
A Compressed Sensing-Based Wearable Sensor Network for Quantitative Assessment of Stroke Patients


Abstract
:1. Introduction
2. Materials and Methods
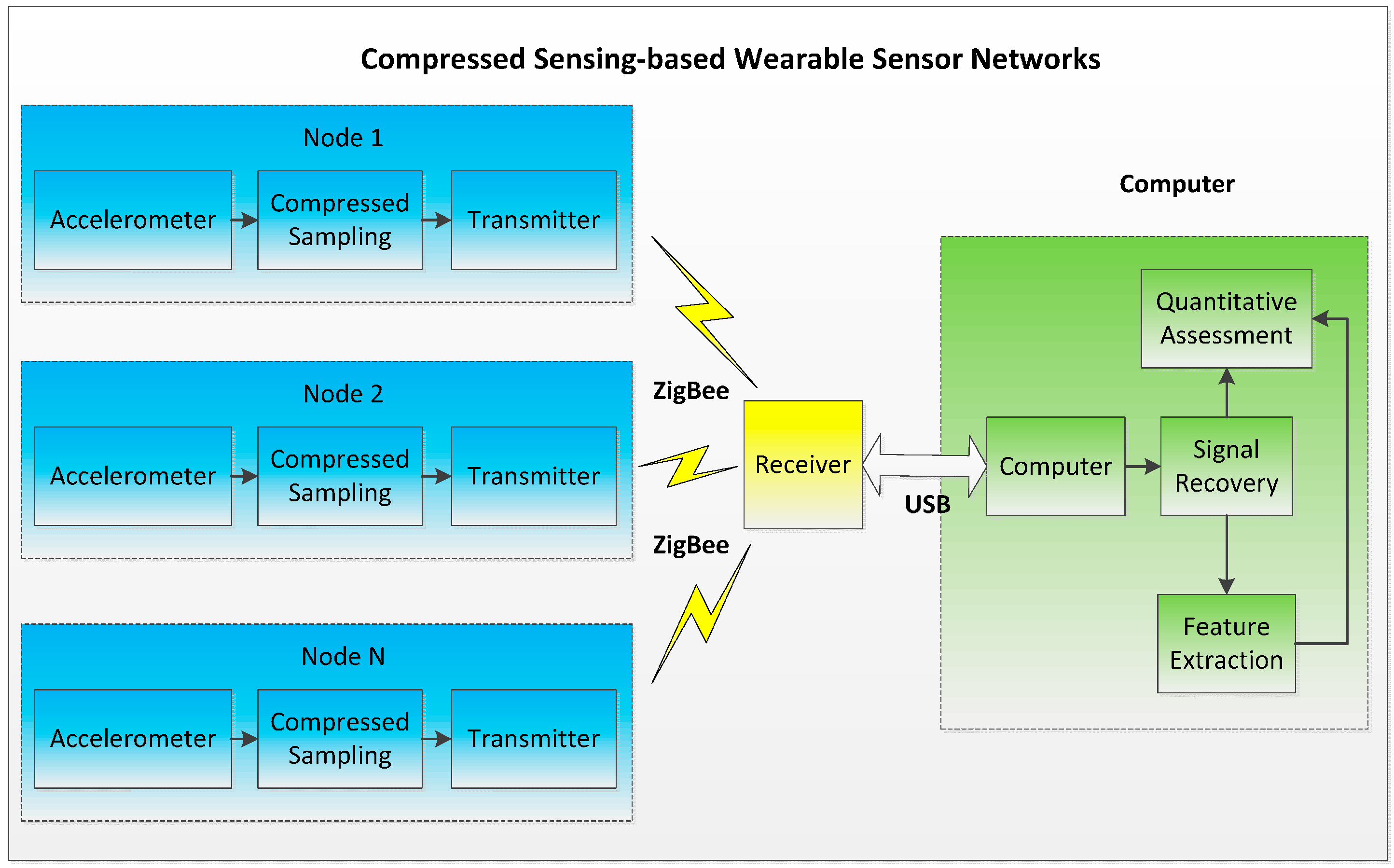
2.1. Compressed Sensing-Based Wearable Sensor Network

2.2. Signal Recovery Algorithms
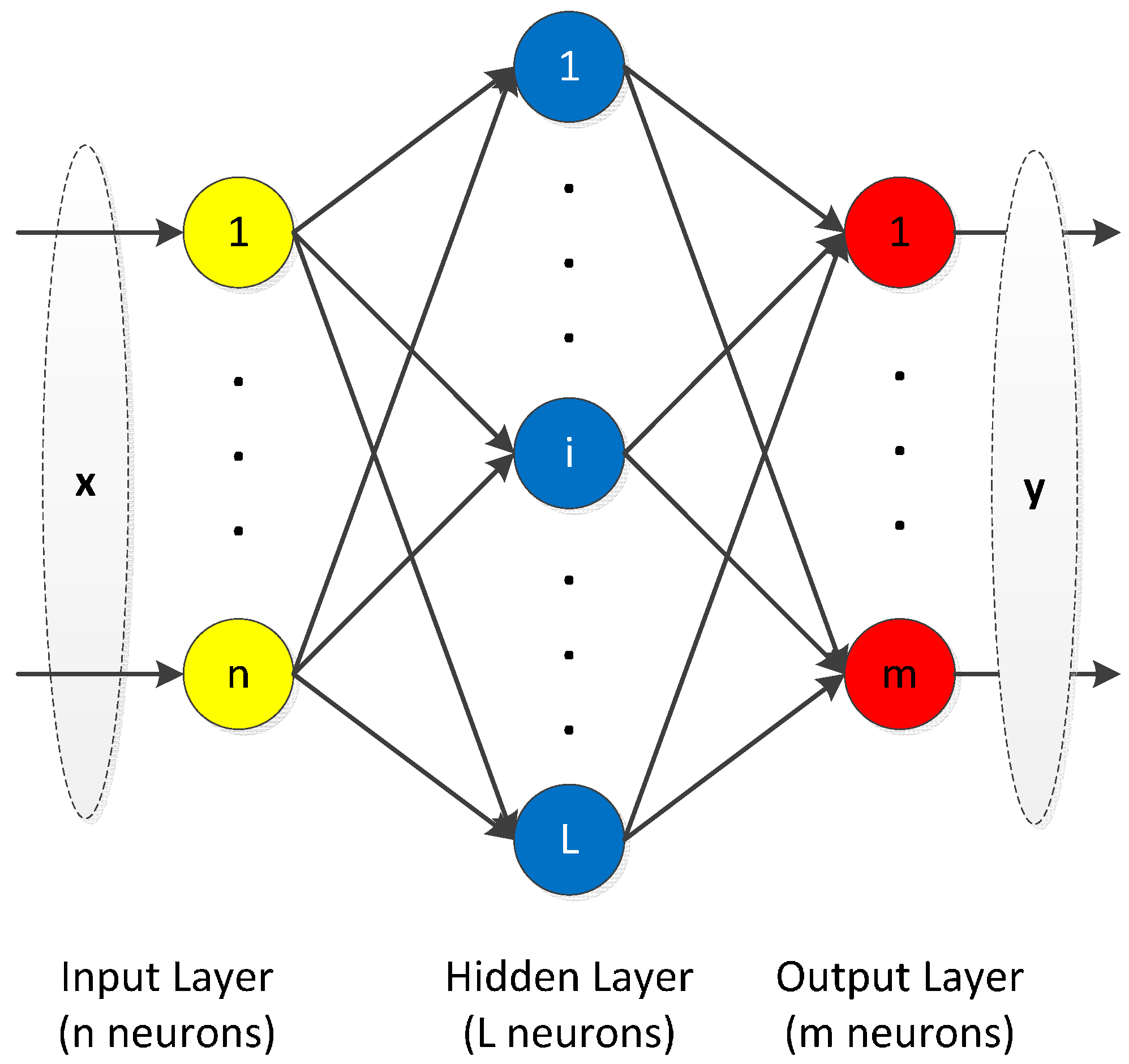
2.3. Extreme Learning Machine


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Step 1: Generate random input weight and bias , . |
| Step 2: Compute the output of neurons in hidden layer according to Equation (6). |
| Step 3: Compute the output weight according to Equation (8). |
2.4. Experiment Protocols
| Brunnstrom Stage Level | Patients | Sex (M/F) | Hemiplegic Side (Left/Right) | Limb Dominance (Left/Right) |
|---|---|---|---|---|
| II | 2 | 0/2 | 2/0 | 0/2 |
| III | 10 | 5/5 | 6/4 | 2/8 |
| IV | 4 | 3/1 | 3/1 | 0/4 |
| V | 7 | 5/2 | 2/5 | 1/6 |

2.4.1. Bobath Handshake
- (1)
- Sit down on a chair, cross the hand and keep the thumb of the hemiplegic side on top.
- (2)
- Straighten the upper extremities, lift above the head and hold for 3 s.
- (3)
- Move the hands back to the initial position.
2.4.2. Shoulder Touch
- (1)
- Sit down on a chair, and naturally droop the upper limb of the hemiplegic side.
- (2)
- Raise the upper limb of the hemiplegic side to the horizontal position.
- (3)
- Move horizontally to the healthy side shoulder and hold for 5 s.
- (4)
- Move back to the initial droop position and take a short break.
3. Results and Discussion
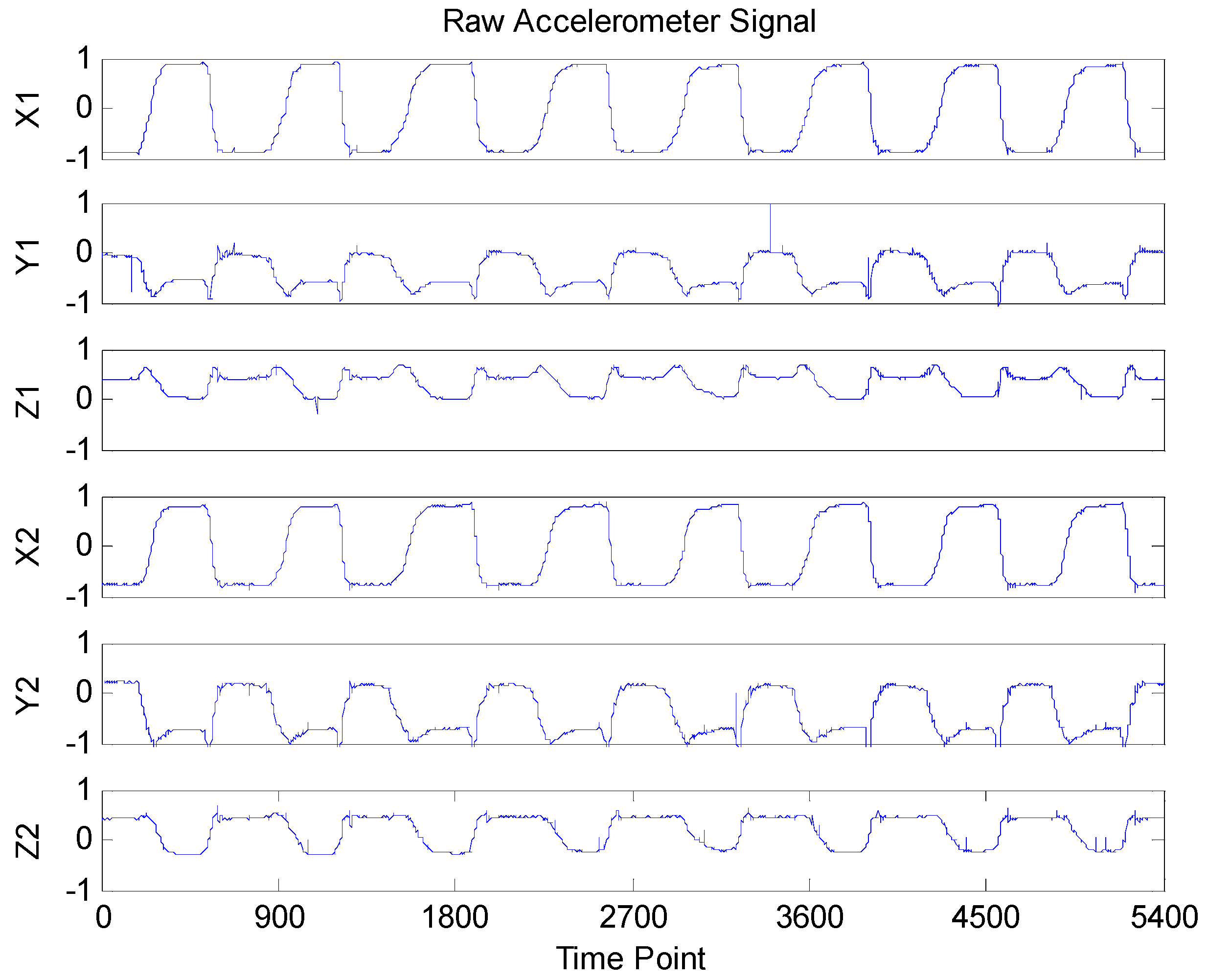
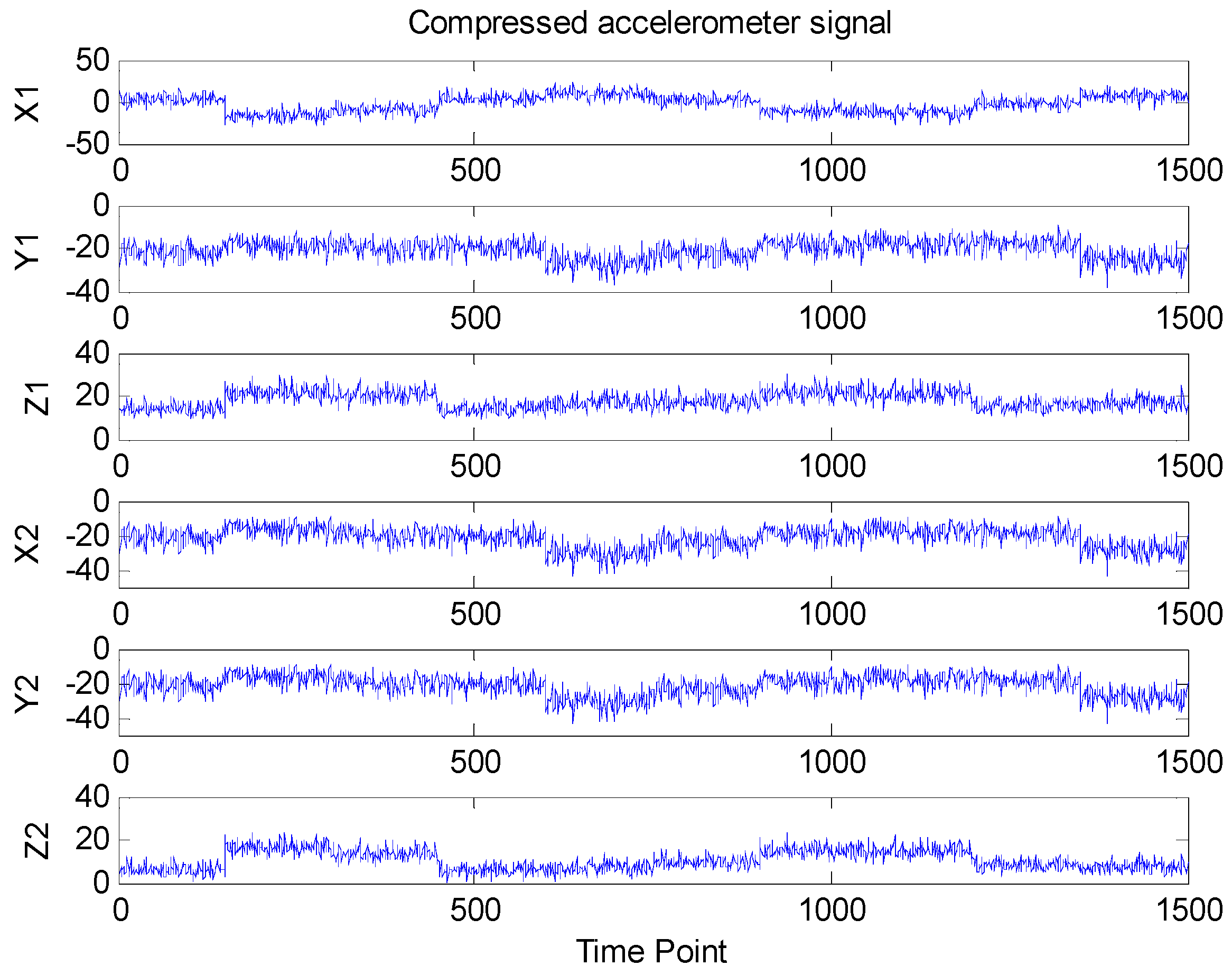
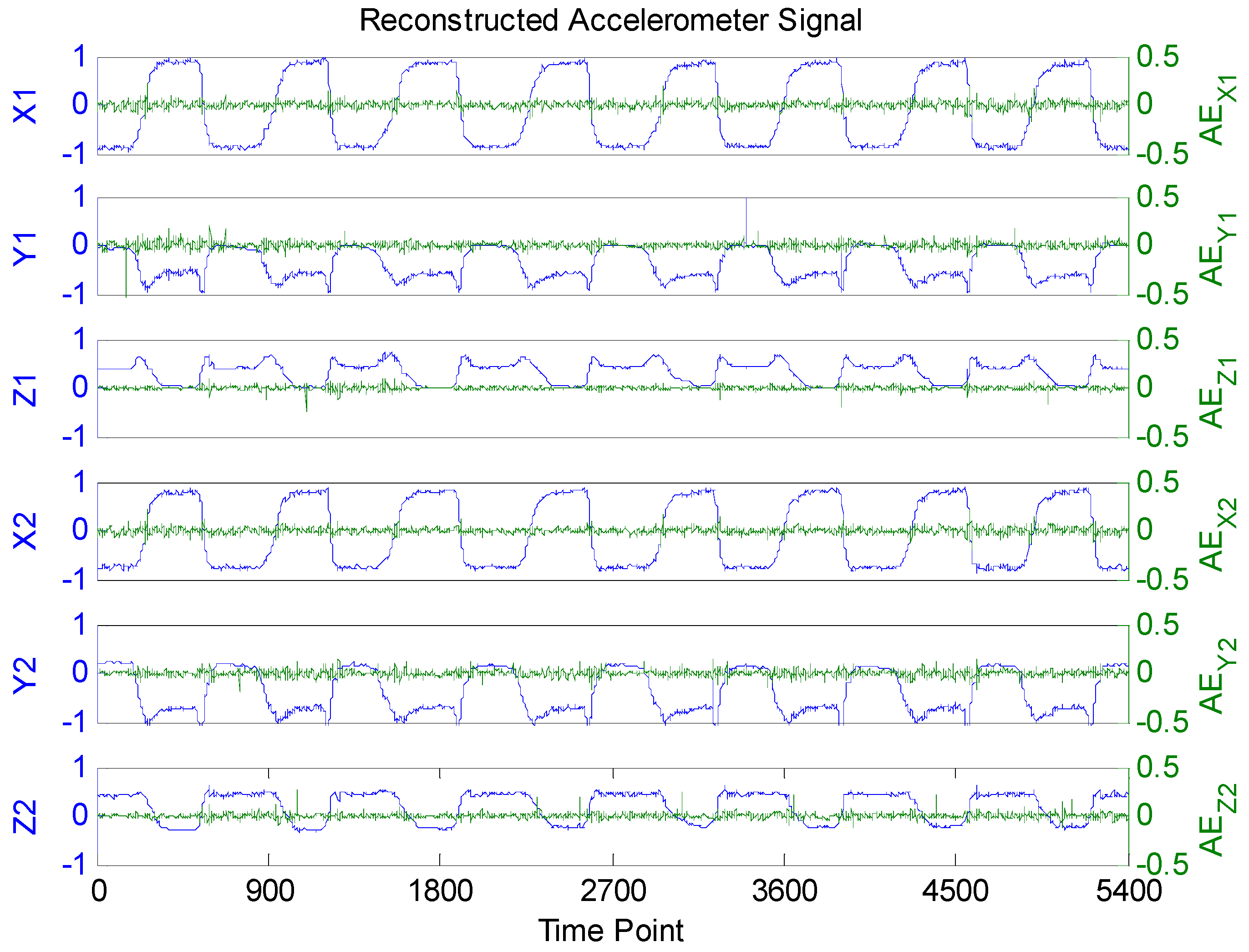
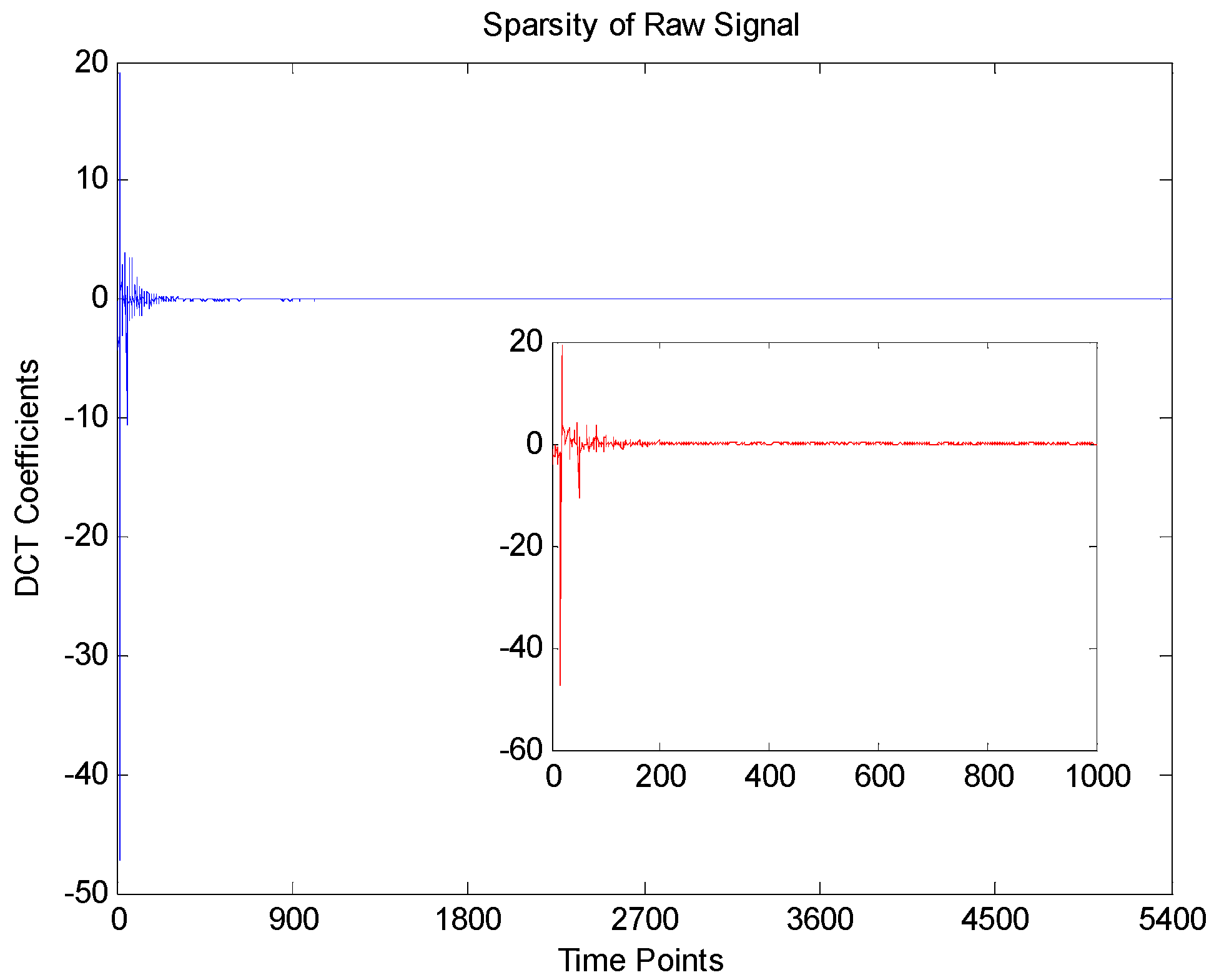
3.1. Accelerometer Signals Compress and Recovery



| Methods | Correlation Coefficients between Reconstructed and Raw Signals | |||||
|---|---|---|---|---|---|---|
| X1 | Y1 | Z1 | X2 | Y2 | Z2 | |
| BSBL | 0.9991 | 0.9957 | 0.9965 | 0.9991 | 0.9979 | 0.9969 |
| BP | 0.8762 | 0.8814 | 0.8729 | 0.8651 | 0.8964 | 0.9015 |
| OMP | 0.9356 | 0.9521 | 0.9188 | 0.9672 | 0.9248 | 0.9366 |
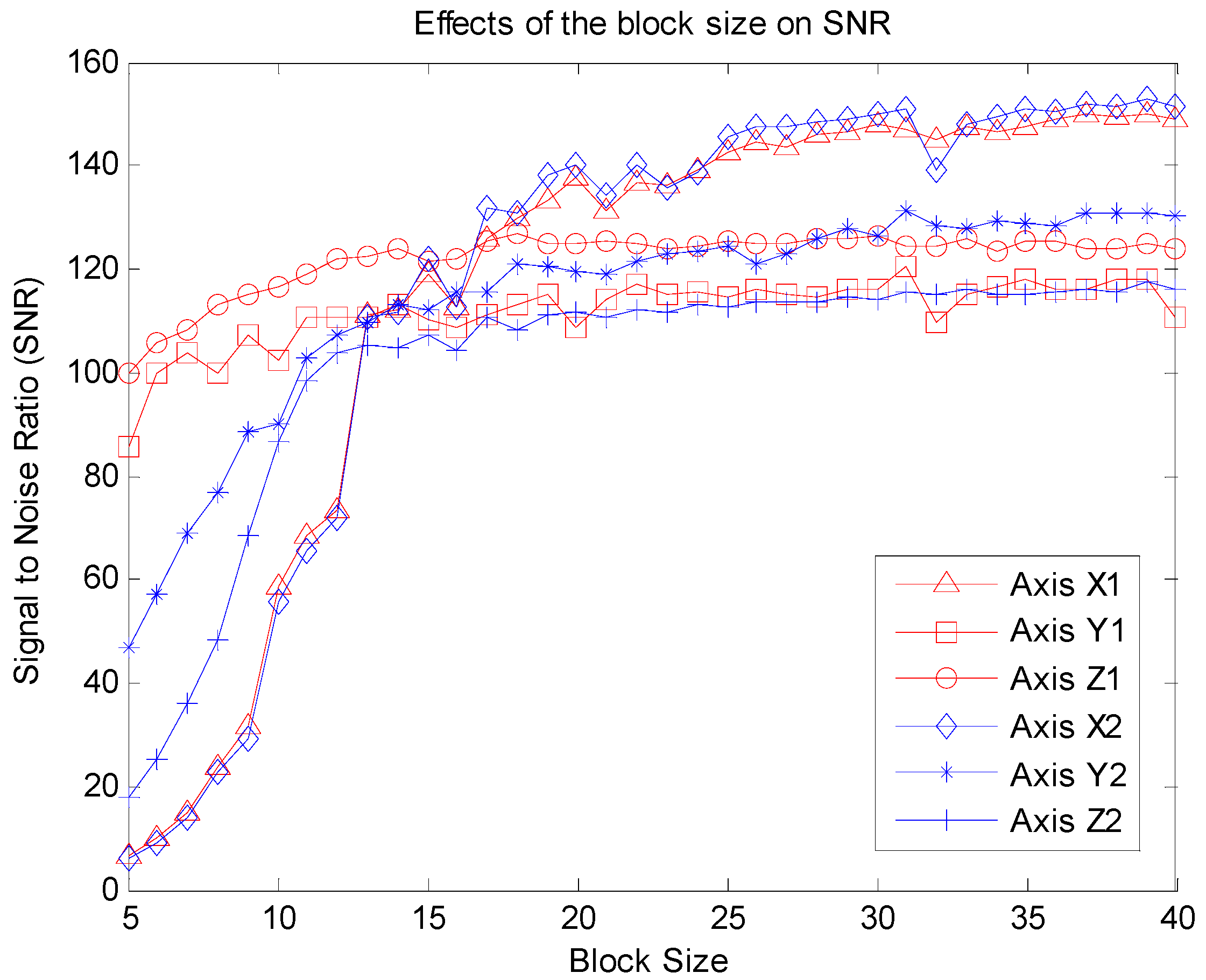
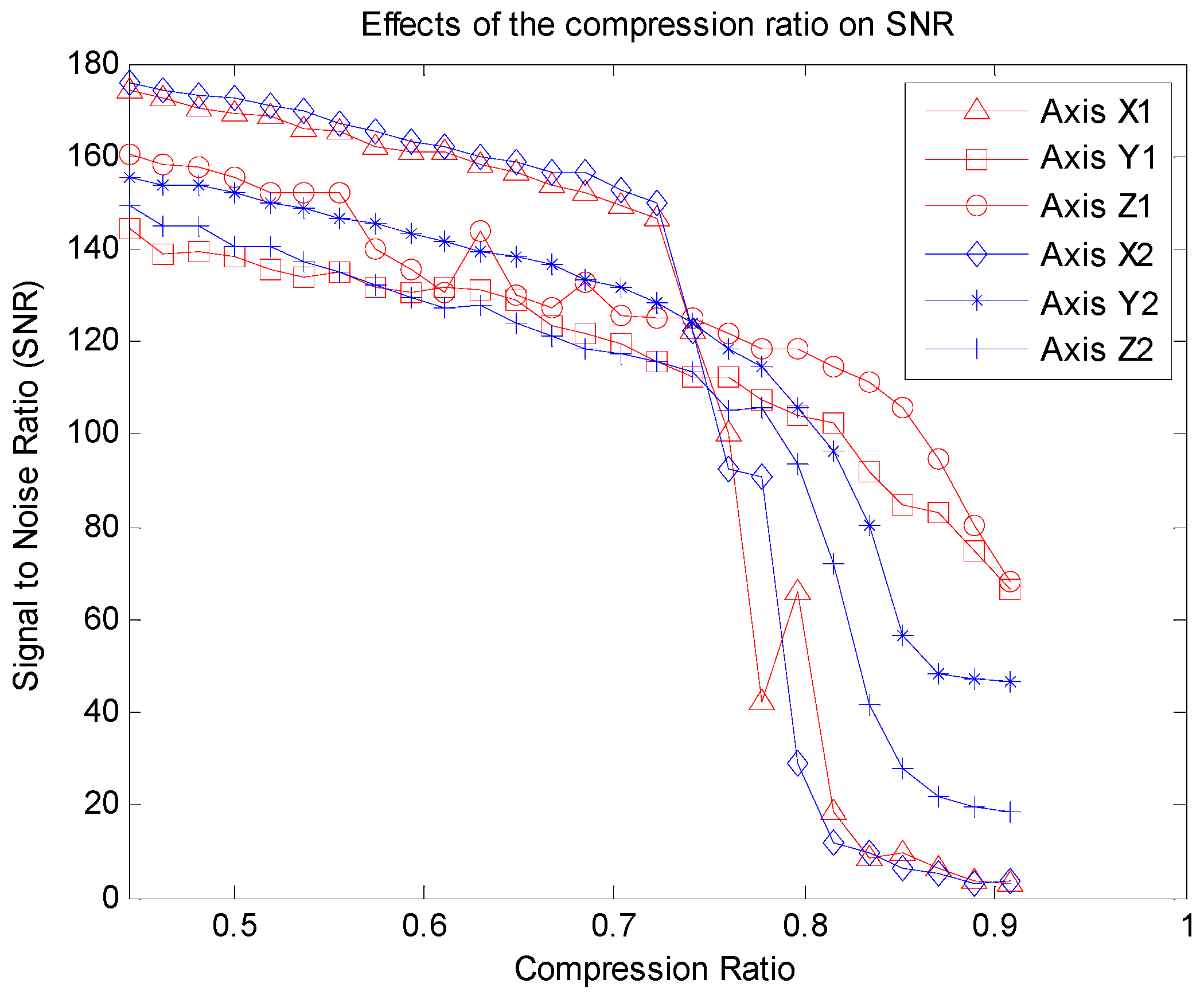
3.2. Effects of Block Size and CR on Recovery Performance



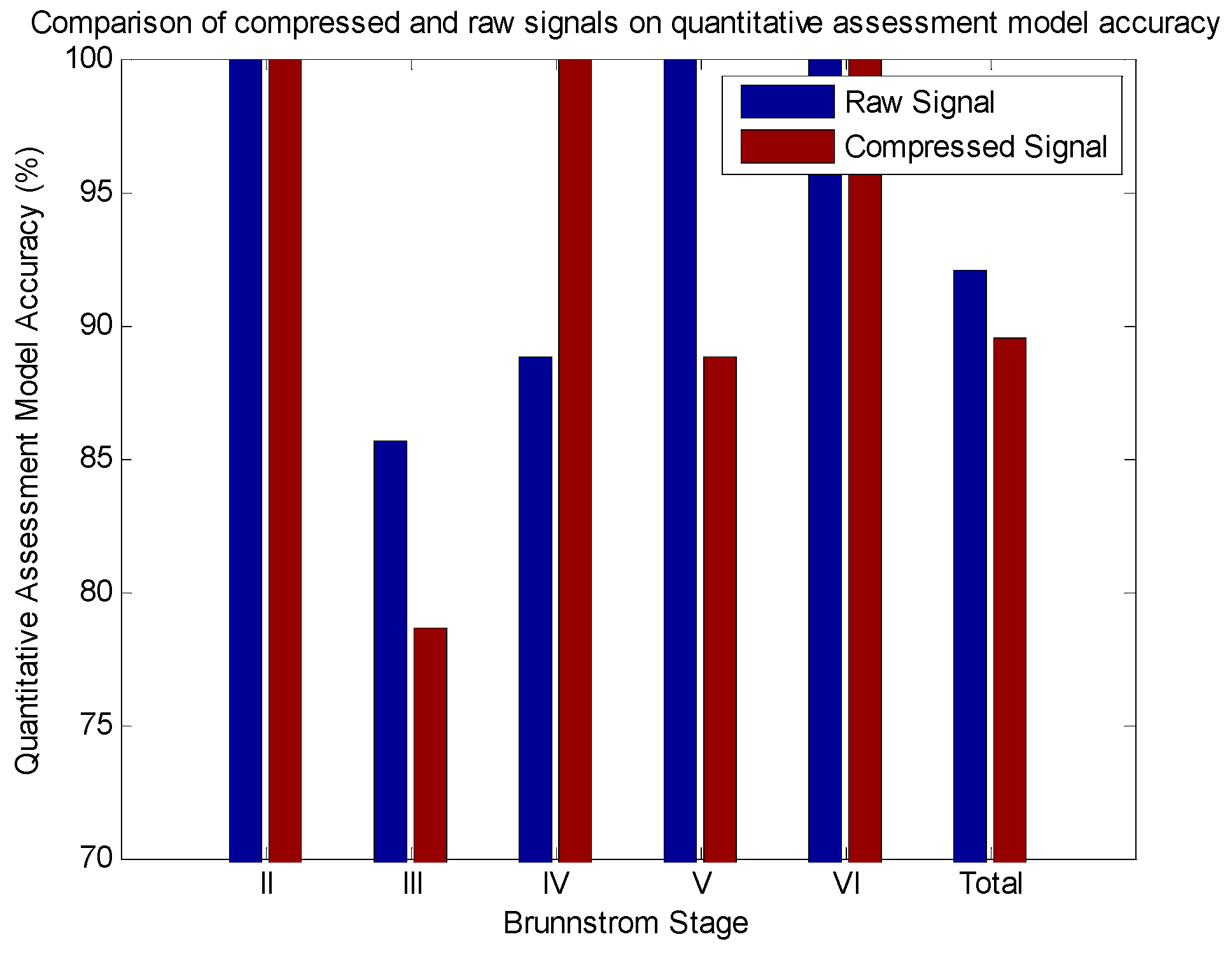
3.3. Effects of Compressed Sensing on Quantitative Assessment Model


| Brunnstrom Stage | Samples in Testing Set | Predictive Accuracy | |
|---|---|---|---|
| Raw Model | Compressed Sensing Model | ||
| II | 2 | 100 (2/2) | 100 (2/2) |
| III | 14 | 85.7 (12/14) | 78.6 (11/14) |
| IV | 9 | 88.8 (8/9) | 100 (9/9) |
| V | 9 | 100 (9/9) | 88.8 (8/9) |
| VI | 4 | 100 (4/4) | 100 (4/4) |
| Total | 38 | 92.1 (35/38) | 89.5 (34/38) |
| Source | Sum of Squares | df | Mean Square | F | Prob > F |
|---|---|---|---|---|---|
| Between Groups | 0.0132 | 1 | 0.01316 | 0.01 | 0.9205 |
| Within Groups | 96.9737 | 74 | 1.31046 | ||
| Total | 96.9868 | 75 |
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CS | Compressed Sensing |
| WSN | Wearable Sensor Network |
| UE | Upper Extremity |
| WMFT | Wolf Motor Function Test |
| FAS | Functional Ability Scale |
| RIP | Restricted Isometry Property |
| MP | Matching Pursuit |
| OMP | Orthogonal Matching Pursuit |
| BP | Basis Pursuit |
| SBL | Sparse Bayesian Learning |
| BSBL | Block Sparse Bayesian Learning |
| CR | Compression Ratio |
| SNR | Signal to Noise Ratio |
| ELM | Extreme Learning Machine |
| DCT | Discrete Cosine Transform |
| RRTAS | Remote Rehabilitation Training and Assessment Software |
Appendix
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. The Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Ozgoren, A.A.; Abdalla, S.; Abd-Allah, F.; et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. The Lancet 2015, 385, 117–171. [Google Scholar]
- Liu, L.; Wang, D.; Wong, K.L.; Wang, Y. Stroke and stroke care in China huge burden, significant workload, and a national priority. Stroke 2011, 42, 3651–3654. [Google Scholar] [CrossRef] [PubMed]
- Langan, J.; DeLave, K.; Phillips, L.; Pangilinan, P.; Brown, S.H. Home-based telerehabilitation shows improved upper limb function in adults with chronic stroke: A pilot study. J. Rehabil. Med. 2013, 45, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Jin, W.; Zhang, X.X.; Xu, W.; Liu, X.N.; Ren, C.C. Telerehabilitation Approaches for Stroke Patients: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Stroke Cerebrovasc.Dis. 2015, 24, 2660–2668. [Google Scholar] [CrossRef] [PubMed]
- Hadjidj, A.; Souil, M.; Bouabdallah, A.; Challal, Y.; Owen, H. Wireless sensor networks for rehabilitation applications: Challenges and opportunities. J. Netw. Comput. Appl. 2013, 36, 1–15. [Google Scholar] [CrossRef]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. NeuroEng. Rehabil. 2012, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Skobel, E.; Martinez-Romero, A.; Scheibe, B.; Schauerte, P.; Marx, N.; Luprano, J.; Knackstedt, C. Evaluation of a newly designed shirt-based ECG and breathing sensor for home-based training as part of cardiac rehabilitation for coronary artery disease. Eur. J. Prev. Cardiol. 2014, 21, 1332–1340. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.H.; Cheng, M.S.; Chang, S.S.; Moore, J.; De Luca, G.; Nawab, S.H.; De Luca, C.J. A combined sEMG and accelerometer system for monitoring functional activity in stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Schwickert, L.; Becker, C.; Lindemann, U.; Maréchal, C.; Bourke, A.; Chiari, L.; Helbostad, J.L.; Zijlstra, W.; Aminian, K.; Todd, C. Fall detection with body-worn sensors. Zeitschrift für Gerontologie und Geriatrie 2013, 46, 706–719. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.A.; Mohktar, M.S.; Kamaruzzaman, S.B.; Lim, K.S.; Pin, T.M.; Ibrahim, F. Smartphone-based solutions for fall detection and prevention: challenges and open issues. Sensors 2014, 14, 7181–7208. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.C.; Hsu, Y.L. A review of accelerometry-based wearable motion detectors for physical activity monitoring. Sensors 2010, 10, 7772–7788. [Google Scholar] [CrossRef] [PubMed]
- Gebruers, N.; Vanroy, C.; Truijen, S.; Engelborghs, S.; De Deyn, P.P. Monitoring of physical activity after stroke: A systematic review of accelerometry-based measures. Arch. Phys. Med. Rehabil. 2010, 91, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; McCullagh, P.; Zhang, J.; Yu, T. A smartphone based real-time daily activity monitoring system. Clust. Comput. 2014, 17, 711–721. [Google Scholar] [CrossRef]
- Chernbumroong, S.; Cang, S.; Yu, H. A practical multi-sensor activity recognition system for home-based care. Decis. Support Syst. 2014, 66, 61–70. [Google Scholar] [CrossRef]
- Bulling, A.; Blanke, U.; Schiele, B. A tutorial on human activity recognition using body-worn inertial sensors. ACM Comput. Surv. (CSUR) 2014, 46. [Google Scholar] [CrossRef]
- Gao, L.; Bourke, A.K.; Nelson, J. Evaluation of accelerometer based multi-sensor versus single-sensor activity recognition systems. Med. Eng. Phys. 2014, 36, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Maetzler, W.; Domingos, J.; Srulijes, K.; Ferreira, J.J.; Bloem, B.R. Quantitative wearable sensors for objective assessment of Parkinson’s disease. Mov. Disord. 2013, 28, 1628–1637. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Quantitative assessment of upper limb motor function in Multiple Sclerosis using an instrumented Action Research Arm Test. J. NeuroEng. Rehabil. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Din, S.D.; Patel, S.; Cobelli, C.; Bonato, P. Estimating Fugl-Meyer clinical scores in stroke survivors using wearable sensors. In Proceedings of 2011 Annual International Conference of the Engineering in Medicine and Biology Society (EMBC), Boston, MA, USA, 30 August–3 September 2011; pp. 5839–5842.
- Patel, S.; Hughes, R.; Hester, T.; Stein, J.; Akay, M.; Dy, J.G.; Bonato, P. A novel approach to monitor rehabilitation outcomes in stroke survivors using wearable technology. Proc. IEEE. 2010, 98, 450–461. [Google Scholar] [CrossRef]
- Uswatte, G.; Foo, W.L.; Olmstead, H.; Lopez, K.; Holand, A.; Simms, L.B. Ambulatory monitoring of arm movement using accelerometry: An objective measure of upper-extremity rehabilitation in persons with chronic stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1498–1501. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Fang, Q.; Gu, X. Fuzzy inference system based automatic Brunnstrom stage classification for upper-extremity rehabilitation. Exp. Syst. Appl. 2014, 41, 1973–1980. [Google Scholar] [CrossRef]
- Zhang, Z.; Fang, Q.; Gu, X. Objective Assessment of Upper Limb Mobility for Post-stroke Rehabilitation. IEEE Trans. Biomed. Eng. 2015. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liparulo, L.; Panella, M.; Gu, X.; Fang, Q. A Fuzzy Kernel Motion Classifier for Autonomous Stroke Rehabilitation. IEEE J. Biomed. Heal. Inform. 2015. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Wang, J.; Fang, Q.; Wang, Y. Brunnstrom stage automatic evaluation for stroke patients using extreme learning machine. In Proceedings of the 2012 IEEE on Biomedical Circuits and Systems Conference (BioCAS), Hsinchu, Taiwan, 28–30 November 2012.
- Donoho, D.L. Compressed sensing. IEEE Trans. Inf. Theory 2006, 52, 1289–1306. [Google Scholar] [CrossRef]
- Baraniuk, R.G. Compressive sensing. IEEE Sign. Process. Mag. 2007, 24, 118–121. [Google Scholar] [CrossRef]
- Candes, E.J.; Romberg, J.K.; Tao, T. Stable signal recovery from incomplete and inaccurate measurements. Commun. Pure Appl. Math. 2006, 59, 1207–1223. [Google Scholar] [CrossRef]
- Tsaig, Y.; Donoho, D.L. Extensions of compressed sensing. Sign. Process. 2006, 86, 549–571. [Google Scholar] [CrossRef]
- Mallat, S.G.; Zhang, Z. Matching pursuits with time-frequency dictionaries. IEEE Trans. Sign. Process. 1993, 41, 3397–3415. [Google Scholar] [CrossRef]
- Tropp, J.; Gilbert, A.C. Signal recovery from random measurements via orthogonal matching pursuit. IEEE Trans. Inf. Theory 2007, 53, 4655–4666. [Google Scholar] [CrossRef]
- Chen, S.S.; Donoho, D.L.; Saunders, M.A. Atomic decomposition by basis pursuit. SIAM J. Sci. Comput. 1998, 20, 33–61. [Google Scholar] [CrossRef]
- Wipf, D.P.; Rao, B.D. Sparse Bayesian learning for basis selection. IEEE Trans. Sign. Process. 2004, 52, 2153–2164. [Google Scholar] [CrossRef]
- Zhang, Z.; Rao, B. Extension of SBL algorithms for the recovery of block sparse signals with intra-block correlation. IEEE Trans. Sign. Process. 2013, 61, 2009–2015. [Google Scholar] [CrossRef]
- Zhang, Z.; Jung, T.-P.; Makeig, S.; Rao, B. Compressed sensing for energy-efficient wireless telemonitoring of noninvasive fetal ECG via block sparse Bayesian learning. IEEE Trans. Biomed. Eng. 2013, 60, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.-B.; Zhou, H.; Ding, X.; Zhang, R. Extreme learning machine for regression and multiclass classification. IEEE Trans. Syst. Man Cybern. Part B: Cybern. 2012, 42, 513–529. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, L.; Xiong, D.; Guo, L.; Wang, J. A Compressed Sensing-Based Wearable Sensor Network for Quantitative Assessment of Stroke Patients. Sensors 2016, 16, 202. https://0-doi-org.brum.beds.ac.uk/10.3390/s16020202
Yu L, Xiong D, Guo L, Wang J. A Compressed Sensing-Based Wearable Sensor Network for Quantitative Assessment of Stroke Patients. Sensors. 2016; 16(2):202. https://0-doi-org.brum.beds.ac.uk/10.3390/s16020202
Chicago/Turabian StyleYu, Lei, Daxi Xiong, Liquan Guo, and Jiping Wang. 2016. "A Compressed Sensing-Based Wearable Sensor Network for Quantitative Assessment of Stroke Patients" Sensors 16, no. 2: 202. https://0-doi-org.brum.beds.ac.uk/10.3390/s16020202