How Does the Urban Environment Affect Health and Well-Being? A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
3. Results
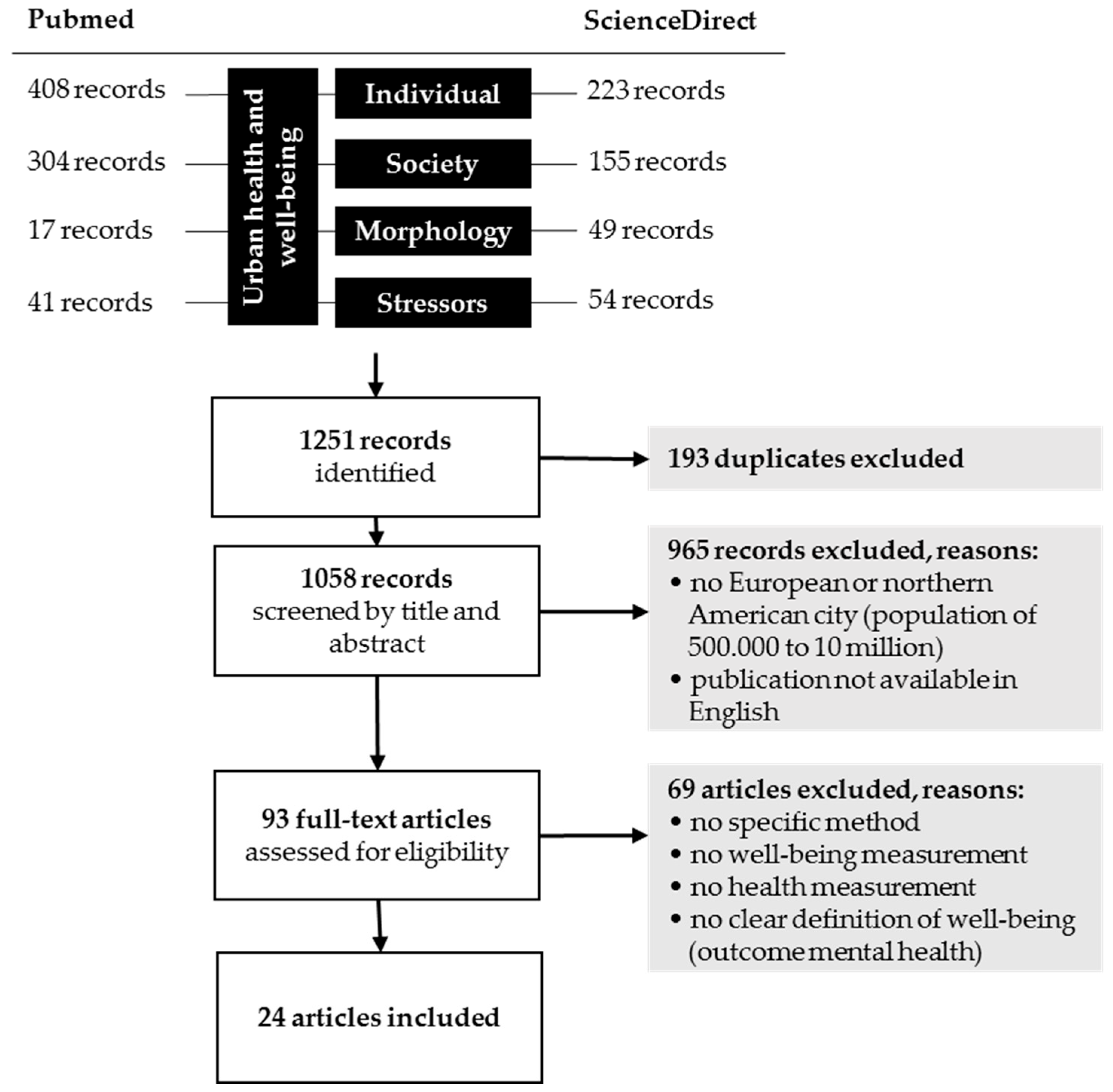
3.1. Study Selection
3.2. Studies on UrbWellth—The Individual Sector
3.3. Studies on UrbWellth—The Society Sector
3.4. Studies on UrbWellth—The Morphology Sector
3.5. Studies on UrbWellth—The Stressors Sector
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2014 Revision, CD-ROM Edition; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2014. [Google Scholar]
- Burdett, R.; Taylor, M.; Kaasa, A. Cities, Health and Well-Being: Conference newspaper. In Proceedings of the Hong Kong Urban Age Conference, Hong Kong, China, 16–17 November 2011; pp. 3–44. [Google Scholar]
- Galea, S.; Freudenberg, N.; Vlahov, D. Cities and population health. Soc. Sci. Med. 2005, 60, 1017–1033. [Google Scholar] [CrossRef] [PubMed]
- Rydin, Y.; Bleahu, A.; Davies, M.; Dávila, J.D.; Friel, S.; de Grandis, G.; Groce, N.; Hallal, P.C.; Hamilton, I.; Howden-Chapman, P.; et al. Shaping cities for health: Complexity and the planning of urban environments in the 21st century. Lancet 2012, 379, 2079–2108. [Google Scholar] [CrossRef]
- Vlahov, D.; Galea, S. Urban health: A new discipline. Lancet 2003, 362, 1091–1092. [Google Scholar] [CrossRef]
- Taylor, M. Cities, health and well-being: Report on a conference organised by LSE Cities at the London School of Economics and Political Science and the Alfred Herrhausen Society, in partnership with the University of Hong Kong. In Proceedings of the Urban Age Conference, Hong Kong, China, 16–17 November 2011; pp. 1–10. [Google Scholar]
- Healthy People 2020. Health-Related Quality of Life and Well-Being. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/health-related-quality-of-life-well-being (accessed on 27 June 2017).
- ICSU. Science Plan on Health and Wellbeing in the Changing Urban Environment: A Systems Approach; ICSU: Paris, France, 2011; Available online: https://www.icsu.org/cms/2017/05/Health-and-wellbeing-in-the-changing-urban-environment-web.pdf (accessed on 20 June 2017).
- Bai, X.; Nath, I.; Capon, A.; Hasan, N.; Jaron, D. Health and wellbeing in the changing urban environment: Complex challenges, scientific responses, and the way forward. Curr. Opin. Environ. Sustain. 2012, 4, 465–472. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for Europe. National Healthy Cities Networks in the WHO European Region—Promoting Health and Well-Being throughout Europe. Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/285995/Healthy-Cities-promoting-health-and-equity.pdf (accessed on 19 April 2016).
- Dodge, R.; Daly, A.; Huyton, J.; Sanders, L. The challenge of defining wellbeing. Int. J. Wellbeing 2012, 2, 222–235. [Google Scholar] [CrossRef]
- Alatartseva, E.; Barysheva, G. Well-being: Subjective and Objective Aspects. Procedia-Soc. Behav. Sci. 2015, 166, 36–42. [Google Scholar] [CrossRef]
- Ballas, D. What makes a ‘happy city’? Cities 2013, 32, S39–S50. [Google Scholar] [CrossRef]
- Von Szombathely, M.; Albrecht, M.; Antanaskovic, D.; Augustin, J.; Augustin, M.; Bechtel, B.; Bürk, T.; Fischereit, J.; Grawe, D.; Hoffmann, P.; et al. A Conceptual Modeling Approach to Health-Related Urban Well-Being. Urban Sci. 2017, 1, 17. [Google Scholar] [CrossRef]
- Marans, R.W. Quality of urban life & environmental sustainability studies: Future linkage opportunities. Habitat Int. 2015, 45, 47–52. [Google Scholar] [CrossRef]
- Babisch, W.; Wolf, K.; Petz, M.; Heinrich, J.; Cyrys, J.; Peters, A. Associations between Traffic Noise, Particulate Air Pollution, Hypertension, and Isolated Systolic Hypertension in Adults: The KORA Study. Environ. Health Perspect. 2014, 122, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Jarup, L.; Babisch, W.; Houthuijs, D.; Pershagen, G.; Katsouyanni, K.; Cadum, E.; Dudley, M.-L.; Savigny, P.; Seiffert, I.; Swart, W.; et al. Hypertension and Exposure to Noise Near Airports: The HYENA Study. Environ. Health Perspect. 2007, 116, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Pascal, M.; Corso, M.; Chanel, O.; Declercq, C.; Badaloni, C.; Cesaroni, G.; Henschel, S.; Meister, K.; Haluza, D.; Martin-Olmedo, P.; et al. Assessing the public health impacts of urban air pollution in 25 European cities: Results of the Aphekom project. Sci. Total Environ. 2013, 449, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Faustini, A.; Stafoggia, M.; Berti, G.; Bisanti, L.; Chiusolo, M.; Cernigliaro, A.; Mallone, S.; Primerano, R.; Scarnato, C.; Simonato, L.; et al. The relationship between ambient particulate matter and respiratory mortality: A multi-city study in Italy. Eur. Respir. J. 2011, 38, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Larson, L.R.; Jennings, V.; Cloutier, S.A. Public Parks and Wellbeing in Urban Areas of the United States. PLoS ONE 2016, 11, e0153211. [Google Scholar] [CrossRef] [PubMed]
- Bertram, C.; Rehdanz, K. The Role of Urban Green Space for Human Well-Being. Ecol. Econ. 2015, 120, 139–152. [Google Scholar] [CrossRef]
- Pedersen, E. City dweller responses to multiple stressors intruding into their homes: Noise, light, odour, and vibration. Int. J. Environ. Res. Public Health 2015, 12, 3246–3263. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.; Prins, R.; Crawford, F.; Humphreys, D.; Mitchell, R.; Sahlqvist, S.; Thomson, H.; Ogilvie, D. Effects of living near an urban motorway on the wellbeing of local residents in deprived areas: Natural experimental study. PLoS ONE 2017, 12, e0174882. [Google Scholar] [CrossRef] [PubMed]
- Grellier, J.; White, M.P.; Albin, M.; Bell, S.; Elliott, L.R.; Gascón, M.; Gualdi, S.; Mancini, L.; Nieuwenhuijsen, M.J.; Sarigiannis, D.A.; et al. BlueHealth: A study programme protocol for mapping and quantifying the potential benefits to public health and well-being from Europe´s blue spaces. BMJ Open 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hogan, M.J.; Leyden, K.M.; Conway, R.; Goldberg, A.; Walsh, D.; McKenna-Plumley, P.E. Happiness and health across the lifespan in five major cities: The impact of place and government performance. Soc. Sci. Med. 2016, 162, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.K.; Wyka, K.E.; Ferris, E.B.; Gardner, J.; Evenson, K.R.; Tripathi, D.; Soto, G.M.; Cato, M.S.; Moon, J.; Wagner, J.; et al. The Physical Activity and Redesigned Community Spaces (PARCS) Study: Protocol of a natural experiment to investigate the impact of citywide park redesign and renovation. BMC Public Health 2016, 16, 1160. [Google Scholar] [CrossRef] [PubMed]
- Kestens, Y.; Chaix, B.; Gerber, P.; Desprès, M.; Gauvin, L.; Klein, O.; Klein, S.; Köppen, B.; Lord, S.; Naud, A.; et al. Understanding the role of contrasting urban contexts in healthy aging: An international cohort study using wearable sensor devices (the CURHA study protocol). BMC Geriatr. 2016, 16, 96. [Google Scholar] [CrossRef] [Green Version]
- McCracken, D.S.; Allen, D.A.; Gow, A.J. Associations between urban greenspace and health-related quality of life in children. Prev. Med. Rep. 2016, 3, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Ram, B.; Nightingale, C.M.; Hudda, M.T.; Kapetanakis, V.V.; Ellaway, A.; Cooper, A.R.; Page, A.; Lewis, D.; Cummins, S.; Giles-Corti, B.; et al. Cohort profile: Examining Neighbourhood Activities in Built Living Environments in London: The ENABLE London-Olympic Park cohort. BMJ Open 2016, 6, e012643. [Google Scholar] [CrossRef] [PubMed]
- Sabel, C.E.; Hiscock, R.; Asikainen, A.; Bi, J.; Depledge, M.; van den Elshout, S.; Friedrich, R.; Huang, G.; Hurley, F.; Jantunen, M.; et al. Public health impacts of city policies to reduce climate change: Findings from the URGENCHE EU-China project. Environ. Health 2016, 15 (Suppl. S1), 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward Thompson, C.; Aspinall, P.; Roe, J.; Robertson, L.; Miller, D. Mitigating Stress and Supporting Health in Deprived Urban Communities: The Importance of Green Space and the Social Environment. Int. J. Environ. Res. Public Health 2016, 13, 440. [Google Scholar] [CrossRef] [PubMed]
- Egan, M.; Lawson, L.; Kearns, A.; Conway, E.; Neary, J. Neighbourhood demolition, relocation and health. A qualitative longitudinal study of housing-led urban regeneration in Glasgow, UK. Health Place 2015, 33, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Egan, M.; Kearns, A.; Mason, P.; Tannahill, C.; Bond, L.; Coyle, J.; Beck, S.; Crawford, F.; Hanlon, P.; Lawson, L.; et al. Protocol for a mixed methods study investigating the impact of investment in housing, regeneration and neighbourhood renewal on the health and wellbeing of residents: The GoWell programme. BMC Med. Res. Methodol. 2010, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.; Read, U.M.; Molaodi, O.R.; Cassidy, A.; Maynard, M.J.; Lenguerrand, E.; Astell-Burt, T.; Teyhan, A.; Whitrow, M.; Enayat, Z.E. The Determinants of young Adult Social well-being and Health (DASH) study: Diversity, psychosocial determinants and health. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1173–1188. [Google Scholar] [CrossRef] [PubMed]
- Hayward, E.; Ibe, C.; Young, J.H.; Potti, K.; Jones, P.; Pollack, C.E.; Gudzune, K.A. Linking social and built environmental factors to the health of public housing residents: A focus group study. BMC Public Health 2015, 15, 351. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.R.; Lewis, D.J.; Fahy, A.; Eldridge, S.; Taylor, S.J.C.; Moore, D.G.; Clark, C.; Stansfeld, S.A.; Cummins, S. Individual socio-demographic factors and perceptions of the environment as determinants of inequalities in adolescent physical and psychological health: The Olympic Regeneration in East London (ORiEL) study. BMC Public Health 2015, 15, 150. [Google Scholar] [CrossRef] [PubMed]
- Völker, S.; Kistemann, T. Developing the urban blue: Comparative health responses to blue and green urban open spaces in Germany. Health Place 2015, 35, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Völker, S.; Kistemann, T. “I’m always entirely happy when I’m here!” Urban blue enhancing human health and well-being in Cologne and Düsseldorf, Germany. Soc. Sci. Med. 2013, 78, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Wood, C.J.; Pretty, J.; Griffin, M. A case-control study of the health and well-being benefits of allotment gardening. J. Public Health 2016, 38, e336–e344. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Jones, A.; Roberts, H. More than A to B: The role of free bus travel for the mobility and wellbeing of older citizens in London. Ageing Soc. 2014, 34, 472–494. [Google Scholar] [CrossRef] [PubMed]
- Phillips, G.; Bottomley, C.; Schmidt, E.; Tobi, P.; Lais, S.; Yu, G.; Lynch, R.; Lock, K.; Draper, A.; Moore, D.; et al. Measures of exposure to the Well London Phase-1 intervention and their association with health well-being and social outcomes. J. Epidemiol. Community Health 2014, 68, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Phillips, G.; Bottomley, C.; Schmidt, E.; Tobi, P.; Lais, S.; Yu, G.; Lynch, R.; Lock, K.; Draper, A.; Moore, D.; et al. Well London Phase-1: Results among adults of a cluster-randomised trial of a community engagement approach to improving health behaviours and mental well-being in deprived inner-city neighbourhoods. J. Epidemiol. Community Health 2014, 68, 606–614. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would you be happier living in a greener urban area? A fixed-effects analysis of panel data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Garvin, E.; Branas, C.; Keddem, S.; Sellman, J.; Cannuscio, C. More than just an eyesore: Local insights and solutions on vacant land and urban health. J. Urban Health 2013, 90, 412–426. [Google Scholar] [CrossRef] [PubMed]
- Honold, J.; Beyer, R.; Lakes, T.; van der Meer, E. Multiple environmental burdens and neighborhood-related health of city residents. J. Environ. Psychol. 2012, 32, 305–317. [Google Scholar] [CrossRef]
- Brown, S.C.; Mason, C.A.; Perrino, T.; Lombard, J.L.; Martinez, F.; Plater-Zyberk, E.; Spokane, A.R.; Szapocznik, J. Built environment and physical functioning in Hispanic elders: The role of “eyes on the street”. Environ. Health Perspect. 2008, 116, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- Kuh, D.; Ben Shlomo, Y. A life Course Approach to Chronic Disease Epidemiology, 2nd ed.; Oxford University Press: Oxford, NY, USA, 2004. [Google Scholar]
- Institute of Community Health Sciences. Health of Young People in East London—The Relachs Study. Available online: http://archive.wolfson.qmul.ac.uk/relachs/academics/publications/Relachs_report.pdf (accessed on 10 August 2017).
- Fagg, J.; Curtis, S.; Stansfeld, S.; Congdon, P. Psychological distress among adolescents, and its relationship to individual, family and area characteristics in East London. Soc. Sci. Med. 2006, 63, 636–648. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.; Patel, V.; Leon, D.A. Child mental health differences amongst ethnic groups in Britain: A systematic review. BMC Public Health 2008, 8, 258. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.A.; Haines, M.M.; Head, J.A.; Bhui, K.; Viner, R.; Taylor, S.J.; Hillier, S.; Klineberg, E.; Booy, R. Ethnicity, social deprivation and psychological distress in adolescents: School-based epidemiological study in east London. Br. J. Psychiatry 2004, 185, 233–238. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, D.; Buffoli, M.; Capasso, L.; Fara, G.M.; Rebecchi, A.; Capolongo, S. Green areas and public health: Improving wellbeing and physical activity in the urban context. Epidemiol. Prev. 2015, 39, 8–13. [Google Scholar] [PubMed]
- Salmond, J.A.; Tadaki, M.; Vardoulakis, S.; Arbuthnott, K.; Coutts, A.; Demuzere, M.; Dirks, K.N.; Heaviside, C.; Lim, S.; Macintyre, H.; et al. Health and climate related ecosystem services provided by street trees in the urban environment. Environ. Health 2016, 15 (Suppl. S1), 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, K.L.; Robbins, A.S.T. Metro nature, environmental health, and economic value. Environ. Health Perspect. 2015, 123, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Tzoulas, K.; Korpela, K.; Venn, S.; Yli-Pelkonen, V.; Kaźmierczak, A.; Niemela, J.; James, P. Promoting ecosystem and human health in urban areas using Green Infrastructure: A literature review. Landsc. Urban Plan. 2007, 81, 167–178. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Bullinger, M. Assessing health-related quality of life in chronically ill children with the German KINDL: First psychometric and content analytical results. Qual. Life Res. 1998, 7, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Dobbinson, S.J.; Veitch, J.; Salmon, J.; Wakefield, M.; Staiger, P.K.; MacInnis, R.J.; Simmons, J. Study protocol for a natural experiment in a lower socioeconomic area to examine the health-related effects of refurbishment to parks including built-shade (ShadePlus). BMJ Open 2017, 7, e013493. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.; Tisdall, R.; Middleton, J.; Verma, A.; van Ameijden, E.; Birt, C.; Macherianakis, A.; Bruce, N.G. Quality of and access to green space in relation to psychological distress: Results from a population-based cross-sectional study as part of the EURO-URHIS 2 project. Eur. J. Public Health 2018, 28, 35–38. [Google Scholar] [CrossRef] [PubMed]
- IPCC. Summary for Policymakers. Available online: https://www.ipcc.ch/pdf/assessment-report/ar5/wg2/ar5_wgII_spm_en.pdf (accessed on 11 September 2017).
- Hiscock, R.; Mudu, P.; Braubach, M.; Martuzzi, M.; Perez, L.; Sabel, C. Wellbeing impacts of city policies for reducing greenhouse gas emissions. Int. J. Environ. Res. Public Health 2014, 11, 12312–12345. [Google Scholar] [CrossRef] [PubMed]
- Duhme, H.; Weiland, S.K.; Keil, U.; Kraemer, B.; Schmid, M.; Stender, M.; Chambless, L. The association between Self-Reported Symptoms of Asthma and Allergic Rhinitis and Self-Reported Traffic Density on Street of Residence in Adolescents. Epidemiology 1996, 6, 578–582. [Google Scholar] [CrossRef]
- Hiramatsu, K.; Yamamoto, T.; Taira, K.; Ito, A.; Nakasone, T. A Survey on Health Effects due to Aircraft Noise on Residents Living Around Kadena Air Base in the Ryukyus. J. Sound Vib. 1997, 205, 451–460. [Google Scholar] [CrossRef]
- Yoshida, T.; Osada, Y.; Kawaguchi, T.; Hoshiyama, Y.; Yoshida, K.; Yamamoto, K. Effects of Road Traffic Noise on Inhabitants of Tokyo. J. Sound Vib. 1997, 205, 517–522. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine Particulate Air Pollution and Hospital Admission for Cardiovascular and Respiratory Diseases. JAMA 2006, 295, 1127. [Google Scholar] [CrossRef] [PubMed]
- Węziak-Białowolska, D. Quality of life in cities—Empirical evidence in comparative European perspective. Cities 2016, 58, 87–96. [Google Scholar] [CrossRef]
- Inoue, S.; Ohya, Y.; Odagiri, Y.; Takamiya, T.; Ishii, K.; Kitabayashi, M.; Suijo, K.; Sallis, J.F.; Shimomitsu, T. Association between Perceived Neighborhood Environment and Walking among Adults in 4 Cities in Japan. J. Epidemiol. 2010, 20, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Jaśkiewicz, M.; Besta, T. Is Easy Access Related to Better Life? Walkability and Overlapping of Personal and Communal Identity as Predictors of Quality of Life. Appl. Res. Qual. Life 2014, 9, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Saelens, B.E.; Handy, S.L. Built environment correlates of walking: A review. Med. Sci. Sports Exerc. 2008, 40, S550–S566. [Google Scholar] [CrossRef] [PubMed]
- Talen, E.; Koschinsky, J. The Walkable Neighborhood: A Literature Review. Int. J. Sustain. Land Use Urban Plan. 2013, 1, 42–63. [Google Scholar] [CrossRef]
- Zuniga-Teran, A.A.; Orr, B.J.; Gimblett, R.H.; Chalfoun, N.V.; Guertin, D.P.; Marsh, S.E. Neighborhood Design, Physical Activity, and Wellbeing: Applying the Walkability Model. Int. J. Environ. Res. Public Health 2017, 14, 76. [Google Scholar] [CrossRef] [PubMed]
- Ashton, K. That ‘Internet of Things’ Thing. RFID J. 2009, 22, 97–114. [Google Scholar]
- Kamel Boulos, M.N.; Al-Shorbaji, N.M. On the Internet of Things, smart cities and the WHO Healthy Cities. Int. J. Health Geogr. 2014, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kamel Boulos, M.N.; Tsouros, A.D.; Holopainen, A. ‘Social, innovative and smart cities are happy and resilient’: Insights from the WHO EURO 2014 International Healthy Cities Conference. Int. J. Health Geogr. 2015, 14, 3. [Google Scholar] [CrossRef] [PubMed]
- Almansa, J. “Vincles BCN”, a Project against Isolation of Senior Citizens, Winner of Bloomberg Mayors Challenge: Mobile World Capital Barcelona. Available online: http://mobileworldcapital.com/684/ (accessed on 21 August 2017).
- Alcaraz, T.G. Could New Technology Help Older People in Barcelona Create Stronger Networks? Available online: https://www.theguardian.com/cities/2014/oct/28/could-new-technology-help-older-people-in-barcelona-create-stronger-networks (accessed on 21 August 2017).
- Kamel Boulos, M.N. Xbox 360 Kinect Exergames for Health. Games Health J. 2012, 1, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Holopainen, A.; Arpola, T.; Wuorisalo, J. Games for Health—Finland. Available online: https://de.slideshare.net/gamesforhealthfinland/health-tuesday-games-for-health-finland (accessed on 21 August 2017).



{kind=link}
{kind=link}
| Author, Year | Individual Sector | Society Sector | Morphology Sector | Stressors Sector |
|---|---|---|---|---|
| Foley et al., 2017 [23] | o | o | x | |
| Grellier et al., 2017 [24] | o | o | x | o |
| Hogan et al., 2016 [25] | x | o | o | |
| Huang et al., 2016 [26] | o | o | x | o |
| Kestens et al., 2016 [27] | x | o | o | |
| McCracken et al., 2016 [28] | o | o | x | |
| Ram et al., 2016 [29] | o | x | o | |
| Sabel et al., 2016 [30] | o | o | o | x |
| Ward-Thompson et al., 2016 [31] | o | o | x | |
| Egan et al., 2015 [32] and 2010 [33] | o | x | o | |
| Harding et al., 2015 [34] | x | o | o | |
| Hayward et al., 2015 [35] | o | x | o | |
| Smith et al., 2015 [36] | x | o | o | |
| Völker et al., 2015 [37] and 2013 [38] | o | o | x | |
| Wood et al., 2015 [39] | o | x | ||
| Green et al., 2014 [40] | x | o | o | |
| Phillips et al., 2014 [41] and 2014 [42] | x | o | ||
| White et al., 2013 [43] | o | o | x | |
| Garvin et al., 2012 [44] | o | o | x | |
| Honold et al., 2012 [45] | o | o | o | x |
| Brown et al., 2008 [46] | o | o | x |
| Authors, Year, Study Area | Study Title | Design | UrbWellth Measurement | Main Findings |
|---|---|---|---|---|
| Hogan et al., 2016 [25], Berlin, Germany; Paris; France; London, UK; New York, USA; Toronto, Canada | Happiness and health across the lifespan in five major cities: The impact of place and government performance. | Cross-sectional survey, N = 1286 (aged 25–34 years); N = 1960 (35–49); N = 953 (50–64); N = 685 (65–85) | Quality of Life Survey | Younger residents preferred better access to cultural, shopping or sport amenities and an attractive city (place variables), which was linked to happiness and health. Happiness and health of older inhabitants was associated with the provision of quality governmental services (performance variables). |
| Kestens et al., 2016 [27], Montreal, Canada; Paris, France; Luxembourg, Luxembourg | Understanding the role of contrasting urban contexts in healthy aging: an international cohort study using wearable sensor devices (the CURHA study protocol). | Cohort study, N = still outstanding | Combination of data from 7-day GPS and accelerometer for daily mobility, 7-day diary of self-reported destinations and social contacts for information about transportation modes, destination types, and social contacts, a socio-spatial questionnaire (VERITAS) for e.g., location of regular destinations or social network characteristics, qualitative assessment of mobility and place experience (Go-along method), CAPI questionnaires for numerous outcomes and control variables including health and perceived environment and GIS to depict among others land use or neighborhood composition. | Still to be published. |
| Harding et al., 2015 [34], London, UK | The Determinants of young Adult Social well-being and Health (DASH) study: diversity, psychosocial determinants, and health. | Cohort study, N = 6643 (2002/2003); N = 4782 (2005/2006); N = 665 (2012–2014); aged 11–13 years | Combination of qualitative interviews, physical measures by trained field assistants/nurses, self-completed questionnaires about socioeconomic and psychosocial factors and health using the SDQ, a TDS, the GHQ-12, and a PBI. | Ethnic minority adolescents reported better mental health than White British but had higher blood pressure compared to White British. |
| Smith et al., 2015 [36], East London, UK | Individual socio-demographic factors and perceptions of the environment as determinants of inequalities in adolescent physical and psychological health: the Olympic Regeneration in East London (ORiEL) study. | Cross-sectional sample, N = 3105 (aged 11–12 years) | Combination of a pseudo-anonymized paper-based questionnaire including the WEMWBS for assessing positive mental well-being, the Short Moods and Feelings Questionnaire to assess depressive symptoms, the Youth-Physical Activity Questionnaire, and a self-assessment of general health and longstanding illness. | Mental health advantage in adolescents increased as positive perception of neighborhood safety, aesthetics, walkability, and services increased. Same trends were found for general health. |
| Green et al., 2014 [40], London, UK | More than A to B: the role of free bus travel for the mobility and wellbeing of older citizens in London. | Cross-sectional sample, N = 47 (aged > 60 years) | Implementation of interviews in either individual (N = 14), dyad (N = 12) or small group (N = 21) settings. | By using free bus travel older citizens can more participate in life in the city, have more possibilities for social interaction, increased health well-being, and reduced chronic loneliness. |
| Phillips et al., 2014 [41] and 2014 [42], London, UK | Well London Phase-1: results among adults of a cluster-randomized trial of a community engagement approach to improving health behaviors and mental well-being in deprived inner-city neighborhoods/measures of exposure to the Well London Phase-1 intervention and their association with health, well-being and social outcomes. | Cluster-randomized-trial, 20 matched pairs of neighbor-hoods, N = 3986. | By using a post-intervention questionnaire survey, primary outcomes (five portions fruits or vegetables/day; 5 × 30 min of moderate intensity physical activity/week, GHQ-12 score, and WEMWBS score) were measured. | Interventions did not improve health behaviors, well-being, and social outcomes. |
| Authors, Year, Study Area | Study Title | Design | UrbWellth Measurement | Main Findings |
|---|---|---|---|---|
| Ram et al., 2016 [29], London, UK | Cohort profile: Examining Neighborhood Activities in Built Living Environments in London: the ENABLE London—Olympic Park cohort. | Controlled cohort study, N = 1497 | Combination of physical activity and location data, anthropometry (Body mass index), questionnaire data using among others the EQ-5D to measure the general health status, the “Neighborhood Physical Activity Questionnaire” and data from the Household Survey 2011. | Still to be published. |
| Egan et al., 2015 [32] and 2010 [33], Glasgow, Scotland, UK | Neighborhood demolition, relocation, and health. A qualitative longitudinal study of housing-led urban regeneration in Glasgow, UK/Protocol for a mixed methods study investigating the impact of investment in housing, regeneration and neighborhood renewal on the health and wellbeing of residents: the GoWell program. | Qualitative longitudinal study including 4 survey waves, up to N = 6008 | Combination of qualitative interviews about participant’s living environment and health behaviors, the SF-12 (Wave 1), and from Wave 2 onwards the WEMWBS. | Inconsistent results suggesting that individual-level contextual differences, together with neighborhood-level factors and variations in intervention implementation of redesign might influence the perception of residents concerning their health and well-being. |
| Hayward et al., 2015 [35], Baltimore, Maryland, USA | Linking social and built environmental factors to the health of public housing residents: a focus group study. | Focus group study, N = 28 | Interviews conducted in six focus groups to assess residents’ perception of health and neighborhood attributes, resources, and social structure. | Identification of four themes: 1. Public housing’s unhealthy physical environment limits health and well-being; 2. The city environment limits opportunities for healthy lifestyle choice; 3. Lack of trust in relationships contributes to social isolation; 4. Increased neighborhood social capital might improve well-being. |
| Authors, Year, Study Area | Study Title | Design | UrbWellth Measurement | Main Findings |
|---|---|---|---|---|
| Foley et al., 2017 [23], Glasgow, Scotland | Effects of living near an urban motorway on the well-being of local residents in deprived areas: natural experimental study | Experimental study involving longitudinal cohort (N = 365) and two cross-sectional samples (baseline: N = 980; follow-up: N = 978) | Health and well-being were assessed using mental (MCS-8) and physical (PCS-8) components of the SF-8-scale and the SWEMWBS. | Participants with and without chronic condition living closer to the motorway experienced significantly reduced mental well-being over time compared to those living further away. |
| Grellier et al., 2017 [24], Bulgaria, Czech Republic, Estonia, Finland, France, Germany, Greece, Ireland, Italy, Portugal, Spain, Sweden, Netherlands, UK | BlueHealth: a study program protocol for mapping and quantifying the potential benefits to public health and well-being from Europe’ s blue spaces | International European Panel study, N = still outstanding | Combination of systematic reviews, analyses of secondary data sets (e.g., GHQ-12, SF-36, Global Life Satisfaction) and analyses of new survey data (e.g., well-being measures such as the WHO-5 Well-being Index and items in the European Social Survey). Additionally, several community-level interventions will be conducted and evaluated. | Still to be published. |
| Huang et al., 2016 [26], New York City, USA | The Physical Activity and Redesigned Community Spaces (PARCS) Study: Protocol of a natural experiment to investigate the impact of citywide park redesign and renovation | Case-control study design, N = 30 intervention park neighborhoods and N = 20 control park neighborhoods | A potential impact of park renovation/redesign on its usage, mental health, and community well-being will be measured by using data about the sociodemographic background of study sites, physical activity measured via a GPS, self-report (using a smartphone-app), and accelerometers together with survey questions from the EURO-URHIS 2 project [58] to measure park satisfaction and perception, psychosocial and mental health by using among others the SF-12 and a perceived stress scale, and finally community well-being (measured e.g., by using the NEWS). | Still to be published. |
| McCracken et al., 2016 [28], Edinburgh, Scotland, UK | Associations between urban greenspace and health-related quality of life in children | Cross-sectional survey, N = 276 (aged 7–13 years) | The Kid-KINDL questionnaire was used to measure health-related quality of life together with self-report of usage of greenspace. Quantity of greenspace was measured by using a GIS, socioeconomic and sociodemographic covariates were collected via a questionnaire. | Results showed that higher greenspace use was significantly associated with better health-related quality of life in children. |
| Ward-Thompson et al., 2016 [31], Scotland, UK | Mitigating Stress and Supporting Health in Deprived Urban Communities: The importance of Green Space and the Social Environment | Cross-sectional survey, N = 406 | Self-reported stress based on the Perceived Stress Scale (PSS), mental well-being based on the SWEMWBS together with a single-item assessment of general health were primary measures, secondary measures were physical activity levels and social well-being, all based on self-report. Additionally, objective and subjective measures on socioeconomic variables, green space and area-level deprivation were collected. | Social isolation and place belonging were strong predictors of stress in three communities. Another community showed poor general health. The amount of green space and access to gardens were significant predictors of stress. For instance, physical activity or frequency of visits to green space in winter were associated with general health. |
| Wood et al., 2015 [39], UK | A case-control study of the health and well-being benefits of allotment gardening | Case-control study, N = 269 | The GHQ-12 was used to assess general health, self-esteem was assessed using the one-page 10-item Rosenberg self-esteem scale, and mood was assessed using the 30-item POMS questionnaire. | Results revealed that allotment gardeners had a significantly better self-esteem, total mood disturbance and general health, experienced less depression and fatigue and more vigor. |
| Völker et al., 2015 [37] and 2013 [38], Cologne and Düsseldorf, Germany | Developing the urban blue: Comparative health responses to blue and green urban open spaces in Germany/Reprint of: “I’m always entirely happy when I’m here!” Urban blue enhancing human health and well-being in Cologne and Düsseldorf, Germany | Cross-sectional survey, N = 113 and N = 42 | Semi-standardized qualitative interviews with open answers. Spatial analyses were conducted using a GIS. | Spending time next to the river enhanced health and well-being. |
| White et al., 2013 [43], England | Would You Be Happier Living in a Greener Urban Area? A Fixed-Effects Analysis of Panel Data | Panel Survey, N = 10,168 | Mental distress was measured with the short-form GHQ-12, global life satisfaction was assessed with one question. Additionally, local-area green space data were used. | A positive effect of living in urban areas with more green spaces compared to areas with less green spaces on mental health and well-being, even after controlling for individual and regional covariates could be detected. |
| Garvin et al., 2012 [44], Philadelphia, Pennsylvania, USA | More Than Just an Eyesore: Local Insights and Solutions on Vacant Land and Urban Health | Cross-sectional survey, N = 29 | Qualitative interviews with open answers. | Vacant land affected community well-being, attracting crime, impacted physical health through injury and mental health through anxiety and stigma. |
| Brown et al., 2008 [46], Miami, Florida | Built Environment and Physical Functioning in Hispanic Elders: The Role of “Eyes on the Street” | Population-based cohort study, N = 273 Hispanics (aged ≥ 70 years) | Combination of the “built environment” measured by using the University of Miami Built Environment Coding System (UMBECS), assessment of social support using three scales, psychological distress by self-reported anxiety and depressive symptoms using a 10-item, Spanish version of the Spielberger State Trait Anxiety Inventory and a 7-item Depressive Affect subscale of the Center for Epidemiological Studies Depression Scale together with measurements of physical functioning and self-rated health. | Architectural features that facilitate visual and social contacts had a significant direct relationship with elder’s physical functioning and an indirect relationship through social support and psychological distress. |
| Authors, Year, Study Area | Study Title | Design | UrbWellth Measurement | Main Findings |
|---|---|---|---|---|
| Sabel et al., 2016 [30], Basel, Switzerland, Kuopio, Finland, Rotterdam, Netherlands, Stuttgart, Germany, and Thessaloniki, Greece, Xi’an and Suzhou, China | Public health impacts of city policies to reduce climate change: findings from the URGENCHE EU-China project | Scenario modelling, N = not accessible | Comparative risk assessment was conducted by calculating DALYs, additionally, well-being cross sectional surveys were conducted. Information about levels of carbon dioxide emissions, health impacting exposures (noise, air pollution or physical activity), health and well-being were established for each city together with atmospheric models and exposure response functions, derived from epidemiological studies (e.g., the WHO HRAPIE) to model associations between these factors and health and well-being in 2020. | Four key findings were: 1. Introduction of electric cars might confer some small health benefits; 2. Reduction of private car use might have benefits for carbon dioxide reduction and positive health impacts; 3. Benefits of carbon dioxide reduction from increasing housing efficiency are likely to be minor and benefits for health and well-being depend on good air exchange; 4. Heating homes by in-home biomass burning might reduce carbon dioxide emission. However, consequences for health and well-being were negative with the technology used in the participating cities. |
| Honold et al., 2012 [45], Berlin, Germany | Multiple environmental burdens and neighborhood-related health of city residents | Cross-sectional study, N = 428 | By using a GIS, street blocks were aggregated to areas of high, average, and low levels of burden (using data of noise, air pollution, and green space). Additionally, household questionnaires dealing with socioeconomic and sociodemographic variables and environmental perception and appraisal were conducted. | Residents from high-burden blocks assessed the environmental conditions more stressful, reported poorer health behavior and were less satisfied with their environmental neighborhood than residents from low burden blocks. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krefis, A.C.; Augustin, M.; Schlünzen, K.H.; Oßenbrügge, J.; Augustin, J. How Does the Urban Environment Affect Health and Well-Being? A Systematic Review. Urban Sci. 2018, 2, 21. https://0-doi-org.brum.beds.ac.uk/10.3390/urbansci2010021
Krefis AC, Augustin M, Schlünzen KH, Oßenbrügge J, Augustin J. How Does the Urban Environment Affect Health and Well-Being? A Systematic Review. Urban Science. 2018; 2(1):21. https://0-doi-org.brum.beds.ac.uk/10.3390/urbansci2010021
Chicago/Turabian StyleKrefis, Anne Caroline, Matthias Augustin, Katharina Heinke Schlünzen, Jürgen Oßenbrügge, and Jobst Augustin. 2018. "How Does the Urban Environment Affect Health and Well-Being? A Systematic Review" Urban Science 2, no. 1: 21. https://0-doi-org.brum.beds.ac.uk/10.3390/urbansci2010021