
COVID-19 In-Hospital Mortality in People with Diabetes Is Driven by Comorbidities and Age—Propensity Score-Matched Analysis of Austrian National Public Health Institute Data

 , , , , , , ,
on behalf of the COVID-19 in Diabetes in Austria Study Groupadd
Show full author list
, , , , , , ,
on behalf of the COVID-19 in Diabetes in Austria Study Groupadd
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Data Extraction and Study Variables
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Comorbidities | ICD-10 Codes |
|---|---|
| Hypertension | I10.x, I11.x–I13.x, I15.x |
| Myocardial infarction/Ischaemic heart disease | I21.x, I22.x, I25.x |
| Congestive heart failure | I09.9, I11.0, I13.0, I13.2, I25.5, I42.0, I42.5–I42.9, I43.x, I50.x, P29.0 |
| Cardiac arrhythmias | I44.1–I44.3, I45.6, I45.9, I47.x–I49.x, R00.0, R00.1, R00.8, T82.1, Z45.0, Z95.0 |
| Valvular disease | A52.0, I05.x–I08.x, I09.1, I09.8, I34.x–I39.x, Q23.0–Q23.3, Z95.2–Z95.4 |
| Peripheral vascular disease | I70.x, I71.x, I73.1, I73.8, I73.9, I77.1, I79.0, I79.2, K55.1, K55.8, K55.9, Z95.8, Z95.9 |
| Cerebrovascular disease | G45.x, G46.x, H34.0, I60.x–I69.x |
| Dementia | F00.x–F03.x, F05.1, G30.x, G31.1 |
| Chronic obstructive pulmonary disease | I27.8, I27.9, J40.x–J47.x, J60.x–J67.x, J68.4, J70.1, J70.3 |
| Pulmonary circulation disorders | I26.x, I27.x, I28.0, I28.8, I28.9 |
| Rheumatic disease | M05.x, M06.x, M31.5, M32.x–M34.x, M35.1, M35.3, M36.0 |
| Peptic ulcer disease | K25.x–K28.x |
| Liver disease | B18.x, K70.0–K70.3, K70.9, K71.3–K71.5, K71.7, K73.x, K74.x, K76.0, K76.2–K76.4, K76.8, K76.9, Z94.4, I85.0, I85.9, I86.4, I98.2, K70.4, K71.1, K72.1, K72.9, K76.5, K76.6, K76.7 |
| Diabetes | E10.x, E11.x, E12.x, E13.x, E14.x |
| Paralysis | G04.1, G11.4, G80.1, G80.2, G81.x, G82.x, G83.0–G83.4, G83.9 |
| Other neurological disorders | G10.x–G13.x, G20.x–G22.x, G25.4, G25.5, G31.2, G31.8, G31.9, G32.x, G35.x–G37.x, G40.x, G41.x, G93.1, G93.4, R47.0, R56.x |
| Hypothyroidism | E00.x–E03.x, E89.0 |
| Renal disease | I12.0, I13.1, N03.2–N03.7, N05.2–N05.7, N18.x, N19.x, N25.0, Z49.0–Z49.2, Z94.0, Z99.2 |
| Any malignancy, except malignant neoplasm of skin | C00.x – C26.x, C30.x – C34.x, C37.x – C41.x, C43.x, C45.x – C58.x, C60.x – C76.x, C81.x – C85.x, C88.x, C90.x – C97.x |
| Metastatic solid tumour | C77.x–C80.x |
| AIDS/HIV | B20.x–B22.x, B24.x |
| Rheumatoid arthritis/collagen vascular diseases | L94.0, L94.1, L94.3, M05.x, M06.x, M08.x, M12.0, M12.3, M30.x, M31.0–M31.3, M32.x–M35.x, M45.x, M46.1, M46.8, M46.9 |
| Coagulopathy | D65–D68.x, D69.1, D69.3–D69.6 |
| Fluid and electrolyte disorders | E22.2, E86.x, E87.x |
| Blood loss anaemia | D50.0 |
| Deficiency anaemia | D50.8, D50.9, D51.x–D53.x |
| Alcohol abuse | F10, E52, G62.1, I42.6, K29.2, K70.0, K70.3, K70.9, T51.x, Z50.2, Z71.4, Z72.1 |
| Drug abuse | F11.x–F16.x, F18.x, F19.x, Z71.5, Z72.2 |
| Psychoses | F20.x, F22.x–F25.x, F28.x, F29.x, F30.2, F31.2, F31.5 |
| Depression | F20.4, F31.3–F31.5, F32.x, F33.x, F34.1, F41.2, F43.2 |
References
- WHO. Situation by Country, Territory & Area. Available online: https://covid19.who.int (accessed on 27 September 2021).
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/mortality-risk-covid (accessed on 9 July 2021).
- Grasselli, G.; Zangrillo, A.; Zanella, A. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Shi, Q.; Zhang, X.; Jiang, F.; Zhang, X.; Hu, N.; Bimu, C.; Feng, J.; Yan, S.; Guan, Y.; Xu, D.; et al. Clinical Characteristics and Risk Factors for Mortality of COVID-19 Patients With Diabetes in Wuhan, China: A Two-Center, Retrospective Study. Diabetes Care 2020, 43, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.-S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.; Ahmed, Z.; Younas, S. COVID-19 and comorbidities: Deleterious impact on infected patients. J. Infect. Public Health 2020, 13, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.I.; Yoon, S.; Lee, H.-J. Impact of comorbidity burden on mortality in patients with COVID-19 using the Korean health insurance database. Sci. Rep. 2021, 11, 6375. [Google Scholar] [CrossRef]
- Sourij, H.; Aziz, F.; Bräuer, A.; Ciardi, C.; Clodi, M.; Fasching, P.; Karolyi, M.; Kautzky-Willer, A.; Klammer, C.; Malle, O.; et al. COVID-19 fatality prediction in people with diabetes and prediabetes using a simple score upon hospital admission. Diabetes Obes. Metab. 2021, 23, 589–598. [Google Scholar] [CrossRef]
- Feldman, E.L.; Savelieff, M.G.; Hayek, S.S.; Pennathur, S.; Kretzler, M.; Pop-Busui, R. COVID-19 and Diabetes: A Collision and Collusion of Two Diseases. Diabetes 2020, 69, 2549–2565. [Google Scholar] [CrossRef]
- Heald, A.H.; Livingston, M.; Moreno, G.; Gibson, J.M. The risk factors potentially influencing risk of serious illness/death in people with diabetes, following SARS-CoV-2 infection: What needs to be done from here. Cardiovasc. Endocrinol. Metab. 2021, 10, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Sutter, W.; Duceau, B.; Vignac, M.; Bonnet, G.; Carlier, A.; Roussel, R.; Trimaille, A.; Pommier, T.; Guilleminot, P.; Sagnard, A.; et al. Association of diabetes and outcomes in patients with COVID-19: Propensity score-matched analyses from a French retrospective cohort. Diabetes Metab. 2021, 47, 101222. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity Measures for Use with Administrative Data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef]
- Corona, G.; Pizzocaro, A.; Vena, W.; Rastrelli, G.; Semeraro, F.; Isidori, A.M.; Pivonello, R.; Salonia, A.; Sforza, A.; Maggi, M. Diabetes is most important cause for mortality in COVID-19 hospitalized patients: Systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2021, 22, 275–296. [Google Scholar] [CrossRef]
- Shang, L.; Shao, M.; Guo, Q.; Shi, J.; Zhao, Y.; Xiaokereti, J.; Tang, B. Diabetes Mellitus is Associated with Severe Infection and Mortality in Patients with COVID-19: A Systematic Review and Meta-analysis. Arch. Med. Res. 2020, 51, 700–709. [Google Scholar] [CrossRef]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Zhang, Y.; Cui, Y.; Shen, M.; Zhang, J.; Liu, B.; Dai, M.; Chen, L.; Han, D.; Fan, Y.; Zeng, Y.; et al. Association of diabetes mellitus with disease severity and prognosis in COVID-19: A retrospective cohort study. Diabetes Res. Clin. Pract. 2020, 165, 108227. [Google Scholar] [CrossRef]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes/Metab. Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.A.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhong, X.; Wang, Y.; Zeng, X.; Luo, T.; Liu, Q. Clinical determinants of the severity of COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0250602. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Xu, J.; Xiao, W.; Shi, L.; Yang, H. The association of diabetes with COVID-19 disease severity: Evidence from adjusted effect estimates. Hormones 2021, 20, 409–414. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.D.; Zheng, M.-H.; Targher, G. Diabetes as a risk factor for greater COVID-19 severity and in-hospital death: A meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1236–1248. [Google Scholar] [CrossRef]
- Gao, X.; Ke, C.; Liu, H.; Liu, W.; Li, K.; Yu, B.; Sun, M. Large-scale Metabolomic Analysis Reveals Potential Biomarkers for Early Stage Coronary Atherosclerosis. Sci. Rep. 2017, 7, 11817. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yang, D.; Cheng, B.; Chen, J.; Peng, A.; Yang, C.; Liu, C.; Xiong, M.; Deng, A.; Zhang, Y.; et al. Clinical Characteristics and Outcomes of Patients With Diabetes and COVID-19 in Association With Glucose-Lowering Medication. Diabetes Care 2020, 43, 1399–1407. [Google Scholar] [CrossRef] [PubMed]
- Ran, J.; Zhao, S.; Han, L.; Ge, Y.; Chong, M.K.; Cao, W.; Sun, S. Increase in Diabetes Mortality Associated With COVID-19 Pandemic in the US. Diabetes Care 2021, 44, e146–e147. [Google Scholar] [CrossRef]

| Variables | Unmatched Cohort | PSM Cohort | ||||||
|---|---|---|---|---|---|---|---|---|
| All | No Diabetes n (%) | Diabetes n (%) | SMD | p-Value | No Diabetes n (%) | Diabetes n (%) | SMD | |
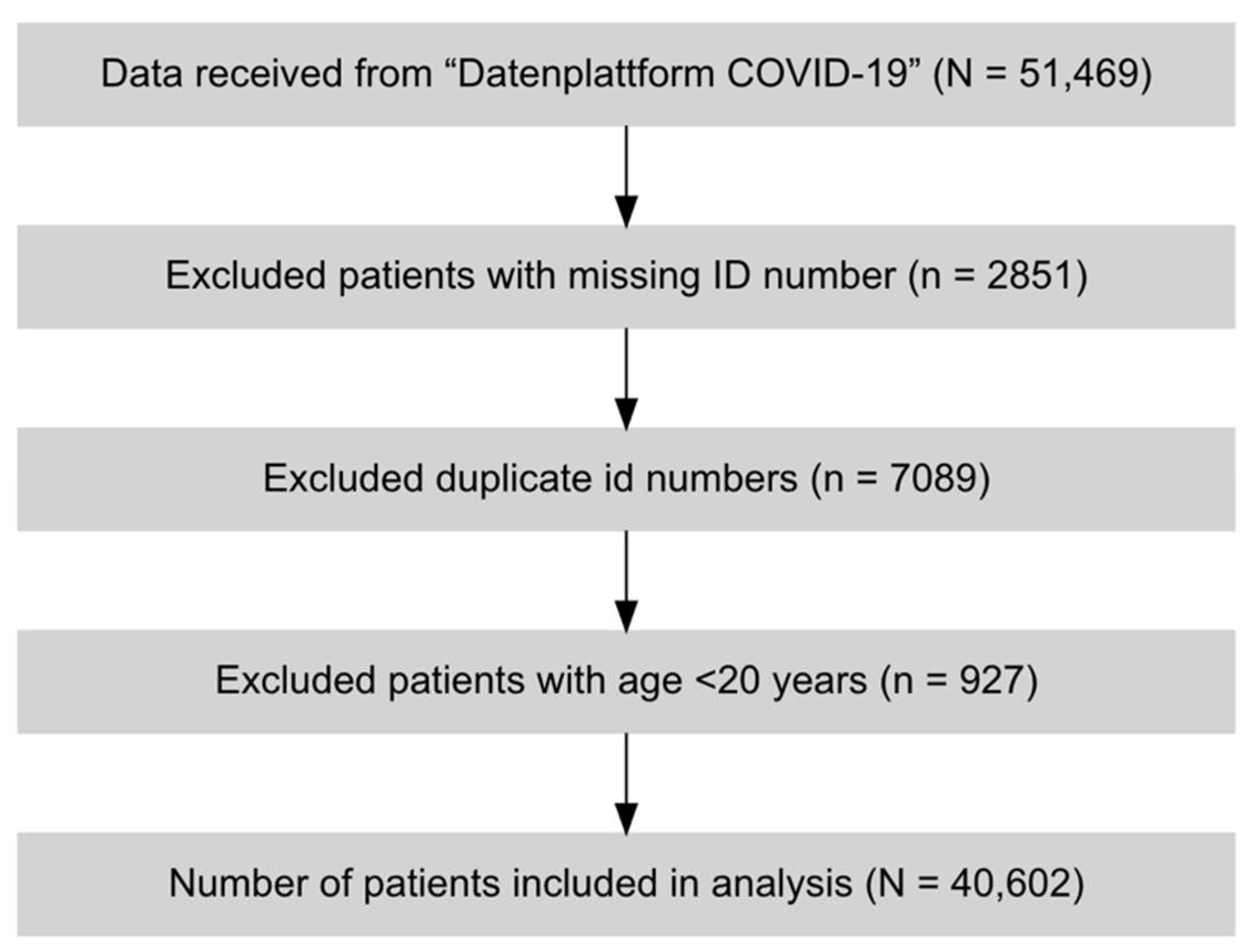
| N | 40,602 | 35,631 (87.8) | 4971 (12.2) | 4971 (50.0) | 4971 (50.0) | |||
| Men | 21,278 (52.4) | 18,419 (51.7) | 2859 (57.5) | 0.117 | <0.001 | 2839 (57.1) | 2859 (57.5) | 0.008 |
| Women | 19,324 (47.6) | 17,212 (48.3) | 2112 (42.5) | 2132 (42.9) | 2112 (42.5) | |||
| Age categories | ||||||||
| 20–29 | 1057 (2.6) | 1050 (2.9) | 7 (0.1) | 0.403 | <0.001 | 5 (0.1) | 7 (0.1) | 0.028 |
| 30–39 | 1576 (3.9) | 1536 (4.3) | 40 (0.8) | 44 (0.9) | 40 (0.8) | |||
| 40–49 | 2479 (6.1) | 2306 (6.5) | 173 (3.5) | 177 (3.6) | 173 (3.5) | |||
| 50–59 | 5363 (13.2) | 4751 (13.3) | 612 (12.3) | 643 (12.9) | 612 (12.3) | |||
| 60–69 | 6674 (16.4) | 5743 (16.1) | 931 (18.7) | 931 (18.7) | 931 (18.7) | |||
| 70–79 | 9664 (23.8) | 8133 (22.8) | 1531 (30.8) | 1490 (30.0) | 1531 (30.8) | |||
| 80–89 | 10,532 (25.9) | 9144 (25.7) | 1388 (27.9) | 1387 (27.9) | 1388 (27.9) | |||
| 90+ | 3257 (8.0) | 2968 (8.3) | 289 (5.8) | 294 (5.9) | 289 (5.8) | |||
| ICU admission | 5968 (14.7) | 5057 (14.2) | 911 (18.3) | 0.110 | <0.001 | 812 (16.3) | 911 (18.3) | 0.053 |
| In-hospital mortality | 6569 (16.2) | 5632 (15.8) | 937 (18.8) | 0.080 | <0.001 | 881 (17.7) | 937 (18.8) | 0.029 |
| Comorbidities | ||||||||
| Myocardial infarction | 340 (0.8) | 236 (0.7) | 104 (2.1) | 0.123 | <0.001 | 107 (2.2) | 104 (2.1) | 0.004 |
| Cardiac arrhythmias | 4235 (10.4) | 3134 (8.8) | 1101 (22.1) | 0.376 | <0.001 | 1217 (24.5) | 1101 (22.1) | 0.055 |
| Valvular heart disease | 990 (2.4) | 738 (2.1) | 252 (5.1) | 0.162 | <0.001 | 307 (6.2) | 252 (5.1) | 0.048 |
| Hypertension | 10,538 (26.0) | 7209 (20.2) | 3329 (67.0) | 1.069 | <0.001 | 3002 (60.4) | 3329 (67.0) | 0.137 |
| CHF | 2011 (5.0) | 1381 (3.9) | 630 (12.7) | 0.323 | <0.001 | 602 (12.1) | 630 (12.7) | 0.017 |
| PVD | 1341 (3.3) | 855 (2.4) | 486 (9.8) | 0.312 | <0.001 | 385 (7.7) | 486 (9.8) | 0.072 |
| Stroke | 1212 (3.0) | 834 (2.3) | 378 (7.6) | 0.244 | <0.001 | 378 (7.6) | 378 (7.6) | 0.002 |
| COPD | 2271 (5.6) | 1699 (4.8) | 572 (11.5) | 0.248 | <0.001 | 568 (11.4) | 572 (11.5) | 0.003 |
| Pulmonary circulation disorders | 591 (1.5) | 474 (1.3) | 117 (2.4) | 0.076 | <0.001 | 129 (2.6) | 117 (2.4) | 0.016 |
| Dementia | 2050 (5.0) | 1570 (4.4) | 480 (9.7) | 0.206 | <0.001 | 488 (9.8) | 480 (9.7) | 0.005 |
| Rheumatoid disease | 254 (0.6) | 198 (0.6) | 56 (1.1) | 0.063 | <0.001 | 77 (1.5) | 56 (1.1) | 0.037 |
| Peptic ulcer disease | 86 (0.2) | 62 (0.2) | 24 (0.5) | 0.054 | <0.001 | 20 (0.4) | 24 (0.5) | 0.012 |
| Liver disease | 1031 (2.5) | 672 (1.9) | 359 (7.2) | 0.258 | <0.001 | 305 (6.1) | 359 (7.2) | 0.044 |
| Paralysis | 126 (0.3) | 98 (0.3) | 28 (0.6) | 0.045 | 0.001 | 34 (0.7) | 28 (0.6) | 0.015 |
| Other neurological disorders | 1071 (2.6) | 839 (2.4) | 232 (4.7) | 0.126 | <0.001 | 201 (4.0) | 232 (4.7) | 0.031 |
| Renal disease | 3173 (7.8) | 2092 (5.9) | 1081 (21.7) | 0.473 | <0.001 | 1051 (21.1) | 1081 (21.7) | 0.015 |
| Cancer | 1318 (3.2) | 1079 (3.0) | 239 (4.8) | 0.092 | <0.001 | 229 (4.6) | 239 (4.8) | 0.009 |
| Hypothyroidism | 1335 (3.3) | 993 (2.8) | 342 (6.9) | 0.192 | <0.001 | 347 (7.0) | 342 (6.9) | 0.004 |
| Coagulation disorders | 252 (0.6) | 179 (0.5) | 73 (1.5) | 0.098 | <0.001 | 46 (0.9) | 73 (1.5) | 0.050 |
| Fluid and electrolyte disorders | 1433 (3.5) | 1131 (3.2) | 302 (6.1) | 0.138 | 0.001 | 307 (6.2) | 302 (6.1) | 0.004 |
| Blood loss anaemia | 37 (0.1) | 28 (0.1) | 9 (0.2) | 0.028 | 0.046 | 8 (0.2) | 9 (0.2) | 0.005 |
| Deficiency anaemia | 371 (0.9) | 259 (0.7) | 112 (2.3) | 0.126 | <0.001 | 71 (1.4) | 112 (2.3) | 0.061 |
| Alcohol abuse | 241 (0.6) | 190 (0.5) | 51 (1.0) | 0.056 | <0.001 | 77 (1.5) | 51 (1.0) | 0.046 |
| Drug abuse | 69 (0.2) | 54 (0.2) | 15 (0.3) | 0.032 | 0.026 | 21 (0.4) | 15 (0.3) | 0.020 |
| Psychosis | 151 (0.4) | 112 (0.3) | 39 (0.8) | 0.064 | <0.001 | 30 (0.6) | 39 (0.8) | 0.022 |
| Depression | 1074 (2.6) | 826 (2.3) | 248 (5.0) | 0.143 | <0.001 | 248 (5.0) | 248 (5.0) | 0.001 |
| Charlson Comorbidity Index | ||||||||
| 0 | 30,361 (74.8) | 28,101 (78.9) | 2260 (45.5) | 0.744 | <0.001 | 2306 (46.4) | 2260 (45.5) | 0.035 |
| 1–2 | 7484 (18.4) | 5703 (16.0) | 1781 (35.8) | 1802 (36.3) | 1781 (35.8) | |||
| 3–4 | 2186 (5.4) | 1441 (4.0) | 745 (15.0) | 694 (14.0) | 745 (15.0) | |||
| 5+ | 571 (1.4) | 386 (1.1) | 185 (3.7) | 169 (3.4) | 185 (3.7) | |||
| Variables | Unmatched Cohort | PSM Cohort | ||||
|---|---|---|---|---|---|---|
| No ICU Admission (N = 34,634) n (%) | ICU Admission (N = 5968) n (%) | OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Diabetes | 4060 (11.7) | 911 (15.3) | 1.36 (1.25–1.47) | <0.001 | 1.15 (1.04–1.28) | 0.009 |
| Men | 17,430 (50.3) | 3848 (64.5) | Reference | Reference | ||
| Women | 17,204 (49.7) | 2120 (35.5) | 0.56 (0.53–0.59) | <0.001 | 0.56 (0.50–0.63) | <0.001 |
| Age groups | ||||||
| 20–29 | 982 (2.8) | 75 (1.3) | Reference | Reference | ||
| 30–39 | 1427 (4.1) | 149 (2.5) | 1.37 (1.03–1.83) | 0.033 | 0.33 (0.09–1.47) | 0.138 |
| 40–49 | 2161 (6.2) | 318 (5.3) | 1.92 (1.49–2.52) | <0.001 | 0.60 (0.18–2.39) | 0.441 |
| 50–59 | 4456 (12.9) | 907 (15.2) | 2.66 (2.10–3.43) | <0.001 | 0.54 (0.17–2.11) | 0.348 |
| 60–69 | 5261 (15.2) | 1413 (23.7) | 3.51 (2.77–4.51) | <0.001 | 0.65 (0.20–2.54) | 0.507 |
| 70–79 | 7838 (22.6) | 1826 (30.6) | 3.04 (2.41–3.90) | <0.001 | 0.48 (0.15–1.89) | 0.271 |
| 80–89 | 9365 (27.0) | 1167 (19.6) | 1.63 (1.29–2.09) | <0.001 | 0.22 (0.07–0.86) | 0.032 |
| 90+ | 3144 (9.1) | 113 (1.9) | 0.47 (0.35–0.64) | <0.001 | 0.04 (0.01–0.17) | <0.001 |
| Comorbidities | ||||||
| Myocardial infarction | 239 (0.7) | 101 (1.7) | 2.48 (1.95–3.12) | <0.001 | 2.27 (1.68–3.04) | <0.001 |
| Cardiac arrhythmias | 3612 (10.4) | 623 (10.4) | 1.00 (0.91–1.09) | 0.978 | 0.93 (0.82–1.05) | 0.267 |
| Valvular heart diseases | 844 (2.4) | 146 (2.5) | 1.00 (0.84–1.20) | 0.957 | 0.87 (0.69–1.10) | 0.255 |
| Hypertension | 8929 (25.8) | 1609 (27.0) | 1.06 (1.00–1.13) | 0.056 | 1.09 (0.98–1.22) | 0.112 |
| Congestive heart failure | 1676 (4.8) | 335 (5.6) | 1.17 (1.04–1.32) | 0.012 | 1.25 (1.08–1.45) | 0.004 |
| Peripheral vascular disease | 1119 (3.2) | 222 (3.7) | 1.16 (1.00–1.34) | 0.054 | 1.07 (0.89–1.28) | 0.449 |
| Stroke | 1024 (3.0) | 188 (3.1) | 1.07 (0.91–1.25) | 0.416 | 1.01 (0.83–1.22) | 0.915 |
| COPD | 1854 (5.3) | 417 (7.0) | 1.33 (1.19–1.48) | <0.001 | 1.23 (1.05–1.43) | 0.010 |
| Pulmonary circulation disorders | 436 (1.3) | 155 (2.6) | 2.09 (1.73–2.51) | <0.001 | 2.19 (1.65–2.87) | <0.001 |
| Dementia | 1975 (5.7) | 75 (1.3) | 0.21 (0.17–0.26) | <0.001 | 0.14 (0.09–0.20) | <0.001 |
| Rheumatoid disorders | 227 (0.7) | 27 (0.5) | 0.69 (0.45–1.01) | 0.059 | 0.65 (0.37–1.07) | 0.097 |
| Peptic ulcer disease | 68 (0.2) | 18 (0.3) | 1.55 (0.89–2.55) | 0.116 | 1.08 (0.46–2.21) | 0.852 |
| Liver disease | 848 (2.5) | 183 (3.1) | 1.26 (1.07–1.48) | 0.006 | 1.15 (0.94–1.40) | 0.173 |
| Paralysis | 105 (0.3) | 21 (0.3) | 1.17 (0.71–1.83) | 0.524 | 1.68 (0.92–2.91) | 0.091 |
| Other neurological disorders | 970 (2.8) | 101 (1.7) | 0.60 (0.48–0.73) | <0.001 | 0.56 (0.40–0.75) | <0.001 |
| Renal disease | 2741 (7.9) | 432 (7.2) | 0.91 (0.82–1.01) | 0.071 | 0.81 (0.71–0.93) | 0.002 |
| Cancer | 1128 (3.3) | 190 (3.2) | 0.98 (0.83–1.14) | 0.774 | 1.00 (0.78–1.27) | 0.999 |
| Hypothyroidism | 1157 (3.3) | 178 (3.0) | 0.89 (0.76–1.04) | 0.150 | 0.93 (0.75–1.14) | 0.508 |
| Coagulation disorders | 167 (0.5) | 85 (1.4) | 2.98 (2.29–3.87) | <0.001 | 4.06 (2.81–5.85) | <0.001 |
| Fluid and electrolyte disorders | 1280 (3.7) | 153 (2.6) | 0.69 (0.58–0.81) | <0.001 | 0.89 (0.71–1.11) | 0.292 |
| Deficiency anemia | 328 (0.9) | 43 (0.7) | 0.76 (0.55–1.04) | 0.084 | 0.72 (0.46–1.09) | 0.123 |
| Alcohol abuse | 188 (0.5) | 53 (0.9) | 1.65 (1.20–2.22) | 0.002 | 1.54 (1.01–2.29) | 0.046 |
| Psychosis | 126 (0.4) | 25 (0.4) | 1.16 (0.74–1.75) | 0.511 | 1.12 (0.58–1.99) | 0.721 |
| Depression | 937 (2.7) | 137 (2.3) | 0.85 (0.70–1.01) | 0.065 | 0.93 (0.72–1.18) | 0.552 |
| Charlson Comorbidity Index | ||||||
| 0 | 25,868 (74.7) | 4493 (75.3) | Reference | Reference | ||
| 1–2 | 6383 (18.4) | 1101 (18.4) | 0.99 (0.92–1.07) | 0.851 | 0.90 (0.80–1.01) | 0.083 |
| 3–4 | 1885 (5.4) | 301 (5.0) | 0.92 (0.81–1.04) | 0.188 | 0.84 (0.72–0.99) | 0.035 |
| 5+ | 498 (1.4) | 73 (1.2) | 0.85 (0.65–1.08) | 0.176 | 0.79 (0.58–1.05) | 0.110 |
| Variables | Unmatched Cohort | PSM Cohort | ||||
|---|---|---|---|---|---|---|
| No In-Hospital Mortality (N = 34,033) n (%) | In-Hospital Mortality (N = 6569) n (%) | OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Diabetes | 4034 (11.9) | 937 (14.3) | 1.24 (1.15–1.34) | <0.001 | 1.08 (0.97–1.19) | 0.146 |
| Men | 17,582 (51.7) | 3696 (56.3) | Reference | Reference | ||
| Women | 16,451 (48.3) | 2873 (43.7) | 0.83 (0.79–0.88) | <0.001 | 0.84 (0.76–0.94) | <0.001 |
| Age | ||||||
| 20–29 | 1048 (3.1) | 9 (0.1) | Reference | Reference | ||
| 30–39 | 1557 (4.6) | 19 (0.3) | 1.41 (0.65–3.31) | 0.396 | 0.14 (0.00–5.63) | 0.250 |
| 40–49 | 2444 (7.2) | 35 (0.5) | 1.65 (0.82–3.68) | 0.168 | 0.12 (0.01–3.42) | 0.165 |
| 50–59 | 5173 (15.2) | 190 (2.9) | 4.20 (2.28–8.92) | <0.001 | 0.46 (0.09–11.60) | 0.533 |
| 60–69 | 6093 (17.9) | 581 (8.8) | 10.90 (5.99–22.90) | <0.001 | 1.05 (0.20–25.80) | 0.965 |
| 70–79 | 8018 (23.6) | 1646 (25.1) | 23.50 (12.9–49.20) | <0.001 | 2.23 (0.43–54.80) | 0.402 |
| 80–89 | 7727 (22.7) | 2805 (42.7) | 41.50 (22.9–87.00) | <0.001 | 3.75 (0.72–92.40) | 0.133 |
| 90+ | 1973 (5.8) | 1284 (19.5) | 74.40 (40.9–157.00) | <0.001 | 6.80 (1.30–168.00) | 0.019 |
| ICU admission | 3991 (11.7) | 1977 (30.1) | 3.24 (3.04–3.45) | <0.001 | 3.09 (2.75–3.47) | <0.001 |
| Comorbidities | ||||||
| Myocardial infarction | 219 (0.6) | 121 (1.8) | 2.90 (2.31–3.62) | <0.001 | 2.27 (1.69–3.03) | <0.001 |
| Cardiac arrhythmias | 3160 (9.3) | 1075 (16.4) | 1.91 (1.77–2.06) | <0.001 | 1.78 (1.60–1.99) | <0.001 |
| Valvular heart disease | 751 (2.2) | 239 (3.6) | 1.67 (1.44–1.94) | <0.001 | 1.62 (1.32–1.96) | <0.001 |
| Hypertension | 8737 (25.7) | 1801 (27.4) | 1.09 (1.03–1.16) | 0.003 | 0.75 (0.68–0.84) | <0.001 |
| Congestive heart failure | 1326 (3.9) | 685 (10.4) | 2.87 (2.61–3.16) | <0.001 | 2.72 (2.38–3.10) | 0.000 |
| Peripheral vascular disease | 962 (2.8) | 379 (5.8) | 2.11 (1.86–2.38) | <0.001 | 1.78 (1.52–2.09) | <0.001 |
| Stroke | 887 (2.6) | 325 (4.9) | 1.95 (1.71–2.21) | <0.001 | 1.75 (1.47–2.07) | <0.001 |
| COPD | 1815 (5.3) | 456 (6.9) | 1.32 (1.19–1.47) | <0.001 | 1.20 (1.03–1.40) | 0.022 |
| Pulmonary circulation disorders | 457 (1.3) | 134 (2.0) | 1.53 (1.26–1.85) | <0.001 | 1.67 (1.24–2.21) | 0.001 |
| Dementia | 1344 (3.9) | 706 (10.7) | 2.93 (2.66–3.22) | <0.001 | 2.32 (2.00–2.68) | <0.001 |
| Rheumatoid disease | 205 (0.6) | 49 (0.7) | 1.24 (0.90–1.68) | 0.183 | 1.37 (0.90–2.03) | 0.140 |
| Peptic ulcer disease | 66 (0.2) | 20 (0.3) | 1.58 (0.93–2.56) | 0.087 | 1.33 (0.62–2.61) | 0.443 |
| Liver disease | 847 (2.5) | 184 (2.8) | 1.13 (0.96–1.32) | 0.144 | 1.03 (0.84–1.26) | 0.782 |
| Paralysis | 100 (0.3) | 26 (0.4) | 1.35 (0.86–2.06) | 0.183 | 0.77 (0.35–1.49) | 0.456 |
| Other neurological disorders | 774 (2.3) | 297 (4.5) | 2.04 (1.77–2.33) | <0.001 | 2.13 (1.72–2.62) | <0.001 |
| Renal disease | 2243 (6.6) | 930 (14.2) | 2.34 (2.15–2.54) | <0.001 | 2.28 (2.04–2.55) | <0.001 |
| Cancer | 965 (2.8) | 353 (5.4) | 1.95 (1.72–2.20) | <0.001 | 1.86 (1.51–2.28) | <0.001 |
| Hypothyroidism | 1171 (3.4) | 164 (2.5) | 0.72 (0.61–0.85) | <0.001 | 0.60 (0.47–0.76) | <0.001 |
| Coagulation disorders | 193 (0.6) | 59 (0.9) | 1.59 (1.18–2.12) | 0.003 | 1.66 (1.09–2.47) | 0.020 |
| Fluid and electrolyte disorders | 1172 (3.4) | 261 (4.0) | 1.16 (1.01–1.33) | 0.036 | 1.19 (0.97–1.45) | 0.094 |
| Deficiency anaemia | 307 (0.9) | 64 (1.0) | 1.08 (0.82–1.41) | 0.567 | 0.84 (0.55–1.24) | 0.394 |
| Alcohol abuse | 177 (0.5) | 64 (1.0) | 1.88 (1.40–2.50) | <0.001 | 1.44 (0.94–2.14) | 0.090 |
| Psychosis | 125 (0.4) | 26 (0.4) | 1.08 (0.69–1.63) | 0.714 | 1.15 (0.61–2.01) | 0.651 |
| Depression | 907 (2.7) | 167 (2.5) | 0.95 (0.80–1.12) | 0.575 | 0.84 (0.65–1.07) | 0.161 |
| Charlson Comorbidity Index | ||||||
| 0 | 26,400 (77.6) | 3961 (60.3) | Reference | Reference | ||
| 1–2 | 5752 (16.9) | 1732 (26.4) | 2.01 (1.88–2.14) | <0.001 | 2.47 (2.18–2.80) | <0.001 |
| 3–4 | 1491 (4.4) | 695 (10.6) | 3.11 (2.82–3.42) | <0.001 | 3.99 (3.44–4.62) | <0.001 |
| 5+ | 390 (1.1) | 181 (2.76) | 3.09 (2.58–3.70) | <0.001 | 4.40 (3.45–5.59) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, F.; Aberer, F.; Bräuer, A.; Ciardi, C.; Clodi, M.; Fasching, P.; Karolyi, M.; Kautzky-Willer, A.; Klammer, C.; Malle, O.; et al. COVID-19 In-Hospital Mortality in People with Diabetes Is Driven by Comorbidities and Age—Propensity Score-Matched Analysis of Austrian National Public Health Institute Data. Viruses 2021, 13, 2401. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122401
Aziz F, Aberer F, Bräuer A, Ciardi C, Clodi M, Fasching P, Karolyi M, Kautzky-Willer A, Klammer C, Malle O, et al. COVID-19 In-Hospital Mortality in People with Diabetes Is Driven by Comorbidities and Age—Propensity Score-Matched Analysis of Austrian National Public Health Institute Data. Viruses. 2021; 13(12):2401. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122401
Chicago/Turabian StyleAziz, Faisal, Felix Aberer, Alexander Bräuer, Christian Ciardi, Martin Clodi, Peter Fasching, Mario Karolyi, Alexandra Kautzky-Willer, Carmen Klammer, Oliver Malle, and et al. 2021. "COVID-19 In-Hospital Mortality in People with Diabetes Is Driven by Comorbidities and Age—Propensity Score-Matched Analysis of Austrian National Public Health Institute Data" Viruses 13, no. 12: 2401. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122401