
Effectiveness of Social Prescribing Programs in the Primary Health-Care Context: A Systematic Literature Review

 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
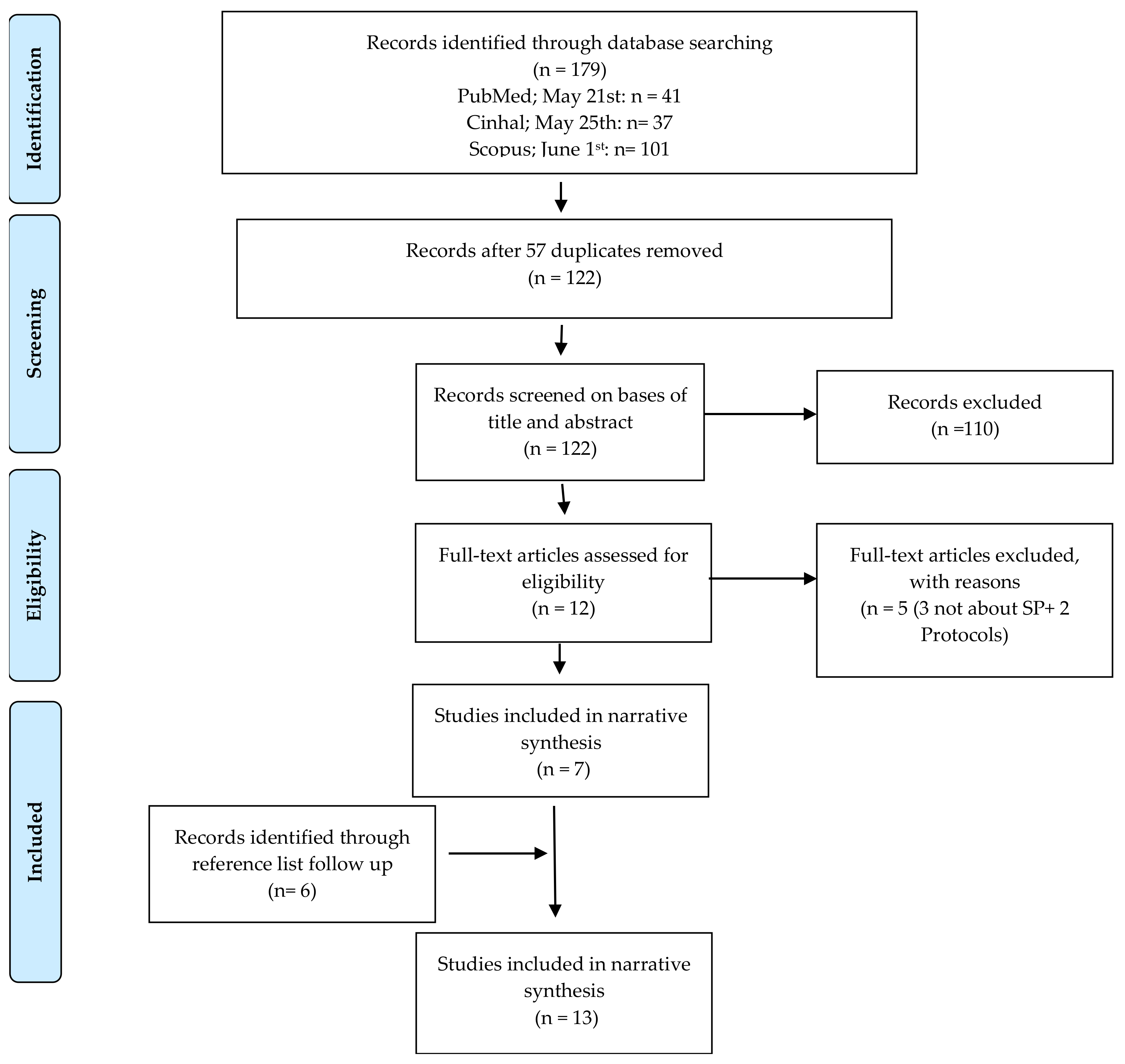
2. Materials and Methods
2.1. Study Design
2.2. Search Methods
2.3. Selection of Articles and Inclusion and Exclusion Criteria
2.4. Data Extraction, Quality Appraisal, and Data Synthesis
3. Results
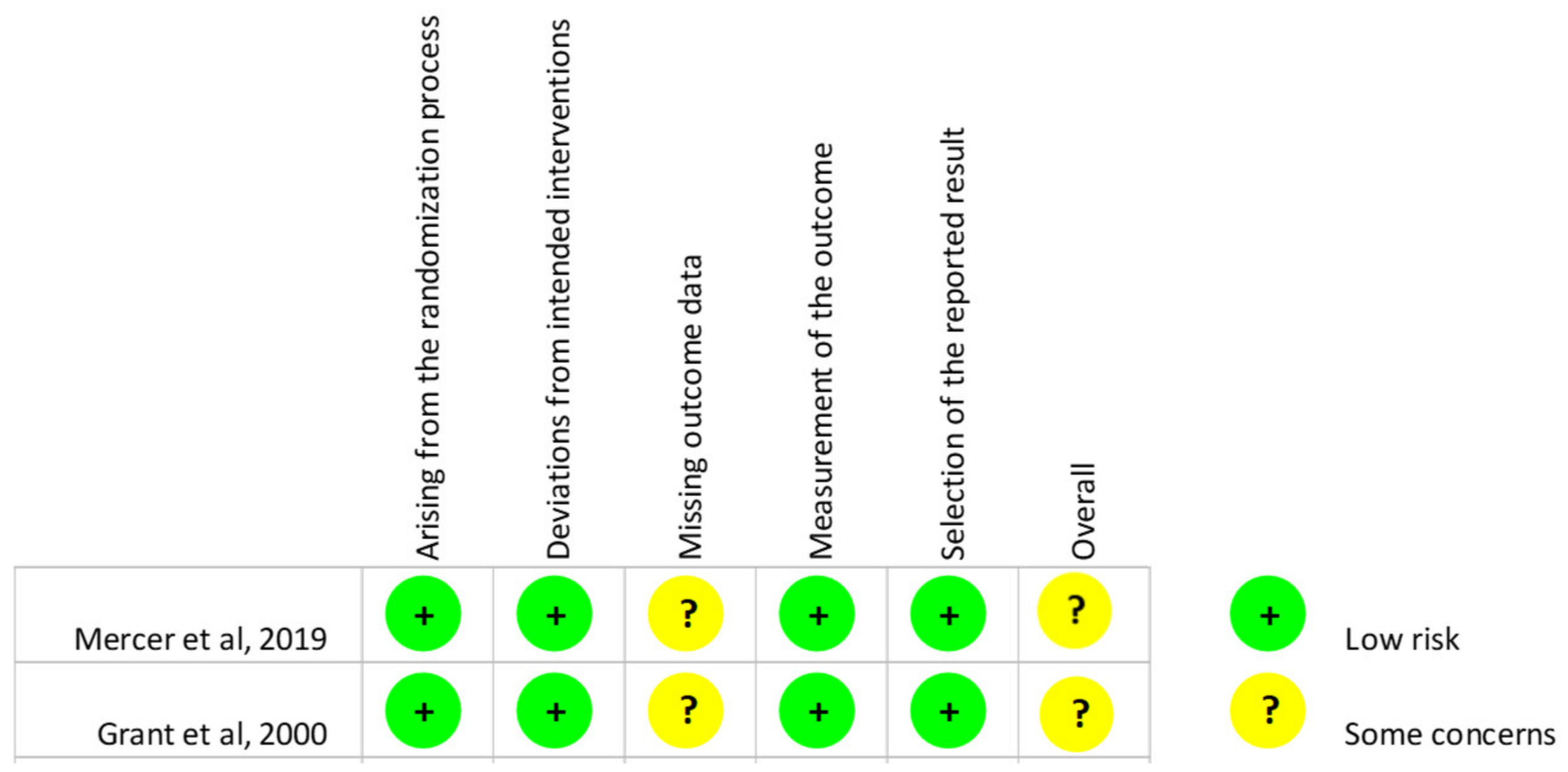
3.1. Quality of the Evidence
3.2. SP Domains and Results of the Effectiveness Assessment
4. Discussion
4.1. SP: Definition, Boundaries, and Key Elements
4.2. Main Findings Regarding Domains of Interventions
4.3. Main Findings Regarding Outcomes
4.4. Strengths and Limitations
4.5. Future Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Comprehensive Search Strategy of SRL
| Search | Query | PubMed Items Found | CINHAL Found | Scopus |
| #1 | “social prescribing” [Title/Abstract] | 125 | 133 | 159 |
| #2 | “social prescription” [Title/Abstract] | 23 | 16 | 85 |
| #3 | “community referral” [Title/Abstract] | 97 | 60 | 211 |
| #4 | “wellbeing program” OR “well being program” OR “well-being program” [Title/Abstract] | 131 | 42 | 236 |
| #5 | “Community prescribing” [Title/Abstract] OR “community prescription” [Title/Abstract] | 54 | 32 | 89 |
| #6 | “social referral” [Title/Abstract] | 4 | 2 | 31 |
| #7 | “non-medical referral” [Title/Abstract] | 0 | 4 | 5 |
| #8 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 | 415 | 274 | 781 |
| #9 | “link worker” [Title/Abstract] | 34 | 33 | 114 |
| #10 | “care navigators” [Title/Abstract] | 29 | 43 | 57 |
| #11 | #9 OR #10 | 63 | 76 | 169 |
| #12 | #8 OR #11 | 466 | 345 | 931 |
| #13 | “community care” [Title/Abstract] | 4677 | 3709 | 65,644 |
| #14 | “primary care” [Title/Abstract] OR “primary-care” [Title/Abstract] | 114,652 | 73,391 | 135,678 |
| #15 | “primary health services” [Title/Abstract] | 340 | 173 | 631 |
| #16 | general practice [Title/Abstract] | 37,966 | 16,537 | 110,772 |
| #17 | primary health care [Title/Abstract] OR “primary healthcare” [Title/Abstract] | 32,179 | 15,804 | 110,713 |
| #18 | “community activities” [Title/Abstract] | 672 | 506 | 2,173 |
| #19 | #13 OR #14 OR #15 OR #16 OR #17 OR #18 | 174,316 | 101,311 | 345,138 |
| #20 | #12 AND #19 | 98 | 90 | 215 |
| #21 | #20 AND trial [Title/Abstract] | 11 | 10 | 19 |
| #22 | #20 AND RCT [Title/Abstract] | 1 | 1 | 3 |
| #23 | #20 AND controlled [Title/Abstract] | 8 | 7 | 41 |
| #24 | #20 AND effectiveness [Title/Abstract] | 18 | 10 | 31 |
| #25 | #20 AND efficacy [Title/Abstract] | 2 | 1 | 4 |
| #26 | #20 AND evaluation [Title/Abstract] | 26 | 23 | 52 |
| #27 | #20 AND (# 21 OR #22 OR #23 OR #24 OR #25 OR #26) | 41 | 37 | 101 |
References
- Crimmins, E.M. Lifespan and Healthspan: Past, Present, and Promise. Gerontologist 2015, 55, 901–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLeod, S.; Schwebke, K.; Hawkins, K.; Ruiz, J.; Hoo, E.; Yeh, C.S. Need for Comprehensive Health Care Quality Measures for Older Adults. Popul. Health Manag. 2018, 21, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Finlay, J.M.; Kobayashi, L.C. Social isolation and loneliness in later life: A parallel convergent mixed-methods case study of older adults and their residential contexts in the Minneapolis metropolitan area, USA. Soc. Sci. Med. 2018, 208, 25–33. [Google Scholar] [CrossRef]
- The Sustainable Development Agenda—United Nations Sustainable Development. Available online: https://www.un.org/sustainabledevelopment/development-agenda/ (accessed on 10 October 2020).
- Costa, A.; Lopes, J.; Seabra, P.; Henriques, A.; Alarcão, V.; Virgolino, A.; Nogueira, P.; Arriaga, M. Is there a link between Social Prescribing and touristic activities involving older individuals: Insights from a scoping review. In Creative Tourism Dynamics: Connecting Travellers, Communities, Cultures and Places; Coimbra Editora: Coimbra, Portugal, 2020; pp. 49–64. [Google Scholar]
- Norris, S.L.; Rehfuess, E.A.; Smith, H.; Tunçalp, Ö.; Grimshaw, J.M.; Ford, N.P.; Portela, A. Complex health interventions in complex systems: Improving the process and methods for evidence-informed health decisions. BMJ Glob. Health 2019, 4, e000963. [Google Scholar] [CrossRef]
- Woolf, S.H.; Aron, L. Health in International Perspective: Shorter Lives, Poorer Health. In Physical and Social Environmental Factors; National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Office of Disease Prevention and Health Promotion NWS-10.4 Data Details—Healthy People. Available online: http://www.healthypeople.gov/2020/topicsobjectives2020/DataDetails.aspx?hp2020id=NWS-10.4 (accessed on 11 May 2014).
- De Silva, M.J.; McKenzie, K.; Harpham, T.; Huttly, S.R.A. Social capital and mental illness: A systematic review. J. Epidemiol. Community Health 2005, 59, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Pilkington, K.; Loef, M.; Polley, M.; Simmons, R.; Portillo, M.C. Searching for Real-World Effectiveness of Health Care Innovations: Scoping Study of Social Prescribing for Diabetes. J. Med Internet Res. 2017, 19, e20. [Google Scholar] [CrossRef] [Green Version]
- Pescheny, J.; Randhawa, G.; Pappas, Y. Patient uptake and adherence to social prescribing: A qualitative study. BJGP Open 2018, 2, 101598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2020, 28, 309–324. [Google Scholar] [CrossRef] [Green Version]
- Polley, M.J.; Fleming, J.; Anfilogoff, T.; Carpenter, A. Making Sense of Social Prescribing; University of Westminster: London, UK, 2017. [Google Scholar]
- Fancourt, D.; Steptoe, A.; Cadar, D. Community engagement and dementia risk: Time-to-event analyses from a national cohort study. J. Epidemiol. Community Health 2020, 74, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Torjesen, I. Social prescribing could help alleviate pressure on GPs. BMJ 2016, 352, i1436. [Google Scholar] [CrossRef] [PubMed]
- NHS England » Social Prescribing in Practice. Available online: https://www.england.nhs.uk/personalisedcare/upc/comprehensive-model/case-studies/social-prescribing-in-practice/ (accessed on 10 October 2020).
- Bickerdike, L.; Booth, A.; Wilson, P.M.; Farley, K.; Wright, K. Social prescribing: Less rhetoric and more reality. A systematic review of the evidence. BMJ Open 2017, 7, e013384. [Google Scholar] [CrossRef]
- NHS England NHS England » Social Prescribing. Available online: https://www.england.nhs.uk/contact-us/privacy-notice/how-we-use-your-information/public-and-partners/social-prescribing/ (accessed on 11 October 2020).
- Fixsen, A.; Seers, H.; Polley, M.; Robins, J. Applying critical systems thinking to social prescribing: A relational model of stakeholder “buy-in. ” BMC Health Serv. Res. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Woodall, J.; Trigwell, J.; Bunyan, A.-M.; Raine, G.; Eaton, V.; Davis, J.; Hancock, L.; Cunningham, M.; Wilkinson, S. Understanding the effectiveness and mechanisms of a social prescribing service: A mixed method analysis. BMC Health Serv. Res. 2018, 18, 604. [Google Scholar] [CrossRef] [Green Version]
- Maughan, D.L.; Patel, A.; Parveen, T.; Braithwaite, I.; Cook, J.; Lillywhite, R.; Cooke, M. Primary-care-based social prescribing for mental health: An analysis of financial and environmental sustainability. Prim. Health Care Res. Dev. 2016, 17, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Risk of Bias Tools. Available online: https://www.riskofbias.info/ (accessed on 26 January 2021).
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 26 January 2021).
- Pescheny, J.V.; Gunn, L.H.; Randhawa, G.; Pappas, Y. The impact of the Luton social prescribing programme on energy expenditure: A quantitative before-and-after study. BMJ Open 2019, 9, e026862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumner, R.C.; Crone, D.M.; Baker, C.; Hughes, S.; Loughren, E.A.; James, D.V.B. Factors associated with attendance, engagement and wellbeing change in an arts on prescription intervention. J. Public Health 2020, 42, E89–E96. [Google Scholar] [CrossRef]
- Prior, F.; Coffey, M.; Robins, A.; Cook, P. Long-Term Health Outcomes Associated With an Exercise Referral Scheme: An Observational Longitudinal Follow-Up Study. J. Phys. Act. Health 2019, 16, 288–293. [Google Scholar] [CrossRef]
- Mercer, S.W.; Fitzpatrick, B.; Grant, L.; Chng, N.R.; McConnachie, A.; Bakhshi, A.; James-Rae, G.; O’Donnell, C.A.; Wyke, S. Effectiveness of Community-Links Practitioners in Areas of High Socioeconomic Deprivation. Ann. Fam. Med. 2019, 17, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Carnes, D.; Sohanpal, R.; Frostick, C.; Hull, S.; Mathur, R.; Netuveli, G.; Tong, J.; Hutt, P.; Bertotti, M. The impact of a social prescribing service on patients in primary care: A mixed methods evaluation. BMC Health Serv. Res. 2017, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kellezi, B.; Wakefield, J.R.H.; Stevenson, C.; McNamara, N.; Mair, E.; Bowe, M.; Wilson, I.; Halder, M.M. The social cure of social prescribing: A mixed-methods study on the benefits of social connectedness on quality and effectiveness of care provision. BMJ Open 2019, 9, e033137. [Google Scholar] [CrossRef] [Green Version]
- Halder, M.M.; Wakefield, J.R.; Bowe, M.; Kellezi, B.; Mair, E.; McNamara, N.; Wilson, I.; Stevenson, C. Evaluation and exploration of a social prescribing initiative: Study protocol. J. Health Psychol. 2018, 26, 345–356. [Google Scholar] [CrossRef] [Green Version]
- Loftus, A.; McCauley, F.; McCarron, M. Impact of social prescribing on general practice workload and polypharmacy. Public Health 2017, 148, 96–101. [Google Scholar] [CrossRef]
- Morton, L.; Ferguson, M.; Baty, F. Improving wellbeing and self-efficacy by social prescription. Public Health 2015, 129, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Grayer, J.; Cape, J.; Orpwood, L.; Leibowitz, J.; Buszewicz, M. Facilitating access to voluntary and community services for patients with psychosocial problems: A before-after evaluation. BMC Fam. Pr. 2008, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Grant, C.; Goodenough, T.; Harvey, I.; Hine, C. A randomised controlled trial and economic evaluation of a referrals facilitator between primary care and the voluntary sector. BMJ 2000, 320, 419–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelpoel, N.; Jarrold, K. Social prescription and the role of participatory arts programmes for older people with sensory impairments. J. Integr. Care 2014, 22, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Van De Venter, E.; Buller, A. Arts on referral interventions: A mixed-methods study investigating factors associated with differential changes in mental well-being. J. Public Health 2015, 37, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moffatt, S.; Steer, M.; Lawson, S.; Penn, L.; O’Brien, N. Link Worker social prescribing to improve health and well-being for people with long-term conditions: Qualitative study of service user perceptions. BMJ Open 2017, 7, e015203. [Google Scholar] [CrossRef] [Green Version]
- Sims-Gould, J.; McKay, H.A.; Hoy, C.L.; Nettlefold, L.; Gray, S.M.; Lau, E.Y.; Bauman, A. Factors that influence implementation at scale of a community-based health promotion intervention for older adults. BMC Public Health 2019, 19, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Petticrew, M. When are complex interventions ‘complex’? When are simple interventions ‘simple’? Eur. J. Public Health 2011, 21, 397–398. [Google Scholar] [CrossRef]
- Minary, L.; Trompette, J.; Kivits, J.; Cambon, L.; Tarquinio, C.; Alla, F. Which design to evaluate complex interventions? Toward a methodological framework through a systematic review. BMC Med Res. Methodol. 2019, 19, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, A.; Bonde, L.O. The use of arts interventions for mental health and wellbeing in health settings. Perspect. Public Health 2018, 138, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.; Ramos, S.; Ferreira, A.R.; Montalvão, J.; Ribeiro, I.; Lima, F. A efetividade do exercício físico no tratamento da depressão. Rev. Port. Enferm. Saúde Ment. 2019, 58–64. [Google Scholar] [CrossRef]
- Bhuyan, K.K. Health promotion through self-care and community participation: Elements of a proposed programme in the developing countries. BMC Public Health 2004, 4, 1–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, A.J. Enhancing Self-efficacy for Optimized Patient Outcomes through the Theory of Symptom Self-management. Cancer Nurs. 2013, 36, E16–E26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among Older People. BioMed Res. Int. 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Sohn, H.; Tucker, A.; Ferguson, O.; Gomes, I.; Dowdy, D. Costing the implementation of public health interventions in resource-limited settings: A conceptual framework. Implement. Sci. 2020, 15, 86. [Google Scholar] [CrossRef]
- Dayson, C.; Bashir, N. The Social and Economic Impact of the Rotherham Social Prescribing Pilot Main Evaluation Report; Sheffield Hallam University: Sheffield, UK, 2014. [Google Scholar]



{kind=link}
{kind=link}
| Author, Year | Study Design | Country, Region | Target Population | Social Context | Social Prescribing Approaches |
|---|---|---|---|---|---|
| Pescheny et al., 2019 [25] | Observational non-controlled before-and-after study | UK, Luton | Patients who health professionals thought would benefit from the program | A deprived area with a large ethnic minority population | “Enabling healthcare professionals to refer patients to a link worker, to co-design a non-clinical social prescription to improve their health and wellbeing” (p. 2) |
| Sumner et al., 2019 [26] | Observational non-controlled before-and-after study | UK, South West of England | Patients experiencing anxiety, depression, or stress; low self-esteem and/or confidence, or overall reduced wellbeing; stress from chronic illness or pain; in need of distraction from behavior-related health issues; or who had experienced a recent major life change or loss | Community mostly with caucasian people, with variable level of deprivation, between medium and very low quintile of Indice of Multiple Deprivation | “Arts on prescription (AoP) is a type of social prescription that refers patients to participate in courses of art” (p. 2) |
| Prior et al., 2019 [27] | Observational non-controlled before-and-after study, with a longer follow up | UK, borough of Tameside | Users aged ≥18 years, identified as inactive with a chronic health condition or significant health risk factors | Region with health inequalities and high levels of chronic health conditions and physical inactivity | “One approach to Physical Activity promotion has been exercise referral schemes, a form of nonmedical intervention or ‘social prescription’.” (p. 1) |
| Mercer et al., 2019 [28] | Quasi-experimental cluster-randomized controlled trial | UK, Glasgow, Scotland | Users > 18 years old | Area of high socioeconomic deprivation | “… aims to link patients to non-medical sources of support within a community, thus expanding options and resources beyond those traditionally provided in primary health care” (p. 1) |
| Carnes et al., 2017 [29] | Mixed-methods study, with a matched control group | UK, London Borough of City and Hackney | Users in general practices who were frequent attenders and/or socially isolated | Area with extreme range of socio-economic deprivation and affluence and a considerable ethnic mix | “a non-medical referral, or linking service, to help people identify their social needs and develop ‘well-being’ action plans to promote, establish or re-establish integration and support in their communities, with the aim of improving personal well-being” (p. 2) |
| Kellezi et al., 2019 [30] | Mixed-methods study | UK, English East Midlands | Above 18 years and that were managing one or more long-term health conditions and feel isolated, lonely, or anxious | Relatively affluent suburban area that experienced much lower levels of crime/deprivation than nearby urban areas | “A non-clinical approach designed to support individuals experiencing chronic mental/physical health problems exacerbated by loneliness, often leading to increased health-care appointment attendance (…) As the name would suggest, SP also has a strong social element: it involves health professionals encouraging patients to join voluntary, community and social enterprise groups within the third-sector” (p. 2 of study protocol [31]) |
| Woodall et al., 2018 [20] | Mixed-methods study | UK, Northern England | Above 14 years old | Area with a strong third sector infrastructure which enabled service users to be supported | “To harness assets within the voluntary and community sectors to improve and encourage self-care and facilitate health-creating communities” (p. 2) |
| Loftus et al., 2017 [32] | Observational non-controlled before-and-after study | UK, Northern Ireland | Patients over 65 years of age with a chronic condition who attended their GP frequently or had multiple medications | Not reported | “…clear, coherent and collaborative process in which health-care practitioners work with patients and service users to select and make referrals to community based services” (p. 97) |
| Morton et al., 2015 [33] | Mixed-methods study | UK, not specified | Patients who experienced mild to moderate mental health difficulties such as anxiety/stress, depression, and low self-esteem | Not reported | “… involves GP’s and other health professionals ‘prescribing’ supportive activities such as: arts and crafts, leisure, stress management, cultural, educational or environmental activities within the patients’ community.” (p. 286) |
| Grayer et al., 2008 [34] | Observational non-controlled before-and-after study | UK, not specified | Patients with psychosocial problems (anxiety, depression, social problems, isolation, housing, financial difficulties) | Not reported | Not defined as SP interventions |
| Grant et al., 2000 [35] | Randomized controlled trial | UK, Avon | Patients (16+ years old) with varied socioeconomic characteristics with psychosocial problems (mostly with mental health problems) | Not reported | Authors do not refer to SP specifically, although the intervention used matches specifications of SP by definition (patients are randomly referred to a voluntary sector organization with the mediation of the Amalthea Project) |
| Vogelpoel et al., 2014 [36] | Mixed-methods study | UK, not specified | Older patients experiencing social isolation and associated health problems who have single or multi-sensory impairment | Not reported | Authors do not provide a clear definition for SP as they refer to social prescribing: “Integrated care approaches (…) can function as a preventative and health-promoting service where practical implications of current and emerging policy guidelines can come to fruition. (…) linking patients accessing primary care with non-medical support services in the community, are an example of integration across sectors and a more holistic alternative to prescription medication.” (p. 41) |
| Van de Venter et al., 2014 [37] | Mixed-methods study | UK, not specified | People with mild-to-moderate mental health problems | Not reported | Instead of SP, the authors use the expression Arts-on-referral (AoR) schemes |
| Authors, Year | Sample Size | Mean Age (Years) | Gender (% Female) | SP Activity (Domains) | SP Intervention | Outcomes (Instruments) | Main Findings |
|---|---|---|---|---|---|---|---|
| Pescheny et al., 2019 [25] | 146 | 51.2 | 70.4 | Art, physical activity, social interaction, and personal development | Intervention: 12 sessions Post-intervention assessment: after 12 sessions Follow up: no | IPAQ | Positive and significant improvement in physical activity |
| Sumner et al., 2019 [26] | 1297 | 51.1 | 77.3 | Arts | Intervention: 8–10 weeks Post-intervention assessment: last day of intervention Follow up: no | WEMWBS | Attendance and engagement, resulted in increased wellbeing for those that engaged and completed the intervention. A lower rate of attendance was found when wellbeing score was lower at baseline |
| Prior et al., 2019 [27] | 273 | 57.7 | 56.0 | Physical activity | Intervention: 24 weeks Post-intervention assessment: 24 weeks Follow up: 52 weeks after the beginning | IPAQ; EQ-5D-3L; EQ-5D VAS; WMWBS; BMI, BP, alcohol and tobacco consumption | Improvements in physical activity over the first 6 months; maintained in the long term (≥12 months). Significant improvements in body composition, systolic blood pressure, quality of life, and mental wellbeing |
| Mercer et al., 2019 [28] | 900 (Intervention Group: 288; Control Group: 612) | Intervention Group: 49.0; Control Group: 56.0 | Intervention Group: 59.2; Control Group: 61.1 | Art, physical activity, social interaction, and personal development | Intervention: flexible Post-intervention assessment: 9 months after the beginning Follow up: no | WEMWBS; EQ-5D-3L; HADS; Work and Social Adjustment Scale, burden of multi-morbidity, and self-reported lifestyle activities | Unable to prove the effectiveness of referral to LW |
| Carnes et al., 2017 [29] | 486 (Intervention Group:184 Control Group:302) | Intervention Group: 56.0; Control Group: 58.0 | Intervention Group: 46.0; Control Group: 54.0 | Physical activities, social interaction activities; personal development, cultural activities, religious activities | Intervention: not reported Post-intervention assessment: 8 months after the beginning of the program Follow up: no | General health score; HADS; Active engagement in life score; Number of regular activities Accident and Emergency visits. | No differences between patients referred (SP) and controls, for depression, anxiety or positive and active engagement in life. No effects in prescribed medical drugs. Number of prescribed medical drugs significantly higher for those referred into SP (before and after the intervention). |
| Kellezi et al., 2019 [30] | 630 | 52.7 | 53.5 | Not specified | Intervention: up to 8 weeks Post-intervention assessment: 4 month after initial referral assessment Follow up: no | Community belonging; ULS-8; number of times they have used primary care | Methodological triangulation offered conclusions that ‘social cure’ processes explained the efficacy of SP. Social prescription was found to reduce primary care usage through increasing social connectedness and reducing loneliness. |
| Woodall et al., 2018 [20] | 342 | 53.1 | 63.9 | Art activities, physical activities, social interaction activities, and personal development | Intervention: On average, 6 sessions Post-intervention assessment: not reported Follow up: no | WMWBS; EQ-5D-3L; Campaign to End Loneliness Measurement Tool | Improvements in wellbeing, perceived health and social connectedness, and reduction of anxiety. |
| Loftus et al., 2017 [32] | 68 | 72.9 | 70.6 | Art activities, physical activities, social interaction activities, technological and technical activities; and personal development | Intervention: 12 weeks Post-intervention assessment: after 12 weeks (6–12 months after the end of the activity) Follow up: no | Routinely collected health data, according to RECORD guidelines | Improvement of patients’ self-esteem and wellbeing. Small effect on GP workload |
| Morton et al., 2015 [33] | 136 | 52.0 | 72.8 | Art activities, and personal development | Intervention: not reported Post-intervention assessment: not specified Follow up: no | HADS; GSE; WEMWBS | Positive improvements in all scales |
| Grayer et al., 2008 [34] | 108 | 43.1 | 62.0 | Educational, recreational and voluntary sector resources | Intervention: not reported Post-intervention assessment: 3 months after the initial appointment in community services Follow up: no | GHQ12; COREOM; WSAS; CSQ; Community Link Evaluation; Measurement of Primary care resources uses | Reduction of percentage of patients with mental health problem.Improvement in social adjustmentReduction of number of primary health-care consultations and of psychotropic medication Clinical changes accompanied by improvements in work and social adjustment scores. |
| Grant et al., 2000 [35] | 161 (Intervention Group:90; Control Group: 71) | Intervention Group: 40.8; Control Group: 45.6 | Intervention Group: 72.0; Control Group: 79.0 | Different areas of intervention (according to the voluntary sector association) | Intervention: not reported Post-intervention assessment: 1 month after the end of the intervention Follow up: 4 months after the end of the intervention | HADS; DUKE-UNC functional social support scale; COOP/WONCA functional health assessment charts; Delighted-terrible faces scale; Health-economic and process measures | Improvements in anxiety, other emotional feelings, ability to carry out everyday activities, feelings about general health, and quality of life. No difference for depression or perceived social support. Costs to NHS were greater in intervention arm |
| Vogelpoel et al., 2014 [36] | 12 | 80.0 | 75.0 | Arts | Intervention: 12 weeks Post-intervention assessment: In last session Follow up: no | WEMWBS; Thiele and Marsden’s. Dynamic Observation scale; Semi-structured interviews | Benefits for wellbeing. Increased self-confidence, development of new friendships, increased mental wellbeing and reduced social isolation, |
| van de Venter et al., 2014 [37] | 44 | 43.0 | 82.0 | Arts | Intervention: 20 weeks Post-intervention assessment: not reported Follow up: no | WEMWBS | Improvements in wellbeing |
| Criteria | Yes | No | NR/NA a |
|---|---|---|---|
| 1. Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | x | ||
| 2. Was the method of randomization adequate (i.e., use of randomly generated assignment)? | x | ||
| 3. Was the treatment allocation concealed (so that assignments could not be predicted)? | x | ||
| 4. Were study participants and providers blinded to treatment group assignment? | x | ||
| 5. Were the people assessing the outcomes blinded to the participants’ group assignments? | x | ||
| 6. Were the groups similar at baseline on important characteristics that could affect outcomes (e.g., demographics, risk factors, co-morbid conditions)? | x | ||
| 7. Was the overall drop-out rate from the study at endpoint 20% or lower than the number allocated to treatment? | x | ||
| 8. Was the differential drop-out rate (between treatment groups) at endpoint 15 percentage points or lower? | x | ||
| 9. Was there high adherence to the intervention protocols for each treatment group? | x | ||
| 10. Were other interventions avoided or similar in the groups (e.g., similar background treatments)? | x | ||
| 11. Were outcomes assessed using valid and reliable measures that were implemented consistently across all study participants? | x | ||
| 12. Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | x | ||
| 13. Were outcomes reported or subgroups analyzed prespecified (i.e., identified before analyses were conducted)? | x | ||
| 14. Were all randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | x |
| Study Question or Objective Clearly Stated | Eligibility/Selection Criteria for the Study Population Prespecified and Clearly Described | Participants in the Study Were Representative of Those Who Would Be Eligible for the SP Intervention | Eligible Participants Were All Enrolled | The Sample Size Was Sufficiently Large | The SP Intervention Was Clearly Described and Delivered Consistently | The Outcome Measures Were Pre-Specified, Clearly Defined, Valid, Reliable, and Assessed Consistently | Outcomes Were Assessed Blindly | The Loss to Follow-Up after Baseline Was 20% or Less | Were Those Lost to Follow-Up Accounted for in the Analysis? | The Statistical Methods Examine Changes in Outcome Measures from before to after the Intervention AND Statistical Tests Provided p Values for the Pre-To-Post Changes | Outcome Measures Were Taken Multiple Times Before the Intervention and Multiple Times after the Intervention | If the Intervention Was Conducted at a Group Level (e.g., a Health Unit, a Community, Etc.), the Statistical Analysis Took into Account the Use of Individual-Level Data to Determine Effects at the Group Level | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pescheny et al., 2019 | yes | NR | no | NR | yes | no | yes | no | no | no | yes | no | NA |
| Notes | Eligibility/selection criteria were not clearly described | ||||||||||||
| Sumner et al., 2019 | yes | no | no | NR | yes | yes | yes | no | no | no | yes | no | NA |
| Notes | Eligibility/selection criteria were not clearly described. Sample was large, providing a strong statistical power | ||||||||||||
| Prior et al., 2019 | yes | yes | no | no | yes | yes | yes | no | no | no | yes | yes | NA |
| Notes | The study reported in this paper has a follow up at week 52 | ||||||||||||
| Kellezi et al., 2019 | yes | yes | no | no | yes | no | yes | no | no | no | yes | no | NA |
| Woodall et al., 2018 | yes | no | no | no | yes | no | yes | no | no | no | yes | no | NA |
| Loftus et al., 2017 | yes | yes | no | no | no | yes | yes | no | yes | yes | yes | no | NA |
| Morton et al., 2015 | no | no | no | no | yes | no | yes | no | no | no | yes | no | NA |
| Grayer et al., 2008 | yes | yes | no | no | no | no | yes | no | yes | no | yes | no | NA |
| Vogelpoel et al., 2014 | yes | yes | no | no | no | yes | yes | no | yes | no | yes | no | NA |
| van de Venter et al., 2014 | yes | no | no | no | no | yes | yes | no | yes | no | yes | no | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, A.; Sousa, C.J.; Seabra, P.R.C.; Virgolino, A.; Santos, O.; Lopes, J.; Henriques, A.; Nogueira, P.; Alarcão, V. Effectiveness of Social Prescribing Programs in the Primary Health-Care Context: A Systematic Literature Review. Sustainability 2021, 13, 2731. https://0-doi-org.brum.beds.ac.uk/10.3390/su13052731
Costa A, Sousa CJ, Seabra PRC, Virgolino A, Santos O, Lopes J, Henriques A, Nogueira P, Alarcão V. Effectiveness of Social Prescribing Programs in the Primary Health-Care Context: A Systematic Literature Review. Sustainability. 2021; 13(5):2731. https://0-doi-org.brum.beds.ac.uk/10.3390/su13052731
Chicago/Turabian StyleCosta, Andreia, C Joana Sousa, Paulo Rosário Carvalho Seabra, Ana Virgolino, Osvaldo Santos, Joaquim Lopes, Adriana Henriques, Paulo Nogueira, and Violeta Alarcão. 2021. "Effectiveness of Social Prescribing Programs in the Primary Health-Care Context: A Systematic Literature Review" Sustainability 13, no. 5: 2731. https://0-doi-org.brum.beds.ac.uk/10.3390/su13052731