.; Geva, D.; Bilenko, N.; Vardi, H.; Elhadad, N.; Mor, K.; Feine, Z.; Shahar, D.R. Effect of a School-Based Intervention on Nutritional Knowledge and Habits of Low-Socioeconomic School Children in Israel: A Cluster-Randomized Controlled Trial. Nutrients 2016, 8, 234. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8040234
Kaufman-Shriqui V, Fraser D, Friger M, Geva D, Bilenko N, Vardi H, Elhadad N, Mor K, Feine Z, Shahar DR. Effect of a School-Based Intervention on Nutritional Knowledge and Habits of Low-Socioeconomic School Children in Israel: A Cluster-Randomized Controlled Trial. Nutrients. 2016; 8(4):234. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8040234
Chicago/Turabian StyleKaufman-Shriqui, Vered, Drora Fraser, Michael Friger, Dikla Geva, Natalya Bilenko, Hillel Vardi, Naama Elhadad, Karen Mor, Zvi Feine, and Danit R. Shahar. 2016. "Effect of a School-Based Intervention on Nutritional Knowledge and Habits of Low-Socioeconomic School Children in Israel: A Cluster-Randomized Controlled Trial" Nutrients 8, no. 4: 234. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8040234