
Polysaccharide-Based Micro- and Nanosized Drug Delivery Systems for Potential Application in the Pediatric Dentistry

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Natural Polysaccharide Drug Carriers in Dentistry
3.1. Chitosan
3.2. Sodium Alginate
3.3. Pectin
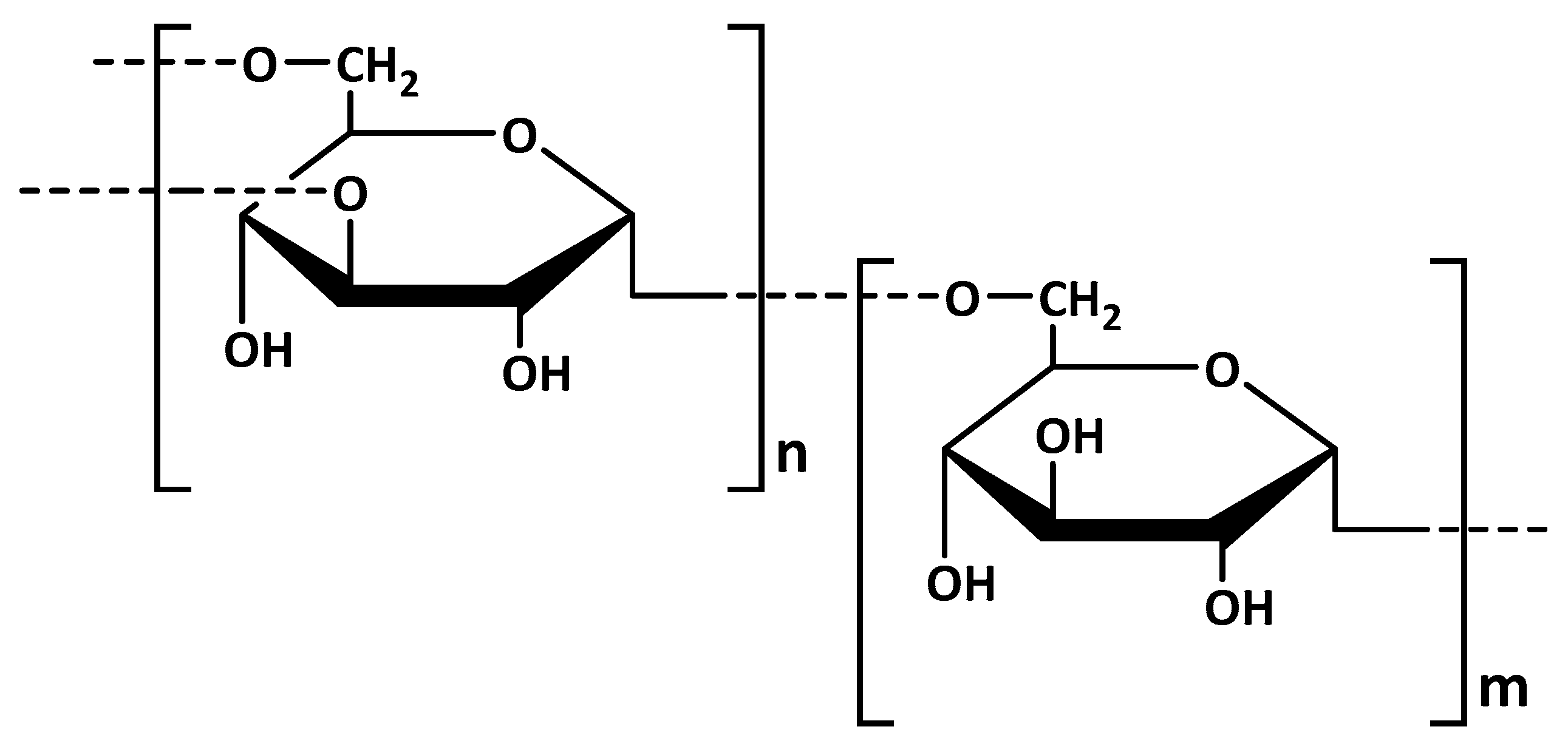
3.4. Dextran
3.5. Starch
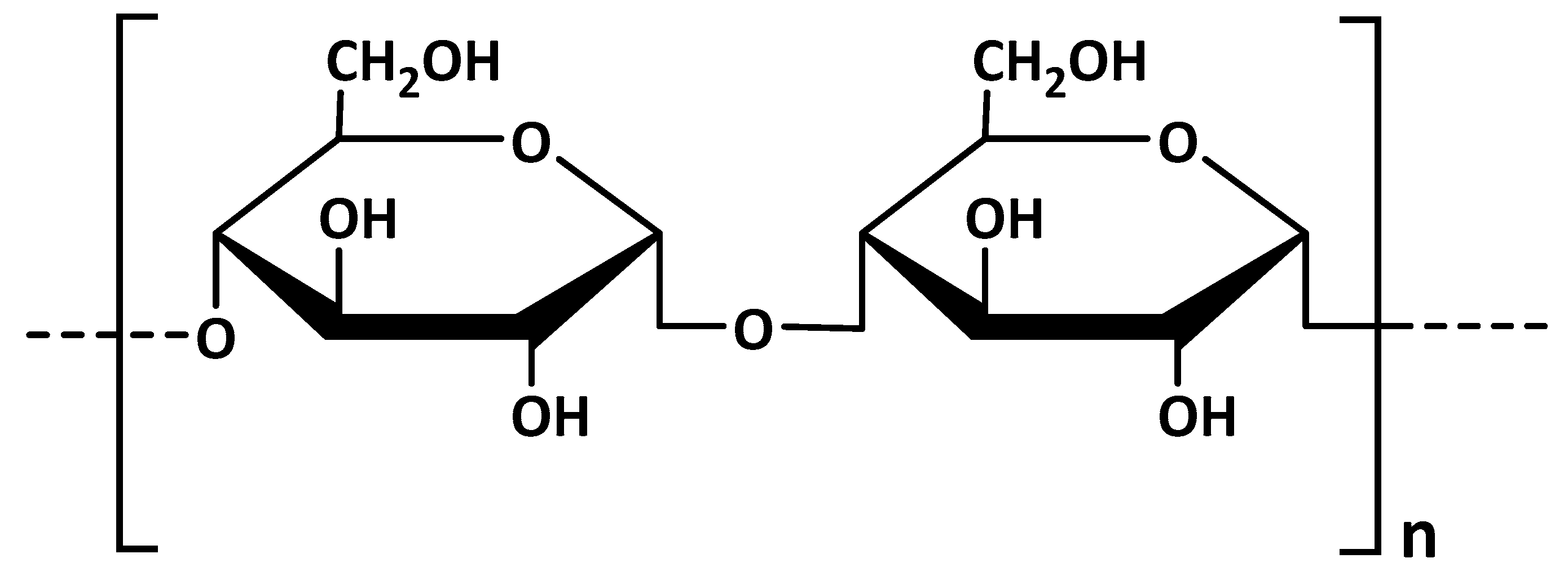
3.6. Other Polysaccharides
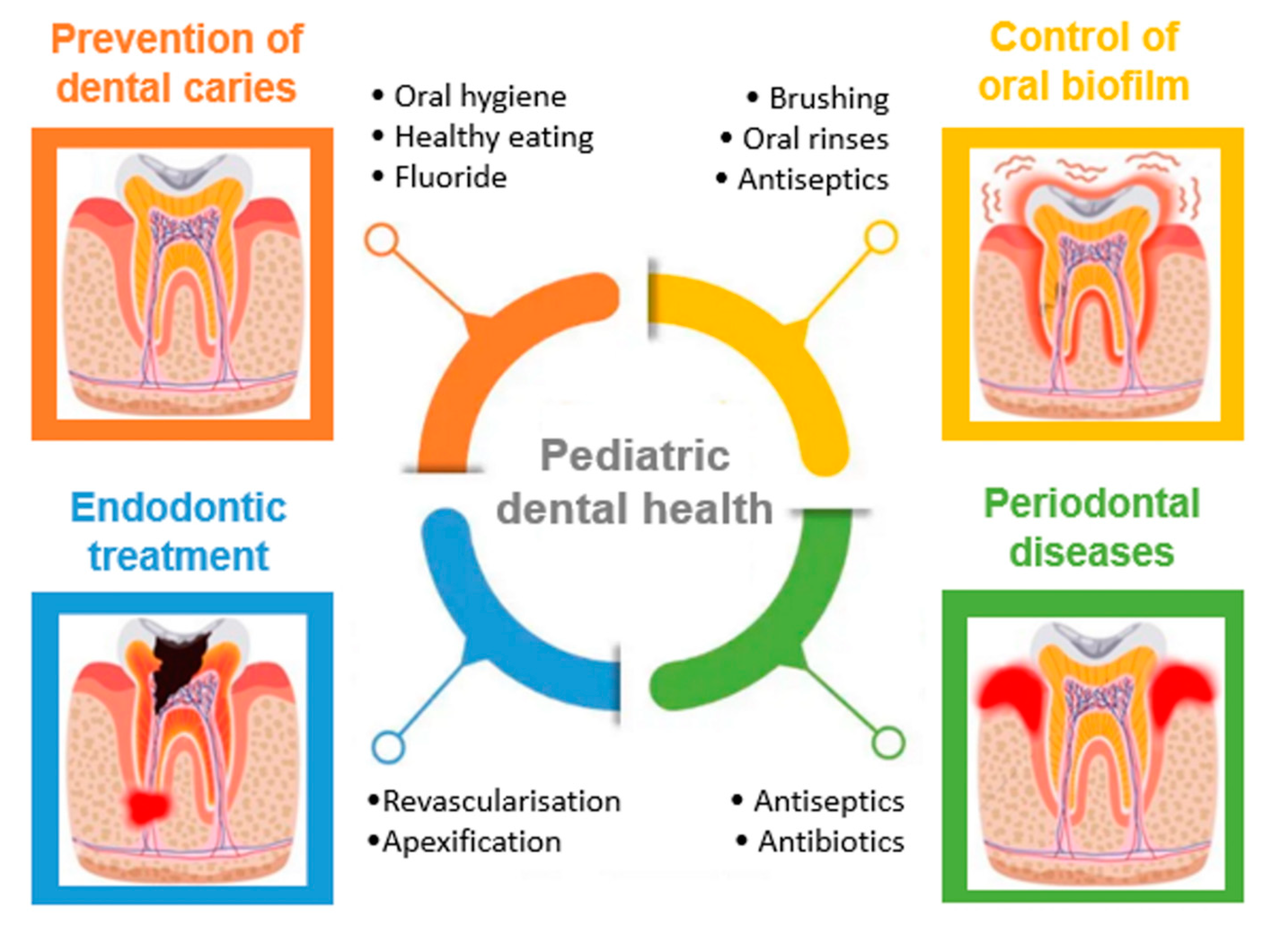
4. Applications of Polysaccharide Micro- and Nanoparticles in Pediatric Dentistry
4.1. Prevention of Dental Caries—Primary and Secondary Prevention
4.1.1. Fluoride
4.1.2. Silver
4.1.3. Calcium Phosphate
4.1.4. Other Effective Preventive Agents
4.2. Control of Oral Biofilm
4.3. Endodontic Treatment
4.4. Periodontal Diseases
4.4.1. Chlorhexidine Gluconate
4.4.2. Antibiotics
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramos-Gomez, F.J.; Crystal, Y.O.; Ng, M.W.; Crall, J.J.; Featherstone, J.D. Pediatric dental care: Prevention and management protocols based on caries risk assessment. J. Calif. Dent. Assoc. 2010, 38, 746–761. [Google Scholar]
- Largent, B.A. The American Academy of Pediatric Dentistry and the specialty of pediatric dentistry. J. Am. Coll. Dent. 2009, 76, 18–22. [Google Scholar]
- Zou, J.; Meng, M.; Law, C.S.; Rao, Y.; Zhou, X. Common dental diseases in children and malocclusion. Int. J. Oral. Sci. 2018, 10, 7. [Google Scholar] [CrossRef]
- Casamassimo, P.S.; Townsend, J.A. 1—The importance of pediatric dentistry. In Pediatric Dentistry Infancy Through Adolescence, 6th ed.; Nowak, A.J., Christensen, J.R., Mabry, T.R., Townsend, J.A., Wells, M.H., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 2–7. [Google Scholar] [CrossRef]
- Zięba, M.; Chaber, P.; Duale, K.; Martinka Maksymiak, M.; Basczok, M.; Kowalczuk, M.; Adamus, G. Polymeric Carriers for Delivery Systems in the Treatment of Chronic Periodontal Disease. Polymers 2020, 12, 1574. [Google Scholar] [CrossRef]
- Ahmadian, E.; Shahi, S.; Yazdani, J.; Maleki Dizaj, S.; Sharifi, S. Local treatment of the dental caries using nanomaterials. Biomed. Pharmacother. 2018, 108, 443–447. [Google Scholar] [CrossRef]
- Huang, J.; Wong, H.L.; Zhou, Y.; Wu, Y.X.; Grad, H.; Komorowski, R.; Friedman, S. In vitro studies and modelling of a controlled-release device for root canal therapy. J. Control Release 2000, 67, 293–307. [Google Scholar] [CrossRef]
- Lee, D.Y.; Spånberg, L.S.W.; Bok, Y.B.; Lee, C.Y.; Kum, K.Y. The sustaining effect of three polymers on the release of chlorhexidine from a controlled release drug device for root canal disinfection. Oral Surg. Oral Med. Oral Pathol. Oral Rad. Endod. 2005, 10, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Birk, S.E.; Boisen, A.; Nielsen, L.H. Polymeric nano- and microparticulate drug delivery systems for treatment of biofilms. Adv. Drug Deliv. Rev. 2021, 174, 30–52. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Chen, W.; Li, F.; Morrow, B.R.; Garcia-Godoy, F.; Hong, L. Sustained Release of Minocycline from Minocycline-Calcium-Dextran Sulfate Complex Microparticles for Periodontitis Treatment. J. Pharm. Sci. 2018, 107, 3134–3142. [Google Scholar] [CrossRef]
- Pistone, S.; Rykke, M.; Smistad, G.; Hiorth, M. Polysaccharide-coated liposomal formulations for dental targeting. Int. J. Pharm. 2017, 516, 106–115. [Google Scholar] [CrossRef] [Green Version]
- Puri, K.; Puri, N. Local drug delivery agents as adjuncts to endodontic and periodontal therapy. J. Med. Life 2013, 6, 414–419. [Google Scholar] [PubMed]
- Pragati, S.; Ashok, S.; Kuldeep, S. Recent advances in periodontal drug delivery systems. Int. J. Drug Deliv. 2009, 1, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Votruba, A.R.; Farokhzad, O.C.; Langer, R. Nanotechnology in drug delivery and tissue engineering: From discovery to applications. Nano Lett. 2010, 10, 3223–3230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patravale, V.B.; Date, A.A.; Kulkarni, R.M. Nanosuspensions: A promising drug delivery strategy. J. Pharm. Pharmacol. 2004, 56, 827–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayak, A.K.; Ahmed, S.A.; Tabish, M.; Hasnain, M.S. Chapter 23—Natural polysaccharides in tissue engineering applications. In Natural Polysaccharides in Drug Delivery and Biomedical Applications, 1st ed.; Hasnain, M.S., Nayak, A.K., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 531–548. [Google Scholar] [CrossRef]
- Claverie, M.; McReynolds, C.; Petitpas, A.; Thomas, M.; Fernandes, S.C.M. Marine-Derived Polymeric Materials and Biomimetics: An Overview. Polymers 2020, 12, 1002. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Yu, S.; Sun, B.; Gao, S.; Guo, S.; Zhao, K. Biomedical Applications of Chitosan and Its Derivative Nanoparticles. Polymers 2018, 10, 462. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Huang, H. Application of dextran as nanoscale drug carriers. Nanomedicine 2018, 13, 3149–3158. [Google Scholar] [CrossRef]
- Venkatesan, J.; Anil, S.; Kim, S.-K.; Shim, M.S. Seaweed Polysaccharide-Based Nanoparticles: Preparation and Applications for Drug Delivery. Polymers 2016, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Jiao, Y.; Wang, Y.; Zhou, C.; Zhang, Z. Polysaccharides-based nanoparticles as drug delivery systems. Adv. Drug Deliv. Rev. 2008, 60, 1650–1662. [Google Scholar] [CrossRef]
- Martău, G.A.; Mihai, M.; Vodnar, D.C. The Use of Chitosan, Alginate, and Pectin in the Biomedical and Food Sector—Biocompatibility, Bioadhesiveness, and Biodegradability. Polymers 2019, 11, 1837. [Google Scholar] [CrossRef] [Green Version]
- Ways, T.M.; Lau, W.M.; Khutoryanskiy, V.V. Chitosan and Its Derivatives for Application in Mucoadhesive Drug Delivery Systems. Polymers 2018, 10, 267. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Hui, D.; Du, C.; Sun, H.; Peng, W.; Pu, X.; Li, Z.; Sun, J.; Zhou, C. Preparation and application of chitosan biomaterials in dentistry. Int. J. Biol. Macromol. 2021, 167, 1198–1210. [Google Scholar] [CrossRef]
- Suresh, P.K.; Dewangan, M.K. Development and in vitro characterization of metronidazole loaded chitosan microspheres for delivery to periodontal pocket. J. Appl. Pharm. Sci. 2011, 1, 165–169. [Google Scholar]
- Pichayakorn, W.; Boonme, P. Evaluation of cross-linked chitosan microparticles containing metronidazole for periodontitis treatment. Mater. Sci. Eng. C 2013, 33, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Aravamudhan, A.; Ramos, D.M.; Nada, A.A.; Kumbar, S.G. Chapter 4—Natural polymers: Polysaccharides and their derivatives for biomedical applications. In Book Natural and Synthetic Biomedical Polymers, 1st ed.; Kumbar, S.G., Laurencin, C.T., Deng, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 67–89. [Google Scholar] [CrossRef]
- Wang, L.; Li, W.; Qin, S. Three Polymers from the Sea: Unique Structures, Directional Modifications, and Medical Applications. Polymers 2021, 13, 2482. [Google Scholar] [CrossRef]
- Díaz-Montes, E. Dextran: Sources, Structures, and Properties. Polysaccharides 2021, 2, 554–565. [Google Scholar] [CrossRef]
- Braga, G.K.; Oliveira, W.P. Manufacturing Drug Loaded Chitosan Microspheres by Spray Drying: Development, Characterization, and Potential Use in Dentistry. Dry. Technol. 2007, 25, 303–310. [Google Scholar] [CrossRef]
- Genta, I.; Perugini, P.; Modena, T.; Pavanetto, F.; Castelli, F.; Muzzarelli, R.A.A.; Muzzarelli, C.; Conti, B. Miconazole-loaded 6-oxychitin–chitosan microcapsules. Carbohydr. Polym. 2003, 52, 11–18. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Y.; Lin, L.; Zhang, J.; Lan, R.; Wu, B. Studies on antimicrobial peptide-loaded nanomaterial for root caries restorations to inhibit periodontitis related pathogens in periodontitis care. J. Microencapsul. 2021, 38, 89–99. [Google Scholar] [CrossRef]
- Ali, A.; Ahmed, S. A review on chitosan and its nanocomposites in drug delivery. Int. J. Biol. Macromol. 2018, 109, 273–286. [Google Scholar] [CrossRef]
- Brasselet, C.; Pierre, G.; Dubessay, P.; Dols-Lafargue, M.; Coulon, J.; Maupeu, J.; Vallet-Courbin, A.; de Baynast, H.; Doco, T.; Michaud, P.; et al. Modification of Chitosan for the Generation of Functional Derivatives. Appl. Sci. 2019, 9, 1321. [Google Scholar] [CrossRef] [Green Version]
- Aguilar, A.; Zein, N.; Harmouch, E.; Hafdi, B.; Bornert, F.; Offner, D.; Clauss, F.; Fioretti, F.; Huck, O.; Benkirane-Jessel, N.; et al. Application of Chitosan in Bone and Dental Engineering. Molecules 2019, 24, 3009. [Google Scholar] [CrossRef] [Green Version]
- Husain, S.; Al-Samadani, K.H.; Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Qasim, S.B. Chitosan Biomaterials for Current and Potential Dental Applications. Materials 2017, 10, 602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radulescu, M.; Ficai, D.; Oprea, O.; Ficai, A.; Andronescu, E.; Holban, A.M. Antimicrobial Chitosan based formulations with impact on different biomedical applications. Curr. Pharm. Biotechnol. 2015, 16, 128–136. [Google Scholar] [CrossRef]
- Yadav, A.; Bhise, S. Chitosan: A potential biomaterial effective against typhoid. Curr. Sci. 2004, 87, 1176–1178. [Google Scholar]
- Qasim, S.B.; Husain, S.; Huang, Y.; Pogorielov, M.; Deineka, V.; Lyndin, M.; Rawlinson, A.; Rehman, I.U. In-vitro and in-vivo degradation studies of freeze gelated porous chitosan composite scaffolds for tissue engineering applications. Polym. Degrad. Stab. 2017, 136, 31–38. [Google Scholar] [CrossRef]
- Ke, C.-L.; Deng, F.-S.; Chuang, C.-Y.; Lin, C.-H. Antimicrobial Actions and Applications of Chitosan. Polymers 2021, 13, 904. [Google Scholar] [CrossRef]
- Aliasghari, A.; Rabbani Khorasgani, M.; Vaezifar, S.; Rahimi, F.; Younesi, H.; Khoroushi, M. Evaluation of antibacterial efficiency of chitosan and chitosan nanoparticles on cariogenic streptococci: An in vitro study. Iran. J. Microbiol. 2016, 8, 93–100. [Google Scholar]
- Covarrubias, C.; Trepiana, D.; Corral, C. Synthesis of hybrid copper-chitosan nanoparticles with antibacterial activity against cariogenic Streptococcus mutans. Dent. Mater. J. 2018, 37, 379–384. [Google Scholar] [CrossRef] [Green Version]
- Young, A.; Smistad, G.; Karlsen, J.; Rolla, G.; Rykke, M. Zeta potentials of human enamel and hydroxyapatite as measured by the coulter DELSA 440. Adv. Dent. Res. 1997, 11, 560–565. [Google Scholar] [CrossRef]
- Divakar, D.D.; Jastaniyah, N.T.; Altamimi, H.G.; Alnakhli, Y.O.; Muzaheed; Alkheraif, A.A.; Haleem, S. Enhanced antimicrobial activity of naturally derived bioactive molecule chitosan conjugated silver nanoparticle against dental implant pathogens. Int. J. Biol. Macromol. 2018, 108, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Boddupalli, B.M.; Mohammed, Z.N.K.; Nath, R.A.; Banji, D. Mucoadhesive drug delivery system: An overview. J. Adv. Pharm. Technol. Res. 2010, 1, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashri, L.Y.; Abou El Ela, A.F.; Ibrahim, M.A.; Alshora, D.H.; Naguib, M. Optimization and evaluation of chitosan buccal films containing tenoxicam for treating chronic periodontitis: In vitro and in vivo studies. J. Drug Deliv. Sci. Technol. 2020, 57, 101720. [Google Scholar] [CrossRef]
- Dias, R.J.; Havaldar, V.D.; Ghorpade, V.S.; Mali, K.K.; Gaikwad, V.K.; Kumbhar, D.M. Development and Evaluation of In-Situ Gel Containing Ornidazole Loaded Microspheres for Treatment of Periodontitis. J. Appl. Pharm. Sci. 2016, 6, 200–209. [Google Scholar] [CrossRef] [Green Version]
- Govender, S.; Pillay, V.; Chetty, D.J.; Essack, S.Y.; Dangor, C.M.; Govender, T. Optimisation and characterisation of bioadhesive controlled release tetracycline microspheres. Int. J. Pharm. 2005, 306, 24–40. [Google Scholar] [CrossRef]
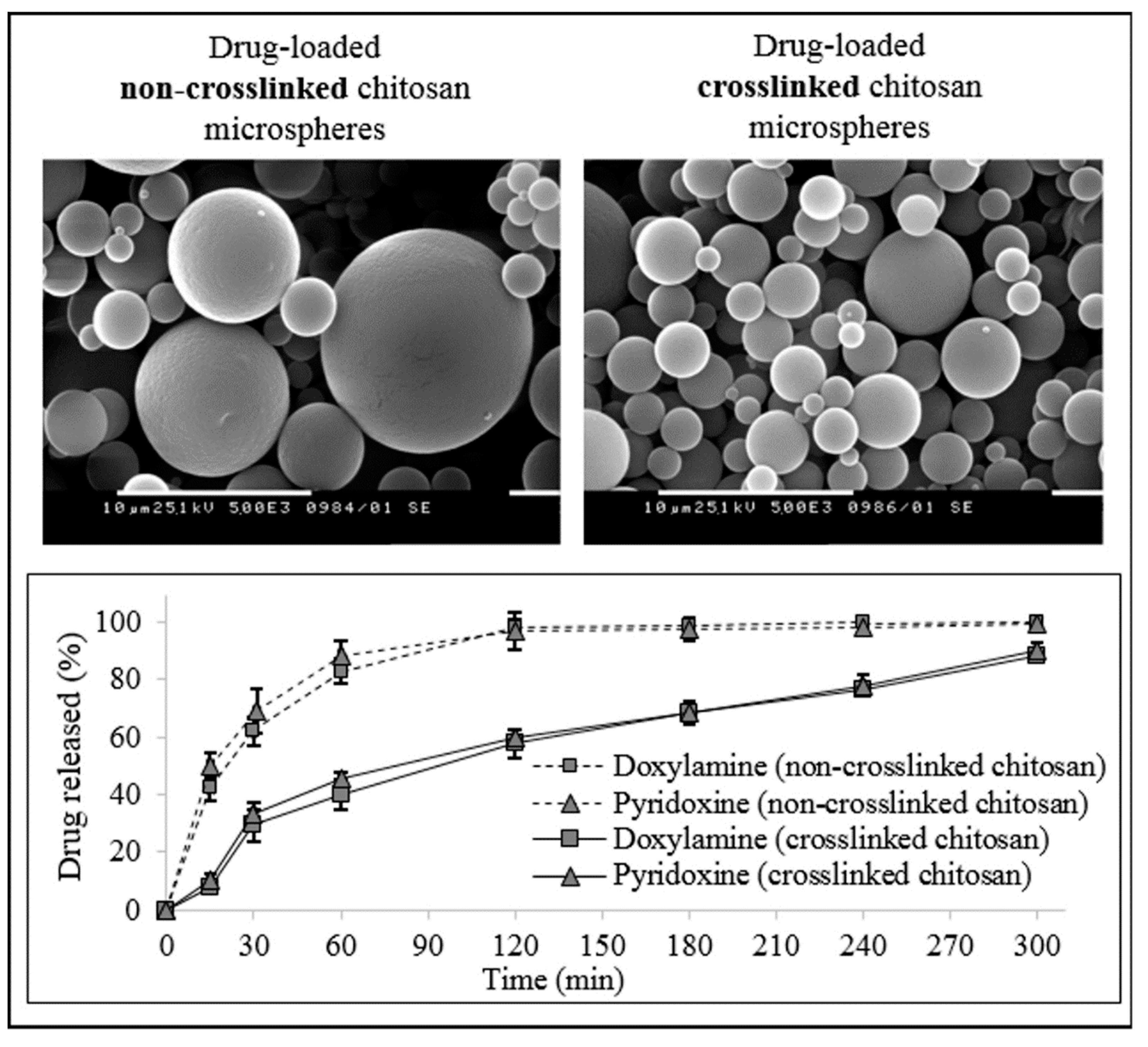
- Katsarov, P.; Pilicheva, B.; Uzunova, Y.; Gergov, G.; Kassarova, M. Chemical cross-linking: A feasible approach to prolong doxylamine/pyridoxine release from spray-dried chitosan microspheres. Eur. J. Pharm. Sci. 2018, 123, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Qian, J.; Zhao, C.; Yang, H.; Zhao, H.; Guo, H. Study on the relationship between crosslinking degree and properties of TPP crosslinked chitosan nanoparticles. Carbohydr. Polym. 2020, 241, 116349. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.; Reist, M.; Mayer, J.M.; Felt, O.; Peppas, N.A. Structure and interactions in covalently and ionically crosslinked chitosan hydrogels for biomedical applications. Eur. J. Pharm. Biopharm. 2004, 57, 19–34. [Google Scholar] [CrossRef]
- Zegan, G.; Anistoroaei, D.; Carausu, E.M.; Cernei, E.R.; Golovencu, L. Amoxicilin and Clavulanic Acid Intercaled Nanostructures for Dentistry Uses. Mater. Plast. 2019, 56, 396–398. [Google Scholar] [CrossRef]
- Shivashankar, M.; Mandal, B.K. Formulation and Evaluation of Bupivacaine-Loaded Glutaraldehyde-Crosslinked High Molecular Weight Chitosan Microspheres. Trop. J. Pharm. Res. 2013, 12, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, S.; Escudero, C.; Sediqi, N.; Smistad, G.; Hiorth, M. Fluoride loaded polymeric nanoparticles for dental delivery. Eur. J. Pharm. Sci. 2017, 15, 326–334. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimi, N.; Soleimani, A.; Rashidiani, J.; Malekafzali, B.; Abedini, F.; Hosseinkhani, H. Chitosan/Fluoride Nanoparticles for Preventing Dental Caries. Curr. Dent. 2019, 1, 61–67. [Google Scholar] [CrossRef]
- Keegan, G.M.; Smart, J.D.; Ingram, M.J.; Barnes, L.M.; Burnett, G.R.; Rees, G.D. Chitosan microparticles for the controlled delivery of fluoride. J. Dent. 2012, 40, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Targino, A.G.R.; Flores, M.A.P.; dos Santos Junior, V.E. An innovative approach to treating dental decay in children. A new anti-caries agent. J. Mater. Sci. Mater. Med. 2014, 25, 2041–2047. [Google Scholar] [CrossRef]
- Dos Santos, V.E.; Vasconcelos, F.A.; Targino, A.G.; Flores, M.A.; Galembeck, A.; Caldas, A.F.; Rosenblatt, A. A new “silver-bullet” to treat caries in children--nano silver fluoride: A randomised clinical trial. J. Dent. 2014, 42, 945–951. [Google Scholar] [CrossRef] [Green Version]
- Cook, W. Alginate dental impression materials: Chemistry, structure, and properties. J. Biomed. Mater. Res. 1986, 20, 1–24. [Google Scholar] [CrossRef]
- Punj, A.; Bompolaki, D.; Garaicoa, J. Dental Impression Materials and Techniques. Dent. Clin. N. Am. 2017, 61, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Manar, J. Alginate as impression material. Int. J. Appl. Dent. Sci. 2018, 4, 300–303. [Google Scholar]
- Baimark, Y.; Srisuwan, Y. Preparation of Polysaccharide-Based Microspheres by a Water-in-Oil Emulsion Solvent Diffusion Method for Drug Carriers. Int. J. Polym. Sci. 2013, 2013, 761870. [Google Scholar] [CrossRef] [Green Version]
- Scholz, M.; Reske, T.; Böhmer, F.; Hornung, A.; Grabow, N.; Lang, H. In vitro chlorhexidine release from alginate based microbeads for periodontal therapy. PLoS ONE 2017, 12, e0185562. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, A.L.; Espinar, F.O.; Méndez, J.B. The Application of Microencapsulation Techniques in the Treatment of Endodontic and Periodontal Diseases. Pharmaceutics 2011, 3, 538–571. [Google Scholar] [CrossRef]
- Park, Y.J.; Lee, J.Y.; Yeom, H.R.; Kim, K.H.; Lee, S.C.; Shim, I.K.; Chung, C.P.; Lee, S.J. Injectable polysaccharide microcapsules for prolonged release of minocycline for the treatment of periodontitis. Biotechnol. Lett. 2005, 27, 1761–1766. [Google Scholar] [CrossRef]
- Ferraz, M.P.; Mateus, A.Y.; Sousa, J.C.; Monteiro, F.J. Nanohydroxyapatite microspheres as delivery system for antibiotics: Release kinetics, antimicrobial activity, and interaction with osteoblasts. J. Biomed. Mater. Res. A 2007, 81, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Alipour, M.; Firouzi, N.; Aghazadeh, Z.; Samiei, M.; Montazersaheb, S.; Khoshfetrat, A.B.; Aghazadeh, M. The osteogenic differentiation of human dental pulp stem cells in alginate-gelatin/Nano-hydroxyapatite microcapsules. BMC Biotechnol. 2021, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- Gawkowska, D.; Cybulska, J.; Zdunek, A. Structure-Related Gelling of Pectins and Linking with Other Natural Compounds: A Review. Polymers 2018, 10, 762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez, S.; Rodríguez-Carvajal, M.A.; Doco, T. A complex plant cell wall polysaccharide: Rhamnogalacturonan II. A structure in quest of a function. Biochimie 2003, 85, 109–121. [Google Scholar] [CrossRef]
- Beyer, M.; Reichert, J.; Sigusch, B.W.; Watts, D.C.; Jandt, K.D. Morphology and structure of polymer layers protecting dental enamel against erosion. Dent. Mater. 2012, 28, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Hiorth, M.; Rykke, M.; Smistad, G. Polymer coated liposomes for dental drug delivery—Interactions with parotid saliva and dental enamel. Eur. J. Pharm. Sci. 2013, 50, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Esposito, E.; Cortesi, R.; Luca, G.; Nastruzzi, C. Pectin-based microspheres: A preformulatory study. Ann. N. Y. Acad. Sci. 2006, 944, 160–179. [Google Scholar] [CrossRef]
- Lascol, M.; Bourgeois, S.; Barratier, C.; Marote, P.; Lantéri, P.; Bordes, C. Development of pectin microparticles by using ionotropic gelation with chlorhexidine as cross-linking agent. Int. J. Pharm. 2018, 542, 205–212. [Google Scholar] [CrossRef]
- Pliszczak, D.; Bourgeois, S.; Bordes, C.; Valour, J.P.; Mazoyer, M.; Orecchioni, M.; Nakache, E.; Lantéri, P. Improvement of an encapsulation process for the preparation of pro- and prebiotics-loaded bioadhesive microparticles by using experimental design. Eur. J. Pharm. Sci. 2011, 44, 83–92. [Google Scholar] [CrossRef]
- Das, S.; Chaudhury, A.; Ng, K.Y. Preparation and evaluation of zinc-pectin-chitosan composite particles for drug delivery to the colon: Role of chitosan in modifying in vitro and in vivo drug release. Int. J. Pharm. 2011, 406, 11–20. [Google Scholar] [CrossRef]
- Jung, J.; Arnold, R.D.; Wicker, L. Pectin and charge modified pectin hydrogel beads as a colon-targeted drug delivery carrier. Colloids Surf. B Biointerfaces 2013, 104, 116–121. [Google Scholar] [CrossRef]
- Grant, G.T.; Morris, E.R.; Rees, D.A. Biological interactions between polysaccharides and divalent cations: The egg-box model. FEBS Lett. 1973, 32, 195–198. [Google Scholar] [CrossRef] [Green Version]
- Cao, L.; Lu, W.; Mata, A.; Nishinari, K.; Fang, Y. Egg-box model-based gelation of alginate and pectin: A review. Carbohydr. Polym. 2020, 242, 116389. [Google Scholar] [CrossRef] [PubMed]
- Klemetsrud, T.; Jonassen, H.; Hiorth, M.; Kjøniksen, A.L.; Smistad, G. Studies on pectin-coated liposomes and their interaction with mucin. Colloids Surf. B Biointerfaces 2013, 103, 158–165. [Google Scholar] [CrossRef]
- Sriamornsak, P.; Thirawong, N.; Nunthanid, J.; Puttipipatkhachorn, S.; Thongborisute, J.; Takeuchi, H. Atomic force microscopy imaging of novel self-assembling pectin–liposome nanocomplexes. Carbohydr. Polym. 2008, 71, 324–329. [Google Scholar] [CrossRef]
- Alund, S.J.; Smistad, G.; Hiorth, M. A multivariate analysis investigating different factors important for the interaction between liposomes and pectin. Colloids Surf. A Physicochem. Eng. Asp. 2013, 420, 1–9. [Google Scholar] [CrossRef]
- Dhaneshwar, S.S.; Kandpal, M.; Gairola, N.; Kadam, S.S. Dextran: A promising macromolecular drug carrier. Indian J. Pharm. Sci. 2006, 68, 705–714. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Ren, B.; Wang, L.; Li, M.; Liu, Y. Preparation and Evaluation of IL-1ra-Loaded Dextran/PLGA Microspheres for Inhibiting Periodontal Inflammation In Vitro. Inflammation 2020, 43, 168–178. [Google Scholar] [CrossRef]
- Chen, F.M.; Wu, Z.F.; Wang, Q.T.; Wu, H.; Zhang, Y.J.; Nie, X.; Jin, Y. Preparation of recombinant human bone morphogenetic protein-2 loaded dextran-based microspheres and their characteristics. Acta Pharmacol. Sin. 2005, 26, 1093–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.M.; Wu, Z.F.; Sun, H.H.; Wu, H.; Xin, S.N.; Wang, Q.T.; Dong, G.Y.; Ma, Z.W.; Huang, S.; Zhang, Y.J.; et al. Release of bioactive BMP from dextran-derived microspheres: A novel delivery concept. Int. J. Pharm. 2006, 307, 23–32. [Google Scholar] [CrossRef]
- Chen, F.M.; Zhao, Y.M.; Zhang, R.; Jin, T.; Sun, H.H.; Wu, Z.F.; Jin, Y. Periodontal regeneration using novel glycidyl methacrylated dextran (Dex-GMA)/gelatin scaffolds containing microspheres loaded with bone morphogenetic proteins. J. Control. Release 2007, 121, 81–90. [Google Scholar] [CrossRef]
- Park, S.-Y.; Kim, K.-H.; Kim, S.; Lee, Y.-M.; Seol, Y.-J. BMP-2 Gene Delivery-Based Bone Regeneration in Dentistry. Pharmaceutics 2019, 11, 393. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.M.; Zhao, Y.M.; Wu, H.; Deng, Z.H.; Wang, Q.T.; Zhou, W.; Liu, Q.; Dong, G.Y.; Li, K.; Wu, Z.F.; et al. Enhancement of periodontal tissue regeneration by locally controlled delivery of insulin-like growth factor-I from dextran-co-gelatin microspheres. J. Control. Release 2006, 114, 209–222. [Google Scholar] [CrossRef]
- Fujiwara, N.; Tabata, M.J.; Endoh, M.; Ishizeki, K.; Nawa, T. Insulin like growth factor-I stimulates cell proliferation in the outer layer of Hertwig’s epithelial root sheath and elongation of the tooth root in mouse molars in vitro. Cell Tissue Res. 2005, 320, 69–75. [Google Scholar] [CrossRef]
- Chen, F.M.; Ma, Z.W.; Dong, G.Y.; Wu, Z.F. Composite glycidyl methacrylated dextran (Dex-GMA)/gelatin nanoparticles for localized protein delivery. Acta Pharmacol. Sin. 2009, 30, 485–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, T.; Duan, Q.; Zhu, J.; Liu, H.; Yu, L. Starch-based biodegradable materials: Challenges and opportunities. Dir. Open Access J. 2020, 3, 8–18. [Google Scholar] [CrossRef]
- Rezapour, N.; Rasekh, B.; Mofradnia, S.R.; Yazdian, F.; Rashedi, H.; Tavakoli, Z. Molecular dynamics studies of polysaccharide carrier based on starch in dental cavities. Int. J. Biol. Macromol. 2019, 121, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Costa One, G.; Reis Albuquerque, A.; Cavalcante Souza, D.; Sampaio, F.C. Evaluation of potential antimicrobial chlorhexidine digluconate microencapsulated in model experimental dental biofilm. BMC Proc. 2014, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Queiroz, V.M.; Kling, I.C.S.; Eltom, A.E.; Archanjo, B.S.; Prado, M.; Simão, R.A. Corn starch films as a long-term drug delivery system for chlorhexidine gluconate. Mater. Sci. Eng. C 2020, 112, 110852. [Google Scholar] [CrossRef]
- Kassaee, M.Z.; Akhavan, A.; Sheikh, N.; Beteshobabrud, R. γ-Ray synthesis of starch-stabilized silver nanoparticles with antibacterial activities. Radiat. Phys. Chem. 2008, 77, 1074–1078. [Google Scholar] [CrossRef]
- Song, J.; Choi, B.; Jin, E.J.; Yoon, Y.; Choi, K.H. Curcumin suppresses Streptococcus mutans adherence to human tooth surfaces and extracellular matrix proteins. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1347–1352. [Google Scholar] [CrossRef]
- Lingström, P.; van Houte, J.; Kashket, S. Food starches and dental caries. Crit. Rev. Oral Biol. Med. 2000, 11, 366–380. [Google Scholar] [CrossRef]
- Goodson, J.M.; Holborow, D.; Dunn, R.L.; Hogan, P.; Dunham, S. Monolithic tetracycline-containing fibers for controlled delivery to periodontal pockets. J. Periodontol. 1983, 54, 575–579. [Google Scholar] [CrossRef]
- Barud, H.S.; Barrios, C.; Regiani, T.; Marques, R.F.; Verelst, M.; Dexpert-Ghys, J.; Messaddeq, Y.; Ribeiro, S.J. Self-supported silver nanoparticles containing bacterial cellulose membranes. Mater. Sci. Eng. C 2008, 28, 515–518. [Google Scholar] [CrossRef]
- Barud, H.S.; Regiani, T.; Marques, R.F.C.; Lustri, W.R.; Messaddeq, Y.; Ribeiro, S.J.L. Antimicrobial Bacterial Cellulose-Silver Nanoparticles Composite Membranes. J. Nanomater. 2011, 2011, 721631. [Google Scholar] [CrossRef] [Green Version]
- Maria, L.C.D.S.; Santos, A.L.; Oliveira, P.C.; Barud, H.S.; Messaddeq, Y.; Ribeiro, S.J. Synthesis and characterization of silver nanoparticles impregnated into bacterial cellulose. Mater. Lett. 2009, 63, 797–799. [Google Scholar] [CrossRef]
- Weyell, P.; Beekmann, U.; Küpper, C.; Dederichs, M.; Thamm, J.; Fischer, D.; Kralisch, D. Tailor-made material characteristics of bacterial cellulose for drug delivery applications in dentistry. Carbohydr. Polym. 2019, 207, 1–10. [Google Scholar] [CrossRef]
- Radwan, E.K.; Kafafy, H.; El-Wakeel, S.T.; Shaheen, T.I.; Gad-Allah, T.A.; El-Kalliny, A.S.; El-Naggar, M.E. Remediation of Cd(II) and reactive red 195 dye in wastewater by nanosized gels of grafted carboxymethyl cellulose. Cellulose 2018, 25, 6645–6660. [Google Scholar] [CrossRef]
- El-Newehy, M.H.; El-Naggar, M.E.; Alotaiby, S.; El-Hamshary, H.; Moydeen, M.; Al-Deyab, S. Green Electrospining of Hydroxypropyl Cellulose Nanofibres for Drug Delivery Applications. J. Nanosci. Nanotechnol. 2018, 18, 805–814. [Google Scholar] [CrossRef]
- De Oliveira Barud, H.G.; da Silva, R.R.; Borges, M.A.C.; Castro, G.R.; Ribeiro, S.J.L.; da Silva Barud, H. Bacterial Nanocellulose in Dentistry: Perspectives and Challenges. Molecules 2021, 26, 49. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef]
- Sahiner, N.; Suner, S.S.; Ayyala, R.S. Mesoporous, degradable hyaluronic acid microparticles for sustainable drug delivery application. Colloids Surf. B Biointerfaces 2019, 177, 284–293. [Google Scholar] [CrossRef]
- Huang, G.; Huang, H. Application of hyaluronic acid as carriers in drug delivery. Drug Deliv. 2018, 25, 766–772. [Google Scholar] [CrossRef]
- Morris, G.; Harding, S. Polysaccharides, microbial. In Encyclopedia of Microbiology, 3rd ed.; Schaechter, M., Ed.; Elsevier: Amsterdam, The Netherlands, 2009; pp. 482–494. [Google Scholar] [CrossRef]
- Mocanu, G.; Mihai, D.; Moscovici, M.; Picton, L.; LeCerf, D. Curdlan microspheres. Synthesis, characterization and interaction with proteins (enzymes, vaccines). Int. J. Biol. Macromol. 2009, 44, 215–221. [Google Scholar] [CrossRef]
- Han, J.; Cai, J.; Borjihan, W.; Ganbold, T.; Rana, T.M.; Baigude, H. Preparation of novel curdlan nanoparticles for intracellular siRNA delivery. Carbohydr. Polym. 2015, 117, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Wu, M.; Wang, C.; Wang, Z.; Chen, T.; Yan, J. Constructing biocompatible carboxylic curdlan-coated zein nanoparticles for curcumin encapsulation. Food Hydrocoll. 2020, 108, 106028. [Google Scholar] [CrossRef]
- Leung, T.C.; Wong, C.K.; Xie, Y. Green synthesis of silver nanoparticles using biopolymers, carboxymethylated-curdlan and fucoidan. Mater. Chem. Phys. 2010, 121, 402–405. [Google Scholar] [CrossRef]
- Needleman, I.G.; Smales, F.C. In vitro assessment of bioadhesion for periodontal and buccal drug delivery. Biomaterials 1995, 16, 617–624. [Google Scholar] [CrossRef]
- Kim, J.; Hwang, J.; Kang, H.; Choi, J. Chlorhexidine-loaded xanthan gum-based biopolymers for targeted, sustained release of antiseptic agent. J. Ind. Eng. Chem. 2015, 32, 44–48. [Google Scholar] [CrossRef]
- Eftaiha, A.F.; Qinna, N.; Rashid, I.S.; Al Remawi, M.M.; Al Shami, M.R.; Arafat, T.A.; Badwan, A.A. Bioadhesive Controlled Metronidazole Release Matrix Based on Chitosan and Xanthan Gum. Mar. Drugs 2010, 8, 1716–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrigy, N.B.; Ordoubadi, M.; Liu, Y.; Melhem, O.; Barona, D.; Wang, H.; Milburn, L.; Ruzycki, C.A.; Finlay, W.H.; Vehring, R. Amorphous pullulan trehalose microparticle platform for respiratory delivery. Int. J. Pharm. 2019, 563, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.D.; Akbuğa, J. Fucosphere—New microsphere carriers for peptide and protein delivery: Preparation and in vitro characterization. J. Microencapsul. 2006, 23, 513–522. [Google Scholar] [CrossRef]
- Toumba, K.J.; Twetman, S.; Splieth, C.; Parnell, C.; van Loveren, C.; Lygidakis, N.A. Guidelines on the use of fluoride for caries prevention in children: An updated EAPD policy document. Eur. Arch. Paediatr. Dent. 2019, 20, 507–516. [Google Scholar] [CrossRef] [Green Version]
- Kanduti, D.; Sterbenk, P.; Artnik, B. Fluoride: A review of use and effects on health. Mater. Socio-Med. 2016, 28, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Ijaz, S.; Marinho, V.; Croucher, R.; Onwude, O.; Rutterford, C. Professionally applied fluoride paint-on solutions for the control of dental caries in children and adolescents. CDSR 2018, 5, CD008364. [Google Scholar] [CrossRef]
- Priyadarsini, S.; Mukherjee, S.; Mishra, M. Nanoparticles used in dentistry: A review. J. Oral Biol. Craniofac. Res. 2018, 8, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Date, A.A.; Hanes, J.; Ensign, L.M. Nanoparticles for oral delivery: Design, evaluation and state-of-the-art. J. Control Release 2016, 240, 504–526. [Google Scholar] [CrossRef] [Green Version]
- Bottenberg, P.; Bultmann, C.; Gräber, H.G. Distribution of fluoride in the oral cavity after application of a bioadhesive fluoride-releasing tablet. J. Dent. Res. 1998, 77, 68–72. [Google Scholar] [CrossRef]
- Owens, T.S.; Danserau, R.; Sakr, A. Development and evaluation of extended release bioadhesive sodium fluoride tablets. Int. J. Pharm. 2005, 288, 109–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Francisco, L.M.; Cerquetani, J.A.; Bruschi, M.L. Development and characterization of gelatin and ethylcellulose microparticles designed as platforms to delivery fluoride. Drug Dev. Ind. Pharm. 2013, 39, 1644–1650. [Google Scholar] [CrossRef]
- Freire, P.; Albuquerque, A.; Sampaio, F.; Galembeck, A.; Flores, M.; Stamford, T.; Rosenblatt, A. AgNPs: The New Allies Against, S. Mutans Biofilm—A Pilot Clinical Trial and Microbiological Assay. Braz. Dent. J. 2017, 28, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Li, Y.; Sun, X.; Kishen, A.; Deng, X.; Yang, X.; Wang, H.; Cong, C.; Wang, Y.; Wu, M. Biomimetic remineralization of demineralized enamel with nano-complexes of phosphorylated chitosan and amorphous calcium phosphate. J. Mater. Sci. Mater. Med. 2014, 25, 2619–2628. [Google Scholar] [CrossRef] [PubMed]
- Leonor, I.B.; Balas, F.; Kawashita, M.; Reis, R.L.; Kokubo, T.; Nakamura, T. Biomimetic apatite deposition on polymeric microspheres treated with a calcium silicate solution. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91B, 239–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruan, Q.; Moradian-Oldak, J. Development of amelogenin-chitosan hydrogel for in vitro enamel regrowth with a dense interface. J. Vis. Exp. 2014, 89, 51606. [Google Scholar] [CrossRef] [PubMed]
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral Biofilms: Pathogens, Matrix, and Polymicrobial Interactions in Microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef]
- Tao, D.; Li, F.; Feng, X.; Wong, M.; Lu, H. Plaque biofilm microbial diversity in infants aged 12 months and their mothers with or without dental caries: A pilot study. BMC Oral Health 2018, 18, 228. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Bhatia, S.; Sodhi, A.S.; Batra, N. Oral microbiome and health. AIMS Microbiol. 2018, 4, 42–66. [Google Scholar] [CrossRef] [PubMed]
- Benoit, D.S.W.; Sims, K.R.; Fraser, D. Nanoparticles for Oral Biofilm Treatments. ACS Nano 2019, 13, 4869–4875. [Google Scholar] [CrossRef] [PubMed]
- Naha, P.C.; Liu, Y.; Hwang, G.; Huang, Y.; Gubara, S.; Jonnakuti, V.; Simon-Soro, A.; Kim, D.; Gao, L.; Koo, H.; et al. Dextran-Coated Iron Oxide Nanoparticles as Biomimetic Catalysts for Localized and pH-Activated Biofilm Disruption. ACS Nano 2019, 13, 4960–4971. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.V.; Silveira, F.F.; Nunes, E. Apexification in non-vital teeth with immature roots: Report of two cases. Iran. Endod. J. 2015, 10, 79–81. [Google Scholar] [PubMed]
- Strom, T.A.; Arora, A.; Osborn, B.; Karim, N.; Komabayashi, T.; Liu, X. Endodontic release system for apexification with calcium hydroxide microspheres. J. Dent. Res. 2012, 91, 1055–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Ghutaimel, H.; Riba, H.; Al-Kahtani, S.; Al-Duhaimi, S. Common periodontal diseases of children and adolescents. Int. Dent. J. 2014, 2014, 850674. [Google Scholar] [CrossRef] [PubMed]
- Pari, A.; Ilango, P.; Subbareddy, V.; Katamreddy, V.; Parthasarthy, H. Gingival diseases in childhood—A review. J. Clin. Diagn. Res. 2014, 8, ZE01–ZE04. [Google Scholar] [CrossRef]
- Drummond, B.K.; Brosnan, M.G.; Leichter, J.W. Management of periodontal health in children: Pediatric dentistry and periodontology interface. Periodontol. 2000 2017, 74, 158–167. [Google Scholar] [CrossRef]
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [Green Version]
- Cekici, A.; Kantarci, A.; Hasturk, H.; van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol. 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Cai, X.; Ou, Y.; Zhou, Y.; Wang, Y. Resolution of inflammation in periodontitis: A review. Int. J. Clin. Exp. Pathol. 2018, 11, 4283–4295. [Google Scholar]
- Prud’homme, T.; Roy, E.; Soueidan, A.; Fouassier, M.; Dajean-Trutaud, S.; Badran, Z. Multidisciplinary Clinical Management of a Localized Aggressive Periodontitis diagnosed in a Child with Glanzmann’s Thrombasthenia. Int. J. Clin. Pediatr. Dent. 2018, 11, 344–348. [Google Scholar] [CrossRef]
- Miller, K.; Treloar, T.; Guelmann, M.; Rody, W.J.; Shaddox, L.M. Clinical Characteristics of Localized Aggressive Periodontitis in Primary Dentition. J. Clin. Pediatr. Dent. 2018, 42, 95–102. [Google Scholar] [CrossRef]
- Shaddox, L.M.; Huang, H.; Lin, T.; Hou, W.; Harrison, P.L.; Aukhil, I.; Walker, C.B.; Klepac-Ceraj, V.; Paster, B.J. Microbiological characterization in children with aggressive periodontitis. J. Dent. Res. 2012, 91, 927–933. [Google Scholar] [CrossRef] [Green Version]
- Tokajuk, G.; Niemirowicz, K.; Deptula, P.; Piktel, E.; Ciesluk, M.; Wileczewska, A.Z.; Dabrowski, J.R.; Bucki, R. Use of magneticnanoparticles as a drug delivery system to improve chlorhexidine antimicrobial activity. Int. J. Nanomed. 2017, 12, 7833–7846. [Google Scholar] [CrossRef] [Green Version]
- Vasiliu, S.; Racovita, S.; Gugoasa, I.A.; Lungan, M.A.; Popa, M.; Desbrieres, J. The Benefits of Smart Nanoparticles in Dental Applications. Int. J. Mol. Sci. 2021, 22, 2585. [Google Scholar] [CrossRef]
- Brookes, Z.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current uses of chlorhexidine for management of oral disease: A narrative review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef]
- Cappelli, D.; Holt, S.C.; Singer, R.E.; Pickrum, H.M.; Ebersole, J.L. Effects of 0.12% chlorhexidine gluconate on experimental gingivitis in non-human primates: Clinical and microbiological alterations. Oral Dis. 2000, 6, 124–131. [Google Scholar] [CrossRef]
- Azimi, M.; Jouybari, L.; Moghadam, S.; Ghaemi, E.; Behnampoor, N.; Sanagoo, A.; Hesam, M. Antimicrobial effects of chlorhexidine, matrica drop mouthwash (chamomile extract), and normal saline on hospitalized patients with endotracheal tubes. Iran. J. Nurs. Midwifery Res. 2016, 21, 458–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovtun, A.; Kozlova, D.; Ganesan, K.; Biewald, C.; Seipold, N.; Gaengler, P.; Arnold, W.H.; Epple, M. Chlorhexidine-loadedcalcium phosphate nanoparticles for dental maintenance treatment combination of mineralizing and antibacterial effect. RCS Adv. 2012, 2, 870–875. [Google Scholar] [CrossRef]
- Prakasam, A.; Elavarasu, S.S.; Natarajan, R.K. Antibiotics in the management of aggressive periodontitis. J. Pharm. Bioallied. Sci. 2012, 4, S252–S255. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Malhotra, R.; Grover, V.; Grover, D. Systemic antibiotic therapy in periodontics. J. Dent. Res. 2012, 9, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Nadig, P.S.; Shah, M.A. Tetracycline as local drug delivery in treatment of chronic periodontitis: A systematic review and meta-analysis. J. Indian Soc. Periodontol. 2016, 20, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Roshna, T.; Nandakumar, K. Generalized aggressive periodontitis and its treatment options: Case reports and review of the literature. J. Med. Case Rep. 2012, 2012, 535321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Zhou, Q.; Jiang, Z.; Wang, Y.; Yang, K.; Qiu, X.; Ji, Q. The effect of doxycycline-containing chitosan/carboxymethyl chitosan nanoparticles on NLRP3 inflammasome in periodontal disease. Carbohydr. Polym. 2020, 237, 116163. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Polymer Microstructures | Polymer Nanostructures |
|---|---|---|
| Size range | 1–1000 µm | 1–1000 nm |
| Preparation methods | Spray-drying Solvent evaporation Ionic gelation Emulsion solvent evaporation Solvent extraction Complex coacervation Polymerization | Nano spray-drying Solvent evaporation Ionic gelation Solvent diffusion Nanoprecipitation Reverse salting-out Polymerization |
| Types of polymer structures | Microspheres Microcapsules Microbeads Microfilms Microneedles Microchips Microsponges | Nanospheres Nanocapsules Nanogels Nanofibers Nanotubes Micelles Polymersomes |
| Advantages as drug carriers | Targeted drug delivery Sustained drug release Multiple unit drug delivery Increased drug loading High drug encapsulation efficiency | Targeted drug delivery Sustained drug release Enhanced drug solubility Improved bioavailability Increased cellular uptake Variable administration routes |
| Active Substance | Production Method | Particle Diameter | Entrapment Efficiency | Application | Ref. |
|---|---|---|---|---|---|
| Amoxicillin Clavulanic acid | Ionic gelation | 45–270 nm | NA* | Bacterial plaque | [52] |
| Bupivacaine | Emulsion technique | NA* | 83% | Dental pain | [53] |
| Ketoprofen | Spray drying | 2–3 µm | 54–62% | Periodontitis | [30] |
| Metronidazole | Emulsion technique | 43 μm | 59% | Periodontitis | [26] |
| Metronidazole | External gelation | 800 µm | 60–75% | Periodontitis | [25] |
| Miconazole | Complex coacervation | 1000 μm | 49–67% | Oral candidiasis | [31] |
| Nal-P-113 peptide | Polymerization | 216.20 nm | 89% | Root caries restoration; periodontitis | [32] |
| Ornidazole | Emulsion- ionotropic gelation | 29–53 µm | 11–32% | Periodontitis | [47] |
| Sodium fluoride | Ionic gelation | 100 nm | 4–6% | Caries prevention | [54] |
| Sodium fluoride | Ionic gelation | 219 nm | 30% | Caries prevention | [55] |
| Sodium fluoride | Spray drying | 3–6 µm | 74–84% | Caries prevention | [56] |
| Silver fluoride | Reduction of silver nitrate | 6 nm | NA * | Caries prevention | [57] |
| Silver sodium fluoride | Reduction of silver nitrate | 3–4 nm | NA * | Caries prevention | [58] |
| Tetracycline | Gelation technique | 1400–1700 μm | NA * | Periodontitis | [48] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsarov, P.; Shindova, M.; Lukova, P.; Belcheva, A.; Delattre, C.; Pilicheva, B. Polysaccharide-Based Micro- and Nanosized Drug Delivery Systems for Potential Application in the Pediatric Dentistry. Polymers 2021, 13, 3342. https://0-doi-org.brum.beds.ac.uk/10.3390/polym13193342
Katsarov P, Shindova M, Lukova P, Belcheva A, Delattre C, Pilicheva B. Polysaccharide-Based Micro- and Nanosized Drug Delivery Systems for Potential Application in the Pediatric Dentistry. Polymers. 2021; 13(19):3342. https://0-doi-org.brum.beds.ac.uk/10.3390/polym13193342
Chicago/Turabian StyleKatsarov, Plamen, Maria Shindova, Paolina Lukova, Ani Belcheva, Cédric Delattre, and Bissera Pilicheva. 2021. "Polysaccharide-Based Micro- and Nanosized Drug Delivery Systems for Potential Application in the Pediatric Dentistry" Polymers 13, no. 19: 3342. https://0-doi-org.brum.beds.ac.uk/10.3390/polym13193342