1. Introduction
The use of inertial sensor technology for human motion analysis is increasing. Inertial sensor technology fuses signals from the accelerometer, gyroscope, and magnetometer to estimate the orientation and position of a body segment [
1,
2]. By applying multiple inertial measurement units on different body segments, three dimensional (3D) joint kinematics can be obtained outside the laboratory [
3]. Before an inertial sensor system can be used in clinical practice, it is important to establish the validity and reliability.
Multiple studies have evaluated the validity or reliability of (3D) kinematics measured by an inertial sensor system [
4]. However, the majority of these studies only assessed knee joint angles and mainly during level walking. In addition, few studies evaluated the reliability and agreement of the hip, knee, and ankle kinematics measured by an inertial sensor system [
5,
6,
7]. One study also included, besides walking, a squat and a vertical jump [
5]. For walking and squatting, acceptable between-day and between-operator reliability were reported, while the reliability and agreement for vertical jump were substantially lower [
5]. However, these tasks are less feasible to perform in other populations, such as persons with degenerative joint disease. Moreover, the studies that assessed the reliability only included the lower limb joint kinematics, without including trunk kinematics. Yet, lateral trunk lean has been reported as a (mal)adaptive movement strategy for persons that suffer from functional limitations (e.g., due to pain) [
8].
In a recent study, the authors assessed the reliability and agreement of the trunk and lower limb joint kinematics during both the open and closed-chain movement phases of transitional movement tasks, which included walking and physically demanding tasks such as a forward lunge, a sideward lunge, and going up and down stairs [
9]. The reliability and agreement of walking were better (i.e., intraclass correlation coefficient (ICC) between 0.4 and 1.0 for all movement phases and standard errors of measurement (SEM) <7.0 degrees) than the reliability of stair negotiation, as stair negotiation had a larger error in all movement plans (i.e., up to 13.5 degrees). The reliability and agreement of flexion/extension and ab/adduction angles during the swing phase and the stance phase of both the forward lunge and the sideward lunge were comparable to that of walking [
9]. Currently, little is known about the reliability and agreement of trunk and lower limb joints’ kinematics measured by inertial sensors during unipodal and bipodal lower limb tasks, such as a single leg squat (SLS) and a sit to stand (STS) task.
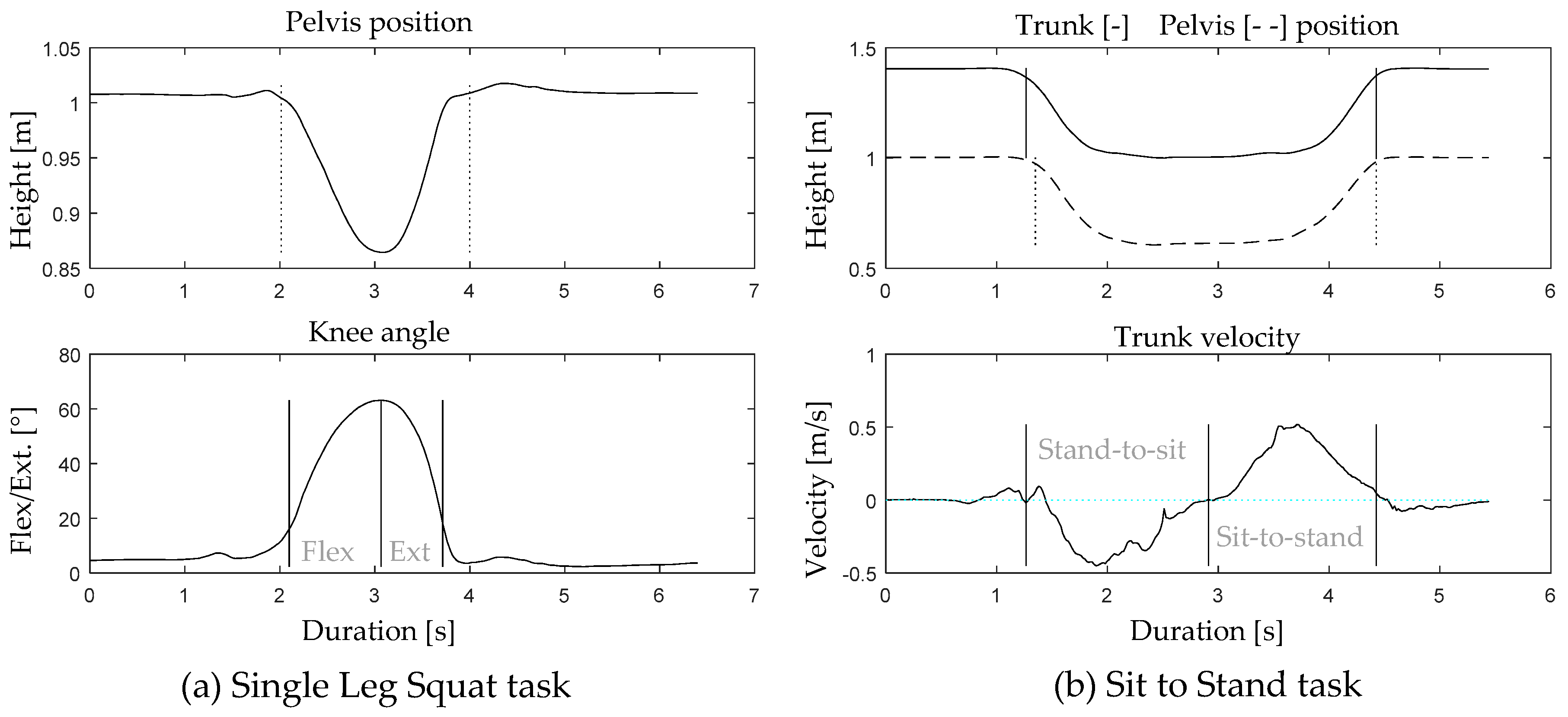
The SLS is a movement task that is commonly used to identify risk factors for lower limb musculoskeletal injury, as this task provides insight into the lower limb joints’ alignment and altered movement patterns of the trunk, pelvis, and lower limb joints [
10]. The STS task is an important activity of daily living and is considered to be essential for independent living in the elderly [
11]. Moreover, the STS task is addressed as a functional and valid measure to assess knee function. In this context, the maximum knee extension angular velocity during the STS task is already reported as a parameter to describe knee function. In addition, lateral trunk lean and asymmetrical loading to the contralateral leg during the STS task are recognized as adaptive movement strategies to avoid pain and compensate for quadriceps weakness [
11,
12]. For both tasks, adequate stability, strength, and neuromuscular control at the level of the trunk, pelvis, hip, and ankle are required for optimal task performance. Given the multidimensionality of the locomotor system, movements can be performed through multiple movement strategies. This implies that the same movement task can be performed in multiple manners by different individuals (i.e., with more or less movement in the different joints and movement planes).
Given that reliability and agreement results are task-specific, this study focusses on the investigation of the reliability and agreement of 3D joint kinematics, assessed by means of an inertial sensor system during a unipodal and a bipodal task. The aim of this study is to investigate the within-session, between-session, and between-operator reliability and agreement of the assessment of the trunk and lower limb joints’ range of motion (ROM) in all movement planes during the performance of the SLS and STS task. Furthermore, the reliability and agreement of the trunk and lower limb joints’ range of motion will be discussed during distinct phases of the movement task (e.g., stand-to-sit and sit-to-stand) in order to make recommendations with regard to task and phase selection for future studies.
4. Discussion
This study aimed to assess the within-session, between-session, and between-operator reliability and agreement of the trunk and lower limb joints’ 3D ROM during the SLS and STS task. Additionally, the reliability and agreement of the different movement phases of the SLS and the STS tasks were reported. For the SLS task, only small differences were found between the flexion and extension phase, in all movement planes. In contrast, during the STS task, larger differences in multiple movement planes were obtained between both movement phases.
4.1. Interpretation of Study Results
4.1.1. Main Movement
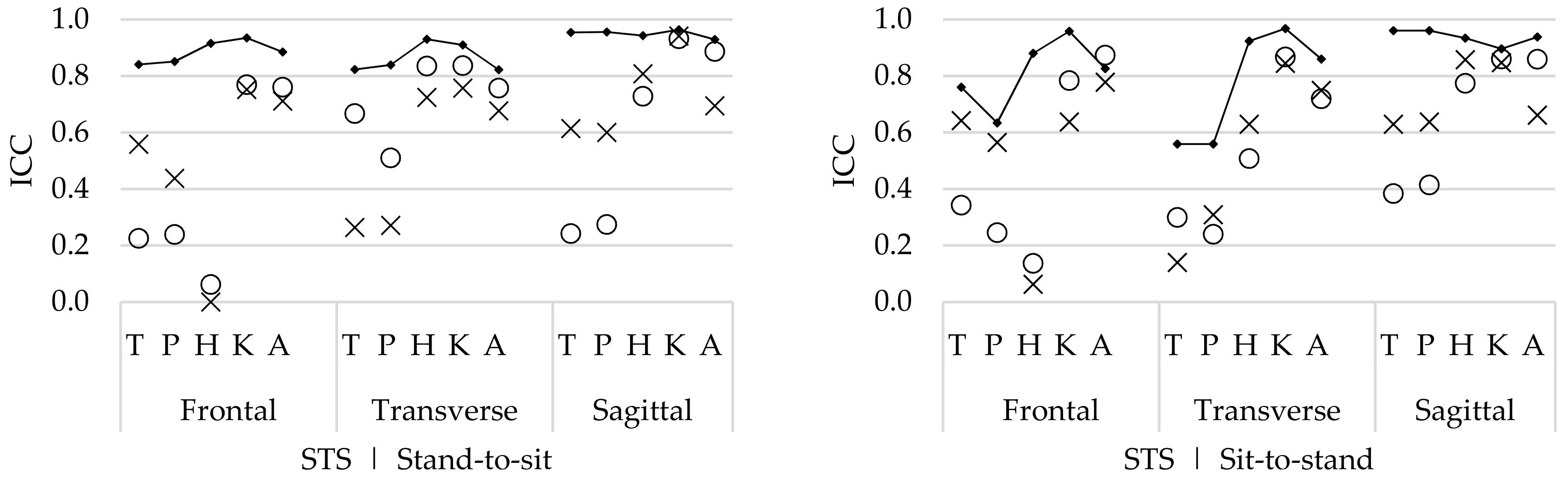
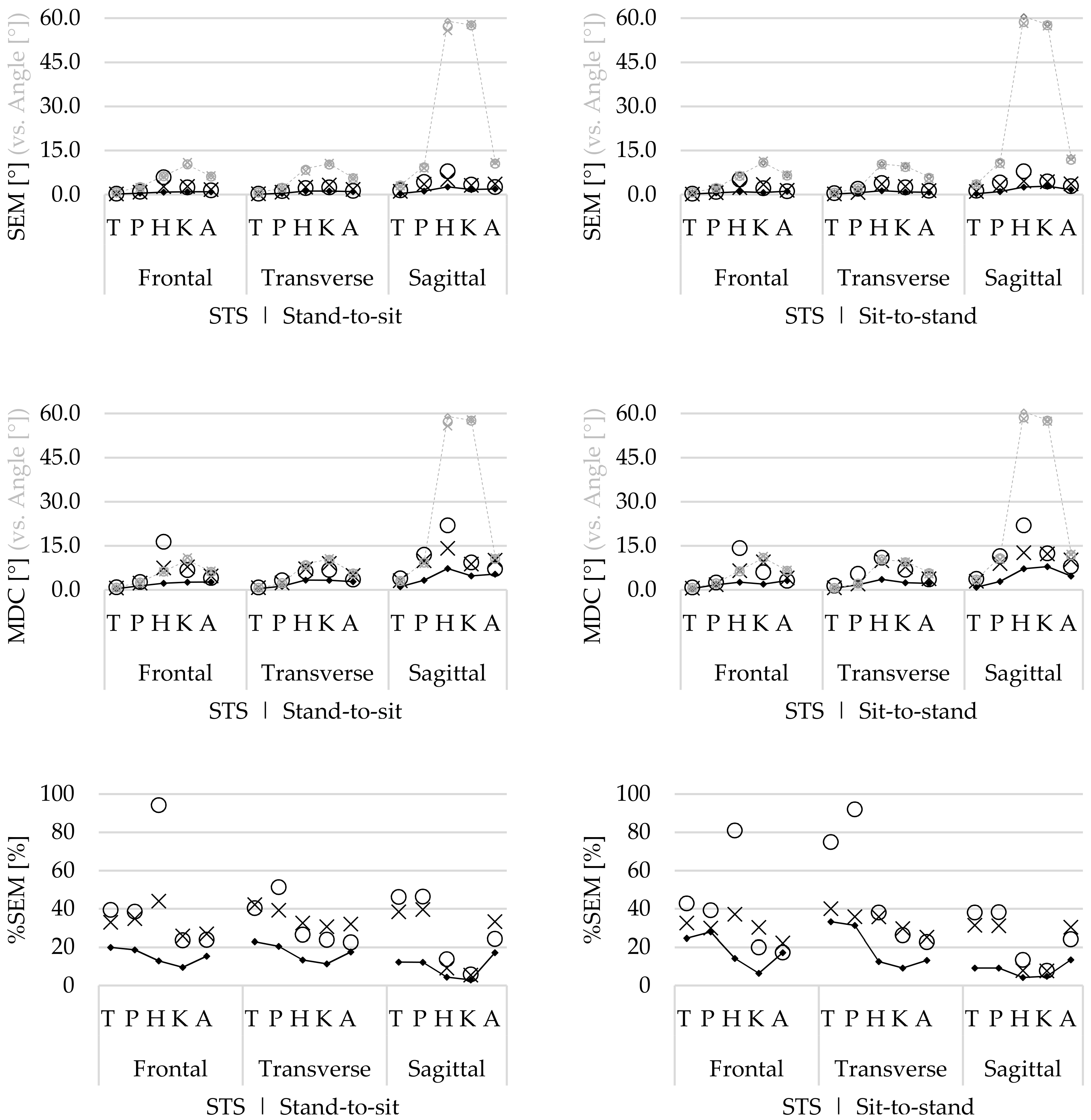
The main movements include the flexion/extension ROM of the trunk and lower limb joints. For the STS task, the within-session ICCs were good to excellent for the hip, knee, and ankle ROM in both movement phases. Between-session and between-operator ICCs were also high for the hip, knee, and ankle ROM in both movement phases, but slightly lower compared with the within-session reliability (
Figure 5). The trunk and pelvis ROM within-session ICCs were acceptable, but lower compared with the hip, knee, and ankle ROM. Also, for the between-session and between-operator reliability, the trunk and pelvis ROM was lower.
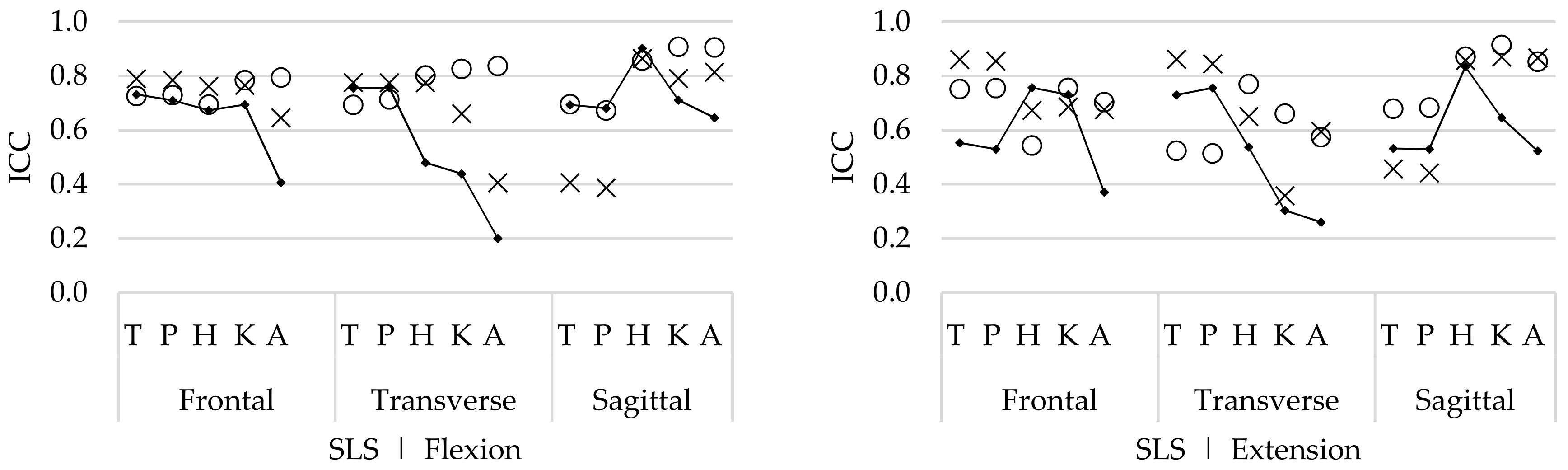
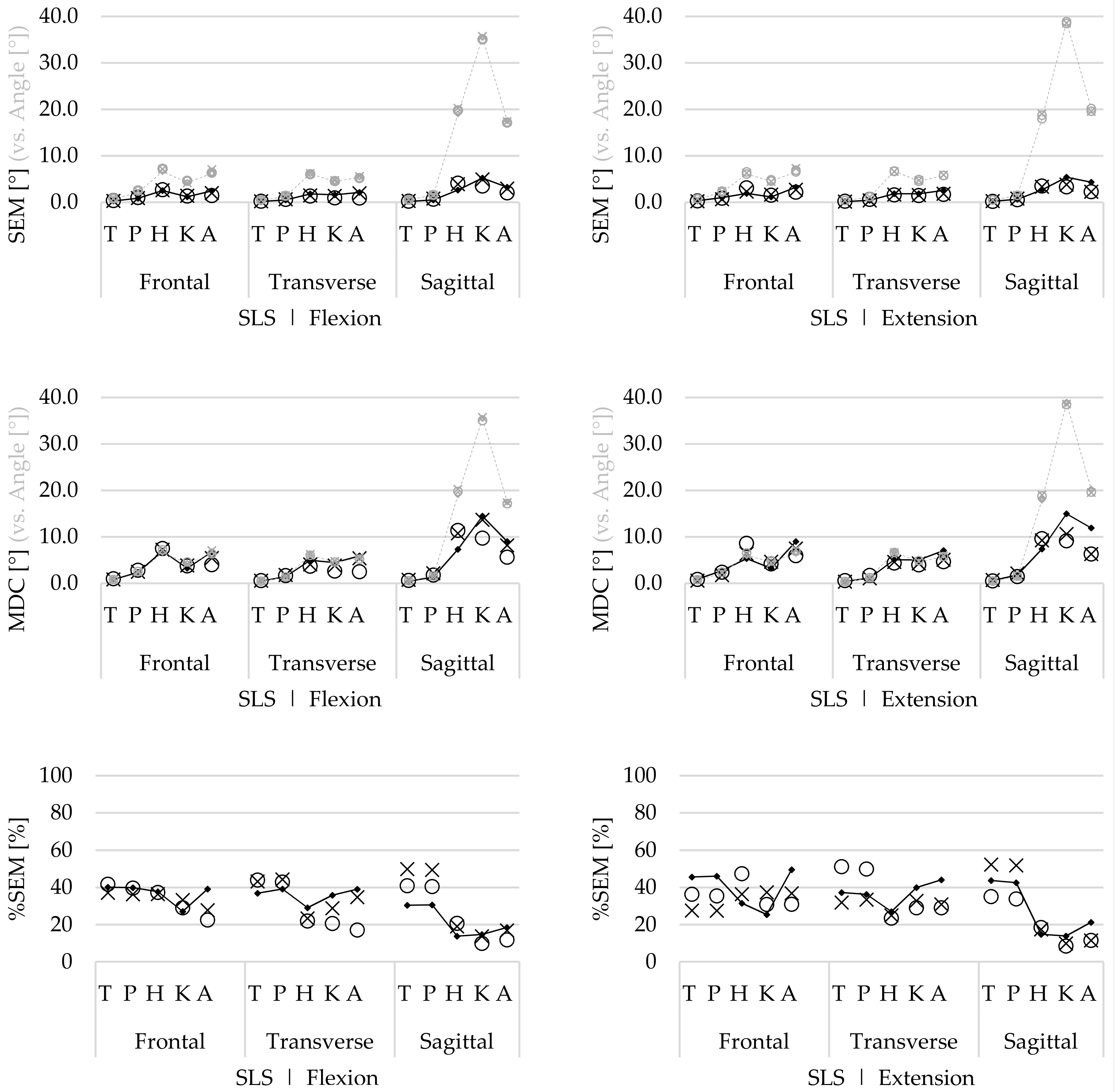
For the SLS, the within-session reliability of the hip ROM was high; however, the reliability of the knee and ankle ROM was lower in both movement phases. These lower ICCs indicate that there is more natural movement variability in these joints. This is also confirmed by the within-session SEM (
Figure 4), which show greater error in the knee flexion/extension ROM during the SLS. These differences in variability might be explained by the fact that the knee flexion angle (depth of the SLS) had no clear endpoint, as the depth of the SLS was standardized based on the maximum knee flexion without losing balance. In contrast, the stool height (at knee height) was a clear endpoint during the STS task, and thus results in less variation between repetitions.
In such cases, thorough instructions and task explanation are critical. Given the fact that the between-session and between-operator reliability were higher, it is expected that these differences were related to natural movement variability in trial-to-trial repetition.
4.1.2. Conjunct Movement
The conjunct movements contain the ab/adduction and in/external rotation ROM in all joints. For the STS task, the within-session reliability was good and higher for all ROMs, compared with the between-session and between-operator ICCs. Differences in the between-session and between-operators ICCs were present for the STS task, but these differences were not consistent (
Figure 3). For the SLS task, the within-session reliability was relatively low (compared with the STS task) for all joints. In contrast to the STS task, the between-session and between-operator ICCs of the SLS task were comparable or higher than the within-session ICCs for all joints.
The within-session agreement results confirm that the STS task was performed with less natural movement variability compared with the SLS task, because the SEM and %SEM were systematically lower for the STS (
Figure 5) compared with those for the SLS task (
Figure 4). However, compared with the within-session agreement, the between-session and between-operator agreement for the SLS remain similar, while the agreement for the STS task decreases. This demonstrates that although there is natural variability during the performance of repetitive SLS movements, this remains constant, as well as between sessions and operators. Furthermore, during the SLS, the ICCs increase for both the between-session and between-operator reliability compared with the within-session ICCs. Therefore, it is assumed that the natural movement variability is inconsistent between trial repetitions. As for this study, healthy participants were recruited, and it seems that they apply different movement strategies to perform the SLS between different repetitions, especially for the hip, knee, and ankle ab/adduction ROM and in/external rotation ROM (
Figure 2). However, by doing this inconsistently, the average over multiple trials will cancel out these differences.
In contrast to the SLS, the agreement decreases for the between-session and between-operator reliability for the STS task. Especially for the joints that include the pelvic sensor in the calculation of the joint angle (i.e., trunk, pelvis, and hip angles), the SEM increases and ICCs are generally lower. During data collection, it was noticed that the position of the pelvis sensor (especially during a dynamical task involving a lot of hip flexion such as the STS task) was easily altered by the participants’ shorts, which moved over or against the sensor, and thus potentially affected the orientation of the sensor (which is used for the calculation of multiple joint angles including the trunk and hip). Moreover, because the between-operator %SEM is ≥75% for the hip, trunk, and pelvic ROM during the STS task, it is presumed that there are methodological differences between sessions and operators.
In comparison, no studies investigated the reliability and agreement of trunk, pelvis, and lower limb joint kinematics during an SLS or STS task by means of an inertial sensor system. Only one study reported acceptable to good reliability and agreement of the flexion/extension kinematics from the lumbar spine and hip joint during functional movement control tasks (including a stand-to-sit-to-stand task) in healthy persons using inertial sensors [
18]. In addition, a recent study reported the reliability and agreement of the SLS task by means of an electromagnetic tracking system [
19]. The reported reliability and agreement of the trunk, pelvis, hip, and knee joints were higher compared with the results in the present study. However, in the study of Nakagawa and colleagues, only young healthy participants (20.8 ± 1.7 years) were included. As it is expected that the lower ICCs for the SLS in the present study are caused by natural movement variability, it appears that this variability is not present in a younger population. Additionally, in comparison with other functional tasks, assessed by means of an inertial sensor system, the SLS task showed good reliability and agreement, especially for the between-session and between-operator reliability, whereas the reliability and agreement of the STS task were comparable to other functional tasks [
5,
9].
4.1.3. Differences in Movement Phases
The SLS task showed slight differences in reliability or agreement between the flexion and extension phase. For the STS task, however, differences between movement phases were more obvious. For the sit-to-stand phase, the within-session ICCs of the trunk and pelvic ab/adduction and in/external rotation ROM were substantially lower compared with the stand-to-sit phase (similar differences were also observed in the agreement metrics). This indicates that both tasks show lower reliability and agreement in the return phase. Similar findings were reported for other functional movement activities such as the forward and sideward lunge. In these tasks, lower reliability was also reported for the swing backwards compared with the swing forward [
9], similar to the swing backward during the forward and sideward lunge, for the sit-to-stand phase and the extension phase of the SLS. This is potentially caused by the fact that extension of the knee joint (pushing the body back up) requires more motor control and force compared with the opposite movement.
4.1.4. Recommendations
For the SLS, it is recommended to use the averaged data over multiple (in this study four) repetitions, as the between session ICCs were substantially better than the within-session ICCs. Furthermore, no differences were observed between phases, thus both phases are reliable for use in the assessment of the SLS task. For the STS task, the individual repetitions showed good reliability and agreement. The averaged repetitions were lower, but not consistently different from each other, which indicates that there are no systematic differences between test sessions or operators. On the contrary, the averaged data showed lower reliability (and agreement) compared with the within-session data, which indicates that there are individual differences in task execution between test occasions. These differences occur predominantly in the angles (trunk, pelvis, and hip joints) that are determined based on position and orientation of the pelvic sensor. Therefore, in the case of a longitudinal data collection, it is recommended that this data collection is performed by one (the same) operator during all sessions. Furthermore, the sensor positioning should be standardized to the highest extent and during the calibration procedure, the participant should be positioned passively in the correct position in order to improve the sensor-to-segment alignment [
13,
20]. Proper strapping of the inertial sensors is required to reduce soft tissue artefacts and the proximity of ferromagnetic materials should be avoided in order to avoid magnetic disturbances [
3,
14]. Finally, it is recommended to ensure that the position and orientation of the pelvic sensor is not affected by the clothing during task execution.
4.2. Limitations and Future Research
As stated above, the within-session ICCs from the SLS were relatively low, whereas the between-session and between-operator ICCs were substantially higher. One reason for this is that the SLS is a clinical test to identify kinematic risk factors for lower limb musculoskeletal injury. It is important to perform this test according to an individual’s potential, in order to increase the clinical utility of the task. Another potential reason for this result could be that the healthy persons assessed in this study are not aware of the fact that they use multiple movement strategies in order to successfully achieve the SLS (i.e., movement redundancy). The authors assume that in the cases in which persons with pathology (e.g., degenerative disorders) are measured during the performance of an SLS, the within-session results might be higher. As it has been shown that movement variability decreases in the cases of pathology, and these persons adapt to a specific movement strategy [
21]. Therefore, to achieve the functional movement task, persons with a painful condition at the knee or hip joint might only rely on one specific movement strategy (i.e., decreased movement redundancy) as a result of their pain, which leads to higher within-session ICCs. Future studies are needed to examine this in a patient population. Furthermore, in this study, only one leg was analysed. However, it is known that movements of the non-weight bearing limb affect the trunk and lower limb joint kinematics [
10]. Therefore, future studies should not only investigate the weight bearing limb, but also focus on the non-weight bearing limb.
Within the present study, trunk and lower limb joint kinematics were recorded using a commercially available inertial sensor system (MVN BIOMECH Awinda, Xsens Technologies). The results thus need be interpreted within the constraints imposed by the specificity of the technology and calibration method. For joint angle calculation, inertial sensor technology generally relies on signal fusion of an integrated accelerometer and gyroscope signal and the magnetometer [
3]. It is known that (double) integration of the accelerometer and gyroscope signal, in order to determine sensor position and orientation, suffers from integration drift. To compensate for this drift, the magnetometer is used as a reference [
2]. Nevertheless, the magnetometer is easily disturbed by ferromagnetic materials or electronic devices, which invalidates the estimated position and orientation of the sensor and may affect the sensor-to-segment alignment during the static calibration [
22]. In order to reduce these errors, it is recommended to avoid the proximity of ferromagnetic materials. New methods have been developed that overcome these constraints by tracking motion without using the magnetometer [
22,
23]. However, these methods still need further development before they can be implemented in clinical research. In addition, careful positioning of the inertial sensors is crucial to maximally reduce soft-tissue artefacts, for example, due to muscle contraction, by positioning the sensor preferably on bony landmarks in order to minimize motion between the sensor and the bones. Proper strapping of the inertial sensor minimizes this movement artefact, but to date, it is impossible to completely avoid these artefacts.
For the present system, the initial static calibration procedure is sensitive to the predefined positioning and alignment of the inertial sensors [
24]. The participant should thus be positioned passively in the correct position in order to improve the sensor-to-segment alignment [
3,
14]. As the measurements in our study were conducted by well-trained operators, we are confident that these effects were maximally reduced, but were likely still present in the data and may affect data interpretation. The results of the present study must be interpreted while keeping this in mind. Future research should focus on improving the algorithms for the sensor-to-segment alignment and calibration procedures, in such a manner that the user is not bounded to a predefined sensor positioning, and so that a non-expert can use such a system. The initial results of studies that facilitate measurements with less accurate sensor alignment are promising [
25,
26,
27]. In the long term, this could lead to new opportunities to use inertial sensor technology outside the laboratory setting, such as in clinical practices or at home situations, which leads to a new range of opportunities.
Finally, as the present study demonstrated the reliability and agreement of functional movement tasks, future research should focus on the accuracy of the inertial sensor system and compare the trunk and lower limb joints’ kinematics measured by means of an inertial sensor system against an optoelectronic system (gold standard). In cases in which the accuracy of the kinematics from the inertial sensor system is known, it can potentially be used to assess (mal)adaptive movement strategies in persons with pathology.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

