Disaster Preparedness and Professional Competence Among Healthcare Providers: Pilot Study Results



1
Department of Aviation Security, Military University of Aviation, 08-521 Dęblin, Poland
2
Department of Emergency Medicine, Medical University of Lublin, 20-059 Lublin, Poland
*
Author to whom correspondence should be addressed.
Sustainability 2020, 12(12), 4931; https://0-doi-org.brum.beds.ac.uk/10.3390/su12124931
Submission received: 12 May 2020
/
Revised: 9 June 2020
/
Accepted: 16 June 2020
/
Published: 17 June 2020
(This article belongs to the Special Issue Emergencies and Public Health Crisis Management- Current Perspectives on Risks and Multiagency Collaboration)
Abstract
:The preparedness of a hospital for mass-casualty incident and disaster response includes activities, programs and systems developed and implemented before the event. These measures are designed to provide the necessary medical care to victims of disasters, and to minimize the negative impact of individual events on medical services. Up until now, there has been no systematic survey in Poland concerning the readiness of hospitals, as well as medical personnel, to deal with mass-casualty incidents. Consequently, little is known about the knowledge, skills, and professional competences of healthcare workers. The objective of this pilot study was to start an exploration and to collect data on the competences of healthcare workers, in addition to assessing the preparedness of hospitals for mass-casualty incidents. Utilizing an anonymous survey of a random sample, 134 healthcare providers were asked to respond to questions about the competencies they needed, and hospital preparedness during disaster response. It turned out that the test subjects evaluate their own preparedness for mass-casualty incidents and disasters better than the preparedness of their current place of work. The pilot study demonstrated that a properly designed questionnaire can be used to assess the relationship between hospital and staff preparedness and disaster response efficiency. Evaluation of the preparedness and effectiveness of disaster response is a means of finding and removing possible gaps and weaknesses in the functioning and effective management of a hospital during mass-casualty incidents.
1. Introduction
In a globalized world, in which crisis incidents are becoming more frequent, more devastating and have a significant impact on the health and lives of societies, the quality of healthcare services, including in particular the operational capacity of hospitals, is crucial for health security. A well-established preparedness program is a prerequisite for the effective response to emergencies of healthcare systems, including hospitals.
The preparedness of a hospital for mass-casualty incident and disaster response includes activities, programs and systems developed and implemented before the event. These measures are designed to provide the necessary medical care to victims of disasters, and to minimize the negative impact of individual events on medical services. These undertakings include, in particular, the appropriate training of medical personnel, appropriate safeguarding of logistics, and having validated emergency response procedures in place in the hospital. Evaluation of preparedness for incidents and disasters, as well as the effectiveness of response, is one way in which to locate and remove possible gaps and weaknesses in the functioning and effective management of the hospital during mass-casualty incidents (events that overwhelm the local healthcare system, where the number of casualties vastly exceeds the local resources and capabilities in a short period of time) [1,2,3].
Even in a well-prepared hospital, responding effectively to a disaster is a complex challenge. In the literature, there are many methods and evaluations [4,5,6,7,8,9,10] of the level of hospital emergency preparedness, but there is no consensus on correct and standardized methods and tools that would clearly define how individual institutions should prepare for crisis incidents [11,12,13,14]. This is largely due to the allocation of individual hospitals as well as, among others, geographical, demographic, climatic, social and economic factors, which may impact upon or be associated with the occurrence of particular events in a given region, or the response to them. It is also unclear whether individual procedures can reliably predict, in real time, the effectiveness of hospital functions [15,16,17]. Although many studies [18,19,20,21,22,23,24,25,26,27] have assessed the correlation between the level of hospital preparedness and disaster response, only a few functional elements have actually been assessed.
Although the World Health Organization (WHO) has developed the Hospital Safety Index (HSI) [28], a checklist of all hazards, which is a standardized, globally accepted method for assessing hospital preparedness, to date there have been no legally regulated international standards for hospital preparedness and response to crisis incidents [29,30,31,32].
Up until now, there has been no systematic survey in Poland concerning the readiness of hospitals, as well as medical personnel, to deal with mass-casualty incidents. Consequently, little is known about the knowledge, skills, and professional competences of healthcare workers [33,34,35]. This information is crucial for the development of effective response plans for individual hospitals, as well as for the preparation of training tailored to the needs of medical personnel [36,37]. The above-mentioned factors prompted the authors to undertake this study.
2. Aim
The main aim of the study is to investigate and to collect data on the competences of healthcare workers, in addition to assessing the preparedness of hospitals for mass-casualty incidents. An additional aim is to use the data from this initial survey to design a more comprehensive analysis of disaster preparedness (preparedness is defined by the United Nations International Strategy for Disaster Reduction as knowledge, capabilities and actions of governments, organizations, community groups and individuals “to effectively anticipate, respond to, and recover from, the impacts of likely, imminent or current hazard events or conditions), as well as new training and exercise models, which could improve the preparedness of health services for mass-casualty incidents and disasters.
3. Materials and Methods
3.1. Test Site
The study was conducted between 10 and 21 February 2020 at Public University Hospital No. 1 (polish SPSK No. 1) in Lublin. This hospital was selected as one of the largest hospitals in the Lublin region, and for this reason, it was chosen for the pilot study. SPSK No. 1 has a total of about 550 beds (including chemotherapy beds). It employs about 1600 people (including doctors, nurses and other medical personnel, as well as administration, technical, cleaning and service personnel). According to the latest data provided by the hospital, the number of hospitalizations for the academic year of 2017–2018 was about 40,000 cases, and the number of surgical procedures performed was about 19,000. The average time of hospitalization was 4.4 days.
3.2. Population Studied
The quantitative pilot study was conducted in the form of an anonymous questionnaire on a random sample of 134 healthcare workers, which account for 11.1% of the total number of employed healthcare workers at SPSK 1. More than half of them were women (56%). Men, on the other hand, constituted 44% of the research group. The respondents were mostly people with over 20 years of service (41.8%), while less frequently they had 6–10 years of service (19.4%), 0–5 years (16.4%), 11–15 years (12.7%) or 16–20 years (9.7%). Doctors (41.8%) and nurses (46.3%) represented the highest proportion of the study group, whereas 11.9% of respondents were paramedics.
3.3. Study Design
An extensive analysis of literature, and then the arrangement of the acquired knowledge through categorization and knowledge mapping, led to the development of a research tool in the form of a close-ended questions questionnaire. A qualitative method was used to verify the research tool and the questionnaire was tested on a sample of 10 people in order to check whether the respondents understood the questions it contained and whether the respondents reacted to some questions. This group was then excluded from the pilot study and their answers were not included in the final analysis. The questionnaire was designed in such a way that the time required to complete it did not exceed 15 min.
3.4. Type of Study
In the pilot study, an original questionnaire was available in both paper and online versions, and contained 18 closed questions and two additional descriptive questions. The respondents were asked about their own competences, experience, courses, and training completed, as well as knowledge about preparedness of the workplace for mass-casualty incidents. Respondents were also asked to rate their own preparedness on a scale from 1 to 10, as well as the preparedness of the hospital in which they worked, for mass-casualty incidents.
3.5. Data Analysis
Statistical analyses were conducted using IBM SPSS Statistics version 26. Frequency analyses, analysis of basic descriptive statistics, correlation analysis using Spearman’s rho coefficient, the chi square test of independence, the Student’s t-test for dependent samples, a one-way analysis of variance, and a Student’s t-test for independent samples in addition to Mann Whitney’s test were performed. The level of statistical significance was set at the classic level of α = 0.05.
3.6. Ethical Considerations
The study is not a medical experiment and legally does not require the approval of the Bioethics Committee.
4. Results
4.1. Frequency Analysis
In response to the question about participation in a mass-casualty incident or disaster as a healthcare worker, the majority of respondents (74.6%) declared that they had not participated in such an event. More than a quarter of the respondents (25.4%) answered in the affirmative to the analyzed question.
The respondents were asked whether the facility where they currently worked has a plan for dealing with mass-casualty incidents and disasters. Most of the respondents (71.6%) answered “yes” to this question. Only 3% of the respondents answered “no” to this question. More than a quarter of the respondents (25.4%) felt they did not know the answer to this question (Table 3).
The respondents most frequently (77.6%) reported that they were familiar with the procedure for dealing with mass-casualty incidents and disasters. Only 22.4% of the research group was not acquainted with the procedure for handling such situations.
Most of the respondents (79.1%) knew who was responsible for managing mass-casualty incidents and disasters in the facility of their current workplace. On the other hand, 20.9% answered in negatively to this question.
In response to the question concerning the knowledge of the procedures to be followed in the event of evacuation during a mass-casualty incident at their workplace, the majority of respondents (87.3%) answered affirmatively. Only 12.7% of respondents did not know the procedures to be followed in this situation.
The respondents were asked whether their workplace had adequate logistical infrastructure for mass-casualty incidents. Most often (41.8%) respondents did not know whether their workplace had such a logistical infrastructure. On the other hand, 39.6% of the respondents believed their workplace to be prepared logistically for mass-casualty incidents. On the other hand, 18.7% of respondents answered negatively to this question.
More than half of the respondents (54.5%) reported a lack of organization with drills regarding disaster management at their workplace. In turn, 45.5% of the respondents stated that such activities had been organized at their workplace.
As far as the frequency of organizing drills is concerned, respondents most frequently reported that such drills were organized less frequently than once every 3 years (91.8%). Individual respondents provided the following answers: once every 3 years (3%), once every 2 years (3%) and annually (2.2%). More than half of the respondents (53.7%) had not received training related to disaster preparedness at their current workplace. However, 46.3% of respondents reported that they had received such training.
In response to the question concerning knowledge of triage, almost all respondents (99.3%) answered yes. Only one person answered negatively to this question.
4.2. Relationship between Sociodemographic Variables and Evaluation of Preparedness for Mass-Casualty Incidents and Disasters
The statistical analyses carried out checked the relationship between sociodemographic variables and the evaluation of preparedness for mass-casualty incidents and disasters. To this end, a correlation analysis using Spearman’s rho coefficient and a one-way analysis of variance were performed.
Initially, the relationship between the seniority of the respondents and the evaluation of preparedness for mass-casualty incidents and disasters was tested. For this purpose, correlation analyses using Spearman’s rho coefficient were performed. The results of this analysis are presented in Table 1.
According to the analyses carried out, seniority is positively linked to the evaluation of the preparedness of the current workplace for a mass-casualty incident or disaster (weak link). This shows that the longer the respondents have been working, the better do they evaluate the preparedness of the institution where they work for a mass-casualty incident or disaster.
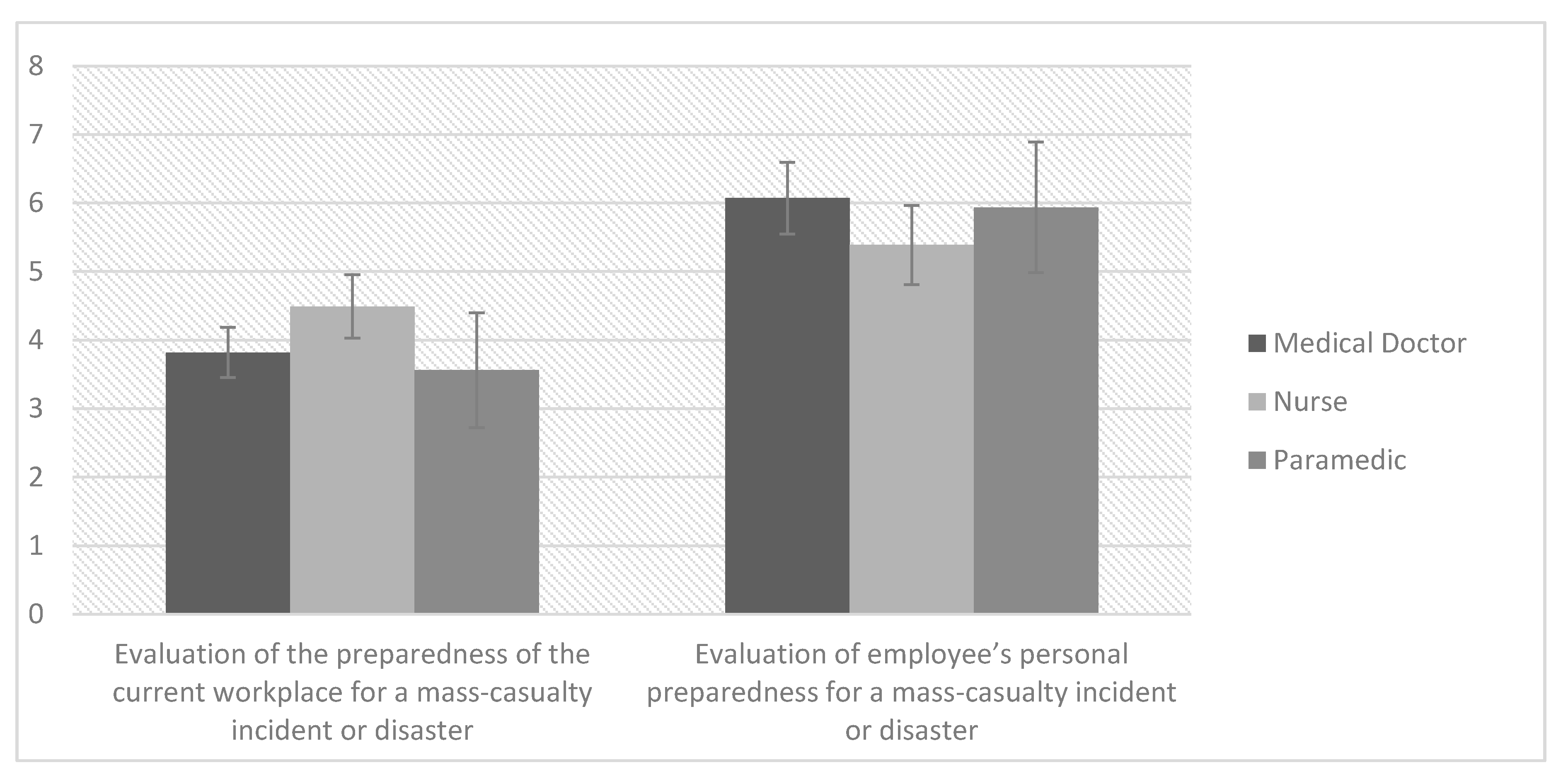
A one-way analysis of variance was then carried out to see if occupation differentiates the evaluation of preparedness for mass-casualty incidents or disasters. The results of this analysis are presented in Figure 1.
The results indicate a statistically significant effect for assessing the preparedness of the current workplace for a mass-casualty incident or disaster. In order to investigate the exact differences, Sidak post hoc tests were performed. The test results show no statistically significant difference.
4.3. Differences between the Evaluation of Preparedness for a Mass-Casualty Incident or Disaster in the Current Place of Work and the Evaluation of One’s Own Preparedness
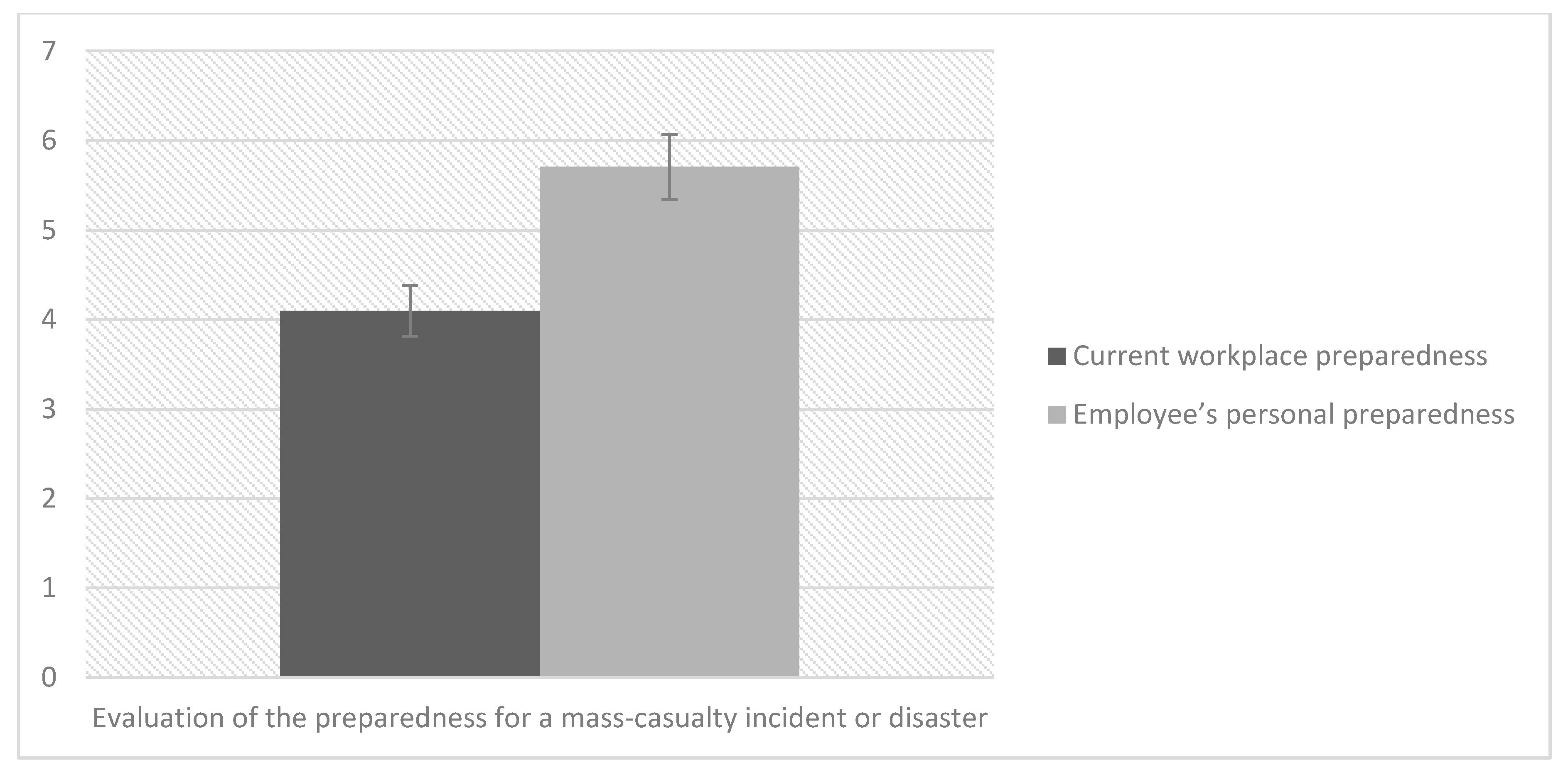
In the next stage of the analyses, it was assessed whether there are differences between the evaluation of one’s own preparedness and the evaluation of the current workplace’s preparedness for a mass-casualty incident and disaster. For this purpose, Student’s t-test was performed for dependent samples. The results of this test are presented in Table 2 and in Figure 2.
The test results indicate statistically significant differences. It turned out that the test subjects evaluate their own preparedness for mass-casualty incidents and disasters better than the preparedness of the current place of work. The strength of this effect is high.
4.4. Differences in the Evaluation of Preparedness for a Mass-Casualty Incident or Disaster Depending on Previous Participation in a Mass-Casualty Incident or Disaster as a Healthcare Professional
It was assessed whether the subjects who had previously been involved in a mass-casualty incident or disaster as a healthcare worker differ in their evaluation of preparedness for such situations from those who had not been involved in such an event. A Mann Whitney test was conducted due to the large numerical differences between the analyzed groups. The results are presented in Table 3.
The results of the tests indicate a statistically significant effect of moderate strength for the evaluation of one’s own preparedness for mass-casualty incidents or disasters. As it turns out, respondents who took part in a mass-casualty incident or disaster as a healthcare worker evaluate their own preparedness much better than respondents who had not been involved in such an event.
4.5. Differences in the Evaluation of Preparedness for a Mass-Casualty Incident or Disaster Depending on the Organisation of Drills by the Institution and Whether They Were Attended by the Respondents
In order to check the differences in the evaluation of preparedness for mass-casualty incidents or disasters between respondents with different opinions concerning the organization of drills by the institution and depending on whether they took place, Student’s t-tests for independent samples and Mann Whitney tests were performed. Initially, a Student’s t-test for independent samples was conducted. It was decided to assess whether the respondents whose institution had organized drills regarding disaster management differed from those whose institution had not conducted such drills in relation to the evaluation of preparedness for such situations. The test results are presented in Table 2.
It was then assessed whether the evaluation of preparedness for such situations is impacted by the frequency of training on what to do in the event of a mass-casualty incident or disaster. Due to significant differences in the number of groups compared, Mann Whitney tests were performed.
The results of this test indicate a statistically significant and moderate effect for the evaluation of the preparedness of the current workplace for a mass-casualty incident or disaster. This results from the fact that the respondents, whose institution organized drills for such situations once every 3 years or more often, better evaluate the preparedness of the institution than the respondents whose institution organized trainings less frequently than once every 3 years. The results of the tests are presented in Table 4.
It was then assessed whether training in preparation for disasters impacts upon the evaluation of preparedness for mass-casualty incidents or disasters. Student’s t-tests for independent tests were performed for this purpose.
The results of this test indicate significant differences for the evaluation of both one’s own preparedness and also that of the institution. Both of these effects are of moderate strength. The analysis showed that after training, the respondents evaluate their own and the institution’s preparedness for a mass-casualty incident or disaster better than the respondents without such training. Test results are presented in Figure 3.
5. Discussion
The creation of hospital crisis management plans, evacuation plans and procedures in the event of mass-casualty incidents, and the necessity for staff to be familiar with them, is an important step towards preparing for such events. However, the lack of such plans may lead to chaos and complete disorientation [38,39,40,41,42].
The research shows that the majority of the respondents knew that the institution at which they currently worked had a plan for dealing with mass-casualty incidents and disasters. Moreover, over 70% of respondents reported that they knew who was responsible for the management of operations in crisis situations and were aware of the procedures to be followed during a disaster.
In mass-casualty incidents and disasters, due to the limited capacity and resources of the emergency services on site, it is not possible to provide medical assistance to all victims simultaneously. Some of them will have to wait for such assistance. In the first instance, medical assistance must be provided to victims who need it at that moment, i.e., people in immediate danger of death. This assistance must be effective. The aim is to provide maximum benefits to as many people as possible under specified conditions. The need to do what is best for victims of a mass-casualty incident or disaster makes it necessary to continuously apply medical segregation of the victims. Triage is one of the most important and often the only undertaking of rescue services providing quick control of the situation in the area of a mass-casualty incident or disaster [43].
In the study concerning triage, almost all respondents declared having the ability to conduct triage.
Each hospital should have its own evacuation plan, as every healthcare facility is different, with different architectural features, number of floors in the building, numbers of patients and their physical and mental condition, equipment, and many other features. Additionally, each event is different. Evacuation can take place in connection with a bomb threat when there are no obstacles in the form of smoke, fire, toxic products from combustion, problems with visibility, or time pressure—as happens in the case of fire. Proper evacuation of a hospital requires a well-thought-out strategy and good preparation and, in order to achieve this, drills carried out in advance [13].
The research demonstrates that the respondents are familiar with the procedures to be followed in case of evacuation in the event of a mass-casualty incident at their workplace. The developing of an evacuation plan for the healthcare facility, familiarizing the entire staff with it, and performing regular evacuation drills, are necessary to ensure the safety of patients and workers [13].
The impact of catastrophes can be avoided or reduced by adopting risk management measures, which should be implemented by taking advantage of local resources and taking appropriate actions in terms of planning, education and training [44,45].
The human factor is a significant problem in the proper, continuous preparation for emergency situations or disasters in healthcare organizations. The shortage of medical personnel [46], the overload of current work, the increasing amount of documentation, and the completion of a number of necessary formalities can make doctors reluctant to participate in such training, especially during prolonged periods of relative calm when there are no unexpected events. It can be a problem to force staff to familiarize themselves with the documentation, operating procedures and evacuation plans for mass-casualty events and disasters. In most cases, this consists of a quick, cursory, thoughtless review, because in times of prolonged security, people do not feel an approaching threat, so they do not have a strong motivation to prepare for crisis situations [47].
More than half of the respondents (54.5%) reported a lack of organization of drills concerning disaster management in their workplace. As far as the frequency of organizing drills is concerned, the majority indicated that such drills were organized less frequently than once every 3 years.
The challenges faced by the healthcare services force them to provide continuous training in the organization of responses to mass-casualty incidents and disasters, and in cooperation with other emergency services. Simulations and drills are organized from time to time, but this is not enough. It is worth remembering that every event, even seemingly simple to perform, is difficult, and not every scenario can be foreseen. There can never be too many drills. Only through continuous practice can the most appropriate procedures and skills to deal with crisis situations be developed. Besides having excellent equipment and access to appropriate personal protective equipment (e.g., in the case of a patient infected with the SARS-CoV-2 coronavirus), above all, working in accordance to safety procedures that have been prepared in advance is an example of exemplary disaster management [48].
The only drawback after the exercises is usually the lack of review and feedback for the participants. This problem was reported by the respondents in the conducted research.
Theory will never equate to practice. Only practiced procedures provide the opportunity to verify the knowledge and skills of staff, and make it possible to carry out an analysis of the speed and effectiveness of the drills, and if necessary to make corrections, eliminate errors and, above all, acquire habits that will guarantee proper behavior [49].
Each hospital should have properly prepared disaster management procedures. Such guidelines should be prepared well in advance. When a threat occurs, it should be sufficient enough to adapt them to the specific situation, so that there is no need to create everything from scratch.
Humanity has experienced many disasters and pandemics in the past, but these have been overcome (e.g., smallpox, plague, measles, polio, whooping cough, typhus, rabies and cholera).
The current pandemic has very clearly shown the speed with which even the best healthcare systems in different countries can be overwhelmed and devastated. These observations show that health should be at the top of the political agenda.
6. Limitations
The main limitation of this study was that only the employees of one hospital were studied. The COVID-19 pandemic proved to be a huge obstacle in further research. Despite these limitations, the study revealed some implementation and scientific gaps for researchers, but at the same time it is a chance to initiate discussion and become a small contribution to solving the crisis that disaster leads to. The experience gained from this study will form the basis for planned future studies with more hospitals, and a more comprehensive approach. It will also help to properly amend the questions, which will make it easier to design a future research tool.
7. Conclusions
The pilot study revealed that a properly designed questionnaire can be used to assess the relationship between hospital and staff preparedness and disaster response efficiency.
The knowledge and skills of health professionals in relation to specific events and their impact on people, as well as the appropriate treatment, are essential for the quality of healthcare services during disasters.
In order to achieve the level of preparedness and the effectiveness of the disaster response, it is necessary that every hospital has pre-prepared and validated procedures.
An experimental study involving a range of hospitals should be carried out, using more comprehensive assessment tools, to assess the correlation between the level of preparedness and performance of the hospital and the impact of the preparation of the hospital and its staff towards the survival of disaster victims.
Evaluation of the preparedness and effectiveness of disaster response is a means of identifying and removing possible gaps and weaknesses in the functioning and effective management of a hospital during mass-casualty incidents.
Author Contributions
Conceptualization: K.G.; data collection: K.G. and M.G.; formal Analysis: K.G. and M.G.; writing—original draft preparation: K.G. and M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Djalali, A.; Carenzo, L.; Ragazzoni, L.; Azzaretto, M.; Petrino, R.; Della Corte, F.; Ingrassia, P.L. Does hospital disaster preparedness predict response performance during a full-scale exercise? A pilot study. Prehospital Disaster Med. 2014, 29, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, C.; Ingrassia, P.L.; Della Corte, F.; Carenzo, L.; Sapori, J.M.; Gabilly, L.; Segond, F.; Grieger, F.; Arnod-Prin, P.; Larrucea, X.; et al. Hospital preparedness and response in CBRN emergencies: TIER assessment tool. Eur. J. Emerg. Med. 2017, 24, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Djalali, A.; Castren, M.; Khankeh, H.; Gryth, D.; Radestad, M.; Öhlen, G.; Kurland, L. Hospital disaster preparedness as measured by functional capacity: A comparison between Iran and Sweden. Prehospital Disaster Med. 2013, 28, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Adini, B.; Laor, D.; Hornik-Lurie, T.; Schwartz, D.; Aharonson-Daniel, L. Improving hospital mass casualty preparedness through ongoing readiness evaluation. Am. J. Med. Qual. 2012, 27, 426–433. [Google Scholar] [CrossRef]
- Cagliuso, N. Stakeholders’ experiences with US hospital emergency preparedness: Part 1. J. Bus. Contin. Emerg. Plan. 2014, 8, 156–168. [Google Scholar]
- Gillett, B.; Silverberg, M.; Roblin, P.; Adelaine, J.; Valesky, W.; Arquilla, B. Computer-facilitated assessment of disaster preparedness for remote hospitals in a long-distance, virtual tabletop drill model. Prehospital Disaster Med. 2011, 26, 230–233. [Google Scholar] [CrossRef]
- Higgins, W.; Wainright III, C.; Lu, N.; Carrico, R. Assessing hospital preparedness using an instrument based on the Mass Casualty Disaster Plan Checklist: Results of a statewide survey. Am. J. Infect. Control 2004, 32, 327–332. [Google Scholar] [CrossRef]
- Mortelmans, L.J.; Gaakeer, M.I.; Dieltiens, G.; Anseeuw, K.; Sabbe, M.B. Are Dutch hospitals prepared for chemical, biological, or radionuclear incidents? A survey study. Prehospital Disaster Med. 2017, 32, 483–491. [Google Scholar] [CrossRef]
- Nekoie-Moghadam, M.; Kurland, L.; Moosazadeh, M.; Ingrassia, P.L.; Della Corte, F.; Djalali, A. Tools and checklists used for the evaluation of hospital disaster preparedness: A systematic review. Disaster Med. Public Health Prep. 2016, 10, 781–788. [Google Scholar] [CrossRef]
- Alruwaili, A.; Islam, S.; Usher, K. Disaster Preparedness in Hospitals in the Middle East: An Integrative Literature Review. Disaster Med. Public Health Prep. 2019, 13, 806–816. [Google Scholar] [CrossRef]
- Lazar, E.J.; Cagliuso, N.V.; Gebbie, K.M. Are we ready and how do we know? The urgent need for performance metrics in hospital emergency management. Disaster Med. Public Health Prep. 2009, 3, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Ogedegbe, C.; Nyirenda, T.; DelMoro, G.; Yamin, E.; Feldman, J. Health care workers and disaster preparedness: Barriers to and facilitators of willingness to respond. Int. J. Emerg. Med. 2012, 5, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goniewicz, K.; Misztal-Okońska, P.; Pawłowski, W.; Burkle, F.M.; Czerski, R.; Hertelendy, A.J.; Goniewicz, M. Evacuation from Healthcare Facilities in Poland: Legal Preparedness and Preparation. International J. Environ. Res. Public Health 2020, 17, 1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beerens, R.J.J.; Tehler, H. Scoping the field of disaster exercise evaluation—A literature overview and analysis. Int. J. Disaster Risk Reduct. 2016, 19, 413–446. [Google Scholar] [CrossRef]
- Hodge, A.J.; Miller, E.L.; Skaggs, M.K.D. Nursing self-perceptions of emergency preparedness at a rural hospital. J. Emerg. Nurs. 2017, 43, 10–14. [Google Scholar] [CrossRef]
- Kollek, D.; Cwinn, A.A. Hospital emergency readiness overview study. Prehospital Disaster Med. 2011, 26, 159–165. [Google Scholar] [CrossRef]
- Cocco, C.; Thomas-Boaz, W. Preparedness planning and response to a mass-casualty incident: A case study of Sunnybrook Health Sciences Centre. J. Bus. Contin. Emerg. Plan. 2019, 13, 6–21. [Google Scholar]
- Valesky, W.; Roblin, P.; Patel, B.; Adelaine, J.; Zehtabchi, S.; Arquilla, B. Assessing hospital preparedness: Comparison of an on-site survey with a self-reported, internet-based, long-distance tabletop drill. Prehospital Disaster Med. 2013, 28, 441–444. [Google Scholar] [CrossRef]
- Adini, B.; Goldberg, A.; Cohen, R.; Bar-Dayan, Y. Relationship between equipment and infrastructure for pandemic influenza and performance in an avian flu drill. Emerg. Med. J. 2009, 26, 786–790. [Google Scholar] [CrossRef]
- Skryabina, E.; Reedy, G.; Amlôt, R.; Jaye, P.; Riley, P. What is the value of health emergency preparedness exercises? A scoping review study. Int. J. Disaster Risk Reduct. 2017, 21, 274–283. [Google Scholar] [CrossRef] [Green Version]
- Verheul, M.L.; Dückers, M.L.; Visser, B.B.; Beerens, R.J.; Bierens, J.J. Disaster exercises to prepare hospitals for mass-casualty incidents: Does it contribute to preparedness or is it ritualism? Prehospital Disaster Med. 2018, 33, 387–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foote, M.; Daver, R.; Quinn, C. Using “mystery patient” drills to assess hospital ebola preparedness in new York City, 2014–2015. Health Secur. 2017, 15, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Williams, M.D. No-Notice Mystery Patient Drills to Assess Emergency Preparedness for Infectious Diseases at Community Health Centers in New York City, 2015-2016. J. Community Health 2019, 44, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Djalali, A.; Ardalan, A.; Ohlen, G.; Ingrassia, P.L.; Della Corte, F.; Castren, M.; Kurland, L. Nonstructural safety of hospitals for disasters: A comparison between two capital cities. Disaster Med. Public Health Prep. 2014, 8, 179–184. [Google Scholar] [CrossRef]
- Arab, M.A.; Khankeh, H.R.; Mosadeghrad, A.M.; Farrokhi, M. Developing a hospital disaster risk management evaluation model. Risk Manag. Healthc. Policy 2019, 12, 287. [Google Scholar] [CrossRef] [Green Version]
- Shabanikiya, H.; Jafari, M.; Gorgi, H.A.; Seyedin, H.; Rahimi, A. Developing a practical toolkit for evaluating hospital preparedness for surge capacity in disasters. Int. J. Disaster Risk Reduct. 2019, 34, 423–428. [Google Scholar] [CrossRef]
- Lennquist Montán, K.; Riddez, L.; Lennquist, S.; Olsberg, A.; Lindberg, H.; Gryth, D.; Örtenwall, P. Assessment of hospital surge capacity using the MACSIM simulation system: A pilot study. Eur. J. Trauma Emerg. Surg. 2017, 43, 525–539. [Google Scholar] [CrossRef]
- World Health Organization; Pan American Health Organization. Hospital Safety Index: Guide for Evaluators, 2nd ed.; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/258966 (accessed on 15 June 2020).
- Fallah-Aliabadi, S.; Ostadtaghizadeh, A.; Ardalan, A.; Fatemi, F.; Khazai, B.; Mirjalili, M.R. Towards developing a model for the evaluation of hospital disaster resilience: A systematic review. BMC Health Serv. Res. 2020, 20, 64. [Google Scholar] [CrossRef] [Green Version]
- Vichova, K.; Hromada, M. The Evaluation System to Ensure the Transport of Emergency Supplies of Fuel to the Hospitals. Transp. Res. Procedia 2019, 40, 1618–1624. [Google Scholar] [CrossRef]
- Khankeh, H.; Mosadeghrad, A.M.; Abbasabadi Arab, M. Developing accreditation standards for disaster risk management: An approach for hospital preparedness improvement–editorial. J. Mil Med. 2019, 20, 574–576. [Google Scholar]
- Martinez, D.; Talbert, T.; Romero-Steiner, S.; Kosmos, C.; Redd, S. Evolution of the Public Health Preparedness and Response Capability Standards to Support Public Health Emergency Management Practices and Processes. Health Secur. 2019, 17, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Veenema, T.G. (Ed.) Disaster Nursing and Emergency Preparedness; Springer Publishing Company: Berlin, Germany, 2018. [Google Scholar]
- Gowing, J.R.; Walker, K.N.; Elmer, S.L.; Cummings, E.A. Disaster preparedness among health professionals and support staff: What is effective? An integrative literature review. Prehospital Disaster Med. 2017, 32, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.; Mahmoud, N. Emergency Preparedness and Perceived Competence in Disaster. Alex. Sci. Nurs. J. 2016, 18, 1–14. [Google Scholar]
- Goniewicz, K.; Goniewicz, M.; Burkle, F.M. The Territorial Defence Force in disaster response in Poland: Civil-military collaboration during a state of emergency. Sustainability 2019, 11, 487. [Google Scholar] [CrossRef] [Green Version]
- Goniewicz, K.; Burkle, F.M. Disaster early warning systems: The potential role and limitations of emerging text and data messaging mitigation capabilities. Disaster Med. Public Health Prep. 2019, 13, 709–712. [Google Scholar] [CrossRef]
- Delshad, V.; Borhani, F.; Khankeh, H.; Abbaszadeh, A.; Sabzalizadeh, S.; Moradian, M.J.; Behzadi, M.J.R.; Abadi, M.G.; Farzinnia, B. The effect of activating early warning system on motahari hospital preparedness. Health Emerg. Disasters Q. 2015, 1, 3–8. [Google Scholar]
- Amiri, M.; Chaman, R.; Raei, M.; Shirvani, S.D.N.; Afkar, A. Preparedness of hospitals in north of iran to deal with disasters. Iran. Red Crescent Med. J. 2013, 15, 519. [Google Scholar] [CrossRef] [Green Version]
- Daneshmandi, M.; Amiri, H.; Vahedi, M.; Farshi, M. Assessing level of Preparedness for disaster in hospitals of a selected medical sciences university-1388. J. Mil Med. 2010, 12, 167–171. [Google Scholar]
- Aladhrai, S.A.; Djalali, A.; Della Corte, F.; Alsabri, M.; El-Bakri, N.K.; Ingrassia, P.L. Impact of the 2011 revolution on hospital disaster preparedness in Yemen. Disaster Med. Public Health Prep. 2015, 9, 396–402. [Google Scholar] [CrossRef]
- Jama, T.J.; Kuisma, M.J. Preparedness of Finnish emergency medical services for chemical emergencies. Prehospital Disaster Med. 2016, 31, 392–396. [Google Scholar] [CrossRef] [Green Version]
- Christian, M.D.; Toltzis, P.; Kanter, R.K.; Burkle, F.M.; Vernon, D.D.; Kissoon, N. Treatment and triage recommendations for pediatric emergency mass critical care. Pediatr. Crit. Care Med. 2011, 12, S109–S119. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, K.; Khorram-Manesh, A.; Hertelendy, A.J.; Goniewicz, M.; Naylor, K.; Burkle, F.M., Jr. Current Response and Management Decisions of the European Union to the COVID-19 Outbreak: A Review. Sustainability 2020, 12, 3838. [Google Scholar] [CrossRef]
- Goniewicz, K.; Magiera, M.; Rucińska, D.; Pawłowski, W.; Burkle, F.M.; Hertelendy, A.J.; Goniewicz, M. Geographic Information System Technology: Review of the Challenges for Its Establishment as a Major Asset for Disaster and Emergency Management in Poland. Disaster Med. Public Health Prep. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dubas-Jakóbczyk, K.; Domagała, A.; Mikos, M. Impact of the doctor deficit on hospital management in Poland: A mixed-method study. Int. J. Health Plan. Manag. 2018. [Google Scholar] [CrossRef]
- Fox, J.H.; Burkle, F.M.; Bass, J.; Pia, F.A.; Epstein, J.L.; Markenson, D. The effectiveness of psychological first aid as a disaster intervention tool: Research analysis of peer-reviewed literature from 1990–2010. Disaster Med. Public Health Prep. 2012, 6, 247–252. [Google Scholar] [CrossRef]
- Smith, N.; Fraser, M. Straining the System: Novel Coronavirus (COVID-19) and Preparedness for Concomitant Disasters. Am J Public Health 2020, 110, 648–649. [Google Scholar] [CrossRef]
- Goniewicz, K.; Burkle, F.M. Challenges in implementing Sendai framework for disaster risk reduction in Poland. Int. J. Environ. Res. Public Health 2019, 16, 2574. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Average with a confidence interval of 95% for the evaluation of preparedness for mass-casualty incidents and disasters by occupation.
Figure 1.
Average with a confidence interval of 95% for the evaluation of preparedness for mass-casualty incidents and disasters by occupation.

Figure 2.
Average with a 95% confidence interval for the evaluation of preparedness for a mass-casualty incident or disaster for the current place of work, and one’s own preparedness.
Figure 2.
Average with a 95% confidence interval for the evaluation of preparedness for a mass-casualty incident or disaster for the current place of work, and one’s own preparedness.

Figure 3.
Average with a 95% confidence interval for evaluations of preparedness for mass-casualty incidents and disasters, categorized by participation in training related to preparation for such situations.
Figure 3.
Average with a 95% confidence interval for evaluations of preparedness for mass-casualty incidents and disasters, categorized by participation in training related to preparation for such situations.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Results of the analysis of correlation between the length of service of the respondents and the evaluation of preparedness for mass-casualty incidents and disasters.
Table 1.
Results of the analysis of correlation between the length of service of the respondents and the evaluation of preparedness for mass-casualty incidents and disasters.
| Length of Service | ||
|---|---|---|
| Evaluation of the preparedness of the current workplace for a mass-casualty incident or disaster | Spearman’s rho | 0.19 |
| significance | 0.033 | |
| Evaluation of one’s own preparedness for mass-casualty incidents or disasters | Spearman’s rho | 0.14 |
| significance | 0.108 |
Table 2.
Differences between the evaluation of preparedness for a mass-casualty incident or disaster in the current place of work, and the evaluation of one’s own preparedness.
Table 2.
Differences between the evaluation of preparedness for a mass-casualty incident or disaster in the current place of work, and the evaluation of one’s own preparedness.
| Current Place of Work | Own | t | p | 95% CI | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | LL | UL | |||
| Evaluation of preparedness for a mass-casualty incident or disaster | 4.10 | 1.68 | 5.71 | 2.14 | −9.28 | <0.001 | −1.95 | −1.27 |
M—mean; Me—median; SD—standard deviation; Bias.—bias; Kurt.—kurtosis; Min & Max.—the lowest and highest value of distribution; D—Kolmogorov–Smirnov test result; p—significance.
Table 3.
Differences between persons who have been involved in a mass-casualty incident or disaster as a healthcare worker, and persons who have not been involved in such an event in terms of their evaluation of preparedness for a mass-casualty incident or disaster.
Table 3.
Differences between persons who have been involved in a mass-casualty incident or disaster as a healthcare worker, and persons who have not been involved in such an event in terms of their evaluation of preparedness for a mass-casualty incident or disaster.
| Have You Ever Been Involved in a Mass-Casualty Incident or Disaster as a Healthcare Professional? | Z | p | ||||
|---|---|---|---|---|---|---|
| Yes (n = 34) | No (n = 100) | |||||
| Average Rank | Me | Average Rank | Me | |||
| Evaluation of the preparedness of the current workplace for a mass-casualty incident or disaster | 65.42 | 4.00 | 67.52 | 4.00 | −0.28 | 0.783 |
| Evaluation of one’s own preparedness for a mass-casualty incident or disaster | 86.12 | 7.00 | 61.17 | 5.00 | −3.27 | 0.001 |
M—mean; Me—median; SD—standard deviation; Bias.—bias; Kurt.—kurtosis; Min & Max.—the lowest and highest value of distribution; D—Kolmogorov–Smirnov test result; p—significance.
Table 4.
Differences in the evaluation of preparedness for a mass-casualty incident or disaster, depending on the organization of drills by the institution, and whether they were attended by the respondents.
Table 4.
Differences in the evaluation of preparedness for a mass-casualty incident or disaster, depending on the organization of drills by the institution, and whether they were attended by the respondents.
| Have There Been Any Disaster Management Drills Organized in the Facility Where you Currently Work? | ||||||||
|---|---|---|---|---|---|---|---|---|
| Yes (n = 60) | No (n = 73) | t | p | 95% CI | ||||
| M | SD | M | SD | LL | UL | |||
| Evaluation of the preparedness of the current workplace for a mass-casualty incident or disaster | 4.43 | 1.58 | 3.82 | 1.72 | 2.12 | 0.036 | 0.04 | 1.18 |
| Evaluation of one’s own preparedness for a mass-casualty incident or disaster | 6.49 | 1.67 | 5.11 | 2.33 | 3.99 | < 0.001 | 0.70 | 2.07 |
| Less than once every 3 years (n = 123) | Once every 3 years or more often (n = 11) | Z | p | |||||
| Average rank | Me | Average rank | Me | |||||
| Evaluation of the preparedness of the current workplace for a mass-casualty incident or disaster | 64.28 | 4.00 | 97.18 | 6.00 | −2.76 | 0.006 | ||
| Evaluation of one’s own preparedness for a mass-casualty incident or disaster | 66.19 | 6.00 | 82.18 | 7.00 | −1.32 | 0.186 | ||
M—mean; Me—median; SD—standard deviation; Bias.—bias; Kurt.—kurtosis; Min & Max.—the lowest and highest value of distribution; D—Kolmogorov–Smirnov test result; p—significance.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Goniewicz, K.; Goniewicz, M. Disaster Preparedness and Professional Competence Among Healthcare Providers: Pilot Study Results. Sustainability 2020, 12, 4931. https://0-doi-org.brum.beds.ac.uk/10.3390/su12124931
AMA Style
Goniewicz K, Goniewicz M. Disaster Preparedness and Professional Competence Among Healthcare Providers: Pilot Study Results. Sustainability. 2020; 12(12):4931. https://0-doi-org.brum.beds.ac.uk/10.3390/su12124931
Chicago/Turabian StyleGoniewicz, Krzysztof, and Mariusz Goniewicz. 2020. "Disaster Preparedness and Professional Competence Among Healthcare Providers: Pilot Study Results" Sustainability 12, no. 12: 4931. https://0-doi-org.brum.beds.ac.uk/10.3390/su12124931
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.