
Interferon-α2b Treatment for COVID-19 Is Associated with Improvements in Lung Abnormalities

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Treatments
2.2. Laboratory Tests
2.3. CT Examination and Imaging Evaluation
2.4. Statistical Analyses
3. Results
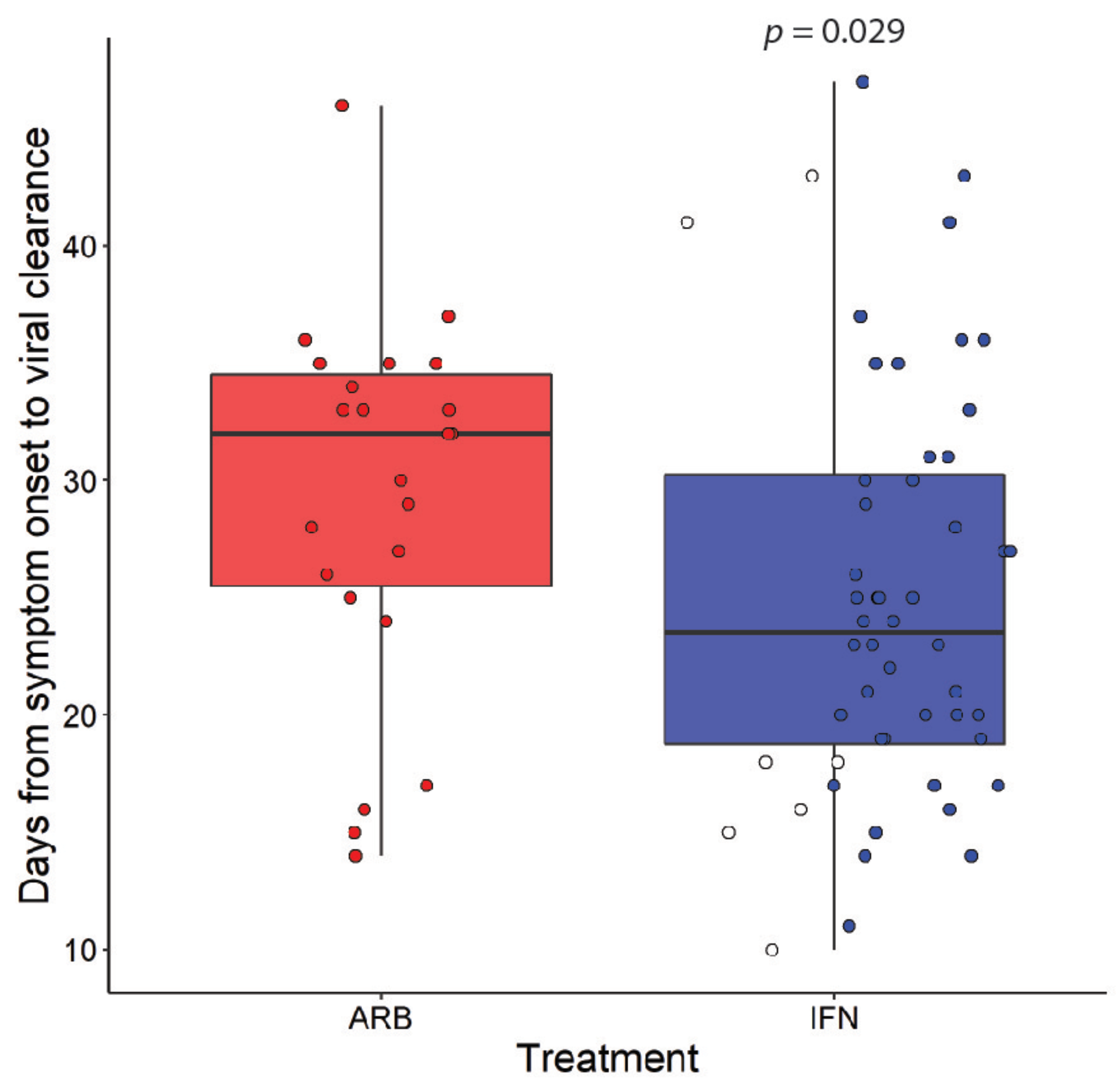
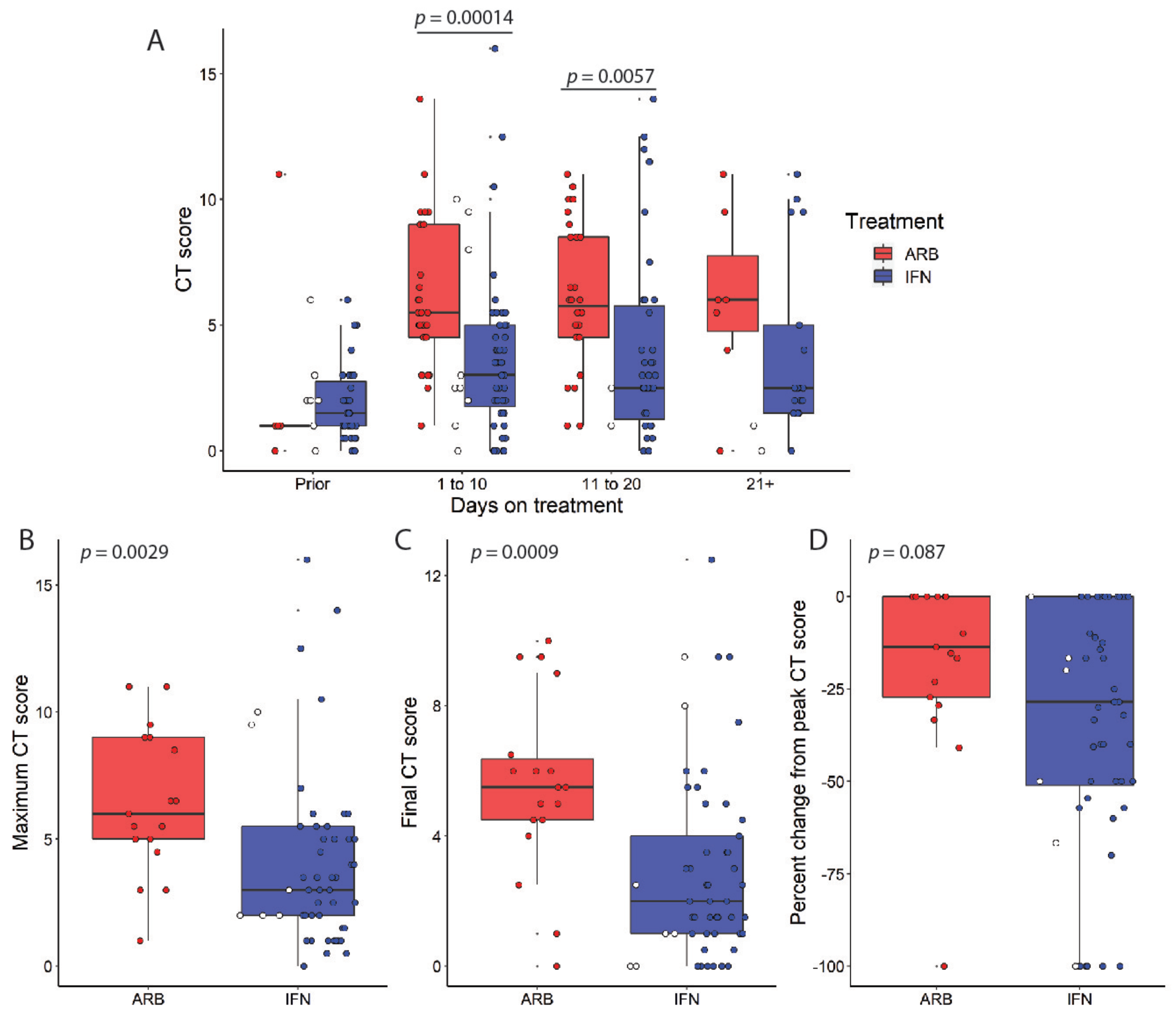
3.1. Lower CT Scores in COVID19 Patients Following IFNa2b Treatment
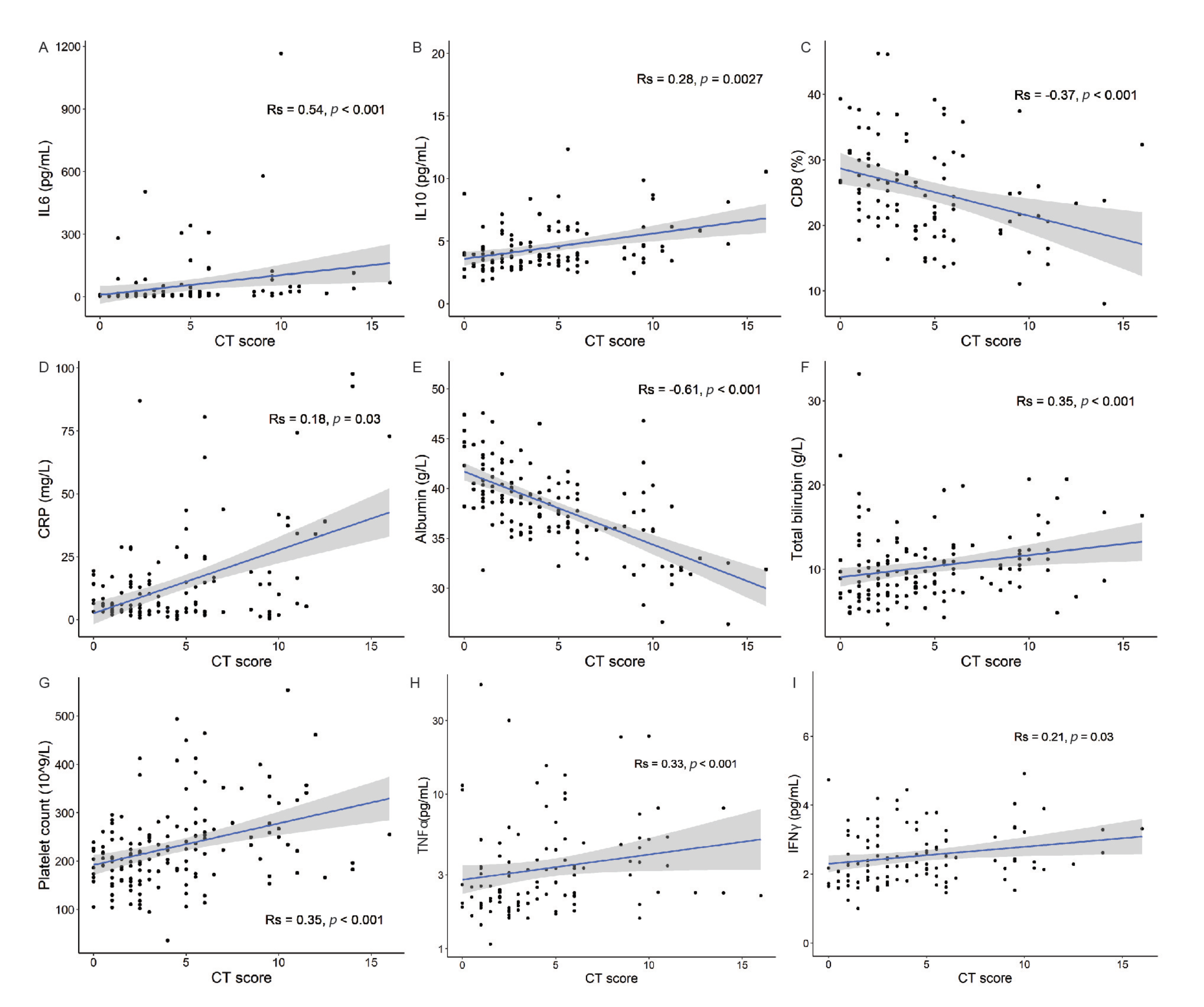
3.2. CT Score Severity Correlates with Clinically Relevant Biomarkers of Disease Severity
3.3. Mixed-Effects Modeling Reveals CRP, Albumin, and Age as the Strongest Predictors of CT Scores
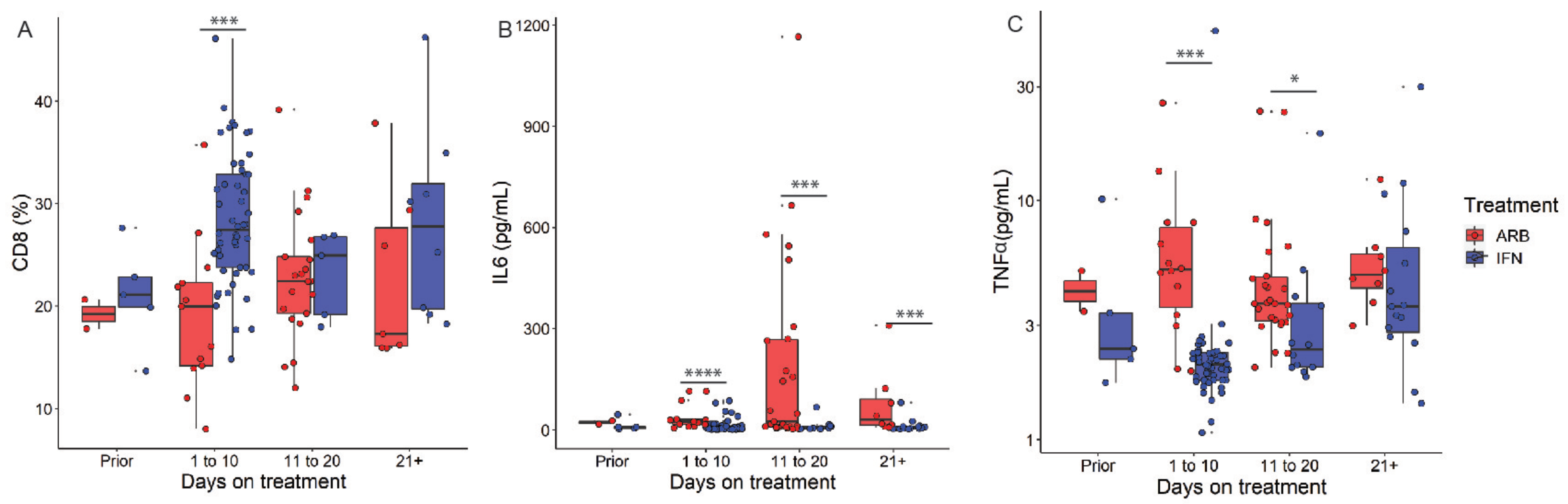
3.4. IFN Effects on Critical Predictors of Worsening Lung Abnormalities
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flanagan, K.L.; Best, E.; Crawford, N.W.; Giles, M.; Koirala, A.; Macartney, K.; Russell, F.; Teh, B.W.; Wen, S.C. Progress and Pitfalls in the Quest for Effective SARS-CoV-2 (COVID-19) Vaccines. Front. Immunol. 2020, 11, 579250. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Renia, L.; Macary, P.A.; Ng, L. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Ghaebi, M.; Osali, A.; Valizadeh, H.; Roshangar, L.; Ahmadi, M. Vaccine development and therapeutic design for 2019-nCoV/SARS-CoV-2: Challenges and chances. J. Cell. Physiol. 2020, 1–12. [Google Scholar] [CrossRef]
- Wang, B.X.; Fish, E.N. Global virus outbreaks: Interferons as 1st responders. Semin. Immunol. 2019, 43, 101300. [Google Scholar] [CrossRef]
- Zhou, Q.; Chen, V.; Shannon, C.P.; Wei, X.-S.; Xiang, X.; Wang, X.; Wang, Z.-H.; Tebbutt, S.J.; Kollmann, T.R.; Fish, E.N. Interferon-α2b treatment for COVID-19. Front. Immunol. 2020, 11, 1061. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-Y.; Liao, C.-H.; Wang, Q.; Tan, Y.-J.; Luo, R.; Qiu, Y.; Ge, X.-Y. The ORF6, ORF8 and nucleocapsid proteins of SARS-CoV-2 inhibit type I interferon signaling pathway. Virus Res. 2020, 286, 198074. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.-C.; Uhl, S.; Hoagland, D.; Moller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced host response to SARS-CoV-2 drives development of COVID-19. Cell 2020, 181, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Chan, J.F.-W.; Wang, Y.; Yuen, T.T.-T.; Chai, Y.; Hou, Y.; Shuai, H.; Yang, D.; Hu, B.; Huang, X.; et al. Comparative Replication and Immune Activation Profiles of SARS-CoV-2 and SARS-CoV in Human Lungs: An Ex Vivo Study with Implications for the Pathogenesis of COVID-19. Clin. Infect. Dis. 2020, 71, 1400–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bost, P.; Giladi, A.; Liu, Y.; Bendjelal, Y.; Xu, G.; David, E.; Blecher-Gonen, R.; Cohen, M.; Medaglia, C.; Li, H.; et al. Host-viral infection maps reveal signatures of severe COVID-19 patients. Cell 2020, 181, 1475–1488. [Google Scholar] [CrossRef]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K.; et al. Clinically Applicable AI System for Accurate Diagnosis, Quantitative Measurements, and Prognosis of COVID-19 Pneumonia Using Computed Tomography. Cell 2020, 181, 1423–1433. [Google Scholar] [CrossRef]
- Shen, C.; Yu, N.; Cai, S.; Zhou, J.; Sheng, J.; Liu, K.; Zhou, H.; Guo, Y.; Niu, G. Quantitative computed tomography analysis for stratifying the severity of Coronavirus Disease 2019. J. Pharm. Anal. 2020, 10, 123–129. [Google Scholar] [CrossRef]
- Tao, A.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Li, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing for Coronavirus Diseases 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 1–10. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Meile, M.; Müller, B.; Kulkarni, P.; Schutz, P. Management of patients with respiratory infections in primary care: Procalcitonin, C-reactive protein, or both? Expert Rev. Respir. Med. 2015, 9, 587–601. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Chen, R.; Wu, T.; Wei, X.; Guo, A. Association between point-of-care CRP testing and antibiotic prescribing in respiratory tract infections: A systemic review and meta-analysis of primary care studies. Br. J. Gen. Pract. 2013, 63, e787–e794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahu, B.R.; Kampa, R.K.; Padhi, A.; Panda, A.K. C-reactive protein: A promising biomarker for poor prognosis in COVID-19 infection. Clin. Chim. Acta 2020, 509, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Huan, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef]
- Aziz, M.; Fatima, R.; Lee-Smith, W.; Assaly, R. The association of low serum albumin level with severe COVID-19: A systematic review and meta-analysis. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef]
- Tang, D.; Comish, P.B.; Kang, R. The hallmarks of COVID-19 disease. PLoS Pathog. 2020, 16, e1008536. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | ARB | IFN | ||||
|---|---|---|---|---|---|---|
| Rs | p | Rs | p | Rs | p | |
| IL-2 | 0.190 | 0.047 | −0.017 | 0.919 | 0.047 | 0.696 |
| IL-4 | 0.097 | 0.313 | −0.343 | 0.032 | −0.004 | 0.977 |
| IL-6 | 0.542 | 0.000 | 0.110 | 0.506 | 0.434 | 0.000 |
| IL-10 | 0.283 | 0.003 | 0.163 | 0.321 | 0.361 | 0.002 |
| TNF-α | 0.272 | 0.004 | 0.156 | 0.342 | −0.030 | 0.801 |
| IFN-γ | 0.212 | 0.026 | −0.092 | 0.579 | 0.172 | 0.151 |
| CD3 cells | −0.114 | 0.265 | 0.300 | 0.076 | −0.265 | 0.037 |
| CD4+ T cells | 0.119 | 0.243 | 0.312 | 0.064 | 0.038 | 0.768 |
| CD8+ T cells | −0.371 | 0.000 | −0.292 | 0.085 | −0.349 | 0.005 |
| B lymphocytes | 0.106 | 0.338 | 0.046 | 0.844 | 0.158 | 0.219 |
| NK cell | 0.159 | 0.152 | −0.267 | 0.242 | 0.166 | 0.198 |
| CD4:CD8 ratio | 0.313 | 0.002 | 0.302 | 0.074 | 0.252 | 0.049 |
| white blood cells | 0.058 | 0.478 | −0.019 | 0.909 | −0.098 | 0.301 |
| neutrophils | 0.066 | 0.419 | 0.031 | 0.853 | −0.099 | 0.297 |
| lymphocytes | −0.093 | 0.256 | −0.088 | 0.601 | −0.113 | 0.230 |
| platelets | 0.355 | 0.000 | 0.200 | 0.229 | 0.303 | 0.001 |
| hemoglobin | −0.125 | 0.124 | 0.190 | 0.254 | −0.183 | 0.051 |
| alanine transaminase | 0.229 | 0.006 | 0.406 | 0.013 | 0.268 | 0.006 |
| aspartate aminotransferase | 0.255 | 0.002 | 0.541 | 0.001 | 0.251 | 0.010 |
| albumin | −0.620 | 0.000 | −0.292 | 0.079 | −0.701 | 0.000 |
| total bilirubin | 0.286 | 0.001 | −0.037 | 0.829 | 0.215 | 0.028 |
| direct bilirubin | 0.197 | 0.019 | −0.110 | 0.518 | 0.201 | 0.040 |
| creatinine | 0.093 | 0.270 | −0.078 | 0.647 | −0.027 | 0.781 |
| blood urea nitrogen | 0.007 | 0.931 | −0.064 | 0.706 | −0.037 | 0.708 |
| glucose | 0.499 | 0.000 | 0.316 | 0.684 | 0.459 | 0.000 |
| CRP | 0.179 | 0.033 | 0.290 | 0.073 | 0.235 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Q.; MacArthur, M.R.; He, X.; Wei, X.; Zarin, P.; Hanna, B.S.; Wang, Z.-H.; Xiang, X.; Fish, E.N. Interferon-α2b Treatment for COVID-19 Is Associated with Improvements in Lung Abnormalities. Viruses 2021, 13, 44. https://0-doi-org.brum.beds.ac.uk/10.3390/v13010044
Zhou Q, MacArthur MR, He X, Wei X, Zarin P, Hanna BS, Wang Z-H, Xiang X, Fish EN. Interferon-α2b Treatment for COVID-19 Is Associated with Improvements in Lung Abnormalities. Viruses. 2021; 13(1):44. https://0-doi-org.brum.beds.ac.uk/10.3390/v13010044
Chicago/Turabian StyleZhou, Qiong, Michael R. MacArthur, Xinliang He, Xiaoshan Wei, Payam Zarin, Bola S. Hanna, Zi-Hao Wang, Xuan Xiang, and Eleanor N. Fish. 2021. "Interferon-α2b Treatment for COVID-19 Is Associated with Improvements in Lung Abnormalities" Viruses 13, no. 1: 44. https://0-doi-org.brum.beds.ac.uk/10.3390/v13010044