Knowledge, Attitudes and Perceptions of Immigrant Parents Towards Human Papillomavirus (HPV) Vaccination: A Systematic Review

 , and
, and
Abstract
:1. Introduction
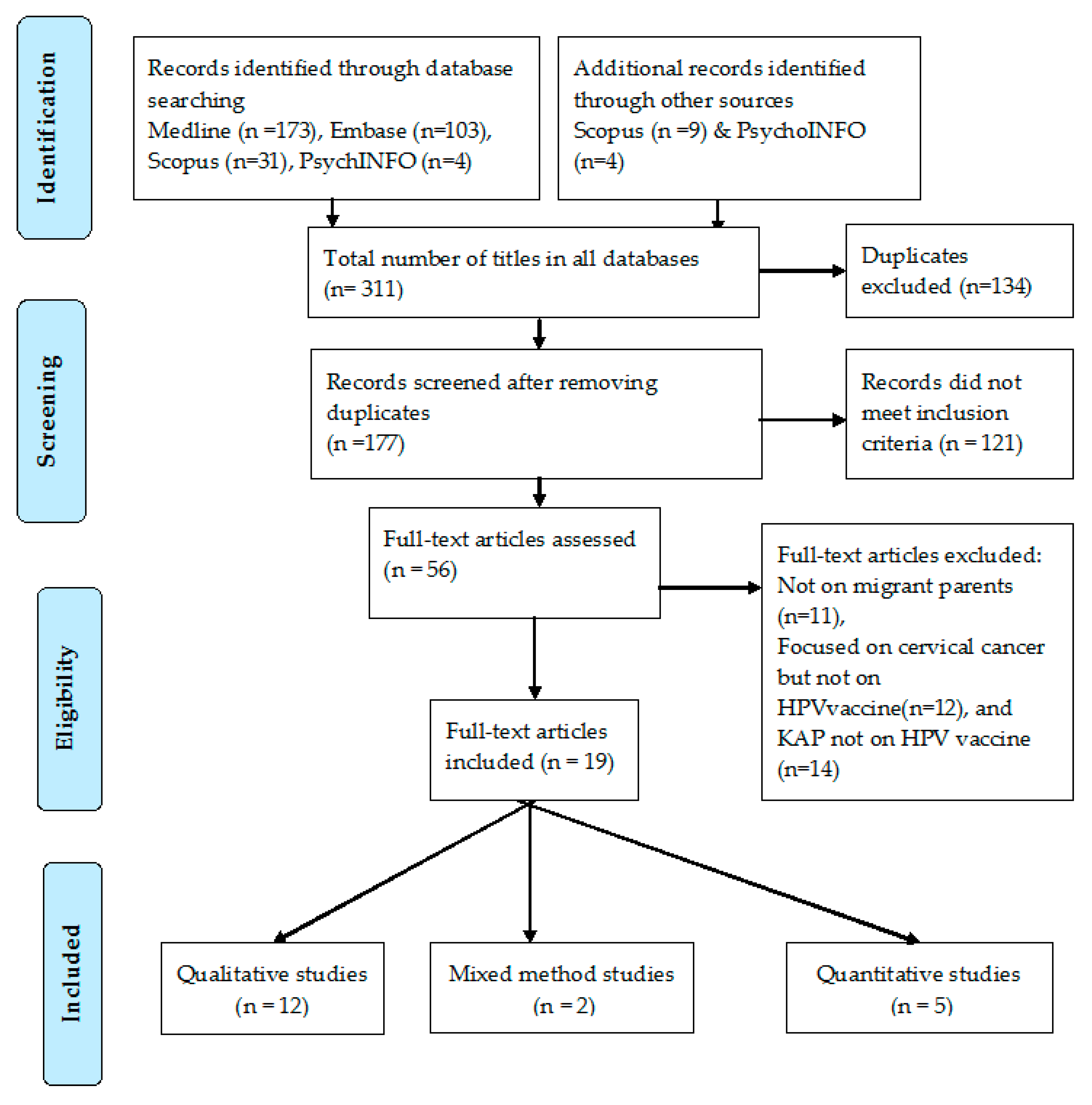
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martins, T.R.; Mendes de Oliveira, C.; Rosa, L.R.; de Campos Centrone, C.; Rodrigues, C.L.; Villa, L.L.; Levi, J.E. HPV genotype distribution in Brazilian women with and without cervical lesions: Correlation to cytological data. Virol. J. 2016, 13, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocjan, B.J.; Bzhalava, D.; Forslund, O.; Dillner, J.; Poljak, M. Molecular methods for identification and characterization of novel papillomaviruses. Clin. Microbiol. Infect. 2015, 21, 808–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, H.; Donovan, B.; Wand, H.; Read, T.R.; Regan, D.G.; Grulich, A.E.; Fairley, C.K.; Guy, R.J. Genital warts in young Australians five years into national human papillomavirus vaccination programme: National surveillance data. Bmj 2013, 346, f2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monsonego, J.; Bosch, F.X.; Coursaget, P.; Cox, J.T.; Franco, E.; Frazer, I.; Sankaranarayanan, R.; Schiller, J.; Singer, A.; Wright, T.C., Jr.; et al. Cervical cancer control, priorities and new directions. Int. J. Cancer 2004, 108, 329–333. [Google Scholar] [CrossRef]
- Achampong, Y.; Kokka, F.; Doufekas, K.; Olaitan, A. Prevention of Cervical Cancer. J. Cancer Ther. 2018, 9, 10. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Bosch, F.X.; Burchell, A.N.; Schiffman, M.; Giuliano, A.R.; de Sanjose, S.; Bruni, L.; Tortolero-Luna, G.; Kjaer, S.K.; Munoz, N. Epidemiology and natural history of human papillomavirus infections and type-specific implications in cervical neoplasia. Vaccine 2008, 26 (Suppl. 10), K1-16. [Google Scholar] [CrossRef]
- Paz-Zulueta, M.; Alvarez-Paredes, L.; Rodriguez Diaz, J.C.; Paras-Bravo, P.; Andrada Becerra, M.E.; Rodriguez Ingelmo, J.M.; Ruiz Garcia, M.M.; Portilla, J.; Santibanez, M. Prevalence of high-risk HPV genotypes, categorised by their quadrivalent and nine-valent HPV vaccination coverage, and the genotype association with high-grade lesions. BMC Cancer 2018, 18, 112. [Google Scholar] [CrossRef]
- Brotherton, J.M.; Gertig, D.M.; May, C.; Chappell, G.; Saville, M. HPV vaccine impact in Australian women: Ready for an HPV-based screening program. Med. J. Aust. 2016, 204, 184. [Google Scholar] [CrossRef] [Green Version]
- Cervantes, J.L.; Doan, A.H. Discrepancies in the evaluation of the safety of the human papillomavirus vaccine. Mem. Inst. Oswaldo Cruz. 2018, 113, e180063. [Google Scholar] [CrossRef]
- Garland, S.M.; Paavonen, J.; Jaisamrarn, U.; Naud, P.; Salmeron, J.; Chow, S.N.; Apter, D.; Castellsague, X.; Teixeira, J.C.; Skinner, S.R.; et al. Prior human papillomavirus-16/18 AS04-adjuvanted vaccination prevents recurrent high grade cervical intraepithelial neoplasia after definitive surgical therapy: Post-hoc analysis from a randomized controlled trial. Int. J. Cancer 2016, 139, 2812–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garland, S.M.; Cornall, A.M.; Brotherton, J.M.L.; Wark, J.D.; Malloy, M.J.; Tabrizi, S.N. Final analysis of a study assessing genital human papillomavirus genoprevalence in young Australian women, following eight years of a national vaccination program. Vaccine 2018, 36, 3221–3230. [Google Scholar] [CrossRef] [PubMed]
- Brotherton, J.M.L.; Bloem, P.N. Population-based HPV vaccination programmes are safe and effective: 2017 update and the impetus for achieving better global coverage. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 42–58. [Google Scholar] [CrossRef]
- Taberna, M.; Mena, M.; Pavon, M.A.; Alemany, L.; Gillison, M.L.; Mesia, R. Human papillomavirus-related oropharyngeal cancer. Ann. Oncol. 2017, 28, 2386–2398. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, K.E.; LaMontagne, D.S.; Watson-Jones, D. Status of HPV vaccine introduction and barriers to country uptake. Vaccine 2018, 36, 4761–4767. [Google Scholar] [CrossRef]
- Lee, V.Y.; Booy, R.; Skinner, R.; Edwards, K.M. The effect of exercise on vaccine-related pain, anxiety and fear during HPV vaccinations in adolescents. Vaccine 2018, 36, 3254–3259. [Google Scholar] [CrossRef]
- Markowitz, L.E.; Tsu, V.; Deeks, S.L.; Cubie, H.; Wang, S.A.; Vicari, A.S.; Brotherton, J.M. Human papillomavirus vaccine introduction—The first five years. Vaccine 2012, 30 (Suppl. 5), F139–F148. [Google Scholar] [CrossRef]
- Kepka, D.; Bodson, J.; Lai, D.; Sanchez-Birkhead, A.C.; Davis, F.A.; Lee, D.; Tavake-Pasi, F.; Napia, E.; Villalta, J.; Mukundente, V.; et al. Diverse caregivers’ hpv vaccine-related awareness and knowledge. Ethn. Health 2018. [Google Scholar] [CrossRef]
- McComb, E.; Ramsden, V.; Olatunbosun, O.; Williams-Roberts, H. Knowledge, Attitudes and Barriers to Human Papillomavirus (HPV) Vaccine Uptake Among an Immigrant and Refugee Catch-Up Group in a Western Canadian Province. J. Immigr. Minor. Health 2018, 20, 1424–1428. [Google Scholar] [CrossRef]
- Lofters, A.K.; Vahabi, M.; Fardad, M.; Raza, A. Exploring the acceptability of human papillomavirus self-sampling among Muslim immigrant women. Cancer Manag. Res. 2017, 9, 323–329. [Google Scholar] [CrossRef] [Green Version]
- Aragones, A.; Genoff, M.; Gonzalez, C.; Shuk, E.; Gany, F. HPV Vaccine and Latino Immigrant Parents: If They Offer It, We Will Get It. J. Immigr. Minor. Health 2016, 18, 1060–1065. [Google Scholar] [CrossRef]
- Stephens, D.P.; Thomas, T.L. Cultural Values Influencing Immigrant Haitian Mothers’ Attitudes Toward Human Papillomavirus Vaccination for Daughters. J. Black Psychol. 2013, 39, 156–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenfield, L.S.; Page, L.C.; Kay, M.; Li-Vollmer, M.; Breuner, C.C.; Duchin, J.S. Strategies for increasing adolescent immunizations in diverse ethnic communities. J. Adolesc. Health 2015, 56, S47–S53. [Google Scholar] [CrossRef] [PubMed]
- Kepka, D.; Ding, Q.; Bodson, J.; Warner, E.L.; Mooney, K. Latino Parents’ Awareness and Receipt of the HPV Vaccine for Sons and Daughters in a State with Low Three-Dose Completion. J. Cancer Educ. 2015, 30, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Bodson, J.; Warner, E.L.; Kepka, D. Moderate Awareness and Limited Knowledge Relating to Cervical Cancer, HPV, and the HPV Vaccine Among Hispanics/Latinos in Utah. Health Promot. Pract. 2016, 17, 548–556. [Google Scholar] [CrossRef]
- Luque, J.S.; Raychowdhury, S.; Weaver, M. Health care provider challenges for reaching Hispanic immigrants with HPV vaccination in rural Georgia. Rural Remote Health 2012, 12, 1975. [Google Scholar]
- Glenn, B.A.; Tsui, J.; Singhal, R.; Sanchez, L.; Nonzee, N.J.; Chang, L.C.; Taylor, V.M.; Bastani, R. Factors associated with HPV awareness among mothers of low-income ethnic minority adolescent girls in Los Angeles. Vaccine 2015, 33, 289–293. [Google Scholar] [CrossRef] [Green Version]
- Albright, K.; Barnard, J.; O’Leary, S.T.; Lockhart, S.; Jimenez-Zambrano, A.; Stokley, S.; Dempsey, A.; Kempe, A. Noninitiation and Noncompletion of HPV Vaccine Among English- and Spanish-Speaking Parents of Adolescent Girls: A Qualitative Study. Acad. Pediatrics 2017, 17, 778–784. [Google Scholar] [CrossRef]
- Salad, J.; Verdonk, P.; de Boer, F.; Abma, T.A. “A Somali girl is Muslim and does not have premarital sex. Is vaccination really necessary?” A qualitative study into the perceptions of Somali women in the Netherlands about the prevention of cervical cancer. Intern 2015, 14, 68. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.D.; De Jesus, M.; Mars, D.; Tom, L.; Cloutier, L.; Shelton, R.C. Decision-making about the HPV vaccine among ethnically diverse parents: Implications for health communications. J. Oncol. 2012. [Google Scholar] [CrossRef]
- Baldwin, A.S.; Bruce, C.M.; Tiro, J.A. Understanding how mothers of adolescent girls obtain information about the human papillomavirus vaccine: Associations between mothers’ health beliefs, information seeking, and vaccination intentions in an ethnically diverse sample. J. Health Psychol. 2013, 18, 926–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopfer, S.; Garcia, S.; Duong, H.T.; Russo, J.A.; Tanjasiri, S.P. A Narrative Engagement Framework to Understand HPV Vaccination Among Latina and Vietnamese Women in a Planned Parenthood Setting. Health Educ. Behav. 2017, 44, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Colon-Lopez, V.; Quinones, V.; Del Toro-Mejias, L.M.; Conde-Toro, A.; Serra-Rivera, M.J.; Martinez, T.M.; Rodriguez, V.; Berdiel, L.; Villanueva, H. HPV Awareness and Vaccine Willingness Among Dominican Immigrant Parents Attending a Federal Qualified Health Clinic in Puerto Rico. J. Immigr. Minority Health 2015, 17, 1086–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, R.B.; Pierre-Joseph, N.; Marquez, C.; Iloka, S.; Clark, J.A. Parents’ opinions of mandatory human papillomavirus vaccination: Does ethnicity matter? Women’s Health Issues 2010, 20, 420–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forster, A.S.; Rockliffe, L.; Marlow, L.A.V.; Bedford, H.; McBride, E.; Waller, J. Exploring human papillomavirus vaccination refusal among ethnic minorities in England: A comparative qualitative study. Psychooncology 2017, 26, 1278–1284. [Google Scholar] [CrossRef] [Green Version]
- Grandahl, M.; Tyden, T.; Gottvall, M.; Westerling, R.; Oscarsson, M. Immigrant women’s experiences and views on the prevention of cervical cancer: A qualitative study. Health Expect. 2015, 18, 344–354. [Google Scholar] [CrossRef]
- Zeraiq, L.; Nielsen, D.; Sodemann, M. Attitudes towards human papillomavirus vaccination among Arab ethnic minority in Denmark: A qualitative study. Scand. J. Public Health 2015, 43, 408–414. [Google Scholar] [CrossRef]
- Mupandawana, E.T.; Cross, R. Attitudes towards human papillomavirus vaccination among African parents in a city in the north of England: A qualitative study. Reprod Health 2016, 13, 97. [Google Scholar] [CrossRef] [Green Version]
- Marlow, L.A.; Wardle, J.; Forster, A.S.; Waller, J. Ethnic differences in human papillomavirus awareness and vaccine acceptability. J. Epidemiol. Community Health 2009, 63, 1010–1015. [Google Scholar] [CrossRef]
- Napolitano, F.; Gualdieri, L.; Santagati, G.; Angelillo, I.F. Knowledge and attitudes toward HPV infection and vaccination among immigrants and refugees in Italy. Vaccine 2018, 36, 7536–7541. [Google Scholar] [CrossRef]
- Grandahl, M.; Larsson, M.; Dalianis, T.; Stenhammar, C.; Tyden, T.; Westerling, R.; Neveus, T. Catch-up HPV vaccination status of adolescents in relation to socioeconomic factors, individual beliefs and sexual behaviour. PLoS ONE 2017, 12, e0187193. [Google Scholar] [CrossRef] [Green Version]
- Taebi, M.; Riazi, H.; Keshavarz, Z.; Afrakhteh, M. Knowledge and Attitude Toward Human Papillomavirus and HPV Vaccination in Iranian Population: A Systematic Review. Asian Pac. J. Cancer Prev. 2019, 20, 1945–1949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashing, K.T.; Carrington, A.; Ragin, C.; Roach, V. Examining HPV- and HPV vaccine-related cognitions and acceptability among US-born and immigrant hispanics and US-born and immigrant non-Hispanic Blacks: A preliminary catchment area study. Cancer Causes Control 2017, 28, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Moller, S.P.; Kristiansen, M.; Norredam, M. Human papillomavirus immunization uptake among girls with a refugee background compared with Danish-born girls: A national register-based cohort study. Eur. J. Cancer Prev. 2018, 27, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Lee, K.S.; Bukhsh, A.; Al-Worafi, Y.M.; Sarker, M.M.R.; Ming, L.C.; Khan, T.M. Outbreak of vaccine-preventable diseases in Muslim majority countries. J. Infect. Public Health 2018, 11, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Pratt, R.; Njau, S.W.; Ndagire, C.; Chaisson, N.; Toor, S.; Ahmed, N.; Mohamed, S.; Dirks, J. “We are Muslims and these diseases don’t happen to us”: A qualitative study of the views of young Somali men and women concerning HPV immunization. Vaccine 2019, 37, 2043–2050. [Google Scholar] [CrossRef]
- Marlow, L.A.; Wardle, J.; Waller, J. Attitudes to HPV vaccination among ethnic minority mothers in the UK: An exploratory qualitative study. Hum. Vaccines 2009, 5, 105–110. [Google Scholar] [CrossRef]
- Painter, J.E.; Viana De, O.M.S.; Jimenez, L.; Avila, A.A.; Sutter, C.J.; Sutter, R. Vaccine-related attitudes and decision-making among uninsured, Latin American immigrant mothers of adolescent daughters: A qualitative study. Hum. Vaccines Immunother. 2019, 15, 121–133. [Google Scholar] [CrossRef] [Green Version]
- Kahn, J.A.; Rosenthal, S.L.; Hamann, T.; Bernstein, D.I. Attitudes about human papillomavirus vaccine in young women. Int. J. STD AIDS 2003, 14, 300–306. [Google Scholar] [CrossRef]
- Ozdemir, S.; Akkaya, R.; Karasahin, K.E. Analysis of community-based researches related to knowledge, awareness, attitude and behaviors towards HPV and HPV vaccine published in Turkey: A systematic review. J. Turk. Ger. Gynecol. Assoc. 2019. [Google Scholar] [CrossRef]
- Berenson, A.B.; Rupp, R.; Dinehart, E.E.; Cofie, L.E.; Kuo, Y.F.; Hirth, J.M. Achieving high HPV vaccine completion rates in a pediatric clinic population. Hum. Vaccines Immunother. 2019, 15, 1562–1569. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Countries | Year Vaccination Introduced | Vaccination Strategy | Recent Reported Coverage (Year of Data) * | Immigrant’s Countries of Origin | HPV Vaccination in Countries of Origin |
|---|---|---|---|---|---|
| USA | 2006 | Primary care/health centre-based | 48.6% (2017) | Mexico, China, Vietnam, South Korea, Portugal, Puerto Rico, Brazil, Argentina, Colombia, Peru, and other parts of South America; South Asia; Somalia, Ethiopia, Eritrea, and other African countries | Many countries of South America notably Mexico, Argentina, Brazil and Colombia have implemented national HPV vaccination, in the remaining countries it has not been implemented or still at preparatory stage |
| Denmark | 2008 | Primary care/health centre-based | 40% (2018), but improving now | Poland, Syria, Turkey, Lebanon, Iraq, Palestine | In most of these countries there is no publicly funded national human papillomavirus vaccination programme |
| Netherlands | 2010 | Mixed: School-based and primary care-based | 45.5% (2018) | European countries, Japan, USA, Australia, Indonesia, Turkey, Surinam, Morocco and Somalia | Except for the Western immigrants, most non-Western immigrants don’t have a vaccination policy in their home countries. |
| UK | 2008 | School-based | 83.8% (2017/18) | Indian subcontinent, Poland, China, Nigeria, Somalia, Central America, and many other countries of Asia, Africa and Europe | In large majority of these countries there is no publicly funded national human papillomavirus vaccination programme but started in some countries (e.g., Sri Lanka) in recent years |
| Sweden | 2011 | School-based | 80% (2018) | Middle East, Africa, Asia, Eastern Europe | In large majority of these countries there is no publicly funded national human papillomavirus vaccination |
| Puerto Rico | 2006 | Primary care/health centre-based | 49.9% (2014) | Mainly from Dominican Republic | In Dominican Republic school-based HPV vaccination was announced in 2016 |
| Author(s), Publication Year [Ref] | Country of Study | Year of Study | Countries of Origin | Population | Mean Age in Years (Range) | Gender (n) | Knowledge Results | |
|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||
| Aragones et al., 2016 [21] | New York City, USA | Not reported | Colombia, Dominican Republic, Ecuador, Mexico | 36 Latino immigrants | 42 (25–65) | 3 | 33 | Most parents were either not informed or possessed inaccurate knowledge about HPV and HPV vaccine. |
| Forster et al., 2016 [35] | Southwest England, UK | 1 March 2015–1 March 2016 | Indian subcontinent, Caribbean, Africa | 33 Minority ethnic | 47 (36–62) | 1 | 32 | Thirteen immigrant parents had not heard about HPV vaccine. |
| Glenn et al., 2015 [27] | Los Angeles, USA | January 2009–January 2010 | Latina, China, Korea, Africa and others | 490 Minorities ethnic | 44 (7.2) | 490 | One third of participants had never heard of HPV or HPV vaccine and had low knowledge. About 63% (n=306) of respondents heard of HPV and another 61% (n=294) heard of HPV vaccine. | |
| Kepka et al., 2015 [24] | Salt Lake City, USA | Not reported | Mexico, Puerto Rico, Brazil, Argentina, Peru, and Portugal | 118 Mexican immigrants | 18–50 (±2.4) | 18 | 97 | Majority had no knowledge about HPV vaccine. |
| Mupandawana1 et al., 2016 [38] | North England, UK | Not reported | South Africa, Zimbabwe, Nigeria, Kenya, and Zambia | 10 African immigrants | Not reported | 5 | 5 | Most participants had inaccurate knowledge about HPV vaccine. |
| Allen et al., 2012 [30] | Boston, USA | February -May 2008 | Hispanic and African American | 64 immigrants | Not reported | 19 | 45 | The majority of parents felt that they did not have adequate information about HPV or HPV vaccine to make an informed decision. |
| Salad et al., 2015 [29] | Netherlands | March–June 2013 | Somalia | 6 immigrants | (23–66) | 6 | Participants described a lack of information about HPV vaccine. | |
| Luque et al., 2012 [26] | Georgia, USA | Not reported | Mexico and Honduras | 12 Hispanic immigrants | (25–44) | 7 | 5 | Parents had little knowledge about HPV vaccine. |
| Bodson et al., 2016 [25] | Salt Lake City, Utah, USA | August 2013–October 2013 | Mexico and others | 108 Hispanic/Latino immigrants101 born out USA | (16– >50) | 16 | 92 | Participants born in Mexico or elsewhere (Spanish background) had lower factual knowledge than participants who were born in the United States. In total, 67.3% of participants had heard of HPV vaccine and 76.4% of HPV. |
| Marlow et al., 2009 [39] | UK | July–August 2008 | Indian subcontinent, Caribbean, Africa, China | Ethnic minority | (16– >50) | 601 | Almost half of ethnic minority parents had not heard of the vaccine before being invited to vaccinate their daughters. | |
| Greenfield, et al., 2015 [23] | Washington, USAWashington, USA | Not reported | Mexico, Somalia, Ethiopia and Eritrea | 156 immigrants’ parents | 41 | Not reported | Lack of knowledge about HPV vaccine was the main reason given by parents that their adolescents had not been vaccinated. | |
| Zeraiq et al., 2105 [37] | Denmark | January 2011–January 2012 | Lebanon, Iraq, Palestine | 23 immigrants | Not reported | 23 | Ethnic minorities had lack of knowledge about HPV and HPV vaccine. | |
| Grandahletal., 2012 [36] | Uppsala, Sweden | February–June 2011 | Middle East, Africa, Asia, East ern Europe | 50 immigrants | (18 [28]–60) | 50 | The participants had limited knowledge about HPV and cervical cancer and HPV vaccine. Lack of knowledge was the main reported barrier to vaccination. | |
| Hopfer et al., 2017 [32] | CA, USA | July 21–August 20, 2016. | Latina and Vietnamese | 48 immigrants | (18–26) | 48 | Lack of awareness about HPV was evident in women’s stories, including confusing HPV with HIV, not knowing that HPV is a sexually transmitted infection. Vietnamese participants (96% (23/24)) were unable to elaborate on what HPV was, many were uncertain about its significance, 25% (2/8) unvaccinated Latina had never heard of HPV. | |
| Stephens et al., 2014 [22] | Haiti, USA | October 2010–May 2011 | Haiti | 31 immigrants. | (18–22 yrs.) | 31 | Mothers had no knowledge about HPV (80.6% (25/31)), very knowledgeable (3.2% (1/31)), fairly knowledgeable (12.9% (4/31)), somewhat knowledgeable (3.2% (1/31)). Mothers had no knowledge about HPV vaccine (83.9% (26/31)), very knowledgeable, fairly knowledgeable (9.7% (3/31)), somewhat knowledgeable (6.4% (2/31)). | |
| López, et al., 2016 [33] | San Juan, Puerto Rico | Not reported | Dominican Republic | 60 immigrants | 38.6 (± 7.2 yrs.) | 5 | 55 | Parents had not heard about HPV (3.3% (2/60)) and yes heard (91.7% (55/60)). Parents had not heard about HPV vaccine for males (38.3% (23/60)), had heard (55% (33/60)) |
| Author(s), Publication Year [Ref] | Country of Study | Year of Study | Population | Mean Rge in Years (Range) | Gender (n) | Attitudes Results | |
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
| Aragones et al. 2016 [21] | NYC (New York City), USA | Not reported | 36 immigrants | 42 (25–65) | 3 | 33 | Parents were motivated to protect the health of their children and were keen to obtain more information regarding HPV and the vaccine. |
| Forster et al., 2017 [35] | Southwest England | 1 March 2015–1 March 2016 | 33 Ethnic minorities | 47 (25–65) | 1 | 32 | Ethnic minority mothers said HPV vaccine was unnecessary as they had been fine without it. Parents expressed a wide range of concerns about the vaccine. A number of non-vaccinating ethnic minority parents believed their daughters were not at risk of contracting HPV or developing cervical cancer. |
| Glenn et al., 2015 [27] | Los Angeles, USA | January 2009–January 2010 | Ethnic minorities | 44 (7.2) | 490 | Ethnic minorities had positive and negative attitudes towards HPV vaccine: 63% of participants expressed positive attitudes towards immunization against HPV disease is a good thing. Participants with negative attitudes (54%): that Immunizations have more side effects than benefits. | |
| Albrigh et al., 2017 [28] | Colorado, USA | July 2012–January 2013 | 41 Ethnic minorities | (18– >50) | 3 | 38 | The most common reported reasons for non-initiation and non-completion among English-speaking parents included a low perceived risk of HPV infection, vaccine safety concerns, and distrust of government and/or medicine. Spanish-speaking parents who had either not encouraged initiation of HPV vaccine series or had not explained the necessity of completing the series, cited concerns that vaccination would encourage sexual activity. |
| Mupandawana et al., 2016 [38] | North England, UK | Not reported | 10 Ethnic minority | Not reported | 5 | 5 | Majority of participants said HPV vaccine was unacceptable, with fear of promiscuity, infertility and concerns about it being a new vaccine with unknown side effects. Religious values and cultural norms influenced vaccine decision-making with fathers acting as the ultimate decision-maker. |
| Allen et al., 2012 [30] | Boston, USA | February–May, 2008 | 64 Ethnic minority | Not reported | 19 | 45 | Participants distrust medical providers and pharmaceutical companies. |
| Salad et al., 2015 [29] | Netherland | March to June 2013 | 6 Immigrants | (23–66) | 6 | Most mothers have distrust towards the Dutch health care system and government and doubts about HPV vaccine age. | |
| Marlow et al., 2009 [39] | UK | July to August 2008. | Ethnic minority | (16– >50) | 601 | Parents with strong religious or cultural views were less likely to accept HPV vaccine. Consistency with attitudes to HPV testing, which some minority women felt reflected non-traditional cultural or religious practices and were concerned it encouraged premature sex. | |
| Greenfield et al. 2015 [23] | Washington, USA | Not reported | 156 immigrants | 41 | 156 gender not distinguished | All three ethnic groups expressed a desire to access vaccine information in their respective languages. | |
| Zeraiq et al., 2015 [37] | Denmark | January 2011 to January 2012 | 23 Ethnic minority | Not reported | 23 | All participating mothers accepted the vaccine for their daughters to prevent cervical cancer. | |
| Grandahl et al., 2012 [36] | Uppsala, Sweden | February to June 2011 | 50 immigrants | (18–60) | 50 | Participants’ expressed that they accepted the vaccination for their daughters, as it was important for their future health. Some women considered girls in the target group were too young and it would be better to wait until they were a little older and had become women. | |
| Perkins et al., 2010 [34] | Boston, Massachusetts, USA | June 2007 to February 2008. | 72 Immigrants | Not reported | 3 | 69 | Attitudes differed dramatically by ethnicity; only 11% of Caucasian parents endorsed school HPV vaccine entry requirements, compared with 78% of African-American parents, 60% of Afro-Caribbean and African parents, and 90% of Latino parents. Most parents expressed favorable opinions toward HPV vaccine for their own daughters. |
| Stephens et al., 2014 [22] | Haiti, USA | October 2010–May 2011 | 31 immigrants | (18–22) | 31 | Immigrant mothers who had little knowledge about HPV or the vaccine, felt unsure about vaccination; their concern centered on conflict with cultural values and perceptions of risks associated with HPV vaccine. | |
| Author(s), Publication Year [Ref] | Country of Study | Year of Study | Population | Age | Gender (n) | Perception Results | |
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
| Forster et al., 2016 [35] | southwest, England | 1 March 2015−1 March 2016 | 33 Ethnic minority | 47 (25–65) | 1 | 32 | Non-vaccinating ethnic minority parents reassured themselves of their decision by reporting that there are approaches other than vaccination to protect against HPV, such as abstinence from sex before marriage, which was related to religious beliefs. |
| Mupandawana1 et al., 2016 [38] | North England, UK | Not reported | 10 Ethnic minority | Not reported | 5 | 5 | HPV vaccine was generally unacceptable within this African community, with culture and religion influencing risk perceptions toward the vaccine and playing important roles in vaccination decision making. |
| Salad et al., 2015 [29] | Netherland | March–June 2013. | 6 Immigrants | (23–66) | 6 | Participants’ belief that abstinence from sex before marriage protect from diseases. | |
| Luque t al., 2012 [26] | Georgia, USA | Not reported | Hispanic immigrant | Not reported | 7 | 5 | Participants had misperceptions about HPV vaccine. They think that the vaccine is unnecessary if they are not having sex. |
| Albright et al., 2017 [28] | Colorado, USA | July 2012–January 2013 | 41 Ethnic minority | (18 to 50) | 3 | 38 | Spanish-speaking parents concerned that vaccinating against HPV would encourage sex. These parents expected their daughters to abstain from sex until marriage, and they did not want to give their daughters the message that sexual activity was permissible or give them a false protection. |
| Marlow et al., 2009 [39] | UK | July–August 2008. | 950 Ethnic minority | (16– >50) | 601 | The main reason for declining HPV vaccine was religious belief. The importance of religion appears to come from a strong belief in sexual abstinence until marriage. | |
| Greenfield et al. 2015 [23] | Washington, USA | Not reported | 156 Immigrants | 41 | 156 gender not stated | All three minority ethnicities had misperceptions about HPV vaccine or HPV disease. Most participants do not believe children are at risk and believe the vaccine could lead to early initiation of sexual activity. | |
| Grandahl et al., 2012 [36] | Uppsala, Sweden | February–June 2011 | 50 immigrants | (18–60) | 50 | Cultural influences on perceptions about protection: participants believed a woman did not have sexual intercourse with a man before marriage. | |
| Baldwin et al., 2012 [31] | Texas, USA | December 2008–May 2010 | 256 Ethnic minority | 42.3 | 256 | Non-White participants were significantly less likely to have talked with others and looked for information about HPV vaccine than White participants. Mothers’ perceptions of vulnerability, severity, varied by race/ethnicity. | |
| Stephens et al., 2014 [22] | Haiti, USA | October 2010–May 2011. | 31 Immigrants | (18–22) | 50 | Most mothers were willing to have their daughters vaccinated against HPV if it would protect or improve their health. Some mothers did not support HPV vaccine for their daughters; the remaining mothers were unsure because of their lack of knowledge. For those mothers who were unsure; concerns centred on conflict with cultural values and their perceptions of the risks associated with the vaccine. | |
| Author (Ref) | Score | Remarks |
|---|---|---|
| Qualitative Studies Assessed by Joanna Briggs Institute Critical Appraisal Checklist | ||
| Aragones et al., 2016 [21] | Met 8 of 10 positive criteria | |
| Allen et al., 2012 [30] | Met 10of 10 positive criteria | Nil |
| Zeraiq et al., 2105 [37] | Met 10 of 10 positive criteria | |
| Albright et al., 2017 [28] | Met 8 of 10 positive criteria | |
| Grandahl et al., 2012 [36] | Met 8 of 10 positive criteria | |
| Stephens et al., 2014 [22] | Met 8 of 10 positive criteria | |
| Forster et al., 2016 [35] | Met 8 of 10 positive criteria | |
| Mupandawana et al., 2016 [38] | Met 8 of 10 positive criteria | |
| Salad et al., 2015 [29] | Met 7 of 10 positive criteria | |
| Luque et al., 2012 [26] | Met 8 of 10 positive criteria | |
| Perkins et al., 2010 [34] | Met 8 of 10 positive criteria | |
| Hopfer et al. 2017 [32] | Met 8 of 10 positive criteria | |
| Quantitative Studies Assessed by Newcastle Ottawa Scale | ||
| Baldwin et al., 2012 [31] | Scored 7 of 9 stars | |
| Bodson et al., 2016 [25] | Scored 7 of 9 stars | It is a mixed method study |
| Glenn et al., 2015 [27] | Scored 7 of 9 stars | Nil |
| Greenfield et al., 2015 [23] | Scored7 of 9 stars | It is a mixed method study |
| Kepka et al., 2015 [24] | Scored 7 of 9 stars | Nil |
| López, et al., 2016 [33] | Scored 8 of 9 stars | |
| Marlow et al., 2009 [39] | Scored 8 of 9 stars | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netfa, F.; Tashani, M.; Booy, R.; King, C.; Rashid, H.; Skinner, S.R. Knowledge, Attitudes and Perceptions of Immigrant Parents Towards Human Papillomavirus (HPV) Vaccination: A Systematic Review. Trop. Med. Infect. Dis. 2020, 5, 58. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5020058
Netfa F, Tashani M, Booy R, King C, Rashid H, Skinner SR. Knowledge, Attitudes and Perceptions of Immigrant Parents Towards Human Papillomavirus (HPV) Vaccination: A Systematic Review. Tropical Medicine and Infectious Disease. 2020; 5(2):58. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5020058
Chicago/Turabian StyleNetfa, Faeza, Mohamed Tashani, Robert Booy, Catherine King, Harunor Rashid, and Susan R. Skinner. 2020. "Knowledge, Attitudes and Perceptions of Immigrant Parents Towards Human Papillomavirus (HPV) Vaccination: A Systematic Review" Tropical Medicine and Infectious Disease 5, no. 2: 58. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed5020058