
Achieving Influenza Vaccine Uptake Target in Canada via a Pharmacy-Led Telephone Discussion during the 2019–2020 Season

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Statistical Analysis
2.3. Patient and Public Involvement
3. Results
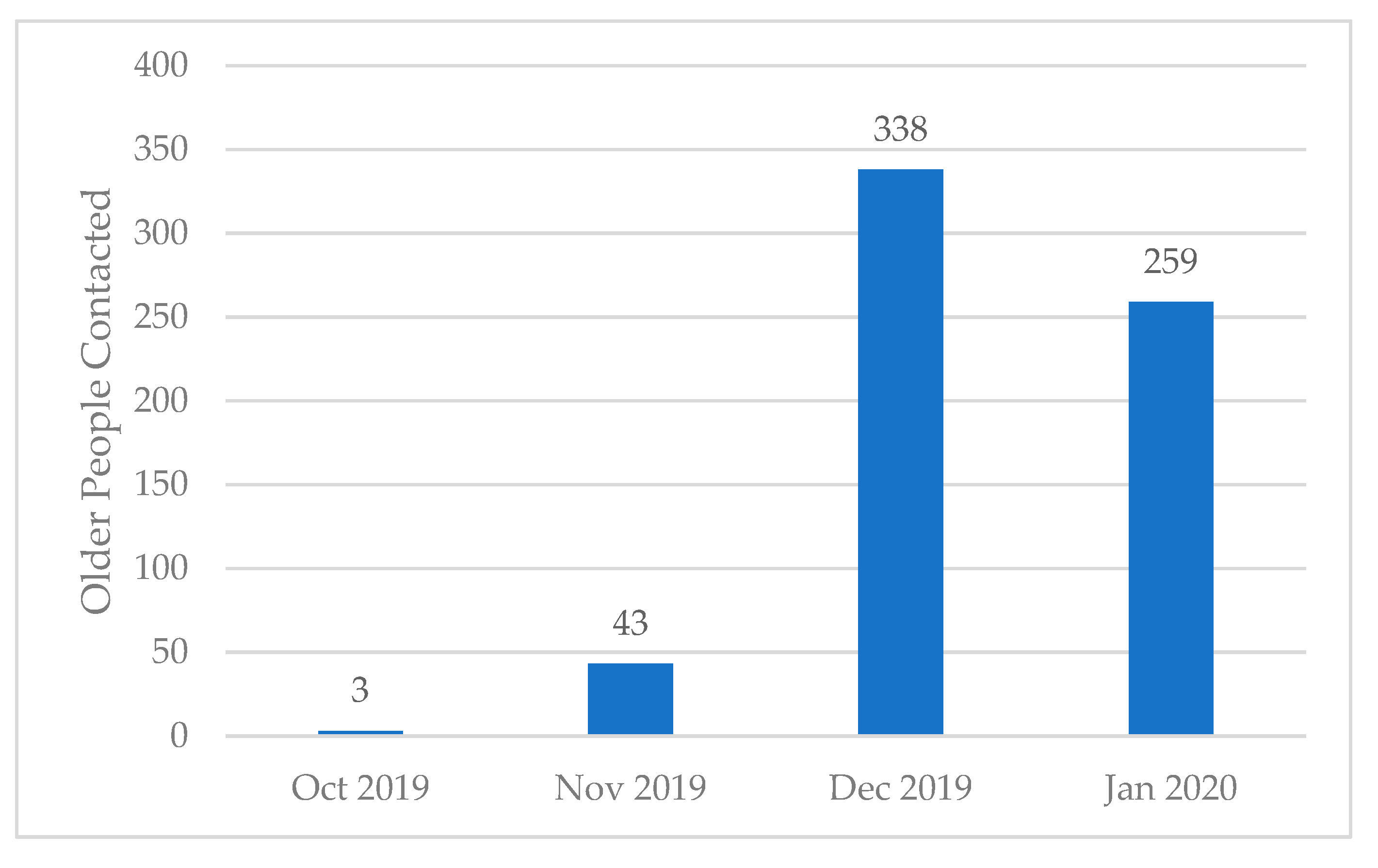
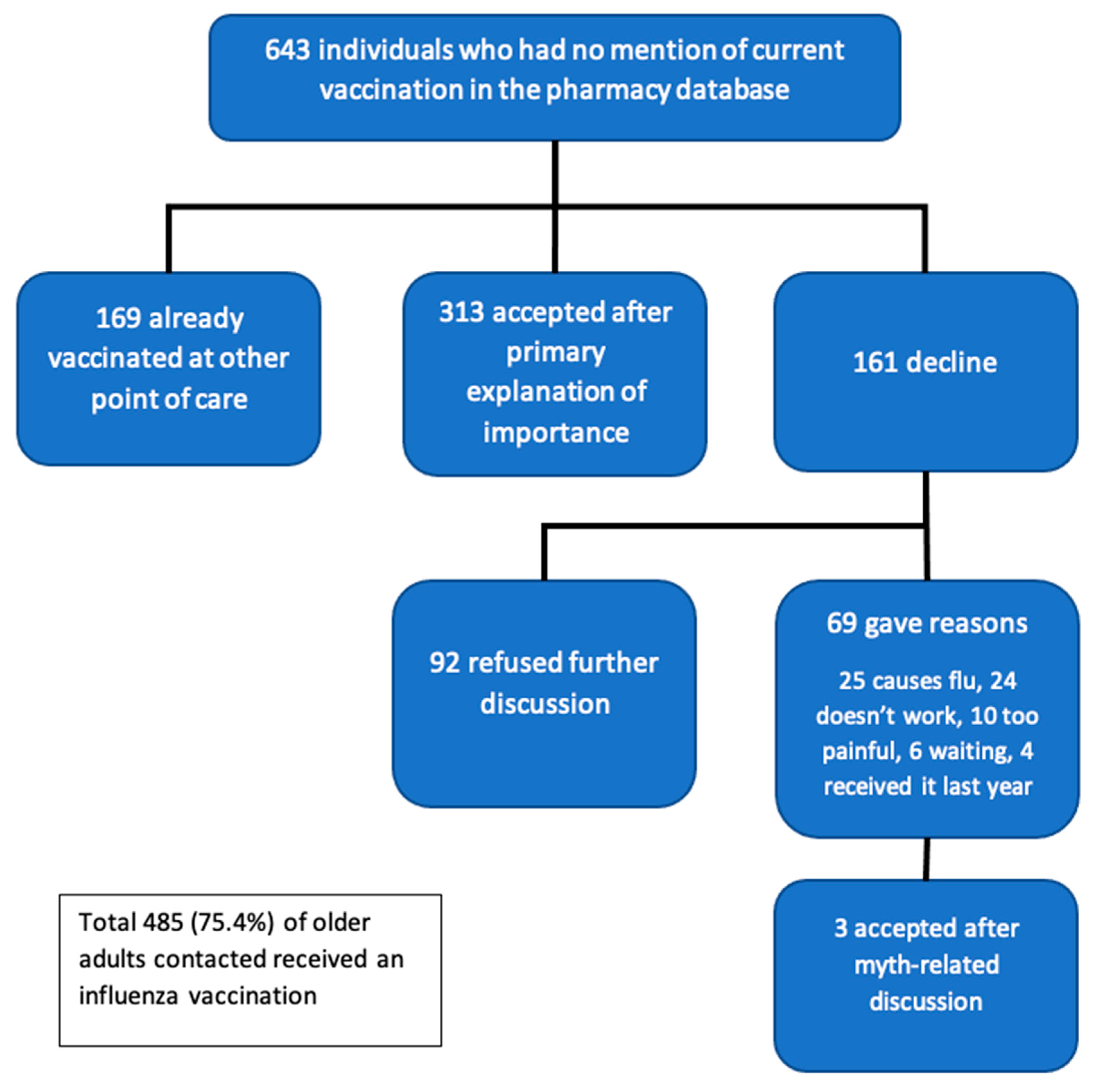
3.1. Evaluation of Primary Outcome
3.2. Reason for Declining the Influenza Vaccine and Efficacy of Correcting Myth
3.3. Interest in Receiving an Enhanced Influenza Vaccine
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Public Health Agency of Canada. Canadian Immunization Guide Chapter on Influenza and Statement on Seasonal Influenza Vaccine for 2020–2021. Available online: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/healthy-living/canadian-immunization-guide-statement-seasonal-influenza-vaccine-2020-2021/naci-2020-2021-seasonal-influenza-stmt-eng.pdf (accessed on 2 May 2020).
- Andrews, M.; Macdonald, S.; Ye, L.; Ambrose, A.; Mcneil, S.A. Impact of Frailty on Influenza Vaccine Effectiveness and Clinical Outcomes: Experience from the Canadian Immunization Research Network (CIRN) Serious Outcomes Surveillance (SOS) Network 2011/12 Season. 2016. Available online: https://idsa.confex.com/idsa/2016/webprogram/Paper59568.html (accessed on 31 July 2020).
- Center for Disease Control. Influenza-Pink Book. Available online: https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/flu.pdf (accessed on 31 July 2020).
- Public Health England. Immunisation against infectious disease-Chapter 19: Influenza. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/663694/Greenbook_chapter_19_Influenza_.pdf (accessed on 5 August 2018).
- World Health Organization. Prevention and control of influenza pandemics and annual epidemics. Available online: https://www.who.int/immunization/sage/1_WHA56_19_Prevention_and_control_of_influenza_pandemics.pdf?ua=1 (accessed on 31 July 2020).
- Service Canada. Vaccine uptake in Canadian adults: Highlights from the 2016 adult National Immunization Coverage Survey (aNICS). Available online: https://www.canada.ca/en/services/health/publications/healthy-living/2016-vaccine-uptake-canadian-adults-survey.html (accessed on 3 February 2020).
- Public Health Agency of Canada. Vaccine uptake in Canadian Adults 2019. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/2018-2019-influenza-flu-vaccine-coverage-survey-results.html (accessed on 16 July 2020).
- Center for Disease Control. Flu Vaccination Coverage, United States, 2018–2019 Influenza Season | FluVaxView | Seasonal Influenza (Flu). Available online: https://www.cdc.gov/flu/fluvaxview/coverage-1819estimates.htm (accessed on 31 July 2020).
- Public Health England. Seasonal Influenza Vaccine Uptake in GP Patients: Winter Season 2018 to 2019. Available online: https://www.gov.uk/government/statistics/seasonal-flu-vaccine-uptake-in-gp-patients-winter-2018-to-2019 (accessed on 31 July 2020).
- Health Protection Scotland. Influenza. Available online: https://www.hps.scot.nhs.uk/a-to-z-of-topics/influenza/ (accessed on 31 July 2020).
- Public Health Wales. Seasonal influenza in Wales 2018/19 Annual Report. Available online: http://www2.nphs.wales.nhs.uk:8080/CommunitySurveillanceDocs.nsf/($All)/E3F7BE45AAB413658025841700552272/$File/Seasonal%20influenza%20in%20Wales%20201819_v1a(final).pdf (accessed on 31 July 2020).
- Public Health Agency. Influenza Weekly Surveillance Bulletin-Northern Ireland, Weeks 19 and 20. Available online: https://www.publichealth.hscni.net/sites/default/files/2019-05/Flu%20Bulletin%20Week%2019-20.pdf (accessed on 31 July 2020).
- Korkmaz, P.; Paşali Kilit, T.; Onbaşi, K.; Mistanoglu Ozatag, D.; Toka, O. Influenza vaccination prevalence among the elderly and individuals with chronic disease, and factors affecting vaccination uptake. Cent. Eur. J. Public Health 2019, 27, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Abbas, K.M.; Kang, G.J.; Chen, D.; Werre, S.R.; Marathe, A. Demographics, perceptions, and socioeconomic factors affecting influenza vaccination among adults in the United States. PeerJ 2018, 6, e5171. [Google Scholar] [CrossRef] [PubMed]
- Mangtani, P.; Breeze, E.; Stirling, S.; Hanciles, S.; Kovats, S.; Fletcher, A. Cross-sectional survey of older peoples’ views related to influenza vaccine uptake. BMC Public Health 2006, 6, 249. [Google Scholar] [CrossRef] [Green Version]
- Nanda, A.; Vura, N.V.R.K.; Gravenstein, S. COVID-19 in older adults. Aging Clin. Exp. Res. 2020, 32, 1199–1202. [Google Scholar] [CrossRef] [PubMed]
- Leung, C. Risk factors for predicting mortality in elderly patients with COVID-19: A review of clinical data in China. Mech. Ageing Dev. 2020, 188, 111255. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, B.; Herndler-Brandstetter, D.; Schwanninger, A.; Weiskopf, D.; Grubeck-Loebenstein, B. Biology of Immune Responses to Vaccines in Elderly Persons. Clin. Infect. Dis. 2008, 46, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- DiazGranados, C.A.; Dunning, A.J.; Kimmel, M.; Kirby, D.; Treanor, J.; Collins, A.; Pollak, R.; Christoff, J.; Earl, J.; Landolfi, V.; et al. Efficacy of High-Dose versus Standard-Dose Influenza Vaccine in Older Adults. N. Engl. J. Med. 2014, 371, 635–645. [Google Scholar] [CrossRef]
- Balasubramani, G.; Choi, W.S.; Nowalk, M.P.; Zimmerman, R.K.; Monto, A.S.; Martin, E.T.; Belongia, E.A.; McLean, H.Q.; Gaglani, M.; Murthy, K.; et al. Relative effectiveness of high dose versus standard dose influenza vaccines in older adult outpatients over four seasons, 2015–2016 to 2018–19. Vaccine 2020, 28, 42. [Google Scholar] [CrossRef]
- Van Aalst, R.; Gravenstein, S.; Mor, V.; Mahmud, S.M.; Wilschut, J.; Postma, M.; Chit, A. Comparative effectiveness of high dose versus adjuvanted influenza vaccine: A retrospective cohort study. Vaccine 2020, 38, 372–379. [Google Scholar] [CrossRef]
- Van Buynder, P.; Konrad, S.; Van Buynder, J.; Brodkin, E.; Krajden, M.; Ramler, G.; Bigham, M. The comparative effectiveness of adjuvanted and unadjuvanted trivalent inactivated influenza vaccine (TIV) in the elderly. Vaccine 2013, 31, 6122–6128. [Google Scholar] [CrossRef] [Green Version]
- Mannino, S.; Villa, M.; Apolone, G.; Weiss, N.S.; Groth, N.; Aquino, I.; Boldori, L.; Caramaschi, F.; Gattinoni, A.; Malchiodi, G.; et al. Effectiveness of Adjuvanted Influenza Vaccination in Elderly Subjects in Northern Italy. Am. J. Epidemiol. 2012, 176, 527–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domnich, A.; Arata, L.; Amicizia, D.; Puig-Barberà, J.; Gasparini, R.; Panatto, D. Effectiveness of MF59-adjuvanted seasonal influenza vaccine in the elderly: A systematic review and meta-analysis. Vaccine 2017, 35, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Bella, A.; Gesualdo, F.; Orsi, A.; Arcuri, C.; Chironna, M.; Loconsole, D.; Napoli, C.; Orsi, G.B.; Manini, I.; Montomoli, E.; et al. Effectiveness of the trivalent MF59 adjuvated influenza vaccine in preventing hospitalization due to influenza B and A(H1N1)pdm09 viruses in the elderly in Italy, 2017–2018 season. Expert Rev. Vaccines 2019, 18, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Lapi, F.; Marconi, E.; Simonetti, M.; Baldo, V.; Rossi, A.; Sessa, A.; Cricelli, C. Adjuvanted versus nonadjuvanted influenza vaccines and risk of hospitalizations for pneumonia and cerebro/cardiovascular events in the elderly. Expert Rev. Vaccines 2019, 18, 663–670. [Google Scholar] [CrossRef]
- Pelton, S.I.; Divino, V.; Shah, D.; Mould-Quevedo, J.; Dekoven, M.; Krishnarajah, G.; Postma, M.J. Evaluating the Relative Vaccine Effectiveness of Adjuvanted Trivalent Influenza Vaccine Compared to High-Dose Trivalent and Other Egg-Based Influenza Vaccines among Older Adults in the US during the 2017–2018 Influenza Season. Vaccines 2020, 8, 446. [Google Scholar] [CrossRef]
- Pebody, R.; Whitaker, H.; Zhao, H.; Andrews, N.; Ellis, J.; Donati, M.; Zambon, M. Protection provided by influenza vaccine against influenza-related hospitalisation in ≥65 year olds: Early experience of introduction of a newly licensed adjuvanted vaccine in England in 2018/19. Vaccine 2020, 38, 173–179. [Google Scholar] [CrossRef]
- Beal, J.L.; Kadakia, N.N.; Reed, J.B.; Illingworth Plake, K.S. Pharmacists’ impact on older adults’ access to vaccines in the United States. Vaccine 2020, 38, 2456–2465. [Google Scholar] [CrossRef]
- Papastergiou, J.; Folkins, C.; Li, W.; Zervas, J. Community pharmacist–administered influenza immunization improves patient access to vaccination. Can. Pharm. J. 2014, 147, 359–365. [Google Scholar] [CrossRef] [Green Version]
- Buchan, S.A.; Rosella, L.C.; Finkelstein, M.; Juurlink, D.; Isenor, J.; Marra, F.; Patel, A.; Russell, M.L.; Quach, S.; Waite, N.; et al. Impact of pharmacist administration of influenza vaccines on uptake in Canada. CMAJ 2016, 189, E146–E152. [Google Scholar] [CrossRef] [Green Version]
- Al Hamarneh, Y.N.; Charrois, T.; Lewanczuk, R.; Tsuyuki, R.T. Pharmacist intervention for glycaemic control in the community (the RxING study). BMJ Open 2013, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Mansell, K.; Edmunds, K.; Guirguis, L. Pharmacists’ Scope of Practice: Supports for Canadians with Diabetes. Can. J. Diabetes 2017, 41, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuki, R.T.; Al Hamarneh, Y.N.; Jones, C.A.; Hemmelgarn, B.R. The Effectiveness of Pharmacist Interventions on Cardiovascular Risk: The Multicenter Randomized Controlled RxEACH Trial. J. Am. Coll. Cardiol. 2016, 67, 2846–2854. [Google Scholar] [CrossRef] [PubMed]
- Schaffner, W.; Chen, W.H.; Hopkins, R.H.; Neuzil, K. Effective Immunization of Older Adults against Seasonal Influenza. Am. J. Med. 2018, 131, 865–873. [Google Scholar] [CrossRef]
- Ang, L.W.; Cutter, J.; James, L.; Goh, K.T. Factors associated with influenza vaccine uptake in older adults living in the community in Singapore. Epidemiol. Infect. 2017, 145, 775–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, D.S.; Kim, K.; Park, S.M. Factors associated with influenza vaccination coverage among the elderly in South Korea: The Fourth Korean National Health and Nutrition Examination Survey (KNHANES IV). BMJ Open 2016, 6, 12. [Google Scholar] [CrossRef] [Green Version]
- Okoli, G.N.; Lam, O.L.T.; Racovitan, F.; Reddy, V.K.; Righolt, C.H.; Neilson, C.; Chit, A.; Thommes, E.; Abou-Setta, A.M.; Mahmud, S.M. Seasonal influenza vaccination in older people: A systematic review and meta-analysis of the determining factors. PLoS ONE 2020, 15. [Google Scholar] [CrossRef]
- Jackson, L.A.; Nelson, J.C.; Benson, P.; Neuzil, K.M.; Reid, R.J.; Psaty, B.M.; Heckbert, S.R.; Larson, E.B.; Weiss, N.S. Functional status is a confounder of the association of influenza vaccine and risk of all cause mortality in seniors. Int. J. Epidemiol. 2006, 35, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Public Health England, Department of Health and Social Care. The National flu Immunisation Programme 2019/20. Available online: https://www.england.nhs.uk/wp-content/uploads/2019/03/annual-national-flu-programme-2019-to-2020-1.pdf (accessed on 20 May 2019).
- Baroy, J.; Chung, D.; Frisch, R.; Apgar, D.; Slack, M.K. The impact of pharmacist immunization programs on adult immunization rates: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 2016, 56, 418–426. [Google Scholar] [CrossRef]
- Thomas, R.E.; Lorenzetti, D.L. Interventions to increase influenza vaccination rates of those 60 years and older in the community. Cochrane Database Syst. Rev. 2018, 2018, CD005188. [Google Scholar] [CrossRef]
- Pullagura, G.R.; Waite, N.M.; Houle, S.K.D.; Violette, R.; Wong, W.W.L. Cost-utility analysis of offering a novel remunerated community pharmacist consultation service on influenza vaccination for seniors in Ontario, Canada. J. Am. Pharm. Assoc. 2019, 59, 489–497. [Google Scholar] [CrossRef]
- Isenor, J.E.; Wagg, A.C.; Bowles, S.K. Patient experiences with influenza immunizations administered by pharmacists. Hum. Vaccin Immunother. 2018, 14, 706–711. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reason | Number of Older Adults (% of Patients Providing Reason) |
|---|---|
| “Flu shot causes the flu” | 25 (36%) |
| “Flu shot doesn’t work” | 24 (35%) |
| “Flu shot is too painful” | 10 (14%) |
| “I would rather wait until the flu comes into the community” | 6 (9%) |
| “I had the flu shot last year; I don’t need it again” | 4 (6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strain, W.D.; Mansi, J.; Boikos, C.; Boivin, M.; Fisher, W.A. Achieving Influenza Vaccine Uptake Target in Canada via a Pharmacy-Led Telephone Discussion during the 2019–2020 Season. Vaccines 2021, 9, 312. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040312
Strain WD, Mansi J, Boikos C, Boivin M, Fisher WA. Achieving Influenza Vaccine Uptake Target in Canada via a Pharmacy-Led Telephone Discussion during the 2019–2020 Season. Vaccines. 2021; 9(4):312. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040312
Chicago/Turabian StyleStrain, William David, James Mansi, Constantina Boikos, Michael Boivin, and William A. Fisher. 2021. "Achieving Influenza Vaccine Uptake Target in Canada via a Pharmacy-Led Telephone Discussion during the 2019–2020 Season" Vaccines 9, no. 4: 312. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040312