1. Introduction
Common and chronic forms of nasal inflammation include rhinosinusitis, nasal polyposis, nonallergic rhinitis with eosinophilia syndrome (NARES) and allergic rhinitis (AR). Allergic rhinitis is the most frequent manifestation of atopic diseases, with almost 80 million people affected in the United States. It accounts for about 50% of patients with chronic rhinitis [
1]. Patients suffer from nasal pruritus and rhinorrhea. Impairment of quality of life, including loss of concentration, loss of sense of smell, headaches and sleep disturbances, are well documented [
2]. Diagnosis of allergic rhinitis is achieved by a combination of differentiated patient history and screening tests, followed by specific in vitro testing and nasal provocation to confirm the diagnosis. Many different inhalant allergens are known to cause allergic symptoms, and the patient’s history gives first clues to the relevant allergens [
3]. In a screening test (usually skin prick test (SPT) or intradermal testing), the sensitization of a patient to a specific allergen can be evaluated. This can then be further specified or confirmed by in vitro diagnosis of specific serum IgE. However, the above tests sometimes show conflicting results and little correlation. Usually, SPT is considered more sensitive than specific serum IgE testing [
4,
5]. Other authors report a better correlation of test results depending on the allergen looked at, with persistent allergens such as mite, dog, cat or mold showing a weaker correlation than seasonal allergens [
6,
7]. The “gold standard” in the diagnosis of allergic rhinitis is nasal provocation [
8,
9] and should be performed before beginning a time-consuming and expensive therapy, such as subcutaneous or sublingual immunotherapy, in cases with indistinct history and unclear results in the above-mentioned methods.
Objective
In this study, we wanted to evaluate the correlation of SPT, intradermal testing and specific serum IgE testing in certain allergens. The intention was to evaluate sensitization rates, symptom patterns and time of symptoms in a cohort of patients (from a midwestern German academic hospital) with suspected allergic rhinitis. Furthermore, we wanted to evaluate whether patients’ complaints correlate with the results of SPT.
2. Materials and Methods
This study was performed in the Department of Otorhinolaryngology, Head and Neck Surgery of the University Medical Center Mainz, Germany. The study was carried out in accordance with the ethical standards established in the Declaration of Helsinki. Patients signed a “Broad consent” at admission which includes using their data and results of diagnostic tests or biomaterials for research as long as they were gathered during clinical routine as designated by the local ethics committee.
The database evaluated comprises 4653 patients with suspected allergic rhinitis who visited the allergy clinic between 1997 and 2010. Patient ages ranged from 0 to 88 years.
Patients were asked to fill in a standardized questionnaire according to Schultze-Werninghaus. This included history of allergic diseases, affected relatives, questions concerning professional environment and living quarters, animal contact, food and drug allergies. To further specify their symptoms, patients were asked about seasonality and duration of asthma, coughs, rhinorrhea, sneezing, nasal obstruction, eye symptoms such as tearing or itching, urticaria, swelling or itching of the mouth, tongue or pharynx, atopic eczema, gastrointestinal symptoms and sense of smell [
10]. Further evaluation to assess severity or more closely define certain symptoms was not used.
Allergic rhinitis was diagnosed using patient history, SPT and/or intradermal testing and in vitro testing of patients’ sera for specific compound IgE antibodies. SPT was used as a screening tool in patients with suspected allergic rhinitis with a standard array of allergens (birch, alder, hazel, beech, rye, grass mix, ribwort, mugwort, Alternaria alternate, Cladosporium herbarum, Aspergillus fumigatus, Fusarium roseum, Penicillium notatum, Botrytis cinerea, cat, dog, Dermatophagoides pteronyssinus and Dermatophagoides farinae; ALK Prick SQ 100 SQ-E/mL, ALK-Abelló, Wedel, Germany). Intradermal testing was used in patients with a suspected allergy and negative results in SPT and for all patients with a suspected mite and mold allergy (Allergopharma, Reinbek, Germany). Histamine served as a positive control and saline solution as a negative control. After 20 min, reactions in the SPT and intradermal test were recorded in four degrees of severity according to wheal size (0 for negative; 1 for a wheal of up to 3 mm; 2 for a wheal of 3 mm to 5 mm and 3 for a wheal of more than 5 mm). For evaluation of data, a score of greater than/equal to 1 was deemed to be a positive result.
For in vitro testing, which was performed to confirm the result of a positive SPT or intradermal testing in all patients, standard specific serum IgE determination was used (ImmunoCAP, Thermo Fisher Scientific). The measured units were divided into seven groups from 0 to VI as designated by the manufacturer. CAP-classes of ≥ II were considered positive. For polysensitized patients test results were included in the calculation for each category.
Statistics
A standard desktop PC with SPSS 23 software was used for the statistical evaluation. In this explorative analysis, values of p = 0.05 were regarded as significant. Mean values of standard deviation were chosen for graphical representation of the results.
For statistical analysis, all patients were divided into five groups. Group one (termed “spring bloomer”) consisted of patients allergic to birch, hazel, alder or beech; group two (termed “summer bloomer”) consisted of patients allergic to rye or grasses; group three (termed “autumn bloomer”) consisted of patients allergic to ribwort and mugwort; group four (termed “mites”) consisted of patients allergic to Dermatophagoides pteronyssinus or farina; and group five (termed “mold”) consisted of patients allergic to Alternaria alternata, Aspergillus fumigatus, Cladosporium herbarum, Fusarium roseum, Penicillium notatum or Botrytis cinerea. If patients were sensitized to more than one allergen they were included in every group they were positive for. Symptoms and their seasonality from the questionnaire were given binominal scores.
To evaluate the concordance of SPT, intradermal test and specific IgE test results, Cohen’s kappa was used. For the assessment of kappa, the classification proposed by Landis and Koch [
11] was used.
For evaluation of the data, two consecutive CAP-classes were taken together so that four classes resulted (0 ≙ ≤ 0.35 KU/L, 1 ≙ 0.36 to 3.49 KU/L, 2 ≙ 3.50 to 52.49 KU/L, 3 ≙ ≥52.50 KU/L).
For evaluation of the probability of symptoms, univariate and multivariate logistic regression were performed leading to adjusted odds ratios. Additionally, for evaluation of the point-in-time symptoms reported by patients, logistic regression was performed. Representations of the results of logistic regression were generated at
https://www.statstodo.com (accessed on 24 April 2020) using a logarithmic scale.
3. Results
3.1. Epidemiology
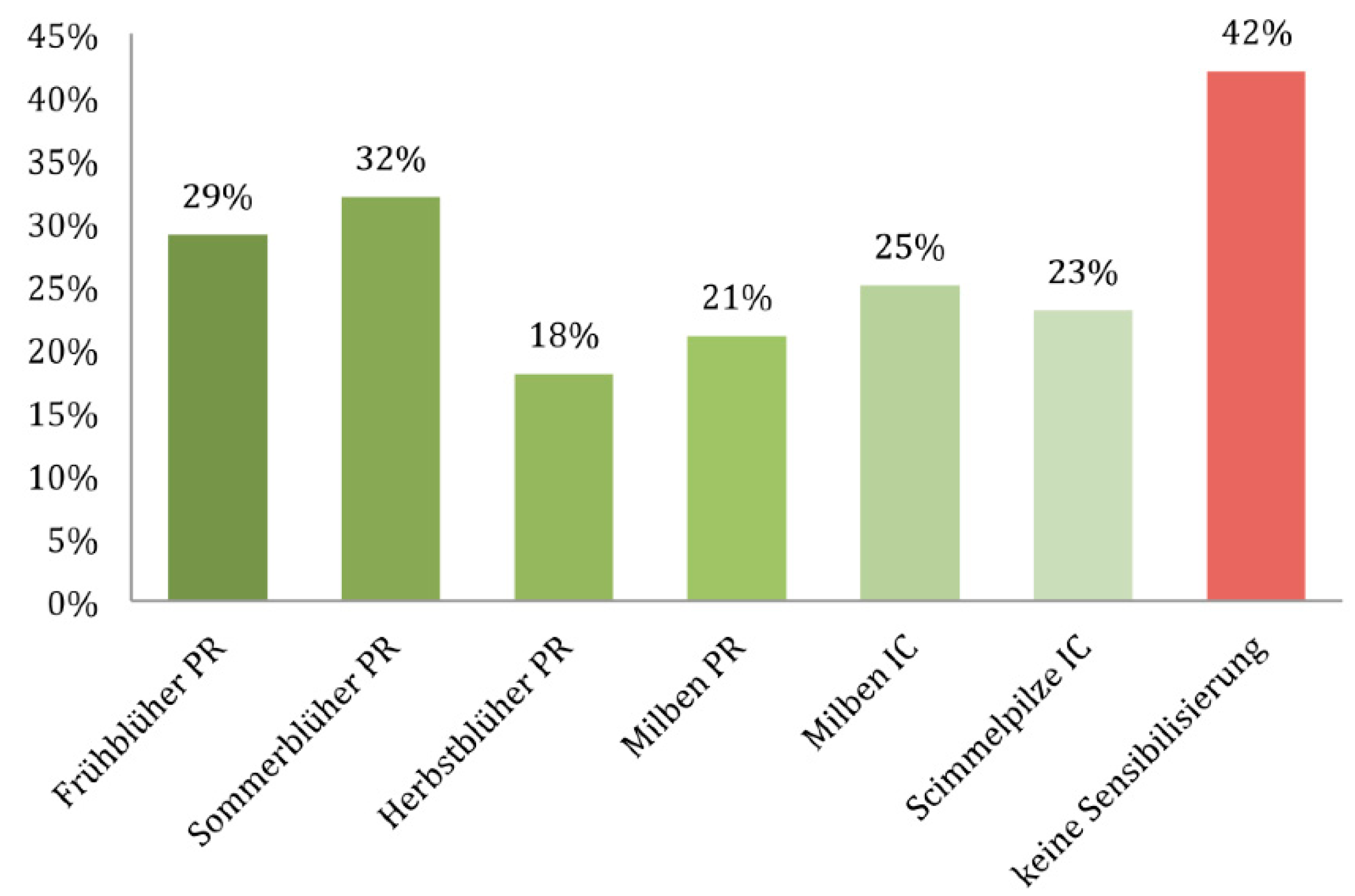
Of the 4653 subjects, 2699 (58%) were sensitized and were divided into the five groups already mentioned (“spring bloomer”, “summer bloomer”, “autumn bloomer”, “mites” and “mold”); 1954 subjects (42%) showed no sensitization (
Figure 1).
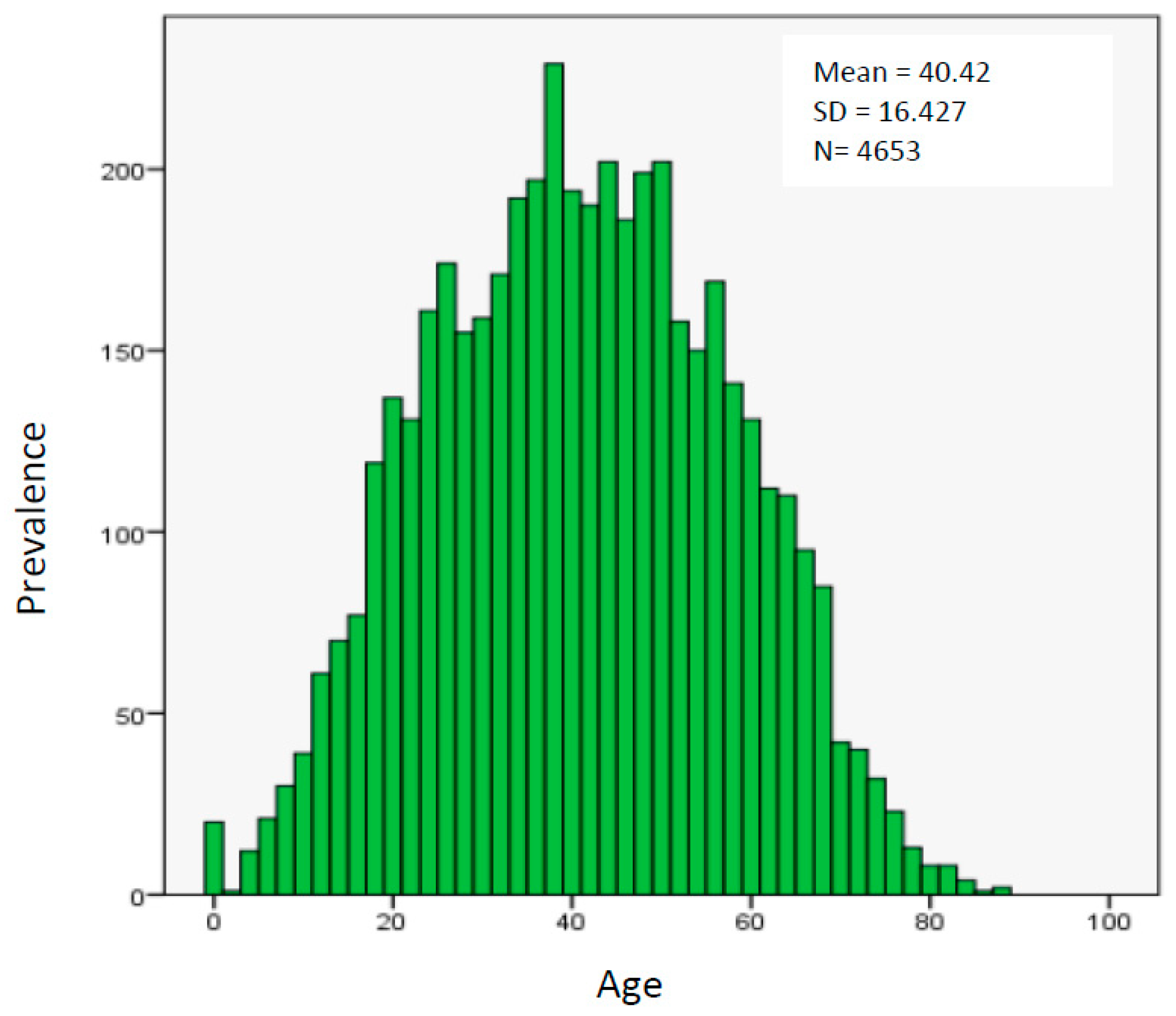
The age distribution of patients showed an almost standard distribution with half aged 28 to 53 years, 25% aged younger than 28 years and 25% aged older than 53 years. Median age was 40.42 years (
Figure 2).
3.2. Spring Bloomer
This group included patients sensitized to birch, hazel, alder or beech. The median age of these patients was 38 years. Patients aged 21 to 40 years constituted the biggest group (44%) followed by patients aged 41 to 60 years (36%). Of these patients, 9.9% were monosensitized. and 90.1% were polysensitized.
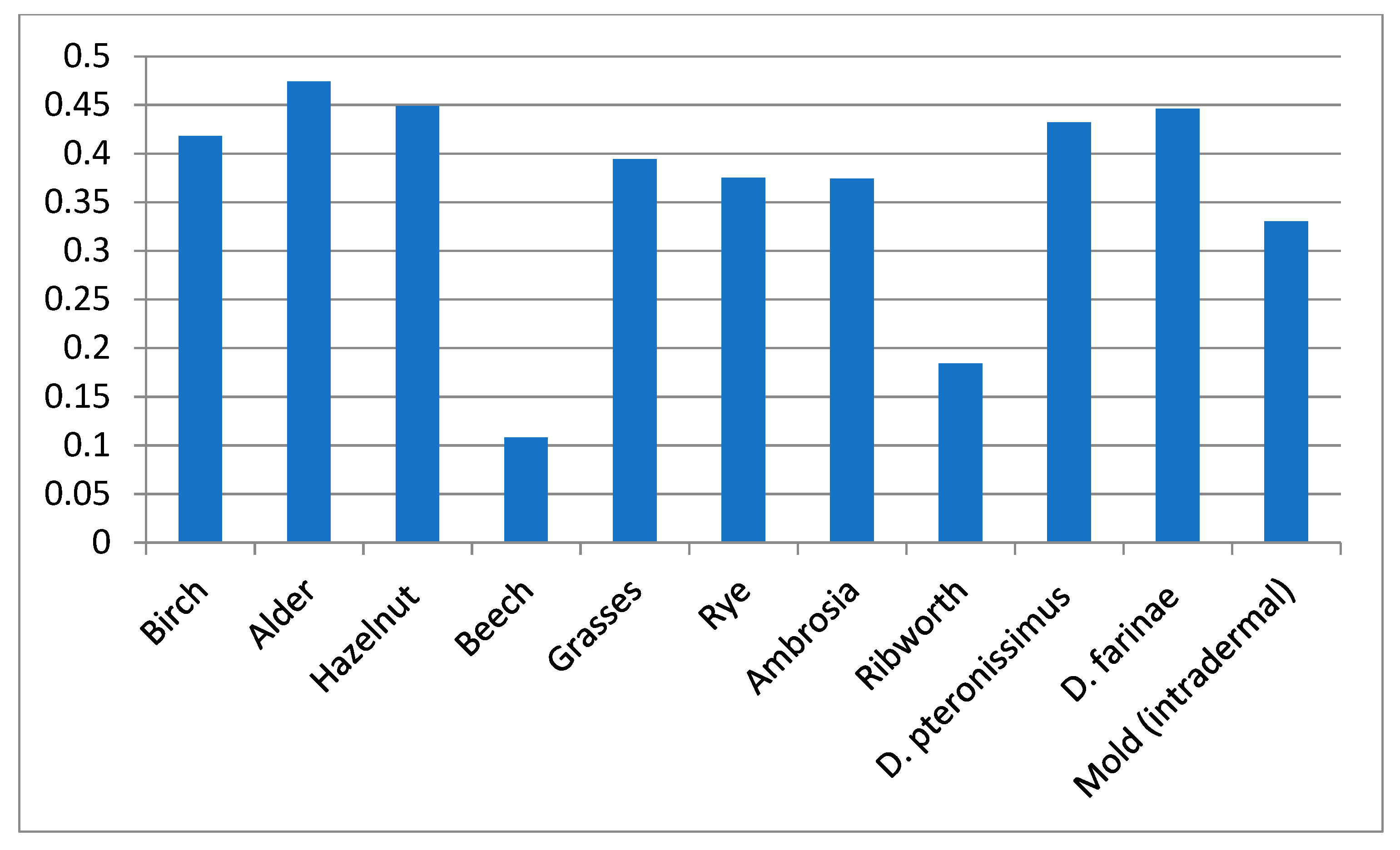
Comparison of SPT and specific serum IgE in these patients led to a moderate concordance according to Landis and Koch, with a kappa coefficient of 0.418 for birch, 0.474 for alder and 0.449 for hazelnut (
p < 0.0001 for all). For beech, no concordance could be found (kappa coefficient = 0.108), probably due to too small a number of subjects (
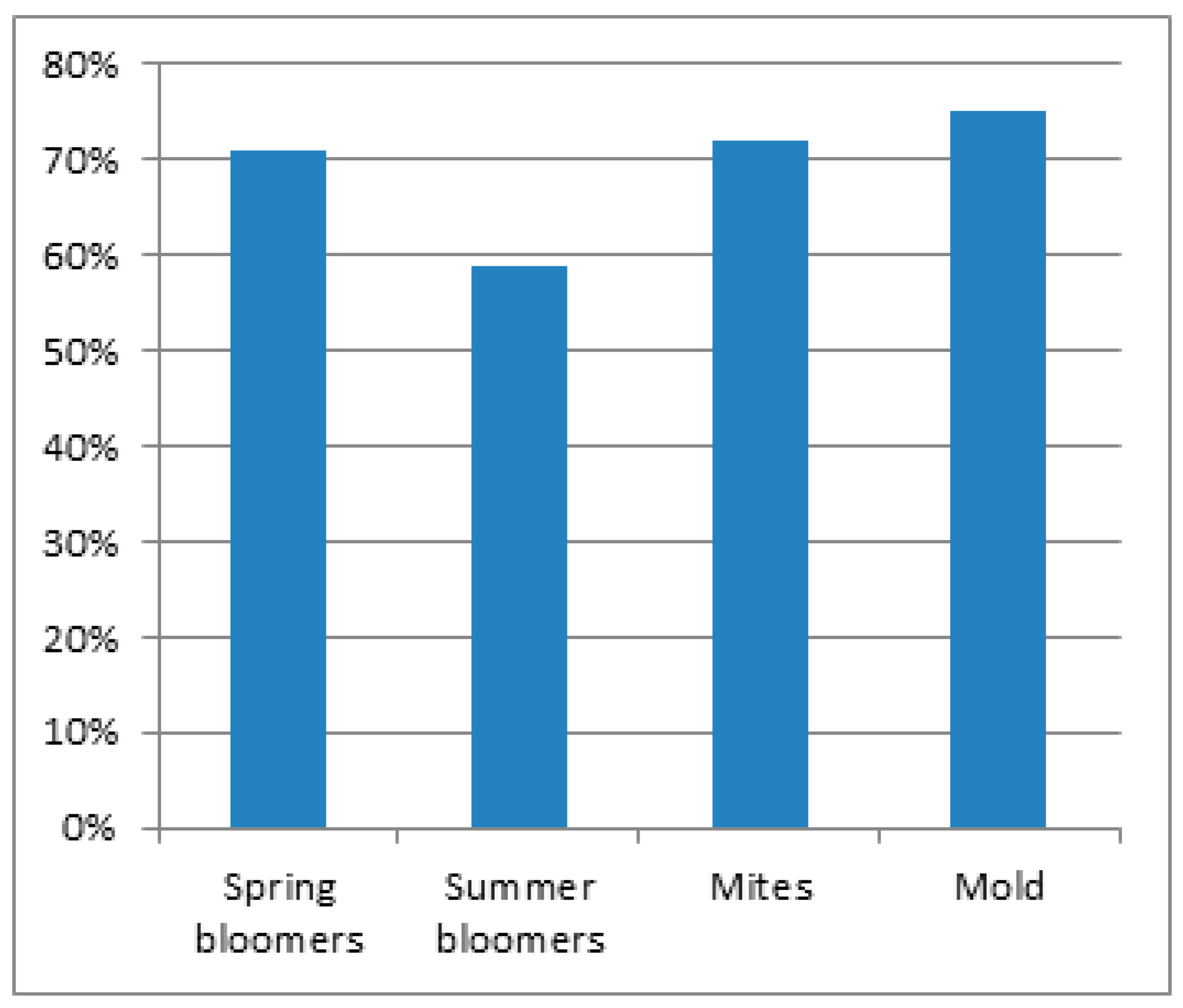
Figure 3). For spring bloomers, this means an overall concordance of 71% for both test methods (
Figure 4).
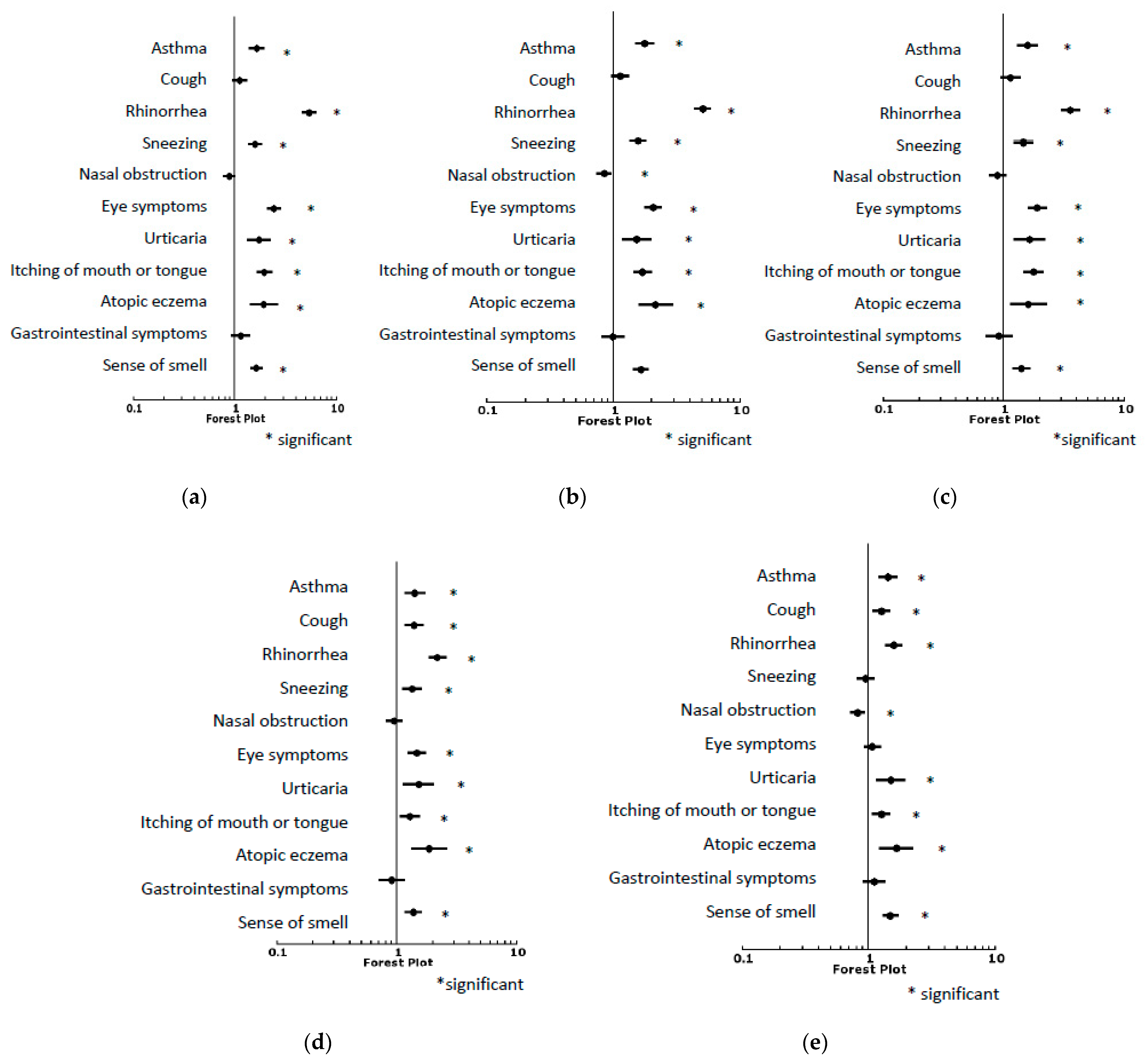
When looking at specific symptoms reported by patients sensitized to spring bloomers, data on 3815 subjects could be evaluated. The probability of rhinorrhea was highest, followed by other symptoms such as asthma, atopic eczema, sense of smell and urticaria. Nasal obstruction and coughing did not have a significantly higher probability in subjects sensitized to spring bloomers, as compared to nonsensitized subjects (
Figure 5a,
Table 1).
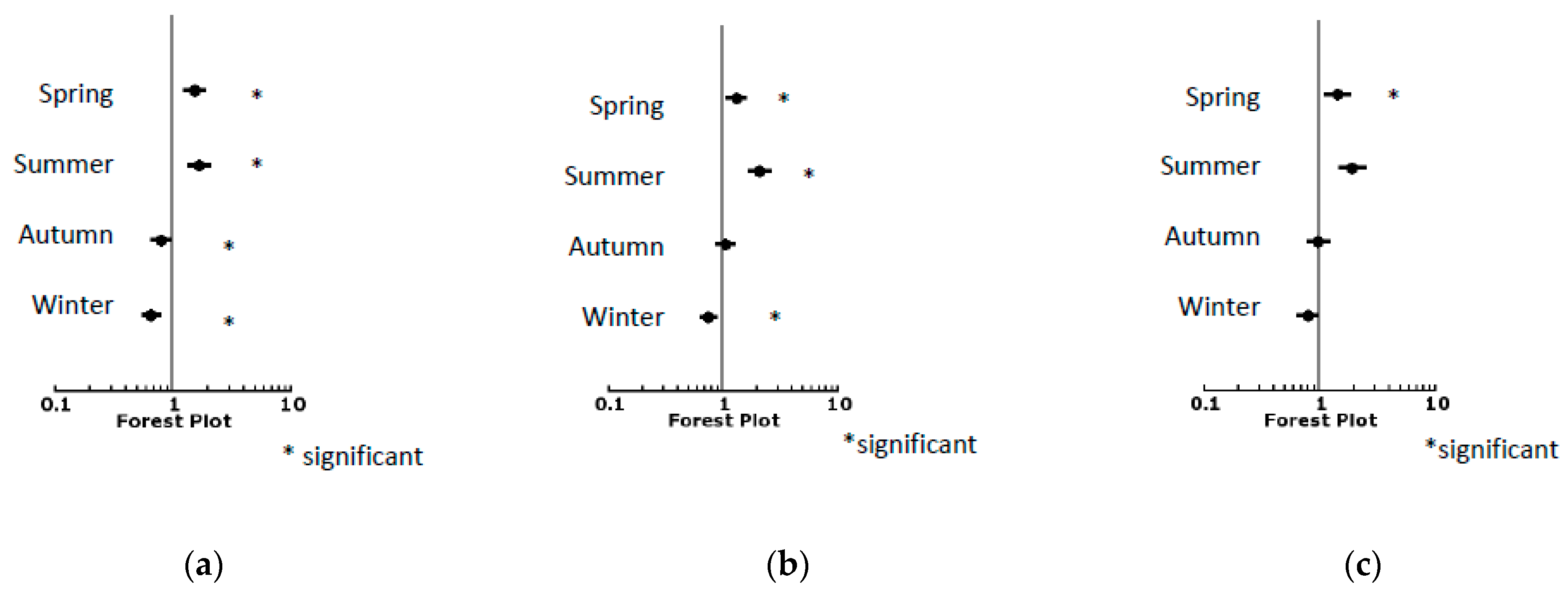
When looking at the time period of symptoms, patients sensitized to spring bloomers had a higher probability of symptoms in spring and summer, and a lower probability in autumn and winter, compared to nonsensitized subjects (
Figure 6a,
Table 1).
To evaluate whether symptom seasonality reported by patients matched their sensitization pattern, a correlation was performed. This shows that patients sensitized to spring bloomers reported symptoms in spring, with a sensitivity of 30.8% and a specificity of 77% (p < 0.0001). The odds ratio was 1.5, which shows that patients who reported symptoms in spring were sensitized 1.5 times more often.
Figure 3.
Kappa coefficients when comparing SPT and specific serum IgE.
Figure 3.
Kappa coefficients when comparing SPT and specific serum IgE.
Figure 4.
Overall concordance of SPT (intradermal test for mold) and specific serum IgE.
Figure 4.
Overall concordance of SPT (intradermal test for mold) and specific serum IgE.
Figure 5.
(a–e) Correlation of symptoms. (a) Symptoms associated with spring bloomers; (b) Symptoms associated with summer bloomers; (c) Symptoms associated with autumn bloomers; (d) Symptoms associated with mites; (e) Symptoms associated with mold.
Figure 5.
(a–e) Correlation of symptoms. (a) Symptoms associated with spring bloomers; (b) Symptoms associated with summer bloomers; (c) Symptoms associated with autumn bloomers; (d) Symptoms associated with mites; (e) Symptoms associated with mold.
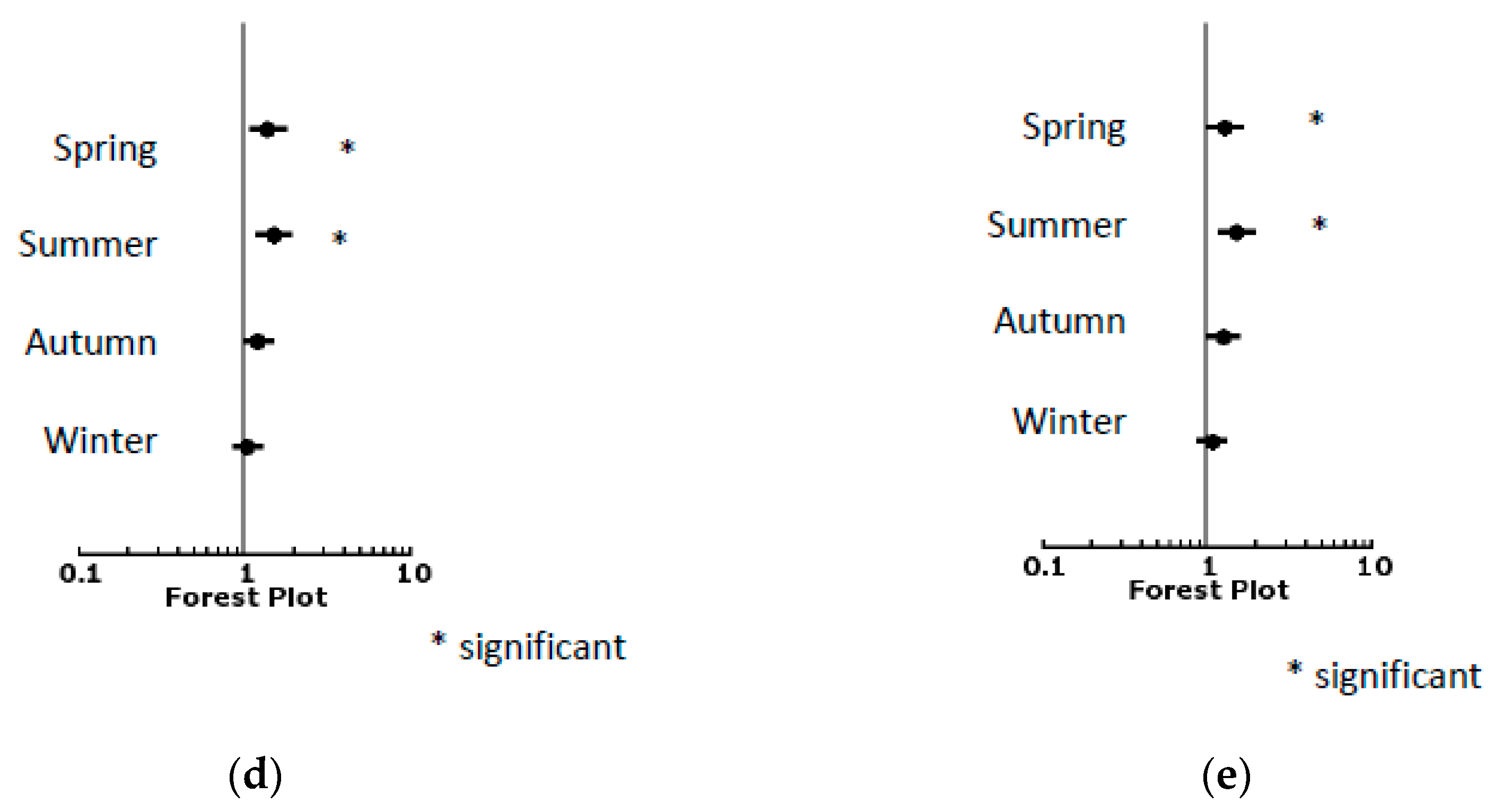
Figure 6.
(a–e) Point in time of symptoms. (a) Time of symptoms associated with spring bloomers; (b) Time of symptoms associated with summer bloomers; (c) Time of symptoms associated with autumn bloomers; (d) Time of symptoms associated with mites; (e) Time of symptoms associated with mold.
Figure 6.
(a–e) Point in time of symptoms. (a) Time of symptoms associated with spring bloomers; (b) Time of symptoms associated with summer bloomers; (c) Time of symptoms associated with autumn bloomers; (d) Time of symptoms associated with mites; (e) Time of symptoms associated with mold.
3.3. Summer Bloomer
Patients sensitized to rye or grasses were included in this group. The median age of these patients was 35 years. The biggest group (49% of patients) comprised those aged 21 to 40 years, followed by patients aged 41 to 60 years (31%). Of these patients, 12.2% were monosensitized, and 87.8% were polysensitized.
In this group, a minor concordance was found when comparing SPT and specific serum IgE with a kappa coefficient of 0.394 (
p < 0.0001) for grasses and 0.375 (
p < 0.0001) for rye (
Figure 3). The accordance of both tests was 59% in this group (
Figure 4).
When looking at specific symptoms reported by patients sensitized to summer bloomers, data on 3815 subjects could be evaluated. The probability of being symptomatic was highest for rhinorrhea, whilst other symptoms such as atopic eczema, eye symptoms, asthma and sense of smell followed. Here again, coughing and gastrointestinal symptoms did not have a significantly higher probability in persons sensitized to summer bloomers as compared to nonsensitized persons, and nasal obstruction was associated with a lower probability in sensitized subjects (
Figure 5b,
Table 2).
Patients sensitized to summer bloomers had a higher probability of symptoms in spring and summer, and a lower probability in winter, compared to nonsensitized persons. In autumn, no significant difference could be found between the groups (
Figure 6b,
Table 2).
To evaluate whether the reported symptom seasonality of patients matched their sensitization patterns, a correlation was again performed. This shows that patients sensitized to summer bloomers reported symptoms in summer, with a sensitivity of 35% and a specificity of 80% (p < 0.0001). The odds ratio shows that patients who reported symptoms in summer were sensitized 2.1 times more often.
3.4. Autumn Bloomer
This group included patients sensitized to ribwort and mugwort. The median age of these patients was 38 years. The largest group comprised patients aged 21 to 40 years (45%), followed by patients aged 41 to 60 years (37%). Only 8.7% of these patients were monosensitized, and 91.3% were polysensitized.
Comparison of the skin prick test and specific serum IgE showed a kappa coefficient of 0.374 (
p < 0.0001) for mugwort (
Figure 3). For ribwort, no concordance could be found (kappa coefficient = 0.184), probably due to an insufficient number of analyzed subjects.
Looking at specific symptoms reported by patients sensitized to autumn bloomers, data of 3808 persons could be evaluated. Rhinorrhea was the most frequent symptom, followed by other symptoms such as eye symptoms, itching of the mouth or pharynx, atopic eczema and urticaria. Here, again, nasal obstruction and coughing did not have a significantly higher probability in patients sensitized to autumn bloomers, as compared to nonsensitized subjects (
Figure 5c,
Table 3).
Patients sensitized to autumn bloomers were most likely to be symptomatic in spring and summer. In winter, they were less likely to have problems than nonsensitized persons. Interestingly, in autumn itself, no significant difference could be found when comparing sensitized to nonsensitized subjects (
Figure 6c,
Table 3).
3.5. Mites
In this group, patients sensitized to Dermatophagoides pteronyssinus or Dermatophagoides farinae were included. These patients had a median age of 36 years, with patients aged 21 to 40 years representing the biggest group (49%). Patients aged 41 to 60 years represented 29%. In 22.4% of cases, patients were monosensitized, whereas 77.6% were polysensitized.
For mites, a moderate correlation was found between SPT and specific IgE, with a kappa coefficient of 0.432 (
p < 0.0001) for Dermatophagoides pteronyssinus and 0.446 (
p < 0.0001) for Dermatophagoides farina, which amounts to a concordance of 72% (
Figure 3 and
Figure 4).
In this group, comparison of the results of SPT and intradermal testing was possible with 3405 subjects. For D. pteronyssinus, the kappa coefficient was 0.642—a significant concordance according to Landis and Koch. For D. farina, the kappa coefficient showed a moderate concordance, with a value of 0.585. p-values were 0.0001. The concordance of both tests was 87%.
Evaluation of specific symptoms in sensitized patients was possible for 3652 persons. For mite-sensitized patients, again, the probability of rhinorrhea was highest, followed by other symptoms such as atopic eczema, urticaria, eye symptoms and asthma following. As with the other groups, nasal obstruction did not have a higher probability in mite-sensitized as compared to nonsensitized subjects (
Figure 5d,
Table 4).
A difference in the times when symptoms were present could be seen in spring and in summer (
Figure 6d,
Table 4).
3.6. Mold
This group included patients sensitized to Alternaria alternata, Aspergillus fumigatus, Cladosporium herbarum, Fusarium roseum, Penicillium notatum or Botrytis cinerea. The median age of these patients was 38 years, with patients aged 21 to 40 years representing the biggest group (43%), followed by patients aged 41 to 60 years (34%). Precisely 34.4% of patients were monosensitized, whereas 65.6% were polysensitized.
Comparison of intradermal testing and specific serum IgE was possible in a total of 1462 patients sensitized to Alternaria alternata. A low concordance was found with a kappa coefficient of 0.330 (
p < 0.0001) and accordance for both tests of 75% (
Figure 3 and
Figure 4).
Specific symptoms in sensitized patients could be evaluated in 3738 subjects. The probability of symptoms of atopic eczema was highest, followed by symptoms of rhinorrhea, urticaria and asthma. Additionally, for mold-sensitized persons, nasal obstruction did not have a significantly higher probability as compared to nonsensitized persons (
Figure 5e,
Table 5).
Subjects sensitized to mold had a higher probability of symptoms in spring and summer as with mites (
Figure 6e,
Table 5).
4. Discussion
This study conducted an explorative analysis, comparing different methods of allergological testing in a large cohort of patients from midwestern Germany. The advantage of this study is the large number of patients tested for allergic rhinitis, which provides consistent testing results of skin tests and specific serum IgE, together with data on symptom duration and questionnaire responses.
These data found overall sensitization rates to be in line with previously published results [
7,
12,
13,
14,
15]. Findings confirm that patients with allergies to inhalant allergens in spring (early bloomers such as birch) and autumn (herbs) have the highest polysensitization rates of around 90%, which is a little higher than previously reported [
15,
16,
17], whereas monosensitizations are higher in house dust mites and mold.
Comparison of SPT and the results of specific serum IgE testing show a moderate correlation for birch, alder, hazelnut and mites, and only a minor correlation for grasses, rye and mugwort. For mites, Chinoy et al. [
4] found a lower concordance of 58.5%, but this might be explained by the use of a Phadebas RAST system, which has a lower sensitivity [
18]. Tang and Wu [
6] and van der Zee [
7] describe a strong concordance of 97% and 93% between intradermal testing and specific IgE testing for mites. As with the above-mentioned studies, SPT in this investigation was more sensitive in detecting sensitization than specific serum IgE testing and shows that additional testing of specific IgE does not necessarily lead to more diagnostic input or a more reliable diagnosis. Pastorello et al. [
19], on the other hand, found a lower diagnostic value (sum of sensitivity and specificity) for the SPT than for specific IgE testing.
When comparing intradermal testing and specific IgE testing, which was regularly performed in Alternaria alternate, similar results were found with only a moderate correlation and a concordance of 75%. For all allergens, the concordance for negative results was good so that none of the tests missed a significant number of patients with an allergy, but for positive results, the prick test had a tendency to show sensitization earlier than the specific serum IgE.
The comparison of intradermal testing and SPT revealed a significant correlation for sensitization to mites. In other studies comparing these methods, percutaneous testing correlated better [
20].
When comparing symptoms reported by patients with a sensitization diagnosed by SPT, a correlation was only found for spring and summer bloomers. The odds ratio for spring bloomers was 1.5 and for summer bloomers 2.1, showing that patients’ history can give a clue to relevant allergens in these seasonal allergies. On the other hand, only 31% of patients who reported allergic symptoms in spring had a sensitization to spring bloomers. This is less than previously reported when comparing patients with allergic rhinitis versus nonallergic rhinitis [
21,
22]. Part of this difference in numbers might be explained by the polysensitization of patients to further seasonal or perennial allergens. Additionally, questionnaires evaluating patient symptoms in allergic rhinitis always have difficulties differentiating between allergic and nonallergic rhinitis, as can be seen in the SAPALDIA study [
23]. For mite and autumn allergies, no correlation could be found between reported symptoms and allergic rhinitis. This shows that testing only patients with clear symptoms leads to undertreatment, especially in patients with mite allergies, and that more uncommon symptoms and findings need to be evaluated for an underlying allergic disease. One additional reason for false-negative test results could be a possible missing of detecting late reaction after IDT [
24].
Interestingly, when looking at specific symptoms, the data in this study suggest that nasal obstruction is a symptom that is not associated with sensitization, as there was no difference between sensitized and nonsensitized persons in all groups. This also seems to be true for patients with mite sensitization and contrasts with other publications [
25,
26,
27,
28,
29]. There may be a certain bias in the acquired data concerning this specific symptom because this study only included patients presenting to an ENT clinic. This might lead to a nonsensitized control group in which patients with nasal complaints, especially nasal obstruction, are overrepresented.
The symptom patients reported most frequently was rhinorrhea. Other symptoms such as eye symptoms, atopic eczema and impairment of sense of smell followed. Symptoms of asthma were most prevalent in patients sensitized to grasses or rye, and symptoms of atopic eczema were most prevalent in patients sensitized to mold. Analysis of the time of year when patients were symptomatic found that all sensitized patients, regardless of the type of sensitization, had a higher probability of symptoms in spring and summer. In wintertime, sensitization to spring and summer bloomers seems to have a protective effect, with sensitized patients having a lower probability of symptoms than nonsensitized persons. This was even similar for mite-sensitized patients who did not differ in their probability of symptoms in autumn or winter from nonsensitized persons.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}