
Microbiome of Saliva and Plaque in Children According to Age and Dental Caries Experience

 , , ,
, , ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
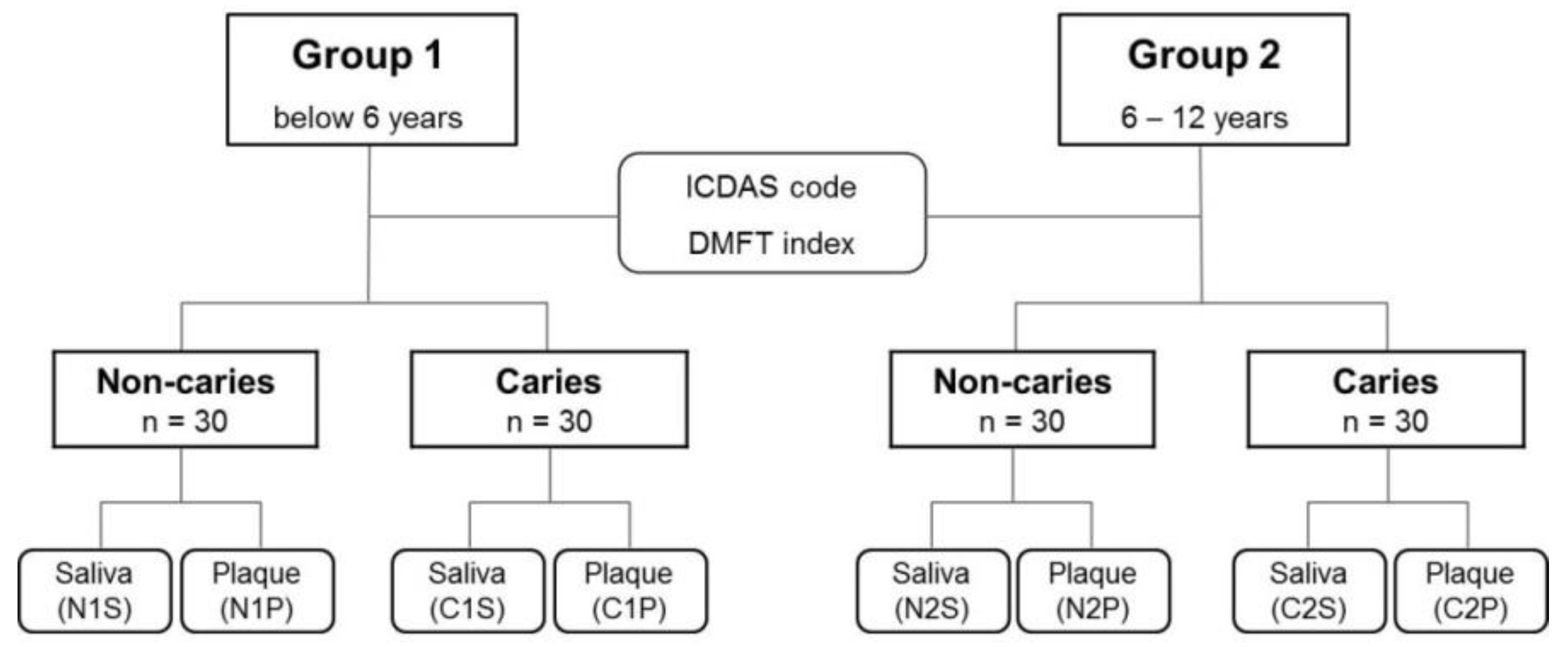
2.1. Patient Selection and Oral Examination
2.2. Sample Preparation and DNA Extraction
2.3. Polymerase Chain Reaction Amplification of 16S rRNA Genes and Sequencing Data Analysis
2.4. Statistical Analysis
2.5. Machine Learning Models for Classifying Non-Caries and Caries Samples
3. Results
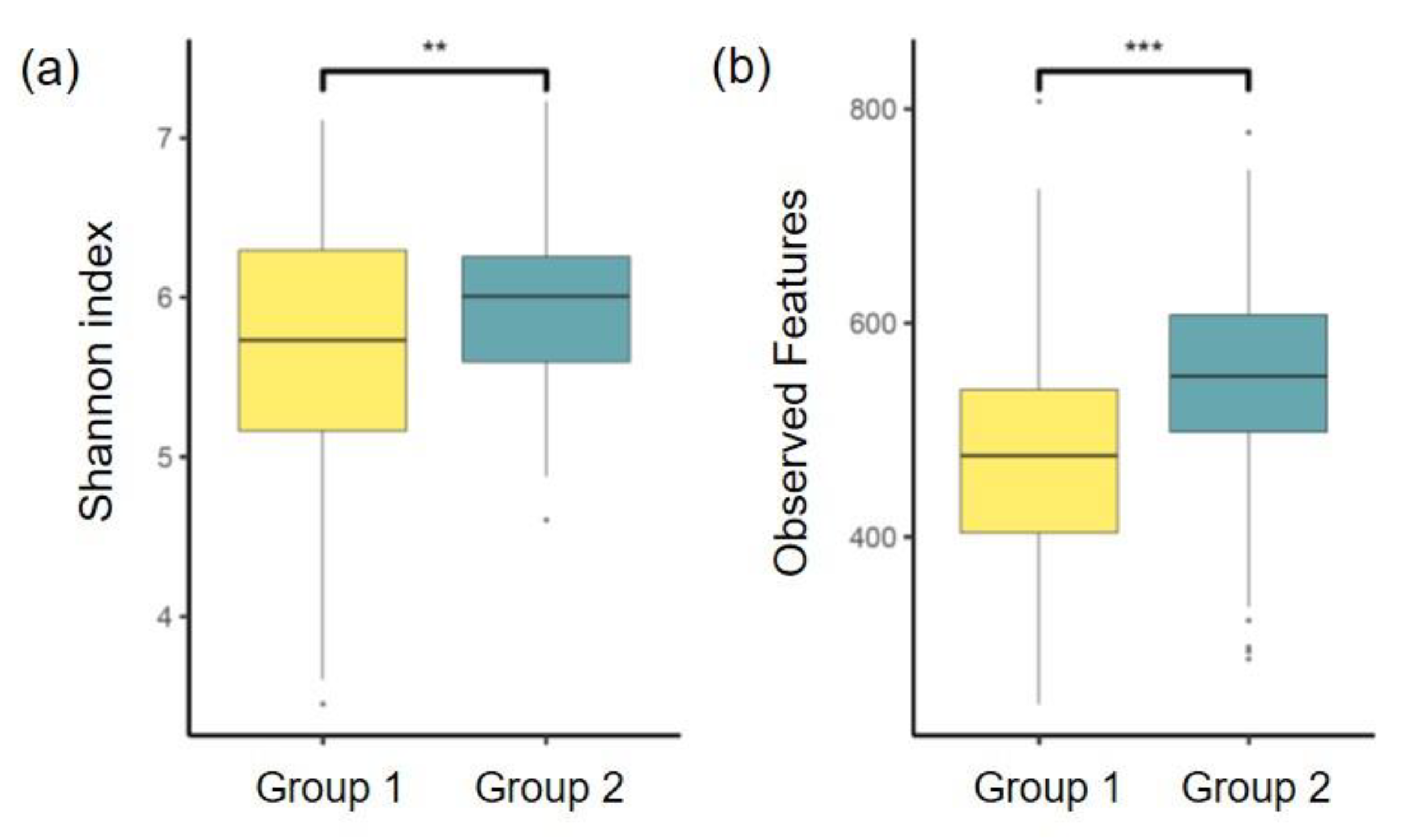
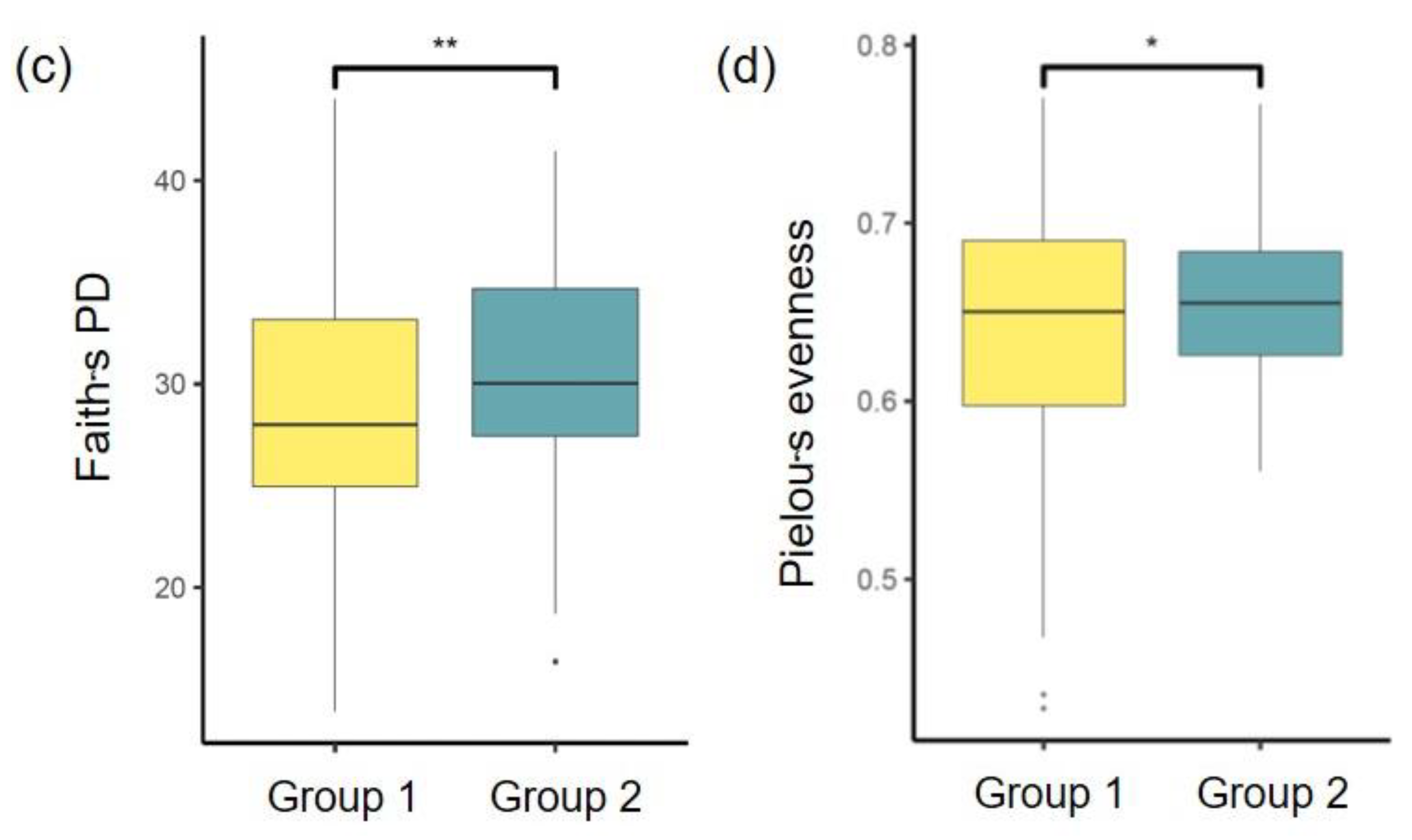
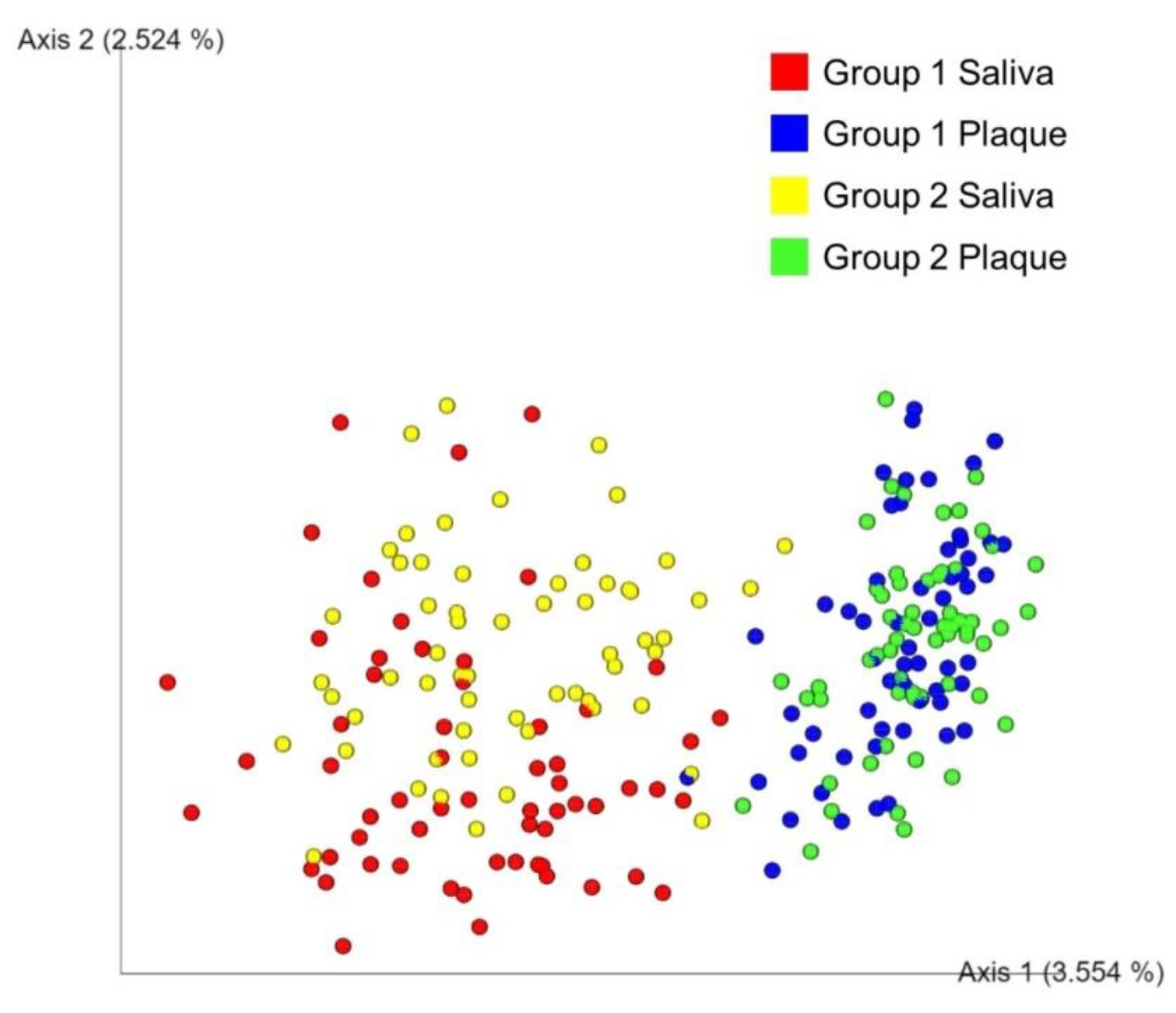
3.1. Alpha and Beta Diversity Analysis
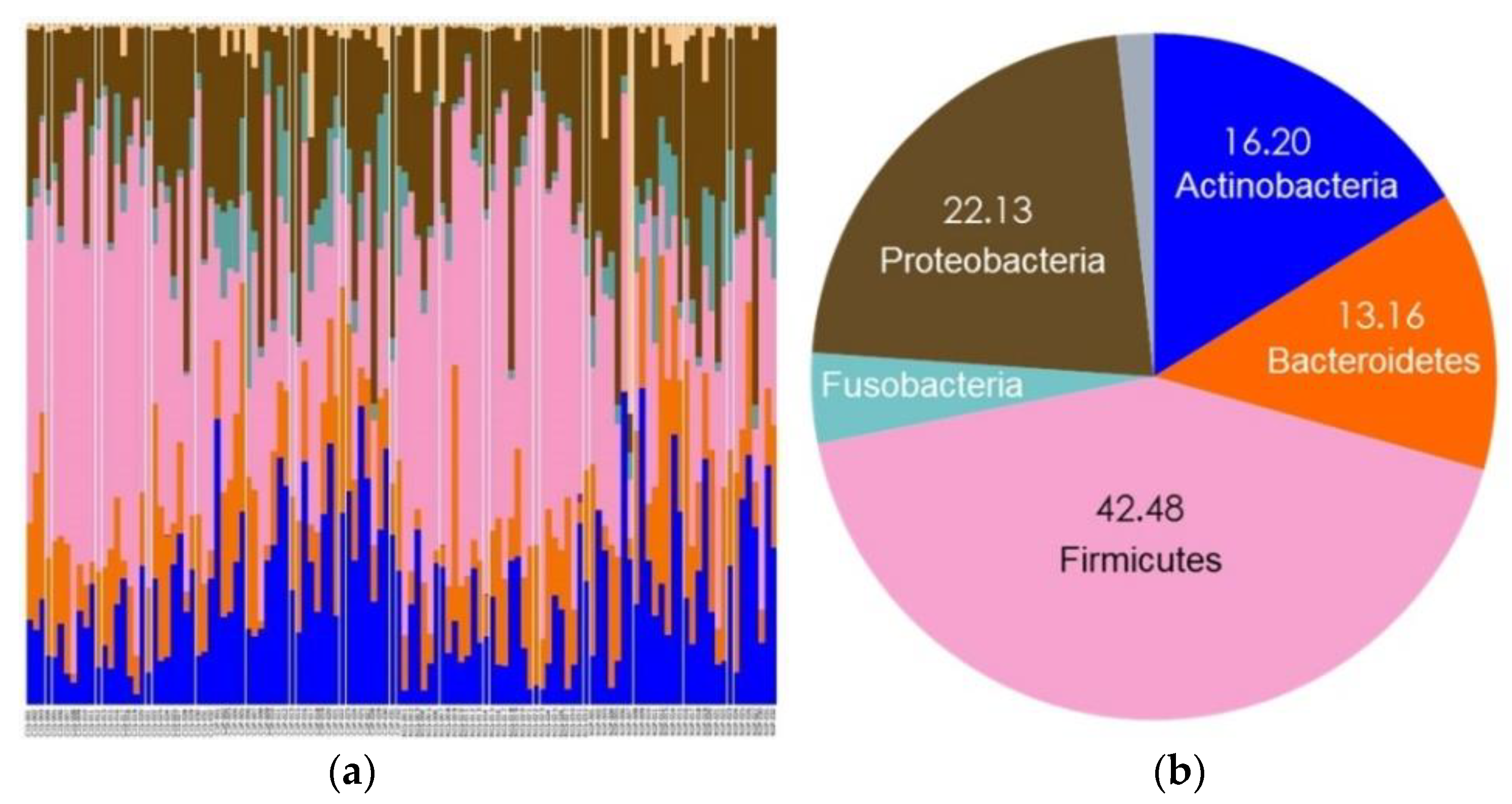
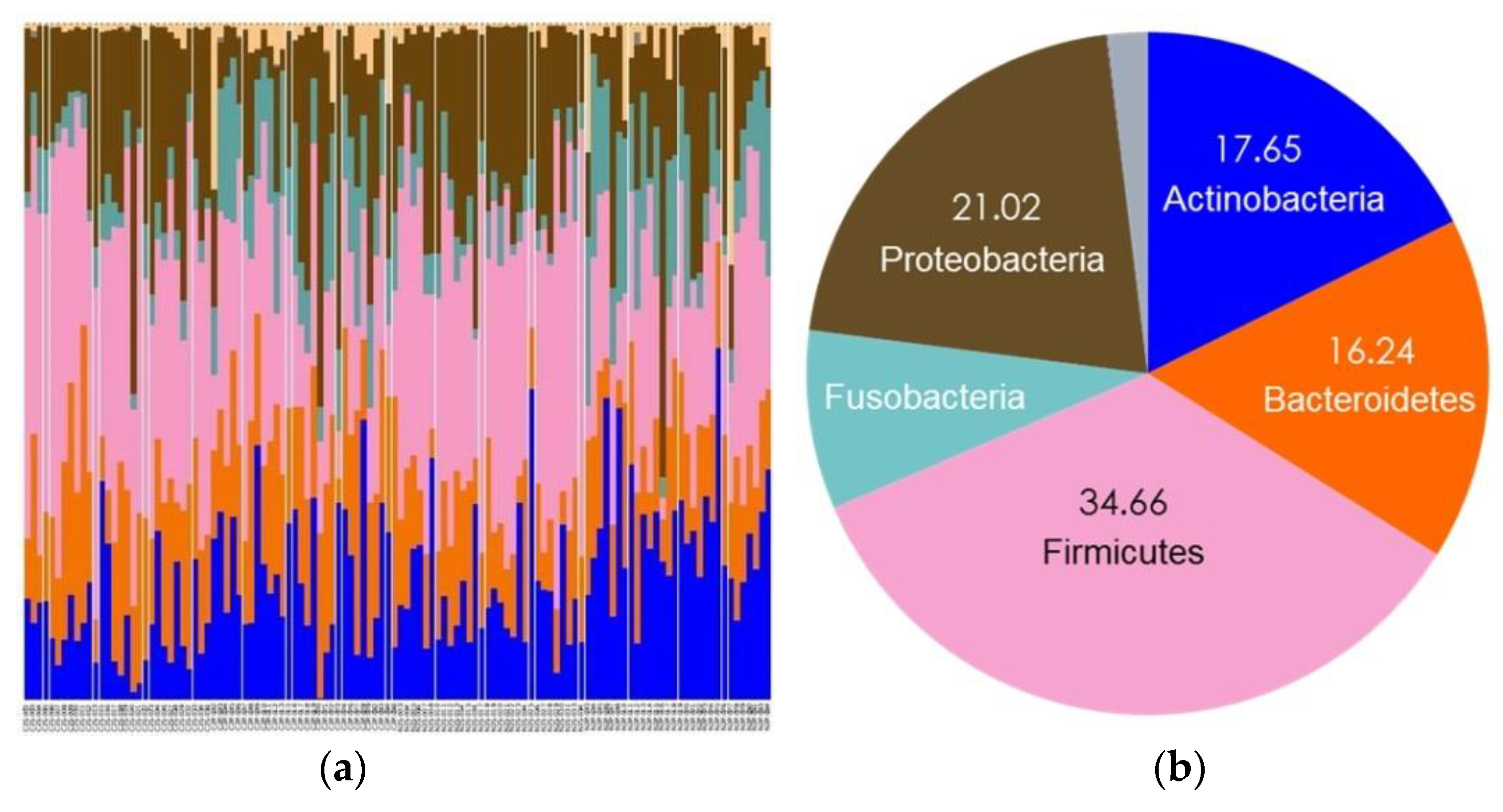
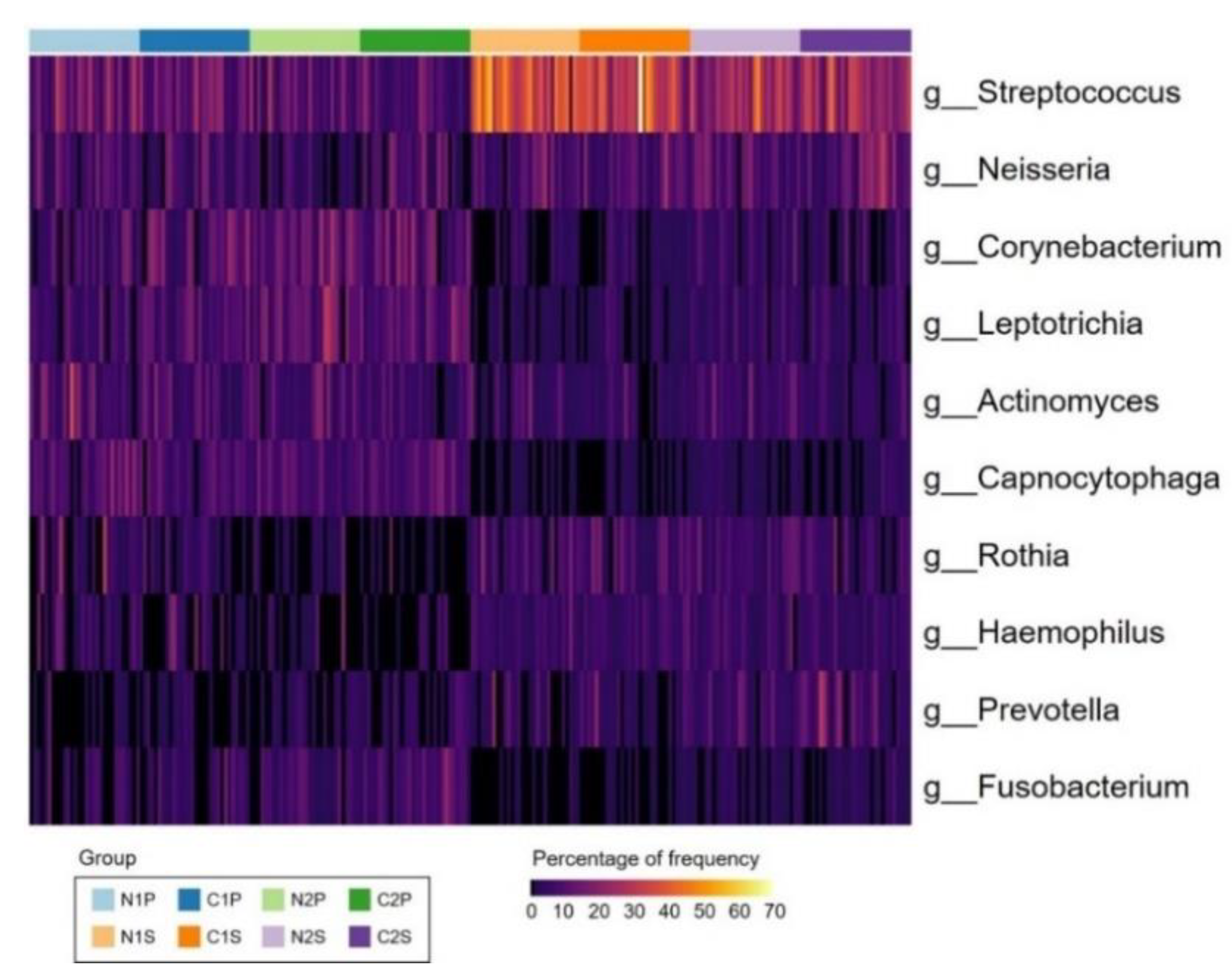
3.2. Bacterial Compositions
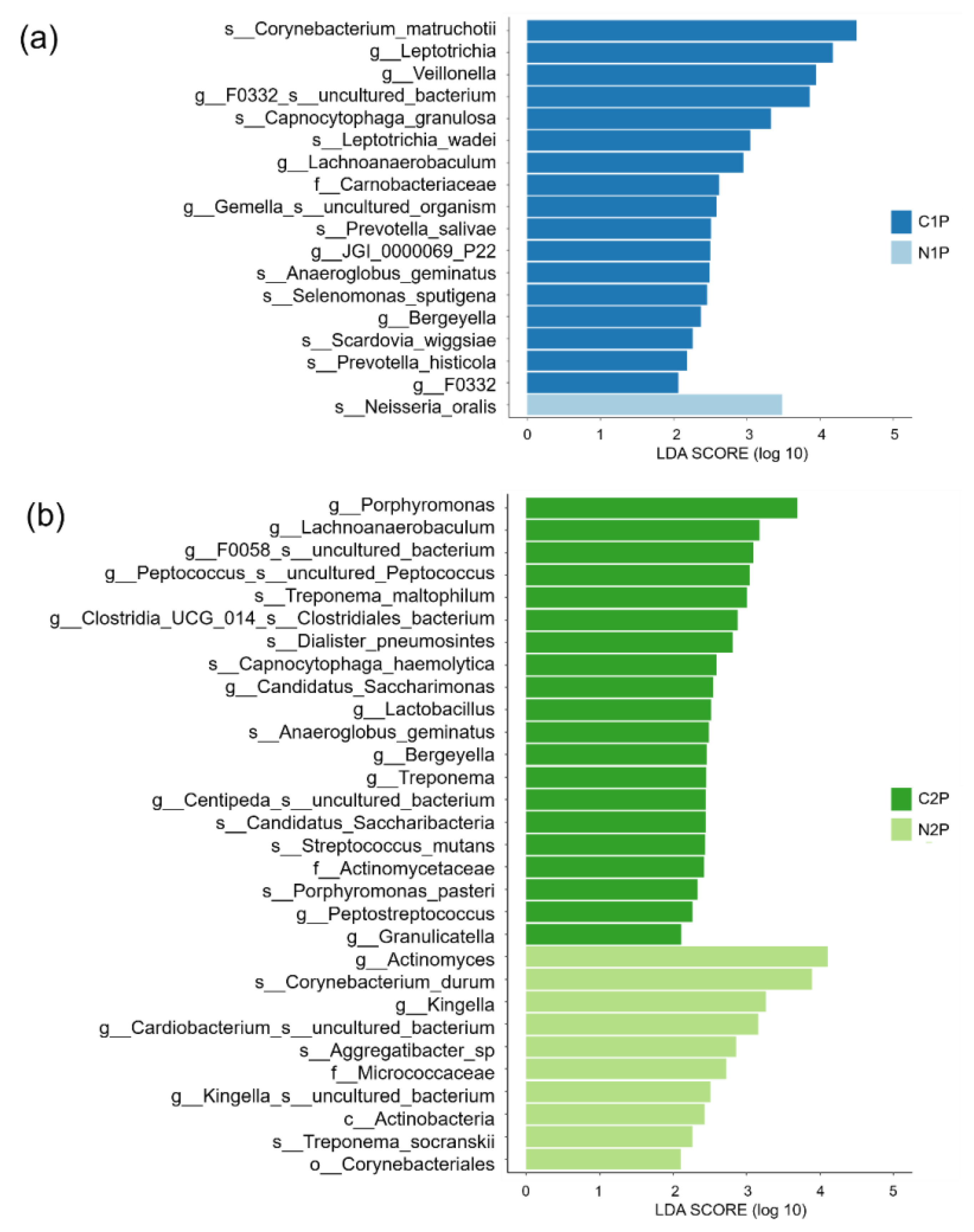
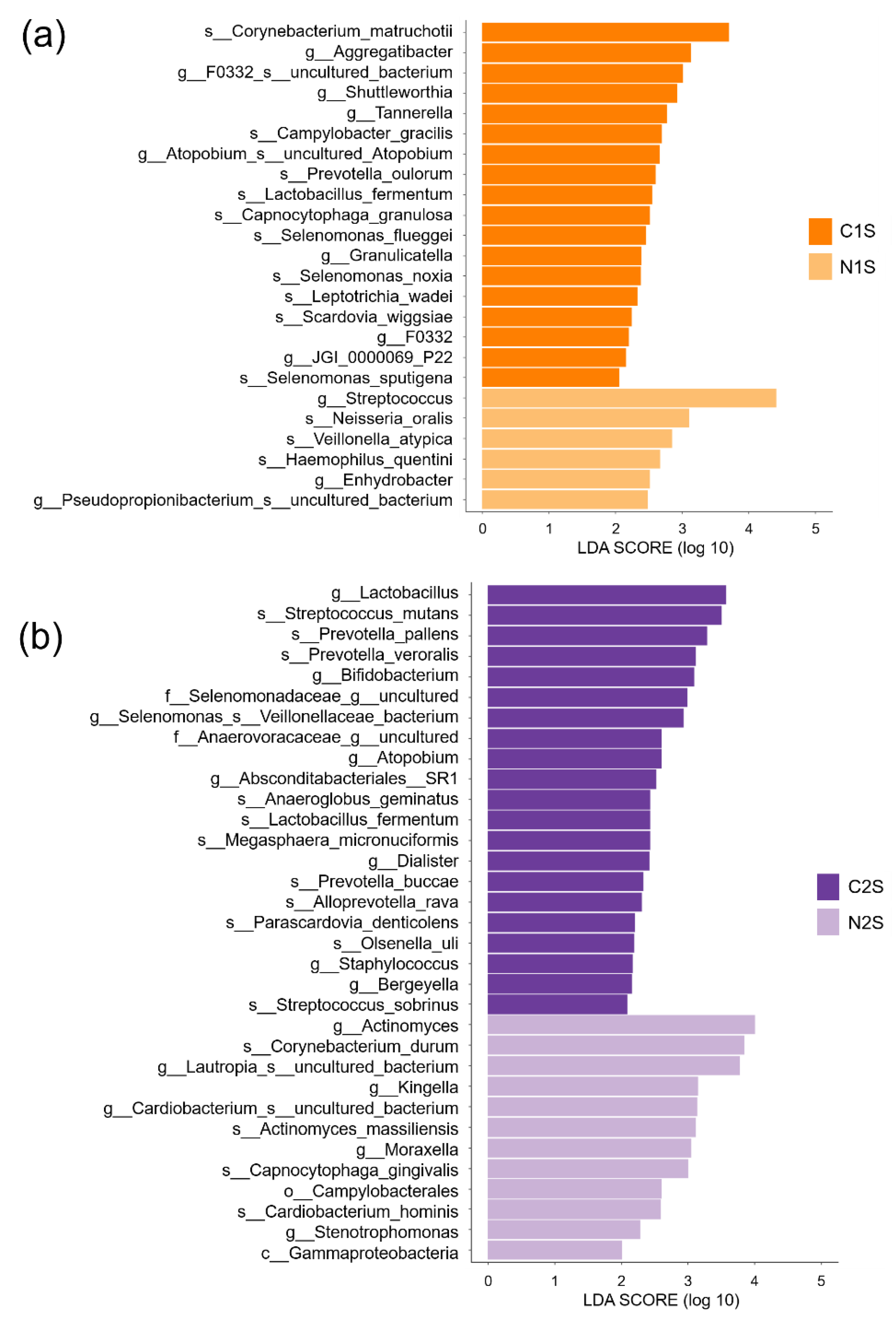
3.3. Differential Abundance Analysis
3.4. Classification of Samples Using the Random Forest Machine Learning Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kazeminia, M.; Abdi, A.; Shohaimi, S.; Jalali, R.; Vaisi-Raygani, A.; Salari, N.; Mohammadi, M. Dental caries in primary and permanent teeth in children’s worldwide, 1995 to 2019: A systematic review and meta-analysis. Head Face Med. 2020, 16, 22. [Google Scholar] [CrossRef]
- Choi, C.H. 2018 Korea National Children’s Oral Health Survey; National Center for Medical Information and Knowledge: Cheongju-si, Korea, 2018. [Google Scholar]
- Featherstone, J.D. Prevention and reversal of dental caries: Role of low level fluoride. Community Dent. Oral Epidemiol. 1999, 27, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.Y.; Park, S.J.; Jeong, D.K.; Kim, K.W.; Lim, S.H.; Lee, S.H.; Choe, S.J.; Chang, Y.H.; Park, I.; Kook, J.K. Isolation and characterization of the mutans streptococci from the dental plaques in Koreans. J. Microbiol. 2007, 45, 246–255. [Google Scholar]
- Deo, P.; Deshmukh, R. Oral microbiome: Unveiling the fundamentals. J. Oral Maxillofac. Pathol. 2019, 23, 122–128. [Google Scholar] [CrossRef]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.R.; Wen-Han, Y.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, L.; Lif Holgerson, P.; Johansson, I. Saliva and tooth biofilm bacterial microbiota in adolescents in a low caries community. Sci. Rep. 2017, 7, 5861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimomura-Kuroki, J.; Yamashita-Matsuda, K.; Miyagawa, Y.; Shimooka, S. Prevalence of cariogenic and periodontopathic bacteria in Japanese children in the primary and mixed dentitions. J. Clin. Pediatr. Dent. 2011, 36, 31–36. [Google Scholar] [CrossRef]
- Lederberg, J.; McCray, A.T. ‘Ome sweet ‘omics—A genealogical treasury of words. Scientist 2001, 15, 8. [Google Scholar]
- Adak, A.; Khan, M.R. An insight into gut microbiota and its functionalities. Cell Mol. Life Sci. 2019, 76, 473–493. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Bonczek, O.; Bielik, P.; Krejčí, P.; Zeman, T.; Izakovičová-Hollá, L.; Šoukalová, J.; Vaněk, J.; Gerguri, T.; Balcar, V.J.; Šerý, O. Next generation sequencing reveals a novel nonsense mutation in MSX1 gene related to oligodontia. PLoS ONE 2018, 13, e0202989. [Google Scholar] [CrossRef]
- Cherkasov, S.V.; Popova, L.Y.; Vivtanenko, T.V.; Demina, R.R.; Khlopko, Y.A.; Balkin, A.S.; Plotnikov, A.O. Oral microbiomes in children with asthma and dental caries. Oral Dis. 2019, 25, 898–910. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, J.W.; Park, Y.S. The Application of Next-Generation Sequencing to Define Factors Related to Oral Cancer and Discover Novel Biomarkers. Life 2020, 10, 228. [Google Scholar] [CrossRef]
- Manoil, D.; Al-Manei, K.; Belibasakis, G.N. A Systematic Review of the Root Canal Microbiota Associated with Apical Periodontitis: Lessons from Next-Generation Sequencing. Proteomics Clin. Appl. 2020, 14, e1900060. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Qi, Y.; Lo, E.C.M.; McGrath, C.; Mei, M.L.; Dai, R. Using next-generation sequencing to detect oral microbiome change following periodontal interventions: A systematic review. Oral Dis. 2020, 27, 1073–1089. [Google Scholar] [CrossRef]
- Chen, T.; Shi, Y.; Wang, X.; Wang, X.; Meng, F.; Yang, S.; Yang, J.; Xin, H. High-throughput sequencing analyses of oral microbial diversity in healthy people and patients with dental caries and periodontal disease. Mol. Med. Rep. 2017, 16, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Crielaard, W.; Zaura, E.; Schuller, A.A.; Huse, S.M.; Montijn, R.C.; Keijser, B.J. Exploring the oral microbiota of children at various developmental stages of their dentition in the relation to their oral health. BMC Med. Genom. 2011, 4, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzidic, M.; Collado, M.C.; Abrahamsson, T.; Artacho, A.; Stensson, M.; Jenmalm, M.C.; Mira, A. Oral microbiome development during childhood: An ecological succession influenced by postnatal factors and associated with tooth decay. ISME J. 2018, 12, 2292–2306. [Google Scholar] [CrossRef] [PubMed]
- Richards, V.P.; Alvarez, A.J.; Luce, A.R.; Bedenbaugh, M.; Mitchell, M.L.; Burne, R.A.; Nascimento, M.M. Microbiomes of Site-Specific Dental Plaques from Children with Different Caries Status. Infect. Immun. 2017, 85. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; He, J.; Xue, J.; Wang, Y.; Li, K.; Zhang, K.; Guo, Q.; Liu, X.; Zhou, Y.; Cheng, L.; et al. Oral cavity contains distinct niches with dynamic microbial communities. Environ. Microbiol. 2015, 17, 699–710. [Google Scholar] [CrossRef]
- Carounanidy, U.; Sathyanarayanan, S. Dental caries—A complete changeover (Part I). J. Conserv. Dent. 2009, 12, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.J.; Kim, J.H.; Lee, D.W.; Yang, Y.M.; Kim, J.G. Prevalence of Periodontopathogens in Saliva and Plaque of Korean Children and Adolescents. J. Korean Acad. Pediatr. Dent. 2016, 43, 8–16. [Google Scholar] [CrossRef]
- Kang, J.G.; Kim, S.H.; Ahn, T.Y. Bacterial diversity in the human saliva from different ages. J. Microbiol. 2006, 44, 572–576. [Google Scholar] [PubMed]
- Kim, B.S.; Han, D.H.; Lee, H.; Oh, B.J. Association of Salivary Microbiota with Dental Caries Incidence with Dentine Involvement after 4 Years. J. Microbiol. Biotechnol. 2018, 28, 454–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.M. Isolation and identification of the abundant bacteria in dental caries in children. J. Korean Soc. Dent. Hyg. 2018, 18, 843–852. [Google Scholar]
- Lee, H.S.; Lee, J.H.; Kim, S.O.; Song, J.S.; Lee, J.H.; Kim, B.I.; Kim, Y.J. Comparison of the oral microbiome of siblings using next-generation sequencing: A pilot study. Oral Dis. 2016, 22, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Omori, M.; Kato-Kogoe, N.; Sakaguchi, S.; Kamiya, K.; Fukui, N.; Gu, Y.H.; Nakamura, S.; Nakano, T.; Hoshiga, M.; Imagawa, A.; et al. Characterization of salivary microbiota in elderly patients with type 2 diabetes mellitus: A matched case-control study. Clin. Oral Investig. 2021, 1–12. [Google Scholar] [CrossRef]
- Kato-Kogoe, N.; Sakaguchi, S.; Kamiya, K.; Omori, M.; Gu, Y.H.; Ito, Y.; Nakamura, S.; Nakano, T.; Tamaki, J.; Ueno, T.; et al. Characterization of Salivary Microbiota in Patients with Atherosclerotic Cardiovascular Disease: A Case-Control Study. J. Atheroscler. Thromb. 2021, 60608. [Google Scholar] [CrossRef]
- Alia-García, E.; Ponce-Alonso, M.; Saralegui, C.; Halperin, A.; Cortés, M.P.; Baquero, M.R.; Parra-Pecharromán, D.; Galeano, J.; Del Campo, R. Machine Learning Study in Caries Markers in Oral Microbiota from Monozygotic Twin Children. Diagnostics 2021, 11, 835. [Google Scholar] [CrossRef]
- Grier, A.; Myers, J.A.; O’Connor, T.G.; Quivey, R.G.; Gill, S.R.; Kopycka-Kedzierawski, D.T. Oral Microbiota Composition Predicts Early Childhood Caries Onset. J. Dent. Res. 2021, 100, 599–607. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, S.; Wu, C.; Chen, X.; Duan, Z.; Xu, Q.; Jiang, W.; Xu, L.; Wang, T.; Su, L.; et al. Oral Microbiome Alterations Associated with Early Childhood Caries Highlight the Importance of Carbohydrate Metabolic Activities. mSystems 2019, 4. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Baez, R.J.; World Health, O. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Naidu, B.; Reginald, B. Quantification and Correlation of Oral Candida with Caries Index Among Different Age Groups of School Children: A Case-Control Study. Ann. Med. Health Sci. Res. 2016, 6, 80–84. [Google Scholar]
- Singla, D.; Sharma, A.; Sachdev, V.; Chopra, R. Distribution of Streptococcus mutans and Streptococcus sobrinus in Dental Plaque of Indian Pre-School Children Using PCR and SB-20M Agar Medium. J. Clin. Diagn. Res. 2016, 10, 60–63. [Google Scholar] [CrossRef]
- Kado, I.; Hisatsune, J.; Tsuruda, K.; Tanimoto, K.; Sugai, M. The impact of fixed orthodontic appliances on oral microbiome dynamics in Japanese patients. Sci. Rep. 2020, 10, 21989. [Google Scholar] [CrossRef]
- Dashper, S.G.; Mitchell, H.L.; KA, L.C.; Carpenter, L.; Gussy, M.G.; Calache, H.; Gladman, S.L.; Bulach, D.M.; Hoffmann, B.; Catmull, D.V.; et al. Temporal development of the oral microbiome and prediction of early childhood caries. Sci. Rep. 2019, 9, 19732. [Google Scholar] [CrossRef]
- Luo, A.H.; Yang, D.Q.; Xin, B.C.; Paster, B.J.; Qin, J. Microbial profiles in saliva from children with and without caries in mixed dentition. Oral Dis. 2012, 18, 595–601. [Google Scholar] [CrossRef]
- Kim, E.H.; Joo, J.Y.; Lee, Y.J.; Koh, J.K.; Choi, J.H.; Shin, Y.; Cho, J.; Park, E.; Kang, J.; Lee, K.; et al. Grading system for periodontitis by analyzing levels of periodontal pathogens in saliva. PLoS ONE 2018, 13, e0200900. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Kim, E.H.; Kim, S.; Kim, H.J.; Jeong, H.O.; Lee, J.; Jang, J.; Joo, J.Y.; Shin, Y.; Kang, J.; Park, A.K.; et al. Prediction of Chronic Periodontitis Severity Using Machine Learning Models Based on Salivary Bacterial Copy Number. Front. Cell Infect. Microbiol. 2020, 10, 571515. [Google Scholar] [CrossRef]
- Chen, H.; Jiang, W. Application of high-throughput sequencing in understanding human oral microbiome related with health and disease. Front. Microbiol. 2014, 5, 508. [Google Scholar] [CrossRef] [Green Version]
- Marsh, P.D. Microbial ecology of dental plaque and its significance in health and disease. Adv. Dent. Res. 1994, 8, 263–271. [Google Scholar] [CrossRef]
- Gomez, J. Detection and diagnosis of the early caries lesion. BMC Oral Health 2015, 15 (Suppl. 1), S3. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.H.; Lee, S.R.; Choi, J.Y.; Choi, Y.S.; Kim, S.H.; Yoon, H.C.; Nelson, G. Detection of Dental Caries and Cracks with Quantitative Light-Induced Fluorescence in Comparison to Radiographic and Visual Examination: A Retrospective Case Study. Sensors 2021, 21, 1741. [Google Scholar] [CrossRef]
- Dİkmen, B. ICDAS II Criteria (International Caries Detection and Assessment System). J. Istanb. Univ. Fac. Dent. 2015, 49, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Braga, M.M.; Oliveira, L.B.; Bonini, G.A.; Bönecker, M.; Mendes, F.M. Feasibility of the International Caries Detection and Assessment System (ICDAS-II) in epidemiological surveys and comparability with standard World Health Organization criteria. Caries Res. 2009, 43, 245–249. [Google Scholar] [CrossRef]
- Bhoopathi, P.H.; Patil, P.U.; Kamath, B.V.; Gopal, D.; Kumar, S.; Kulkarni, G. Caries Detection with ICDAS and the WHO Criteria: A Comparitive Study. J. Clin. Diagn Res. 2017, 11, 9–12. [Google Scholar] [CrossRef]
- Cavalheiro, C.P.; Souza, P.S.; Pedrotti, D.; Casagrande, L.; Ardenghi, T.M.; Rocha, R.O.; Raggio, D.P.; Lenzi, T.L. Shortening of etching time of the dentin in primary teeth restorations: A randomized clinical trial. Braz. Oral Res. 2020, 34, e081. [Google Scholar] [CrossRef]
- Segata, N.; Haake, S.K.; Mannon, P.; Lemon, K.P.; Waldron, L.; Gevers, D.; Huttenhower, C.; Izard, J. Composition of the adult digestive tract bacterial microbiome based on seven mouth surfaces, tonsils, throat and stool samples. Genome Biol. 2012, 13, R42. [Google Scholar] [CrossRef] [Green Version]
- Simón-Soro, A.; Tomás, I.; Cabrera-Rubio, R.; Catalan, M.D.; Nyvad, B.; Mira, A. Microbial geography of the oral cavity. J. Dent. Res. 2013, 92, 616–621. [Google Scholar] [CrossRef]
- Yang, F.; Zeng, X.; Ning, K.; Liu, K.L.; Lo, C.C.; Wang, W.; Chen, J.; Wang, D.; Huang, R.; Chang, X.; et al. Saliva microbiomes distinguish caries-active from healthy human populations. ISME J. 2012, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bik, E.M.; Long, C.D.; Armitage, G.C.; Loomer, P.; Emerson, J.; Mongodin, E.F.; Nelson, K.E.; Gill, S.R.; Fraser-Liggett, C.M.; Relman, D.A. Bacterial diversity in the oral cavity of 10 healthy individuals. ISME J. 2010, 4, 962–974. [Google Scholar] [CrossRef] [PubMed]
- Cephas, K.D.; Kim, J.; Mathai, R.A.; Barry, K.A.; Dowd, S.E.; Meline, B.S.; Swanson, K.S. Comparative analysis of salivary bacterial microbiome diversity in edentulous infants and their mothers or primary care givers using pyrosequencing. PLoS ONE 2011, 6, e23503. [Google Scholar] [CrossRef]
- Ren, W.; Zhang, Q.; Liu, X.; Zheng, S.; Ma, L.; Chen, F.; Xu, T.; Xu, B. Exploring the oral microflora of preschool children. J. Microbiol 2017, 55, 531–537. [Google Scholar] [CrossRef]
- Shi, W.; Tian, J.; Xu, H.; Zhou, Q.; Qin, M. Distinctions and associations between the microbiota of saliva and supragingival plaque of permanent and deciduous teeth. PLoS ONE 2018, 13, e0200337. [Google Scholar] [CrossRef] [PubMed]
- Samaranayake, L. Essential Microbiology for Dentistry, 4th ed.; Elsevier, Churchill Livingstone: London, UK, 2013; pp. 265–286. [Google Scholar]
- Shi, W.; Qin, M.; Chen, F.; Xia, B. Supragingival Microbial Profiles of Permanent and Deciduous Teeth in Children with Mixed Dentition. PLoS ONE 2016, 11, e0146938. [Google Scholar] [CrossRef] [Green Version]
- Inquimbert, C.; Bourgeois, D.; Bravo, M.; Viennot, S.; Tramini, P.; Llodra, J.C.; Molinari, N.; Dussart, C.; Giraudeau, N.; Carrouel, F. The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk. Microorganisms 2019, 7, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgeois, D.; David, A.; Inquimbert, C.; Tramini, P.; Molinari, N.; Carrouel, F. Quantification of carious pathogens in the interdental microbiota of young caries-free adults. PLoS ONE 2017, 12, e0185804. [Google Scholar] [CrossRef] [Green Version]
- Bao, K.; Bostanci, N.; Thurnheer, T.; Belibasakis, G.N. Proteomic shifts in multi-species oral biofilms caused by Anaeroglobus geminatus. Sci. Rep. 2017, 7, 4409. [Google Scholar] [CrossRef] [Green Version]
- Badet, C.; Thebaud, N.B. Ecology of lactobacilli in the oral cavity: A review of literature. Open Microbiol. J. 2008, 2, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Caufield, P.W.; Schön, C.N.; Saraithong, P.; Li, Y.; Argimón, S. Oral Lactobacilli and Dental Caries: A Model for Niche Adaptation in Humans. J. Dent. Res. 2015, 94, 110s–118s. [Google Scholar] [CrossRef] [PubMed]
- Idate, U.; Bhat, K.; Kotrashetti, V.; Kugaji, M.; Kumbar, V. Molecular identification of Capnocytophaga species from the oral cavity of patients with chronic periodontitis and healthy individuals. J. Oral Maxillofac. Pathol. 2020, 24, 397. [Google Scholar] [CrossRef] [PubMed]
- Schoilew, K.; Ueffing, H.; Dalpke, A.; Wolff, B.; Frese, C.; Wolff, D.; Boutin, S. Bacterial biofilm composition in healthy subjects with and without caries experience. J. Oral Microbiol. 2019, 11, 1633194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qudeimat, M.A.; Alyahya, A.; Karched, M.; Behbehani, J.; Salako, N.O. Dental plaque microbiota profiles of children with caries-free and caries-active dentition. J. Dent. 2021, 104, 103539. [Google Scholar] [CrossRef] [PubMed]
- Wolfgang, W.J.; Passaretti, T.V.; Jose, R.; Cole, J.; Coorevits, A.; Carpenter, A.N.; Jose, S.; Van Landschoot, A.; Izard, J.; Kohlerschmidt, D.J.; et al. Neisseria oralis sp. nov., isolated from healthy gingival plaque and clinical samples. Int. J. Syst. Evol. Microbiol. 2013, 63, 1323–1328. [Google Scholar] [CrossRef]
- Popa, C.; Filioreanu, A.M.; Stelea, C.; Maftei, G.A.; Popescu, E. Prevalence of oral lesions modulated by patient’s age: The young versus the elderly. Rom. J. Oral Rehabil. 2018, 10, 50–56. [Google Scholar]
- Martu, M.-A.; Maftei, G.-A.; Luchian, I.; Popa, C.; Filioreanu, A.-M.; Tatarciuc, D.; Nichitean, G.; Hurjui, L.-L.; Foia, L.-G. Wound Healing of Periodontal and Oral Tissues: Part II—Patho-Physiological Conditions and Metabolic Diseases. Review. Rom. J. Oral Rehabil. 2020, 12, 30–40. [Google Scholar]
- Solomon, S.M.; Bataiosu, M.; Popescu, D.M.; Rauten, A.M.; Gheorghe, D.N.; Petrescu, R.A.; Maftei, G.A.; Maglaviceanu, C.F. Biochemical Assesment of Salivary Parameters in Young Patients with Dental Lesions. Rev. Chim. 2019, 70, 4095–4097. [Google Scholar] [CrossRef]
- Fiorillo, L. Oral Health: The First Step to Well-Being. Medicina 2019, 55, 676. [Google Scholar] [CrossRef] [Green Version]
- Gupta, V.K.; Paul, S.; Dutta, C. Geography, Ethnicity or Subsistence-Specific Variations in Human Microbiome Composition and Diversity. Front. Microbiol. 2017, 8, 1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Gender | n | Mean Age (SD) | p-Value | |
|---|---|---|---|---|---|
| Non-caries | (N1) 1 | Male | 10 | 4.3 (0.5) | 0.731 |
| Female | 20 | 4.4 (0.7) | |||
| Caries | (C1) 1 | Male | 15 | 4.6 (0.7) | 0.603 |
| Female | 15 | 4.5 (0.7) | |||
| Non-caries | (N2) 2 | Male | 14 | 8.1 (1.3) | 0.560 |
| Female | 16 | 7.9 (1.4) | |||
| Caries | (C2) 2 | Male | 21 | 7.9 (1.3) | 0.733 |
| Female | 9 | 7.9 (1.4) | |||
| Total | 120 | 6.2 (2.0) | |||
| Groups (n) | d + D 1 | ICDAS 2 Score |
|---|---|---|
| Mean (SD) | Mean (SD) | |
| Non-caries (60) | 0.00 (0.00) | 0.30 (0.71) |
| Caries (60) | 5.73 (3.51) | 4.12 (0.78) |
| p-value | <0.001 * | <0.001 * |
| Group | Feature Combination | Accuracy | Balanced Accuracy | Precision | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| N1P vs. C1P | V + Lep | 0.78 (0.14) | 0.81 (0.13) | 0.80 (0.19) | 0.80 (0.15) | 0.81 (0.16) |
| N1S vs. C1S | Sw + Cgra + Str + Cm + Gra + Agg + No + Lw | 0.70 (0.18) | 0.71 (0.19) | 0.67 (0.18) | 0.74 (0.20) | 0.69 (0.20) |
| N2P vs. C2P | Cun + Gra + Lac + Por + CS + cbac + Cd + Kun | 0.73 (0.10) | 0.75 (0.10) | 0.73 (0.17) | 0.74 (0.08) | 0.75 (0.13) |
| N2S vs. C2S | Sta + Act + Cun + B + Ato + Cgin | 0.83 (0.13) | 0.84 (0.13) | 0.87 (0.12) | 0.82 (0.14) | 0.86 (0.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.; Park, S.; Um, S.; Kim, S.; Lee, J.; Jang, J.; Jeong, H.-o.; Shin, J.; Kang, J.; Lee, S.; et al. Microbiome of Saliva and Plaque in Children According to Age and Dental Caries Experience. Diagnostics 2021, 11, 1324. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081324
Lee E, Park S, Um S, Kim S, Lee J, Jang J, Jeong H-o, Shin J, Kang J, Lee S, et al. Microbiome of Saliva and Plaque in Children According to Age and Dental Caries Experience. Diagnostics. 2021; 11(8):1324. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081324
Chicago/Turabian StyleLee, Eungyung, Suhyun Park, Sunwoo Um, Seunghoon Kim, Jaewoong Lee, Jinho Jang, Hyoung-oh Jeong, Jonghyun Shin, Jihoon Kang, Semin Lee, and et al. 2021. "Microbiome of Saliva and Plaque in Children According to Age and Dental Caries Experience" Diagnostics 11, no. 8: 1324. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11081324