Dietary Pattern Trajectories from 6 to 12 Months of Age in a Multi-Ethnic Asian Cohort

 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Subjects and Methods
2.1. Maternal and Infant Characteristics
2.2. Infant Dietary Assessment
2.3. Identifying Dietary Patterns
2.4. Construction of Dietary Pattern Trajectories
2.5. Statistical Analysis
3. Results
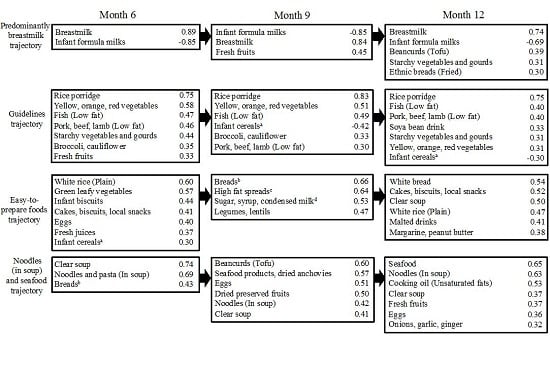
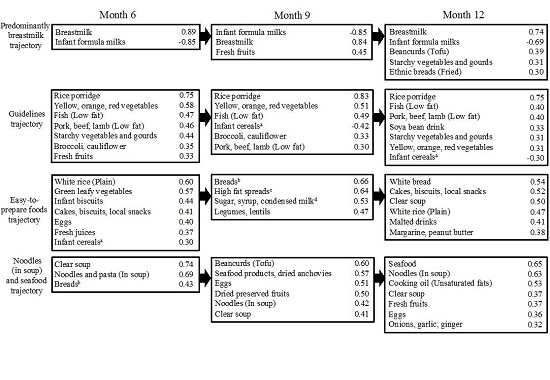
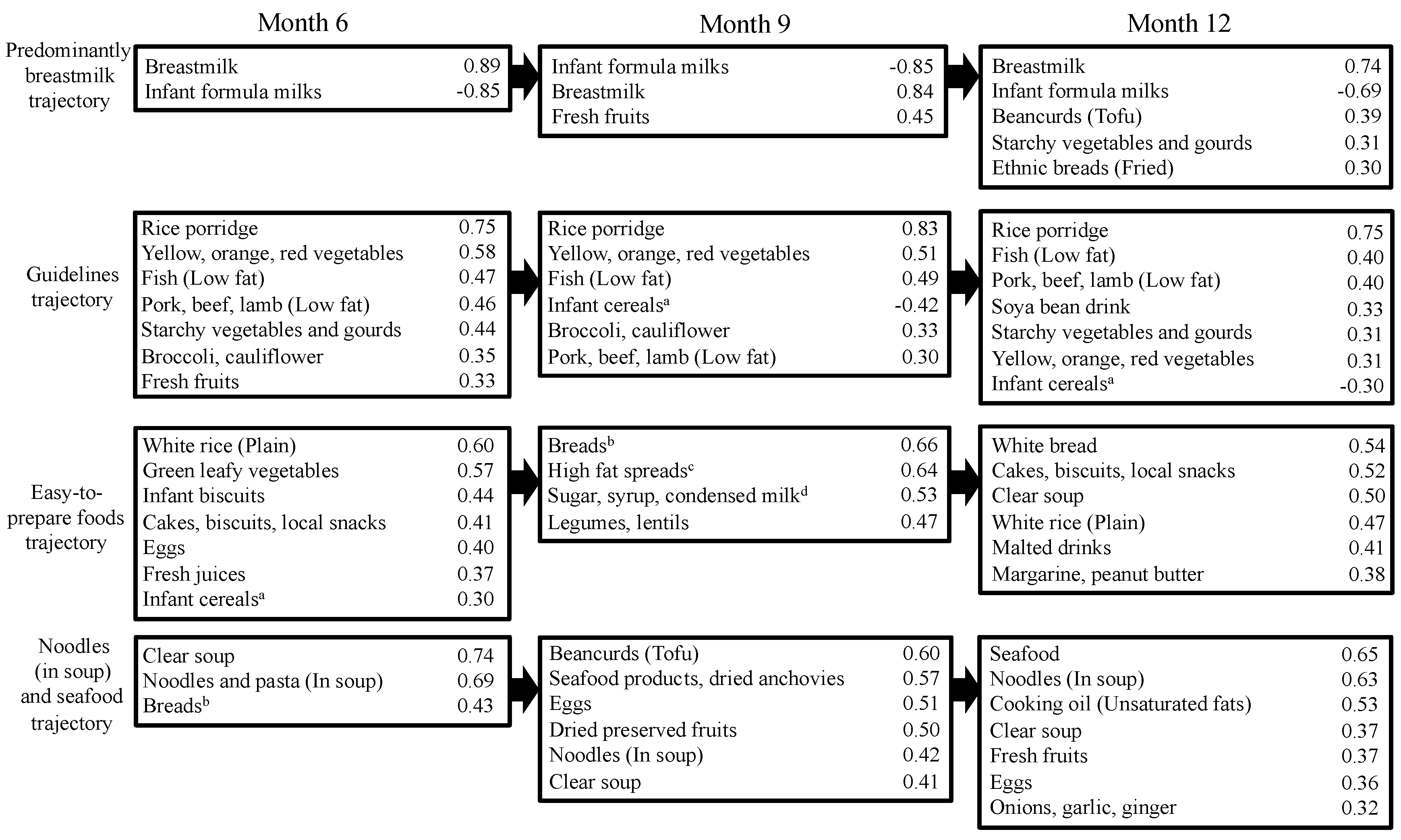
3.1. Dietary Pattern Trajectories
3.2. Characteristics of Study Population with Trajectory Estimates
3.3. Associations with Trajectory Intercepts
3.4. Associations with Trajectory Slopes
4. Discussion
4.1. Dietary Patterns
4.2. Associations between Maternal Factors and Trajectory Intercepts
4.3. Associations between Maternal Factors and Trajectory Slopes
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Oellingrath, I.M.; Svendsen, M.V.; Brantsaeter, A.L. Tracking of eating patterns and overweight—A follow-up study of Norwegian schoolchildren from middle childhood to early adolescence. Nutr. J. 2011, 10, 106. [Google Scholar] [CrossRef] [PubMed]
- Mikkila, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, M.; Brantsæter, A.L.; Haugen, M.; Meltzer, H.M.; Nystad, W.; Andersen, L.F. Changes and tracking of fruit, vegetables and sugar-sweetened beverages intake from 18 months to 7 years in the Norwegian Mother and Child. Cohort Study. BMC Public Health 2013, 13, 793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grieger, J.A.; Scott, J.; Cobiac, L. Dietary patterns and breast-feeding in Australian children. Public Health Nutr. 2011, 14, 1939–1947. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children's Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pract. Res. 2007, 68, s1–s56. [Google Scholar] [PubMed]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Kong, K.L.; Eiden, R.D.; Sharma, N.N.; Xie, C. Sociodemographic differences and infant dietary patterns. Pediatrics 2014, 134, e1387–e1398. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Mølgaard, C.; Michaelsen, K.F.; Carlsen, E.M.; Bro, R.; Pipper, C.B. Indicators of dietary patterns in Danish infants at 9 months of age. Food Nutr. Res. 2015, 59, 27665. [Google Scholar] [PubMed]
- Smithers, L.G.; Golley, R.K.; Mittinty, M.N.; Brazionis, L.; Northstone, K.; Emmett, P.; Lynch, J.W. Dietary patterns at 6, 15 and 24 months of age are associated with IQ at 8 years of age. Eur. J. Epidemiol. 2012, 27, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Martyn, C.N.; Marriott, L.D.; Limond, J.; Crozier, S.; Inskip, H.M.; Godfrey, K.M.; Law, C.M.; Cooper, C.; Robinson, S.M.; et al. Dietary patterns in infancy and cognitive and neuropsychological function in childhood. J. Child. Psychol. Psychiatr. 2009, 50, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Smithers, L.G.; Golley, R.K.; Mittinty, M.N.; Brazionis, L.; Northstone, K.; Emmett, P.; Lynch, J.W. Do dietary trajectories between infancy and toddlerhood influence IQ in childhood and adolescence? Results from a prospective birth cohort study. PLoS ONE 2013, 8, e58904. [Google Scholar]
- Smithers, L.G.; Brazionis, L.; Golley, R.K.; Mittinty, M.N.; Northstone, K.; Emmett, P.; McNaughton, S.A.; Campbell, K.J.; Lynch, J.W. Associations between dietary patterns at 6 and 15 months of age and sociodemographic factors. Eur. J. Clin. Nutr. 2012, 66, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Betoko, A.; Charles, M.A.; Hankard, R.; Forhan, A.; Bonet, M.; Saurel-Cubizolles, M.J.; Heude, B.; de Lauzon-Guillain, B. EDEN mother-child cohort study group. Infant feeding patterns over the first year of life: Influence of family characteristics. Eur. J. Clin. Nutr. 2013, 67, 631–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiefte-de Jong, J.C.; de Vries, J.H.; Bleeker, S.E.; Jaddoe, V.W.; Hofman, A.; Raat, H.; Moll, H.A. Socio-demographic and lifestyle determinants of “Western-like” and “Health conscious” dietary patterns in toddlers. Br. J. Nutr. 2013, 109, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Ystrom, E.; Niegel, S.; Vollrath, M.E. The impact of maternal negative affectivity on dietary patterns of 18-month-old children in the Norwegian Mother and Child. Cohort Study. Matern. Child. Nutr. 2009, 5, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Betoko, A.; Forhan, A.; Charles, M.A.; Heude, B.; de Lauzon-Guillain, B. EDEN Mother–Child Cohort Study Group. Dietary patterns track from infancy to preschool age: Cross-sectional and longitudinal perspectives. J. Nutr. 2015, 145, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Marriott, L.; Poole, J.; Crozier, S.; Borland, S.; Lawrence, W.; Law, C.; Godfrey, K.; Cooper, C.; Inskip, H.; et al. Dietary patterns in infancy: The importance of maternal and family influences on feeding practice. Br. J. Nutr. 2007, 98, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Murakami, K.; Hirota, Y. Osaka Maternal and Child Health Study Group. Dietary patterns in infancy and their associations with maternal socio-economic and lifestyle factors among 758 Japanese mother-child pairs: The Osaka Maternal and Child. Health Study Matern. Child. Nutr. 2014, 10, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Herbison, C.E.; Jacoby, P.; Ambrosini, G.L.; O’Sullivan, T.A.; Ayonrinde, O.T.; Olynyk, J.K.; Black, L.J.; Beilin, L.J.; Mori, T.A.; et al. The Western dietary pattern is prospectively associated with nonalcoholic fatty liver disease in adolescence. Am. J. Gastroenterol. 2013, 108, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Brazionis, L.; Golley, R.K.; Mittinty, M.N.; Smithers, L.G.; Emmett, P.; Northstone, K.; Lynch, J.W. Characterization of transition diets spanning infancy and toddlerhood: A novel, multiple-time-point application of principal components analysis. Am. J. Clin. Nutr. 2012, 95, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Smith, Z.; Knight, T.; Sahota, P.; Kernohan, E.; Baker, M. Dietary patterns in Asian and Caucasian men in Bradford: Differences and implications for nutrition education. J. Hum. Nutr. Diet. 1993, 6, 323–333. [Google Scholar] [CrossRef]
- Vergne, S.; Sauvant, P.; Lamothe, V.; Chantre, P.; Asselineau, J.; Perez, P.; Durand, M.; Moore, N.; Bennetau-Pelissero, C. Influence of ethnic origin (Asian v. Caucasian) and background diet on the bioavailability of dietary isoflavones. Br. J. Nutr. 2009, 102, 1642–1653. [Google Scholar] [PubMed]
- Soh, S.E.; Tint, M.T.; Gluckman, P.D.; Godfrey, K.M.; Rifkin-Graboi, A.; Chan, Y.H.; Stünkel, W.; Holbrook, J.D.; Kwek, K.; Chong, Y.S.; et al. Cohort profile: Growing Up in Singapore Towards healthy Outcomes (GUSTO) birth cohort study. Int. J. Epidemiol. 2014, 43, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [PubMed]
- Ponza, M.; Devaney, B.; Ziegler, P.; Reidy, K.; Squatrito, C. Nutrient intakes and food choices of infants and toddlers participating in WIC. J. Am. Diet. Assoc. 2004, 104, s71–s79. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Chen, H.; Fung, T.T.; Logroscino, G.; Schwarzschild, M.A.; Hu, F.B.; Ascherio, A. Prospective study of dietary pattern and risk of Parkinson disease. Am. J. Clin. Nutr. 2007, 86, 1486–1494. [Google Scholar] [PubMed]
- Crozier, S.R.; Robinson, S.M.; Borland, S.E.; Inskip, H.M.; SWS Study Group. Dietary patterns in the Southampton Women′s Survey. Eur. J. Clin. Nutr. 2006, 60, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Joliffe, I.T.; Morgan, B.J. Principal component analysis and exploratory factor analysis. Stat. Methods Med. Res. 1992, 1, 69–95. [Google Scholar] [CrossRef] [PubMed]
- Michels, K.B.; Schulze, M.B. Can dietary patterns help us detect diet-disease associations? Nutr. Res. Rev. 2005, 18, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Foote, K.D.; Marriott, L.D. Weaning of infants. Arch. Dis. Child. 2003, 88, 488–492. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines Approved by the Guidelines Review Committee. In Infant and Young Child. Feeding: Model. Chapter for Textbooks for Medical Students and Allied Health Professionals; World Health Organization: Geneva, Switzerzland, 2009. [Google Scholar]
- Health Promotion Board. Healthy Start for Your Baby; Health Promotion Board: Singapore, Singapore, 2012. [Google Scholar]
- Heck, K.E.; Braveman, P.; Cubbin, C.; Chávez, G.F.; Kiely, J.L. Socioeconomic status and breastfeeding initiation among California mothers. Public Health Rep. 2006, 121, 51–59. [Google Scholar] [PubMed]
- Celi, A.C.; Rich-Edwards, J.W.; Richardson, M.K.; Kleinman, K.P.; Gillman, M.W. Immigration, race/ethnicity, and social and economic factors as predictors of breastfeeding initiation. Arch. Pediatr. Adolesc. Med. 2005, 159, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, S.S.; Griffiths, L.J.; Dezateux, C.; Law, C. Millennium Cohort Study Child Health Group. Maternal employment and breast-feeding initiation: Findings from the Millennium Cohort Study. Paediatr. Perinat. Epidemiol. 2007, 21, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Khoury, A.J.; Moazzem, S.W.; Jarjoura, C.M.; Carothers, C.; Hinton, A. Breast-feeding initiation in low-income women: Role of attitudes, support, and perceived control. Womens Health Issues 2005, 15, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Barton, S.J. Infant feeding practices of low-income rural mothers. MCN Am. J. Matern Child. Nurs. 2001, 26, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Manpower. Maternity Leave Eligibility and Entitlement, 2016. Available online: http://www.mom.gov.sg/employment-practices/leave/maternity-leave/eligibility-and-entitlement (accessed on 1 June 2016).
- Bava, C.M.; Jaeger, S.R.; Park, J. Constraints upon food provisioning practices in “busy” women’s lives: trade-offs which demand convenience. Appetite 2008, 50, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G. Nutrition, growth, and complementary feeding of the breastfed infant. Pediatr. Clin. N. Am. 2001, 48, 87–104. [Google Scholar] [CrossRef]
- WHO. Report by the Secretariat. In Infant and Young Children Nutrition; Global Strategy for Infant and Young Child Feeding; WHA55.25 Geneva: Fifty-fifth World Health Assembly; WHO: Geneva, Switerzland, 2002. [Google Scholar]


{kind=link}
{kind=link}
| Maternal and Child Characteristics | β (95% CI) | |||
|---|---|---|---|---|
| Predominantly Breastmilk | Guidelines | Easy-to-Prepare Foods | Noodles (in Soup) and Seafood | |
| Maternal characteristics | ||||
| Ethnicity | ||||
| Indian | −0.245 (−0.463, −0.026) * | 0.069 (−0.035, 0.173) | 0.123 (0.063, 0.184) *** | 0.028 (−0.015, 0.072) |
| Malay | −0.259 (−0.476, −0.042) * | −0.069 (−0.172, 0.034) | 0.031 (−0.029, 0.091) | 0.028 (−0.015, 0.071) |
| Chinese | Reference | Reference | Reference | Reference |
| Maternal Age | ||||
| 18–29 | 0.084 (−0.123, 0.292) | −0.026 (−0.125, 0.073) | −0.088 (−0.145, −0.030) ** | 0.035 (−0.006, 0.076) |
| 30–34 | 0.040 (−0.161, 0.241) | −0.006 (−0.102, 0.089) | −0.069 (−0.125, −0.014) * | 0.034 (−0.005, 0.074) |
| >34 | Reference | Reference | Reference | Reference |
| Maternal Education b | ||||
| Primary education | −0.781 (−1.021, −0.541) *** | 0.081 (−0.033, 0.195) | −0.025 (−0.091, 0.041) | −0.003 (−0.051, 0.044) |
| Post-secondary | −0.480 (−0.683, −0.277) *** | 0.174 (0.077, 0.270) *** | <0.001 (−0.056, 0.056) | −0.007 (−0.047, 0.033) |
| University and other | Reference | Reference | Reference | Reference |
| Household Income (SGD) | ||||
| <1999 | −0.441 (−0.746, −0.137) ** | −0.065 (−0.21, 0.080) | 0.053 (−0.031, 0.137) | −0.013 (−0.073, 0.047) |
| 2000–5999 | −0.057 (−0.258, 0.145) | −0.034 (−0.13, 0.061) | 0.019 (−0.037, 0.074) | 0.029 (−0.010, 0.069) |
| >6000 | Reference | Reference | Reference | Reference |
| Employment | ||||
| Unemployed | 0.273 (0.096, 0.449) ** | 0.014 (−0.069, 0.098) | 0.009 (−0.040, 0.058) | 0.019 (−0.016, 0.054) |
| Employed | Reference | Reference | Reference | Reference |
| Maternal BMI at 26 weeks c | ||||
| <18.5–24.9 | 0.126 (−0.093, 0.344) | 0.015 (−0.089, 0.119) | 0.010 (−0.050, 0.070) | −0.022 (−0.065, 0.022) |
| 25.0–29.9 | 0.214 (−0.005, 0.433) | 0.059 (−0.045, 0.163) | 0.015 (−0.046, 0.075) | −0.009 (−0.052, 0.034) |
| >30.0 | Reference | Reference | Reference | Reference |
| Alcohol d | ||||
| Yes | 0.080 (−0.095, 0.255) | 0.030 (−0.053, 0.113) | −0.019 (−0.068, 0.029) | 0.013 (−0.021, 0.048) |
| No | Reference | Reference | Reference | Reference |
| Smoking d | ||||
| Yes | −0.209 (−0.456, 0.038) | −0.005 (−0.123, 0.112) | 0.039 (−0.030, 0.107) | −0.010 (−0.059, 0.039) |
| No | Reference | Reference | Reference | Reference |
| Cohabitation e | ||||
| Not living together | 0.022 (−0.719, 0.762) | 0.021 (−0.331, 0.372) | −0.039 (−0.244, 0.165) | 0.063 (−0.083, 0.209) |
| Living together | Reference | Reference | Reference | Reference |
| Infant characteristics | ||||
| Gender | ||||
| Female | 0.027 (−0.122, 0.176) | 0.012 (−0.059, 0.082) | −0.042 (−0.083, −0.001) * | −0.016 (−0.045, 0.013) |
| Male | Reference | Reference | Reference | Reference |
| Parity | ||||
| First child | −0.202 (−0.371, −0.033) ** | 0.014 (−0.066, 0.094) | 0.032 (−0.015, 0.079) | 0.005 (−0.029, 0.038) |
| Not first child | Reference | Reference | Reference | Reference |
| Maternal and Child Characteristics | β (95% CI) | |||
|---|---|---|---|---|
| Predominantly Breastmilk | Guidelines | Easy-to-Prepare Foods | Noodles (in soup) and Seafood | |
| Maternal characteristics | ||||
| Ethnicity | ||||
| Indian | 0.026 (0.013, 0.040) *** | −0.040 (−0.052, −0.028) *** | 0.000 (−0.008, 0.008) | −0.013 (−0.020, −0.005) ** |
| Malay | 0.013 (−0.001, 0.026) | −0.014 (−0.026, −0.002) * | 0.004 (−0.004, 0.012) | −0.013 (−0.021, −0.006) ** |
| Chinese | Reference | Reference | Reference | Reference |
| Maternal Age | ||||
| 18–29 | −8.823×10−5 (−0.013, 0.013) | 0.005 (−0.007, 0.016) | 0.009 (0.001, 0.017) * | −0.005 (−0.012, 0.002) |
| 30–34 | 0.003 (−0.010, 0.015) | 0.007 (−0.004, 0.018) | 0.006 (−0.002, 0.013) | −0.003 (−0.010, 0.004) |
| >34 | Reference | Reference | Reference | Reference |
| Maternal Education b | ||||
| Primary education | 0.029 (0.014, 0.044) *** | 0.001 (−0.012, 0.015) | 0.008 (−0.001, 0.017) | −0.002 (−0.010, 0.007) |
| Post-secondary | 0.013 (0.000, 0.026) * | −0.004 (−0.015, 0.007) | 0.003 (−0.004, 0.011) | 0.004 (−0.003, 0.011) |
| University and other | Reference | Reference | Reference | Reference |
| Household Income (SGD) | ||||
| <1999 | 0.002 (−0.017, 0.021) | −0.013 (−0.030, 0.004) | −0.001 (−0.013, 0.010) | −0.001 (−0.011, 0.010) |
| 2000–5999 | −0.009 (−0.022, 0.004) | −0.004 (−0.015, 0.007) | −0.001 (−0.009, 0.006) | −0.002 (−0.009, 0.005) |
| >6000 | Reference | Reference | Reference | Reference |
| Employment | ||||
| Unemployed | 0.007 (−0.004, 0.018) | 0.001 (−0.009, 0.011) | 0.001 (−0.005, 0.008) | 0.002 (−0.004, 0.008) |
| Employed | Reference | Reference | Reference | Reference |
| Maternal BMI at 26 weeks c | ||||
| <18.5–24.9 | −0.010 (−0.023, 0.004) | 0.003 (−0.009, 0.015) | −0.004 (−0.012, 0.004) | 0.003 (−0.004, 0.011) |
| 25.0–29.9 | −0.008 (−0.022, 0.006) | −0.007 (−0.020, 0.005) | −0.002 (−0.010, 0.006) | 0.001 (−0.006, 0.009) |
| >30.0 | Reference | Reference | Reference | Reference |
| Alcohol d | ||||
| Yes | −0.002 (−0.013, 0.009) | −0.002 (−0.011, 0.008) | 0.001 (−0.006, 0.007) | −0.004 (−0.010, 0.002) |
| No | Reference | Reference | Reference | Reference |
| Smoking d | ||||
| Yes | 0.005 (−0.010, 0.020) | −0.004 (−0.017, 0.010) | −0.002 (−0.012, 0.007) | −0.001 (−0.009, 0.008) |
| No | Reference | Reference | Reference | Reference |
| Cohabitation e | ||||
| Not living together | 0.011 (−0.035, 0.058) | −0.002 (−0.042, 0.039) | 0.018 (−0.010, 0.045) | −0.013 (−0.038, 0.013) |
| Living together | Reference | Reference | Reference | Reference |
| Infant characteristics | ||||
| Gender | ||||
| Female | −0.003 (−0.012, 0.006) | −0.005 (−0.014, 0.003) | 0.004 (−0.002, 0.009) | −0.001 (−0.006, 0.004) |
| Male | Reference | Reference | Reference | Reference |
| Parity | ||||
| First child | 0.014 (0.004, 0.025) ** | 0.006 (−0.003, 0.016) | −0.006 (−0.012, 0.001) | −0.004 (−0.010, 0.002) |
| Not first child | Reference | Reference | Reference | Reference |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, G.H.; Toh, J.Y.; Aris, I.M.; Chia, A.-R.; Han, W.M.; Saw, S.M.; Godfrey, K.M.; Gluckman, P.D.; Chong, Y.-S.; Yap, F.; et al. Dietary Pattern Trajectories from 6 to 12 Months of Age in a Multi-Ethnic Asian Cohort. Nutrients 2016, 8, 365. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8060365
Lim GH, Toh JY, Aris IM, Chia A-R, Han WM, Saw SM, Godfrey KM, Gluckman PD, Chong Y-S, Yap F, et al. Dietary Pattern Trajectories from 6 to 12 Months of Age in a Multi-Ethnic Asian Cohort. Nutrients. 2016; 8(6):365. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8060365
Chicago/Turabian StyleLim, Geraldine Huini, Jia Ying Toh, Izzuddin M. Aris, Ai-Ru Chia, Wee Meng Han, Seang Mei Saw, Keith M. Godfrey, Peter D. Gluckman, Yap-Seng Chong, Fabian Yap, and et al. 2016. "Dietary Pattern Trajectories from 6 to 12 Months of Age in a Multi-Ethnic Asian Cohort" Nutrients 8, no. 6: 365. https://0-doi-org.brum.beds.ac.uk/10.3390/nu8060365