
Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach

 ,
,  ,
,  ,
,  ,
,  , ,
, ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Variables
2.3. Ethical Considerations
2.4. Data Mining
2.4.1. Data Analysis
2.4.2. Decision Tree Analysis
2.4.3. Multi-Level Regression
3. Results
3.1. Descriptive Statistics
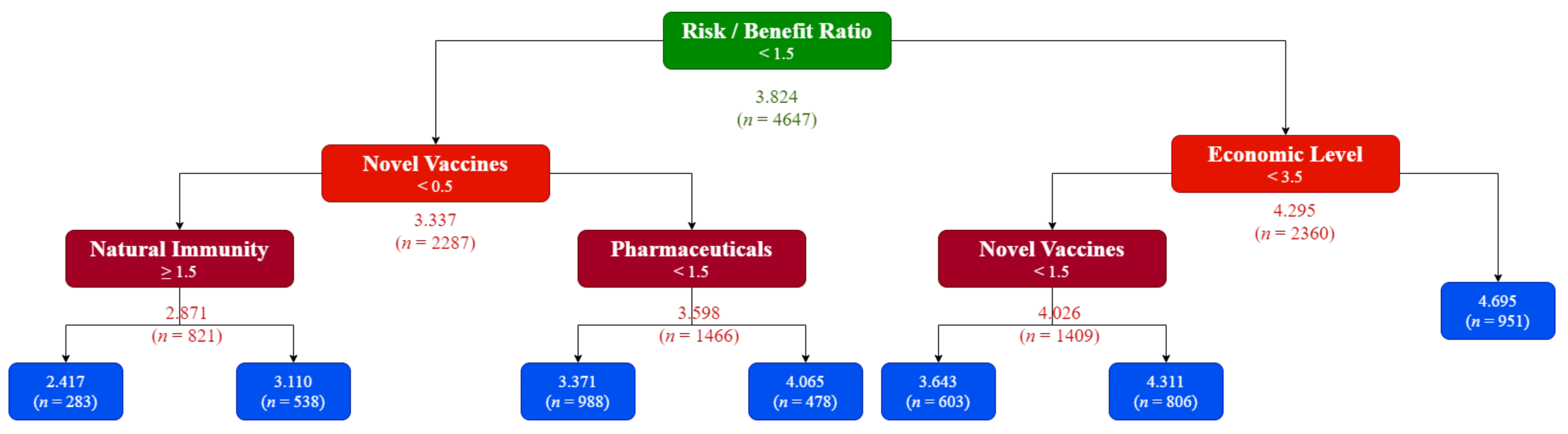
3.2. Decision Tree Analysis
3.3. Bivariate Correlation
3.4. Multi-Level Regression
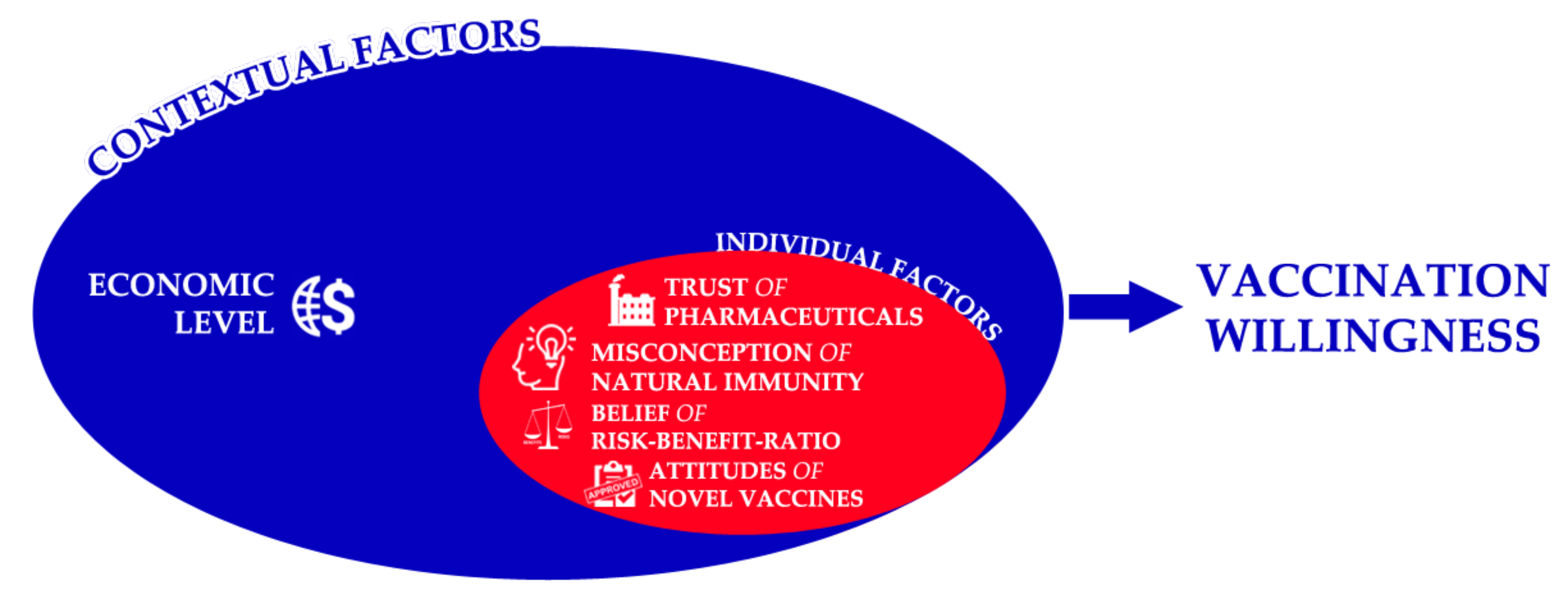
3.5. Socio-Ecological Model
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Members of IADS-SCORE Consortium
- Faculty of Dentistry, McGill University, Canada (Jacques Jaar); Schulich School of Medicine & Dentistry, Western University, Canada (Nima Lighvan); Faculty of Dentistry, University of British Columbia, Canada (Karen Lin);
- Faculty of Dentistry, SEGi University, Malaysia (Sandy Tan Qing Wen); Faculty of Dentistry, University of Malaya, Malaysia (Tan Hian Wei);
- School of Dentistry, Kathmandu University School of Medical Sciences, Nepal (Nitesh Singh);
- Department of Oral and Maxillofacial Surgery, School of Dentistry, Zanjan University of Medical Sciences, Iran (Parsa Firoozi); Department of Oral and Maxillofacial Surgery, School of Dentistry, Islamic Azad University Isfahan, Iran (Mohammad Mostafa Aghamohseni; Samin Sirous);
- Institute of Dentistry, CMH Lahore Medical College and Institute of Dentistry, Pakistan (Aneeqa Aslam; Maha Sohail); Dental College, Akhtar Saeed Medical and Dental College, Pakistan (Mehroz Ahmad Khan);
- Faculty of Dentistry, Beirut Arab University, Lebanon (Julien Issa; Mirna Abou Ibrahim);
- Faculty of Dental Medicine, Catholic University of Portugal, Portugal (António Coimbra Amaral);
- Faculty of Dental Sciences, Aldent University, Albania (Ersid Domnori);
- Faculty of Odontology, Universidad San Francisco De Quito, Ecuador (Jorge Ayala); Faculty of Odontology, Catholic University of Cuenca, Ecuador (Maria Sol Medina);
- Faculty of Dentistry, Universitas Indonesia, Indonesia (Viandra Tjokroadiredjo; Farih Aminah)
- Department of Dentistry, Al-rafidain University College, Iraq (Noor Sarmad); College of Dentistry, Uruk University, Iraq (Nabaa Abduladheem); Department of Dentistry, Al-rasheed University College, Iraq (Batool Mohammed);
- Department of Neuroscience, Reproductive Sciences and Dentistry, University of Naples Federico II, Italy (Matteo Cafasso); Department of Biomedical, Surgical and Dental Sciences, School of Dentistry, University of Milan, Italy (Gregorio Tortora); Department of Medicine and Surgery, School of Dentistry, University of Insubria, Italy (Anita Homayuni);
- Faculty of Dentistry, Riga Stradiņš University, Latvia (Kristīne Romanovska);
- Faculty of Odontology, Medical Academy, Lithuanian University of Health Sciences, Lithuania (Kriste Trijonytė; Julius Mikonis);
- Faculty of Dentistry, University of Khartoum, Sudan (Ahmed Abdalla); Faculty of Dentistry, Al Neelain University, Sudan (Zeinab Hassan); Faculty of Dentistry, University of Medical Sciences and Technology, Sudan (Aya Abdelrahim);
- Faculty of Dental Medicine, Monastir University, Tunisia (Haythem Ben Hadj Belgacem; Maya Fedhila);
- Faculty of Dentistry, Istanbul University, Turkey (İrem Erdoğdu); Faculty of Dentistry, Beykent University, Turkey (Berk Koparan); Faculty of Dentistry, Yeditepe University, Turkey (Ezgi Y eşiltan); Faculty of Dentistry, Marmara University, Turkey (Serap Beşiroğlu);
- Faculty of Dentistry, Ural State Medical University, Russia (Tatiana Spitsyna);
- Faculty of Dental Medicine, University of Rijeka, Croatia (Valentina Marasović; Elizabeta Vrkljan; Lovre Labura);
- Institute of Dentistry, Faculty of Medicine, University of Tartu, Estonia (Estelle Saavaste);
- College of Dentistry, University of Florida, United States of America (Natalie Atyeo); School of Dentistry, University of Michigan, United States of America (Alexandra Herzog);
- Oral Health Research and Promotion Unit, Faculty of Dentistry, Al-Quds University, Palestine (Mayar Danadneh)
References
- D’souza, G.; Dowdy, D. What is Herd Immunity and How Can We Achieve It with COVID-19? Available online: https://www.jhsph.edu/covid-19/articles/achieving-herd-immunity-with-covid19.html (accessed on 17 August 2021).
- Liao, J.; Fan, S.; Chen, J.; Wu, J.; Xu, S.; Guo, Y.; Li, C.; Zhang, X.; Wu, C.; Mou, H.; et al. Epidemiological and Clinical Characteristics of COVID-19 in Adolescents and Young Adults. Innov. 2020, 1, 100001. [Google Scholar] [CrossRef]
- Barber, S.J.; Kim, H. COVID-19 Worries and Behavior Changes in Older and Younger Men and Women. J. Gerontol. 2021, 76, e17–e23. [Google Scholar] [CrossRef] [PubMed]
- Ceccato, I.; Palumbo, R.; Di Crosta, A.; La Malva, P.; Marchetti, D.; Maiella, R.; Verrocchio, M.C.; Marin, A.; Mammarella, N.; Palumbo, R.; et al. Age-related differences in the perception of COVID-19 emergency during the Italian outbreak. Aging Ment. Health 2020, 25, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Barari, S.; Caria, S.; Davola, A.; Falco, P.; Fetzer, T.; Fiorin, S.; Hensel, L.; Ivchenko, A.; Jachimowicz, J.; King, G.; et al. Evaluating COVID-19 Public Health Messaging in Italy: Self-Reported Compliance and Growing Mental Health Concerns. medRxiv 2020. [Google Scholar] [CrossRef]
- Guastafierro, E.; Toppo, C.; Magnani, F.G.; Romano, R.; Facchini, C.; Campioni, R.; Brambilla, E.; Leonardi, M. Older Adults’ Risk Perception during the COVID-19 Pandemic in Lombardy Region of Italy: A Cross-sectional Survey. J. Gerontol. Soc. Work 2021, 64, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- PAHO. Introducing COVID-19 Vaccination: Guidance for Determining Priority Groups and Microplanning; Pan American Health Organization (PAHO): Washington, DC, USA, 2021. [Google Scholar]
- Russo, A.G.; Decarli, A.; Valsecchi, M.G. Strategy to identify priority groups for COVID-19 vaccination: A population based cohort study. Vaccine 2021, 39, 2517–2525. [Google Scholar] [CrossRef]
- Benis, A.; Seidmann, A.; Ashkenazi, S. Reasons for Taking the COVID-19 Vaccine by US Social Media Users. Vaccines 2021, 9, 315. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. Global Prevalence and Drivers of Dental Students’ COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Kateeb, E.; Danadneh, M.; Pokorná, A.; Klugarová, J.; Abdulqader, H.; Klugar, M.; Riad, A. Predictors of Willingness to Receive COVID-19 Vaccine: Cross-Sectional Study of Palestinian Dental Students. Vaccines 2021, 9, 954. [Google Scholar] [CrossRef]
- Almaghaslah, D.; Alsayari, A.; Kandasamy, G.; Vasudevan, R. COVID-19 Vaccine Hesitancy among Young Adults in Saudi Arabia: A Cross-Sectional Web-Based Study. Vaccines 2021, 9, 330. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Antalová, N.; Krobot, M.; Zviadadze, N.; Serdiuk, I.; Koščík, M.; Klugar, M. Prevalence and Drivers of COVID-19 Vaccine Hesitancy among Czech University Students: National Cross-Sectional Study. Vaccines 2021, 9, 948. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, A.; Kaiser, J.; Vaccari, C.; Freeman, D.; Lambe, S.; Loe, B.S.; Vanderslott, S.; Lewandowsky, S.; Conroy, M.; Ross, A.R.N.; et al. Online Social Endorsement and Covid-19 Vaccine Hesitancy in the United Kingdom. Soc. Media Soc. 2021, 7. [Google Scholar] [CrossRef]
- Juvinyà-Canal, D.; Suñer-Soler, R.; Porquet, A.B.; Vernay, M.; Blanchard, H.; Bertran-Noguer, C. Health Literacy among Health and Social Care University Students. Int. J. Environ. Res. Public Health 2020, 17, 2273. [Google Scholar] [CrossRef] [Green Version]
- Vozikis, A.; Drivas, K.; Milioris, K. Health literacy among university students in Greece: Determinants and association with self-perceived health, health behaviours and health risks. Arch. Public Heal. 2014, 72, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sukys, S.; Cesnaitiene, V.J.; Ossowsky, Z.M. Is health education at university associated with students’ health literacy? evidence from cross-sectional study applying HLS-EU-Q. Biomed Res. Int. 2017, 2017. [Google Scholar] [CrossRef]
- Belingheri, M.; Facchetti, R.; Scordo, F.; Butturini, F.; Turato, M.; De Vito, G.; Cesana, G.; Riva, M.A. Risk behaviors among Italian healthcare students: A cross-sectional study for health promotion of future healthcare workers. Med. Lav. 2019, 110, 155. [Google Scholar] [CrossRef]
- Alba, L.H.; Badoui, N.; Gil, F. Attitude toward preventive counseling and healthy practices among medical students at a Colombian university. Front. Med. 2015, 9, 251–259. [Google Scholar] [CrossRef]
- Frank, E.; Carrera, J.S.; Elon, L.; Hertzberg, V.S. Predictors of US medical students’ prevention counseling practices. Prev. Med. 2007, 44, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Lobelo, F.; Duperly, J.; Frank, E. Physical activity habits of doctors and medical students influence their counselling practices. Br. J. Sports Med. 2009, 43, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Alawia, R.; Riad, A.; Kateeb, E. Risk perception and readiness of dental students to treat patients amid COVID-19: Implication for dental education. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Alawia, R.; Riad, A.; Kateeb, E. Knowledge and attitudes among dental students about COVID-19 and its precautionary measures: A cross-sectional study. J. Oral Med. Oral Surg. 2021, 27, 17. [Google Scholar] [CrossRef]
- Wu, D.T.; Wu, K.Y.; Nguyen, T.T.; Tran, S.D. The impact of COVID-19 on dental education in North America—Where do we go next? Eur. J. Dent. Educ. 2020, 24, 825–827. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.; Aziz, K.; Ojcius, D.M. Impact of COVID-19 on dental education in the United States. J. Dent. Educ. 2020, 84, 718–722. [Google Scholar] [CrossRef] [PubMed]
- Machado, R.A.; Bonan, P.R.F.; Da Cruz Perez, D.E.; Martelli Júnior, H. COVID-19 pandemic and the impact on dental education: Discussing current and future perspectives. Braz. Oral Res. 2020, 34, e083. [Google Scholar] [CrossRef]
- dos Santos, J.A.; Normando, A.G.C.; da Silva, R.L.C.; Acevedo, A.C.; Canto, G.D.L.; Sugaya, N.; Santos-Silva, A.R.; Guerra, E.N.S. Oral Manifestations in Patients with COVID-19: A 6-Month Update. J. Dent. Res. 2021. [Google Scholar] [CrossRef]
- Riad, A.; Kassem, I.; Badrah, M.; Klugar, M. Acute Parotitis as a Presentation of COVID-19? Oral Dis. 2020, odi.13571. [Google Scholar] [CrossRef]
- Riad, A.; Kassem, I.; Hockova, B.; Badrah, M.; Klugar, M. Halitosis in COVID-19 patients. Spec. Care Dent. 2021, 41, 282–285. [Google Scholar] [CrossRef]
- Riad, A.; Kassem, I.; Stanek, J.; Badrah, M.; Klugarova, J.; Klugar, M. Aphthous Stomatitis in COVID-19 Patients: Case-series and Literature Review. Dermatol. Ther. 2021, 34. [Google Scholar] [CrossRef] [PubMed]
- Hocková, B.; Riad, A.; Valky, J.; Šulajová, Z.; Stebel, A.; Slávik, R.; Bečková, Z.; Pokorná, A.; Klugarová, J.; Klugar, M. Oral Complications of ICU Patients with COVID-19: Case-Series and Review of Two Hundred Ten Cases. J. Clin. Med. 2021, 10, 581. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Gomaa, E.; Hockova, B.; Klugar, M. Oral Candidiasis of COVID-19 Patients: Case Report and Review of Evidence. J. Cosmet. Dermatol. 2021, 20, 1580–1584. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Kassem, I.; Hockova, B.; Badrah, M.; Klugar, M. Tongue ulcers associated with SARS--CoV-2 infection: A case series. Oral Dis. 2020, odi.13635. [Google Scholar] [CrossRef]
- Riad, A.; Boccuzzi, M.; Sagiroglu, D.; Klugar, M.; Krsek, M. Pediatric multisystem inflammatory syndrome temporally associated with SARS-COV-2: Oral manifestations and implications. Int. J. Paediatr. Dent. 2020, 31, ipd.12694. [Google Scholar] [CrossRef]
- Umeizudike, K.A.; Isiekwe, I.G.; Fadeju, A.D.; Akinboboye, B.O.; Aladenika, E.T. Nigerian undergraduate dental students’ knowledge, perception, and attitude to COVID-19 and infection control practices. J. Dent. Educ. 2021, 85, 187–196. [Google Scholar] [CrossRef]
- Davide, S.; Macarelli, C.; Lam, A. Vaccination Recommendations for Oral Health Professionals. Available online: https://decisionsindentistry.com/article/vaccination-recommendations-for-oral-health-professionals/ (accessed on 15 April 2021).
- Souza, R.A.; Namen, F.M.; Galan, J., Jr.; Vieira, C.; Sedano, H.O. Infection Control Measures Among Senior Dental Students in Rio de Janeiro State, Brazil. J. Public Health Dent. 2006, 66, 282–284. [Google Scholar] [CrossRef]
- Singh, A.; Purohit, B.M.; Bhambal, A.; Saxena, S.; Singh, A.; Gupta, A. Knowledge, Attitudes, and Practice Regarding Infection Control Measures among Dental Students in Central India. J. Dent. Educ. 2011, 75, 421–427. [Google Scholar] [CrossRef]
- Shetty, S.; Prabhu, S.; Shetty, V.; Shetty, A.K. Knowledge, attitudes and factors associated with acceptability of human papillomavirus vaccination among undergraduate medical, dental and nursing students in South India. Hum. Vaccin. Immunother. 2019, 15, 1656–1665. [Google Scholar] [CrossRef]
- Rutkoski, H.; Tay, D.L.; Dixon, B.L.; Pinzon, L.M.; Mooney, R.; Winkler, J.R.; Kepka, D. A Multi-state Evaluation of Oral Health Students’ Knowledge of Human Papillomavirus-Related Oropharyngeal Cancer and HPV Vaccination. J. Cancer Educ. 2020, 35, 1017–1025. [Google Scholar] [CrossRef]
- Farsi, N.J.; Al Sharif, S.; Al Qathmi, M.; Merdad, M.; Marzouki, H.; Merdad, L. Knowledge of Human Papillomavirus (HPV) and Oropharyngeal Cancer and Acceptability of the HPV Vaccine among Dental Students. Asian Pac. J. Cancer Prev. 2020, 21, 3595–3603. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and Behaviors towards SARS-CoV-2 Vaccination among Healthcare Workers: A Cross-Sectional Study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef] [PubMed]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020, 1–5. [Google Scholar] [CrossRef]
- Sovicova, M.; Zibolenova, J.; Svihrova, V.; Hudeckova, H. Odds Ratio Estimation of Medical Students’ Attitudes towards COVID-19 Vaccination. Int. J. Environ. Res. Public Health 2021, 18, 6815. [Google Scholar] [CrossRef]
- Olaimat, A.N.; Aolymat, I.; Shahbaz, H.M.; Holley, R.A. Knowledge and Information Sources About COVID-19 among University Students in Jordan: A Cross-Sectional Study. Front. Public Health 2020, 8, 254. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in the diagnosis of COVID-19: Challenges and perspectives. Int. J. Biol. Sci. 2021, 17, 1581. [Google Scholar] [CrossRef]
- Gunasekeran, D.V.; Tseng, R.M.W.W.; Tham, Y.-C.; Wong, T.Y. Applications of digital health for public health responses to COVID-19: A systematic scoping review of artificial intelligence, telehealth and related technologies. NPJ Digit. Med. 2021, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- van der Schaar, M.; Alaa, A.M.; Floto, A.; Gimson, A.; Scholtes, S.; Wood, A.; McKinney, E.; Jarrett, D.; Lio, P.; Ercole, A. How artificial intelligence and machine learning can help healthcare systems respond to COVID-19. Mach. Learn. 2020, 110, 1–14. [Google Scholar] [CrossRef]
- Mendels, D.-A.; Dortet, L.; Emeraud, C.; Oueslati, S.; Girlich, D.; Ronat, J.-B.; Bernabeu, S.; Bahi, S.; Atkinson, G.J.H.; Naas, T. Using artificial intelligence to improve COVID-19 rapid diagnostic test result interpretation. Proc. Natl. Acad. Sci. USA 2021, 118, 2021. [Google Scholar] [CrossRef]
- Hussain, A.; Tahir, A.; Hussain, Z.; Sheikh, Z.; Gogate, M.; Dashtipour, K.; Ali, A.; Sheikh, A. Artificial Intelligence–Enabled Analysis of Public Attitudes on Facebook and Twitter Toward COVID-19 Vaccines in the United Kingdom and the United States: Observational Study. J. Med. Internet Res. 2021, 23, e26627. [Google Scholar] [CrossRef]
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J.; Marani, H.; Monkman, H. COVID-19 vaccine hesitancy in Canada: A content analysis of Tweets using the Theoretical Domains Framework. J. Med. Internet Res. 2020, 23, e26874. [Google Scholar] [CrossRef] [PubMed]
- International Association of Dental Students (IADS) Workforce. Available online: https://iads-web.org/governance/workforce/ (accessed on 14 March 2021).
- International Association of Dental Students (IADS) Delegates List. Available online: https://iads-web.org/governance/delegates/ (accessed on 14 March 2021).
- KoBoToolbox.org KoBoToolbox. Available online: https://support.kobotoolbox.org/welcome.html (accessed on 15 August 2020).
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R.; Eskola, J.; et al. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strategic Advisory Group of Experts on Immunization (SAGE). Report of the Sage Working Group on Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Dudley, M.Z.; Privor-Dumm, L.; Dubé, È.; MacDonald, N.E. Words matter: Vaccine hesitancy, vaccine demand, vaccine confidence, herd immunity and mandatory vaccination. Vaccine 2020, 38, 709–711. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA−J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. UroToday Int. J. 2009, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proton Technologies AG General Data Protection Regulation (GDPR) Compliance Guidelines. Available online: https://gdpr.eu/ (accessed on 1 May 2020).
- Boerner, F.; Keelan, J.; Winton, L.; Jardine, C.; Driedger, S.M. Understanding the interplay of factors informing vaccination behavior in three Canadian provinces. Hum. Vaccines Immunother. 2013, 9, 1477–1484. [Google Scholar] [CrossRef] [Green Version]
- jamovi (Version 1.6) The jamovi Project. Available online: https://www.jamovi.org/ (accessed on 2 August 2021).
- World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 14 March 2021).
- Al-Jayyousi, G.F.; Sherbash, M.A.M.; Ali, L.A.M.; El-Heneidy, A.; Alhussaini, N.W.Z.; Elhassan, M.E.A.; Nazzal, M.A. Factors Influencing Public Attitudes towards COVID-19 Vaccination: A Scoping Review Informed by the Socio-Ecological Model. Vaccines 2021, 9, 548. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, V.; Lagravinese, R.; Resce, G. Predicting vaccine hesitancy from area-level indicators: A machine learning approach. medRxiv 2021. [Google Scholar] [CrossRef]
- Kollamparambil, U.; Oyenubi, A.; Nwosu, C. COVID19 Vaccine Intentions in South Africa: Health Communication Strategy to Address Vaccine Hesitancy. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.J.; Strych, U.; Dor, A.; Franklin Fowler, E.; Motta, M. Correlates and Disparities of COVID-19 Vaccine Hesitancy. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef]
- Sandhofer, M.J.; Robak, O.; Frank, H.; Kulnig, J.; Sandhofer, M.J.; Frank, H.; Robak, O.; Kulnig, J. Vaccine hesitancy in Austria A cross-sectional survey. Wien. Klin. Wochenschr. 2017, 129, 59–64. [Google Scholar] [CrossRef]
- Raude, J.; Fressard, L.; Gautier, A.; Pulcini, C.; Peretti-Watel, P.; Verger, P. Opening the ‘Vaccine Hesitancy’ black box: How trust in institutions affects French GPs’ vaccination practices. Expert Rev. Vaccines 2016, 15, 937–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalok, A.; Loh, S.Y.E.; Chew, K.T.; Abdul Aziz, N.H.; Shah, S.A.; Ahmad, S.; Mohamed Ismail, N.A.; Abdullah Mahdy, Z. Vaccine hesitancy towards childhood immunisation amongst urban pregnant mothers in Malaysia. Vaccine 2020, 38, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental vaccine hesitancy in Italy—Results from a national survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Rungkitwattanakul, D.; Yabusaki, A.; Singh, D.; Lawson, P.; Nwaogwugwu, U.; Iheagwara, O.S.; Mere, C. COVID-19 vaccine hesitancy among African American hemodialysis patients: A single-center experience. Hemodial. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 1–8. [Google Scholar] [CrossRef]
- Díaz Crescitelli, M.E.; Ghirotto, L.; Sisson, H.; Sarli, L.; Artioli, G.; Bassi, M.C.; Appicciutoli, G.; Hayter, M. A Meta-Synthesis Study of the Key Elements Involved in Childhood Vaccine Hesitancy. Public Health 2020, 180, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Siddique, A.B.; Akter, R.; Tasnim, R.; Sujan, M.S.H.; Ward, P.R.; Sikder, M.T. Knowledge, attitudes and perceptions towards COVID-19 vaccinations: A cross-sectional community survey in Bangladesh. medRxiv 2021. [Google Scholar] [CrossRef]
- Dinga, J.N.; Sinda, L.K.; Titanji, V.P.K. Assessment of vaccine hesitancy to a covid-19 vaccine in cameroonian adults and its global implication. Vaccines 2021, 9, 175. [Google Scholar] [CrossRef] [PubMed]
- Acheampong, T.; Akorsikumah, E.A.; Osae-Kwapong, J.; Khalid, M.; Appiah, A.; Amuasi, J.H. Examining Vaccine Hesitancy in Sub-Saharan Africa: A Survey of the Knowledge and Attitudes among Adults to Receive COVID-19 Vaccines in Ghana. Vaccines 2021, 9, 814. [Google Scholar] [CrossRef] [PubMed]
- Afolabi, A.A.; Ilesanmi, O.S. Dealing with vaccine hesitancy in Africa: The prospective COVID-19 vaccine context. Pan Afr. Med. J. 2021, 38, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Maraqa, B.; Nazzal, Z.; Rabi, R.; Sarhan, N.; Al-Shakhrah, K.; Al-Kaila, M. COVID-19 vaccine hesitancy among health care workers in Palestine: A call for action. Prev. Med. 2021, 149, 106618. [Google Scholar] [CrossRef] [PubMed]
- Rey, D.; Fressard, L.; Cortaredona, S.; Bocquier, A.; Gautier, A.; Peretti-Watel, P.; Verger, P.; On Behalf of the Baromètre Santé 2016 Group. Vaccine hesitancy in the French population in 2016, and its association with vaccine uptake and perceived vaccine risk–benefit balance. Eurosurveillance 2018, 23, 17-00816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef] [PubMed]
- Miko, D.; Costache, C.; Colosi, H.A.; Neculicioiu, V.; Colosi, I.A. Qualitative Assessment of Vaccine Hesitancy in Romania. Medicina 2019, 55, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Mekhemar, M.; Conrad, J.; Klugarová, J.; Koščík, M.; Klugar, M.; Attia, S. Safety of ChAdOx1 nCoV-19 Vaccine: Independent Evidence from Two EU States. Vaccines 2021, 9, 673. [Google Scholar] [CrossRef] [PubMed]
- Alhazmi, A.; Alamer, E.; Daws, D.; Hakami, M.; Darraj, M.; Abdelwahab, S.; Maghfuri, A.; Algaissi, A. Evaluation of Side Effects Associated with COVID-19 Vaccines in Saudi Arabia. Vaccines 2021, 9, 674. [Google Scholar] [CrossRef] [PubMed]
- Klugar, M.; Riad, A.; Mekhemar, M.; Conrad, J.; Buchbender, M.; Howaldt, H.-P.; Attia, S. Side Effects of mRNA-Based and Viral Vector-Based COVID-19 Vaccines among German Healthcare Workers. Biology 2021, 10, 752. [Google Scholar] [CrossRef]
- Riad, A.; Schünemann, H.; Attia, S.; Peričić, T.P.; Žuljević, M.F.; Jürisson, M.; Kalda, R.; Lang, K.; Morankar, S.; Yesuf, E.A.; et al. COVID-19 Vaccines Safety Tracking (CoVaST): Protocol of a Multi-Center Prospective Cohort Study for Active Surveillance of COVID-19 Vaccines’ Side Effects. Int. J. Environ. Res. Public Health 2021, 18, 7859. [Google Scholar] [CrossRef] [PubMed]
- Jęśkowiak, I.; Wiatrak, B.; Grosman-Dziewiszek, P.; Szeląg, A. The Incidence and Severity of Post-Vaccination Reactions after Vaccination against COVID-19. Vaccines 2021, 9, 502. [Google Scholar] [CrossRef]
- Riad, A.; Sağıroğlu, D.; Üstün, B.; Pokorná, A.; Klugarová, J.; Attia, S.; Klugar, M. Prevalence and Risk Factors of CoronaVac Side Effects: An Independent Cross-Sectional Study among Healthcare Workers in Turkey. J. Clin. Med. 2021, 10, 2629. [Google Scholar] [CrossRef]
- Riad, A.; Hocková, B.; Kantorová, L.; Slávik, R.; Spurná, L.; Stebel, A.; Havriľak, M.; Klugar, M. Side Effects of mRNA-Based COVID-19 Vaccine: Nationwide Phase IV Study among Healthcare Workers in Slovakia. Pharmaceuticals 2021, 14, 873. [Google Scholar] [CrossRef]
- Eskola, J.; Duclos, P.; Schuster, M.; MacDonald, N.E.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; et al. How to deal with vaccine hesitancy? Vaccine 2015, 33, 4215–4217. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Item | Outcome |
|---|---|
| Contextual Drivers | |
| Do reports you hear/read in the media/on social media make you reconsider the choice to take the COVID-19 vaccine? | No |
| Not Sure | |
| Yes | |
| Do celebrities, religious or political leaders influence your decision about being vaccinated? | No |
| Not Sure | |
| Yes | |
| Do you trust that your government is making decisions in your best interest with respect to what vaccines are provided (e.g., your government purchases the highest quality vaccines available)? | No |
| Not Sure | |
| Yes | |
| Do you trust pharmaceutical companies to provide credible data on COVID-19 vaccine safety and the effectiveness of the vaccines? | No |
| Not Sure | |
| Yes | |
| Do you know anyone who will not take the vaccine because of religious or cultural values? | No |
| Not Sure | |
| Yes | |
| If “Yes”, do you agree with these people? | No |
| Not Sure | |
| Yes | |
| Individual/Group Drivers | |
| Do you think that there are better ways to prevent COVID-19 than using vaccines (e.g., developing immunity by becoming sick and recovering)? | No |
| Not Sure | |
| Yes | |
| Do you feel you have enough information about COVID-19 vaccines and their safety? | No |
| Not Sure | |
| Yes | |
| Vaccine-Specific Drivers | |
| Do you think that the benefits of COVID-19 vaccines outweigh their reported side effects/adverse reactions? | No |
| Not Sure | |
| Yes | |
| In general, when a new vaccine is introduced, are you inclined to consent to your vaccination? | No |
| Not Sure | |
| Yes | |
| Do you feel confident that the health center or doctor’s office will have the COVID-19 vaccines you need, when you need them? | No |
| Not Sure | |
| Yes |
| Variable | Outcome | Cd | Variable | Outcome | Cd | Variable | Outcome | Cd |
|---|---|---|---|---|---|---|---|---|
| Gender | Female | 1 | Knowing Fatality | No | 0 | Pharmaceuticals | Yes | 2 |
| Male | 2 | Yes | 1 | Cultural Values | No | 0 | ||
| Academic Level | 1st Year | 1 | Flu Vaccine | Never | 0 | Not Sure | 1 | |
| 2nd Year | 2 | Sometimes | 1 | Yes | 2 | |||
| 3rd Year | 3 | Always | 2 | Agreement with Values | No | 0 | ||
| 4th Year | 4 | Mandatory | 3 | Not Sure | 1 | |||
| 5th Year | 5 | Willingness of Vaccination | Totally Disagree | 1 | Yes | 2 | ||
| 6th Year | 6 | Disagree | 2 | Natural Immunity | No | 0 | ||
| Internship | 7 | Not Sure | 3 | Not Sure | 1 | |||
| Fresh Graduate | 8 | Agree | 4 | Yes | 2 | |||
| Clinical Training | Pre-clinical | 1 | Totally Agree | 5 | Perceived Knowledge | No | 0 | |
| Clinical | 2 | Media/Social Media | No | 0 | Not Sure | 1 | ||
| Economic Level | Low income | 1 | Not Sure | 1 | Yes | 2 | ||
| Lower-middle income | 2 | Yes | 2 | Risk/Benefit Ratio | No | 0 | ||
| Upper-middle income | 3 | Public Figures | No | 0 | Not Sure | 1 | ||
| High income | 4 | Not Sure | 1 | Yes | 2 | |||
| Prior Infection | No | 0 | Yes | 2 | Novel Vaccines | No | 0 | |
| Yes | 1 | Government | No | 0 | Not Sure | 1 | ||
| Providing Care | No | 0 | Not Sure | 1 | Yes | 2 | ||
| Yes | 1 | Yes | 2 | Local Availability | No | 0 | ||
| Knowing Patient | No | 0 | Pharmaceuticals | No | 0 | Not Sure | 1 | |
| Yes | 1 | Not Sure | 1 | Yes | 2 |
| Variable | Outcome | Frequency (n) | Percentage (%) | Cumulative Percentage (%) |
|---|---|---|---|---|
| Demographic Characterstics | ||||
| Gender | Female | 4682 | 70.5% | 70.5% |
| Male | 1836 | 27.7% | 98.2% | |
| Non-binary | 53 | 0.8% | 99% | |
| Prefer not to say | 68 | 1% | 100% | |
| Academic Level | First Year | 979 | 14.7% | 14.7% |
| Second Year | 1227 | 18.5% | 33.2% | |
| Third Year | 1422 | 21.4% | 54.6% | |
| Fourth Year | 1259 | 19% | 73.6% | |
| Fifth Year | 817 | 12.3% | 85.9% | |
| Sixth Year | 240 | 3.6% | 89.5% | |
| Internship/Fresh Graduate | 695 | 10.5% | 100% | |
| Clinical Training | Pre-clinical Stage | 2206 | 33.2% | 33.2% |
| Clinical Stage | 4433 | 66.8% | 100% | |
| Economic Level | Low-income Country | 467 | 7% | 7% |
| Lowe-middle-income Country | 1232 | 18.6% | 25.6% | |
| Upper-middle-income Country | 3035 | 45.7% | 71.3% | |
| High-income Country | 1905 | 28.7% | 100% | |
| COVID-19-Related Experience | ||||
| Prior Infection | Yes | 1105 | 16.6% | 16.6% |
| No | 5534 | 83.4% | 100% | |
| Providing Care | Yes | 1808 | 27.2% | 27.2% |
| No | 4831 | 72.8% | 100% | |
| Knowing Patient | Yes | 5801 | 87.4% | 87.4% |
| No | 838 | 12.6% | 100% | |
| Knowing Dead | Yes | 3031 | 45.7% | 45.7% |
| No | 3608 | 54.3% | 100% | |
| Attitudes Towards COVID-19 Vaccine | ||||
| I am willing to take the COVID-19 vaccine once it becomes available to me. | Totally Disagree | 491 | 7.4% | 7.4% |
| Disagree | 434 | 6.5% | 13.9% | |
| Not Sure | 1494 | 22.5% | 36.4% | |
| Agree | 1495 | 22.5% | 59% | |
| Totally Agree | 2725 | 41% | 100% | |
| Contextual Drivers | ||||
| Do reports you hear/read in the media/on social media make you re-consider the choice to take the COVID-19 vaccine? | No | 2903 | 43.7% | 43.7% |
| Not Sure | 1519 | 22.9% | 66.6% | |
| Yes | 2217 | 33.4% | 100% | |
| Do celebrities, religious or political leaders influence your decision about being vaccinated? | No | 4734 | 71.3% | 71.3% |
| Not Sure | 827 | 12.5% | 83.8% | |
| Yes | 1078 | 16.2% | 100% | |
| Do you trust that your government is making decisions in your best interest with respect to what vaccines are provided? | No | 2178 | 32.8% | 32.8% |
| Not Sure | 2130 | 32.1% | 64.9% | |
| Yes | 2331 | 35.1% | 100% | |
| Do you trust pharmaceutical companies to provide credible data on COVID-19 vaccine safety and the effectiveness of the vaccines? | No | 1448 | 21.8% | 21.8% |
| Not Sure | 2041 | 30.7% | 52.6% | |
| Yes | 3150 | 47.4% | 100% | |
| Do you know anyone who will not take the vaccine because of religious or cultural values? | No | 4286 | 64.6% | 64.6% |
| Not Sure | 830 | 12.5% | 77.1% | |
| Yes | 1523 | 22.9% | 100% | |
| If “Yes”, do you agree with these people? | No | 6260 | 94.3% | 94.3% |
| Not Sure | 192 | 2.9% | 97.2% | |
| Yes | 187 | 2.8% | 100% | |
| Individual/Group Drivers | ||||
| Do you think that there are better ways to prevent COVID-19 than using vaccines? | No | 2928 | 44.1% | 44.1% |
| Not Sure | 1955 | 29.4% | 73.6% | |
| Yes | 1756 | 26.4% | 100% | |
| Do you feel you have enough information about COVID-19 vaccines and their safety? | No | 2710 | 40.8% | 40.8% |
| Not Sure | 1838 | 27.7% | 68.5% | |
| Yes | 2091 | 31.5% | 100% | |
| Vaccine-Specific Drivers | ||||
| Do you think that the benefits of COVID-19 vaccines outweigh their reported side effects/adverse reactions? | No | 1188 | 17.9% | 17.9% |
| Not Sure | 2082 | 31.4% | 49.3% | |
| Yes | 3369 | 50.7% | 100% | |
| In general, when a new vaccine is introduced, are you inclined to consent to your vaccination? | No | 1606 | 24.2% | 24.2% |
| Not Sure | 2162 | 32.6% | 56.8% | |
| Yes | 2871 | 43.2% | 100% | |
| Do you feel confident that the health center or doctor’s office will have the COVID-19 vaccines you need, when you need them? | No | 1778 | 26.8% | 26.8% |
| Not Sure | 2158 | 32.5% | 59.3% | |
| Yes | 2703 | 40.7% | 100% | |
| Economic Level | Pharmaceutical Industry | Natural Immunity | Risk/Benefit Ratio | Novel Vaccines | Vaccination Willingness | ||
|---|---|---|---|---|---|---|---|
| Economic Level | ρ | 1.000 | |||||
| Sig. | N/A | ||||||
| Pharmaceutical Industry | ρ | 0.209 | 1.000 | ||||
| Sig. | <0.001 | N/A | |||||
| Natural Immunity | ρ | −0.222 | −0.113 | 1.000 | |||
| Sig. | <0.001 | <0.001 | N/A | ||||
| Risk/Benefit Ratio | ρ | 0.199 | 0.389 | −0.125 | 1.000 | ||
| Sig. | <0.001 | <0.001 | <0.001 | N/A | |||
| Novel Vaccines | ρ | 0.167 | 0.396 | −0.085 | 0.385 | 1.000 | |
| Sig. | <0.001 | <0.001 | <0.001 | <0.001 | N/A | ||
| Vaccination Willingness | ρ | 0.236 | 0.401 | −0.267 | 0.390 | 0.424 | 1.000 |
| Sig. | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | N/A |
| Groups | Name | SD | Variance | ICC |
|---|---|---|---|---|
| Economic Level | (Intercept) | 0.142 | 0.0202 | 0.0191 |
| Residual | 1.019 | 1.0388 |
| 95% Confidence Intervale | |||||||
|---|---|---|---|---|---|---|---|
| Predictor | Estimate | SE | Lower | Upper | df | t | Sig. |
| (Intercept) | 3.809 | 0.073 | 3.666 | 3.951 | 2.96 | 52.3 | <0.001 |
| Pharmaceutical Industry | 0.304 | 0.018 | 0.269 | 0.340 | 6633.72 | 16.8 | <0.001 |
| Natural Immunity | −0.270 | 0.016 | −0.301 | −0.239 | 6604.25 | −17.1 | <0.001 |
| Risk/Benefit Ratio | 0.285 | 0.019 | 0.248 | 0.322 | 6633.77 | 15.2 | <0.001 |
| Novel Vaccines | 0.382 | 0.018 | 0.347 | 0.417 | 6633.99 | 21.5 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riad, A.; Huang, Y.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E.; IADS-SCORE. Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach. Vaccines 2021, 9, 1158. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101158
Riad A, Huang Y, Abdulqader H, Morgado M, Domnori S, Koščík M, Mendes JJ, Klugar M, Kateeb E, IADS-SCORE. Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach. Vaccines. 2021; 9(10):1158. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101158
Chicago/Turabian StyleRiad, Abanoub, Yi Huang, Huthaifa Abdulqader, Mariana Morgado, Silvi Domnori, Michal Koščík, José João Mendes, Miloslav Klugar, Elham Kateeb, and IADS-SCORE. 2021. "Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach" Vaccines 9, no. 10: 1158. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101158