Higher PD-L1 Immunohistochemical Detection Signal in Frozen Compared to Matched Paraffin-Embedded Formalin-Fixed Tissues

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Consenting
2.2. Tissue Fixation and Embedding
2.3. Antibodies
2.4. Immunohistochemistry (IHC)
2.4.1. IHC on Sections of FR Tissues
2.4.2. IHC in Sections of FFPE Tissues
2.5. Pathology Scoring
2.6. Statistical Analysis
3. Results
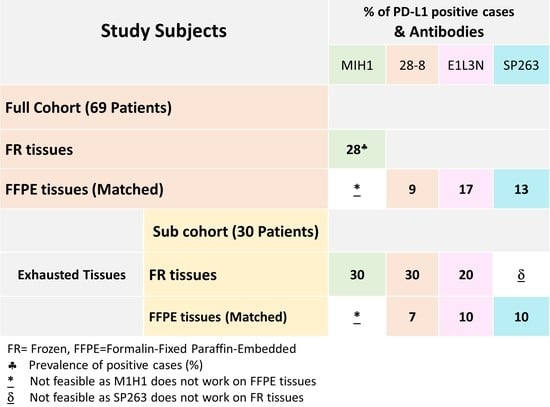
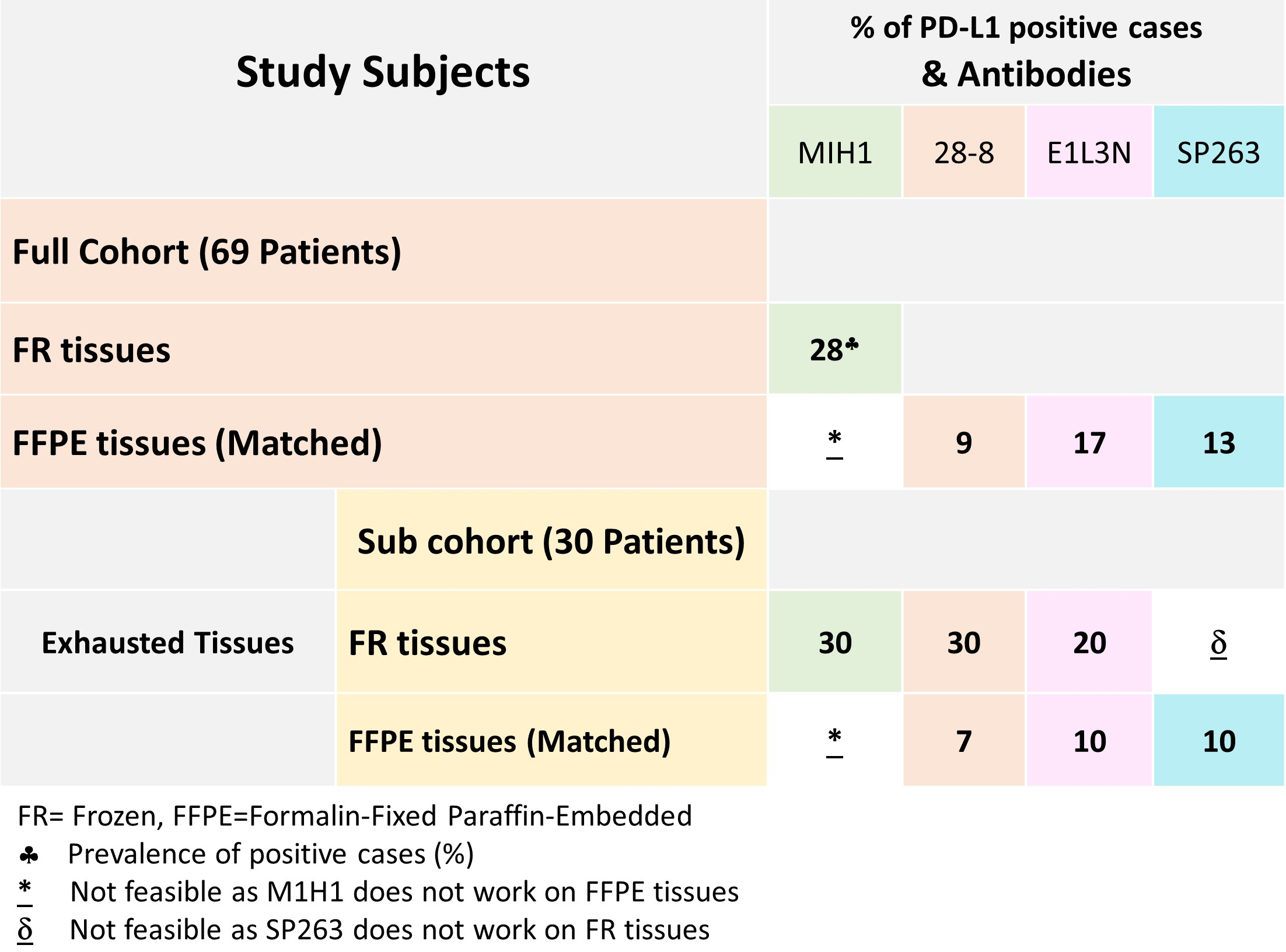
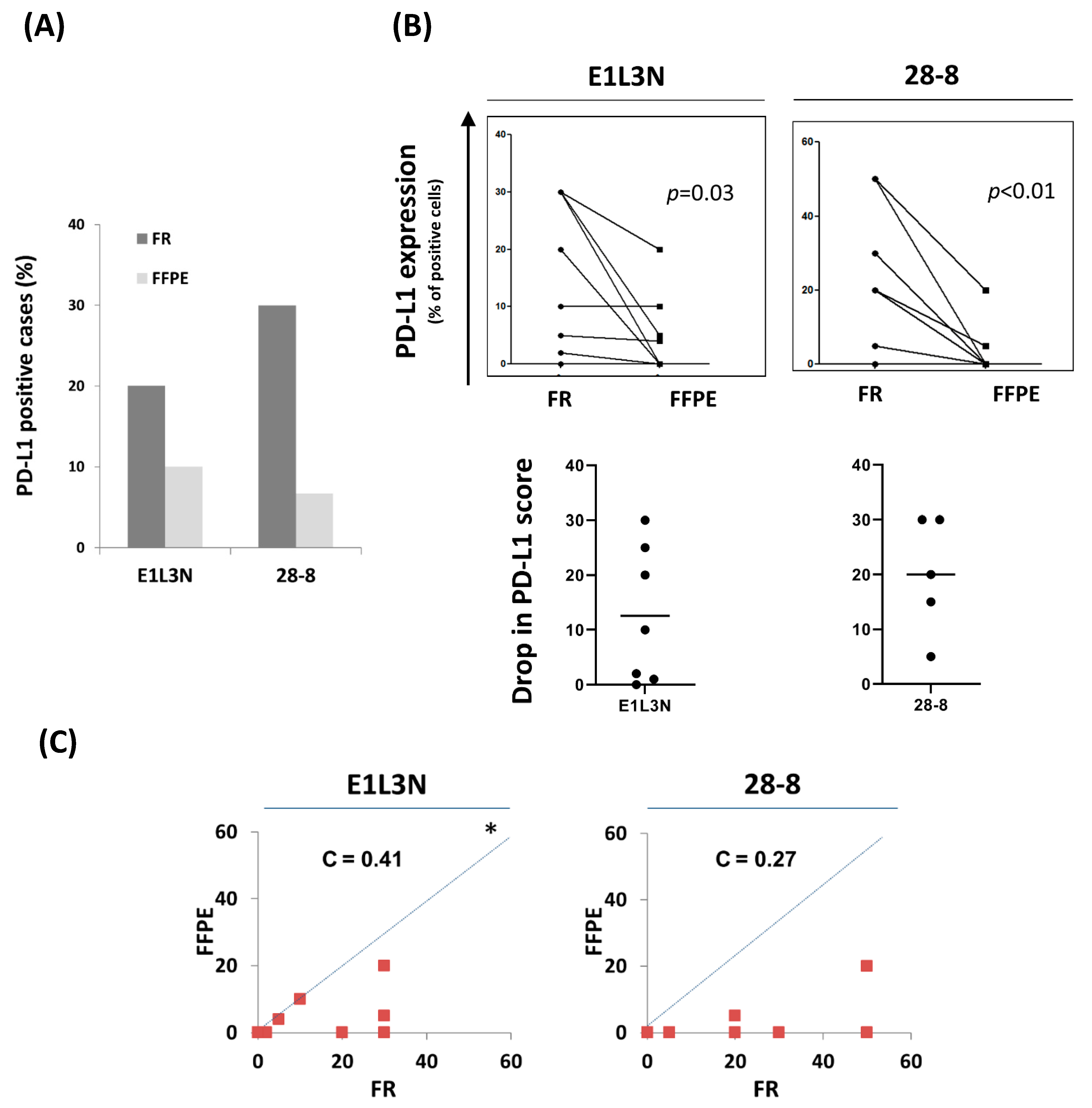
3.1. Lower Prevalence of PD-L1 Positive Tumors in FFPE Compared to FR Tissues
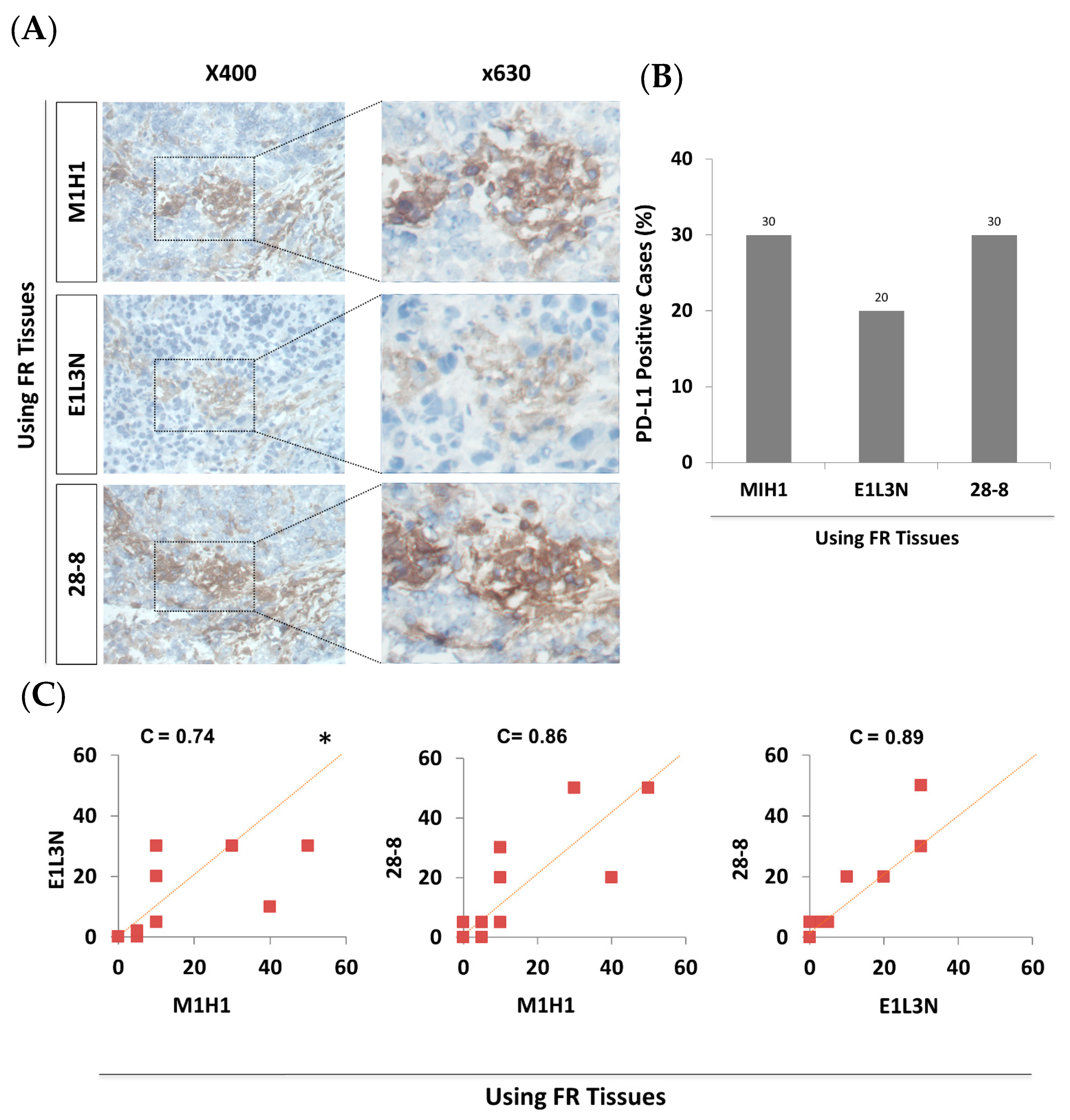
3.2. PD-L1 Score and Prevalence of PD-L1 Positive Cases in FR Tissues Were Comparable within All Tested Antibodies
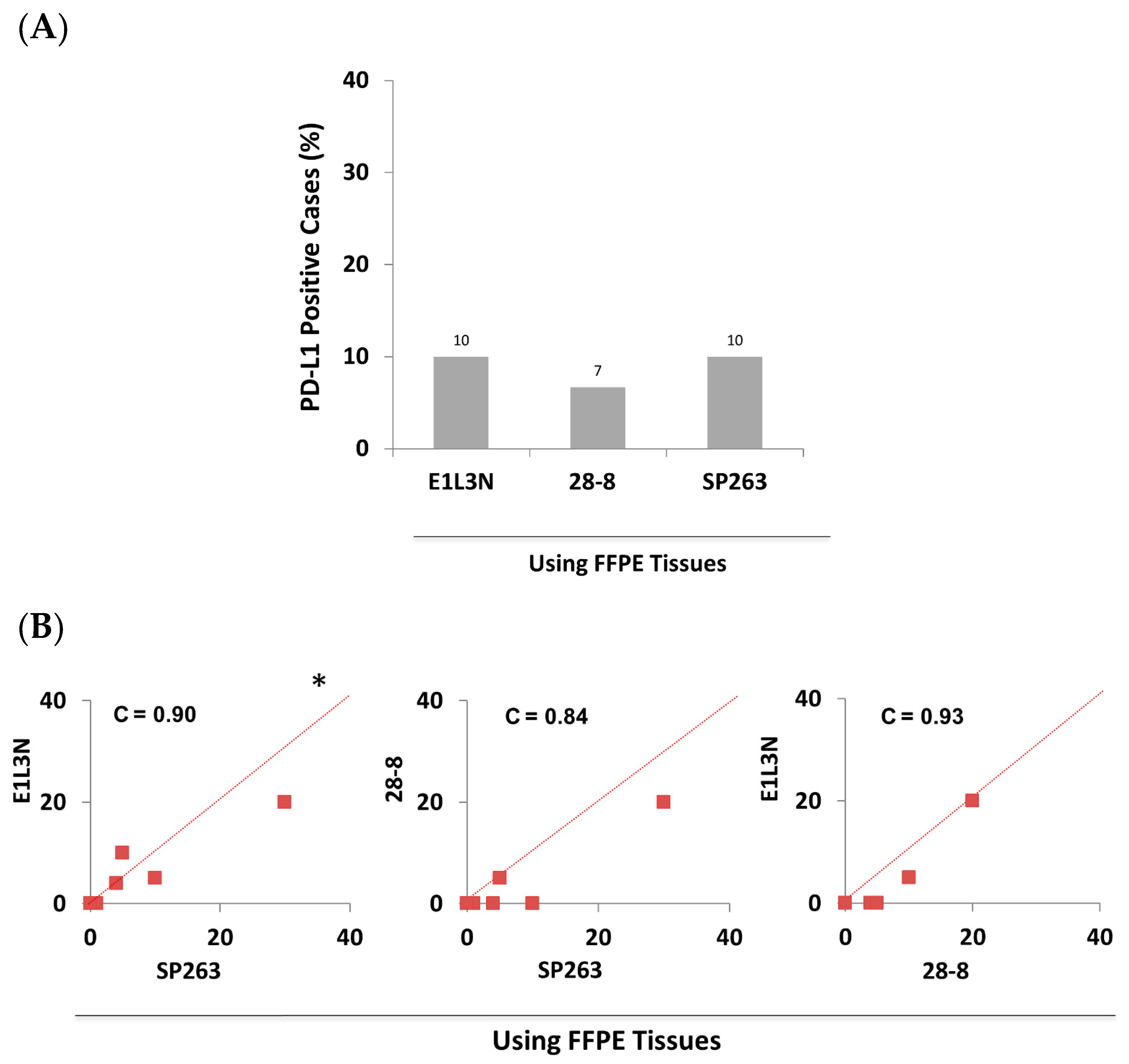
3.3. PD-L1 Score and Prevalence of PD-L1 Positive Cases in FFPE Tissues Were Comparable within All Tested Antibodies
3.4. The Drop in Prevalence of PD-L1 Positivity and Its Score in FFPE Tissues Compared to FR Tissues Is Consistent within All Tested Antibodies
3.5. The Decrease in Sensitivity of Anti-PD-L1 Antibodies in FFPE Tissues Is Predominantly due to the Preservation Method
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PD-L1 | programmed death ligand-1 |
| FR | Frozen |
| FFPE | Formalin-Fixed Paraffin-Embedded |
| IHC | Immunohistochemistry |
| C | Lin’s concordance correlation coefficient |
References
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef]
- Afreen, S.; Dermime, S. The immunoinhibitory B7-H1 molecule as a potential target in cancer: Killing many birds with one stone. Hematol. /Oncol. Stem Cell Ther. 2014, 7, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homet Moreno, B.; Ribas, A. Anti-programmed cell death protein-1/ligand-1 therapy in different cancers. Br. J. Cancer 2015, 112, 1421–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.P.; Kurzrock, R. PD-L1 Expression as a Predictive Biomarker in Cancer Immunotherapy. Mol Cancer 2015, 14, 847–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Dieras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Ghebeh, H.; Mohammed, S.; Al-Omair, A.; Qattan, A.; Lehe, C.; Al-Qudaihi, G.; Elkum, N.; Alshabanah, M.; Bin Amer, S.; Tulbah, A.; et al. The B7-H1 (PD-L1) T lymphocyte-inhibitory molecule is expressed in breast cancer patients with infiltrating ductal carcinoma: Correlation with important high-risk prognostic factors. Neoplasia 2006, 8, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Ghebeh, H.; Tulbah, A.; Mohammed, S.; Elkum, N.; Bin Amer, S.M.; Al-Tweigeri, T.; Dermime, S. Expression of B7-H1 in breast cancer patients is strongly associated with high proliferative Ki-67-expressing tumor cells. Int. J. Cancer 2007, 121, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Philips, A.V.; Meric-Bernstam, F.; Qiao, N.; Wu, Y.; Harrington, S.; Su, X.; Wang, Y.; Gonzalez-Angulo, A.M.; Akcakanat, A.; et al. PD-L1 expression in triple-negative breast cancer. Cancer Immunol. Res. 2014, 2, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Muenst, S.; Schaerli, A.R.; Gao, F.; Daster, S.; Trella, E.; Droeser, R.A.; Muraro, M.G.; Zajac, P.; Zanetti, R.; Gillanders, W.E.; et al. Expression of programmed death ligand 1 (PD-L1) is associated with poor prognosis in human breast cancer. Breast Cancer Res. Treat. 2014, 146, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, T.; Zeng, Y.D.; Qin, G.; Xu, F.; Lu, J.B.; Fang, W.F.; Xue, C.; Zhan, J.H.; Zhang, X.K.; Zheng, Q.F.; et al. High PD-L1 expression was associated with poor prognosis in 870 Chinese patients with breast cancer. Oncotarget 2015, 6, 33972–33981. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.R.; Glont, S.E.; Blows, F.M.; Provenzano, E.; Dawson, S.J.; Liu, B.; Hiller, L.; Dunn, J.; Poole, C.J.; Bowden, S.; et al. PD-L1 protein expression in breast cancer is rare, enriched in basal-like tumours and associated with infiltrating lymphocytes. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. / Esmo 2015, 26, 1488–1493. [Google Scholar] [CrossRef] [PubMed]
- Karnik, T.; Kimler, B.F.; Fan, F.; Tawfik, O. PD-L1 in Breast Cancer: Comparative Analysis of Three Different Antibodies. Hum. Pathol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.Y.; Lee, Y.K.; Koo, J.S. Expression of PD-L1 in triple-negative breast cancer based on different immunohistochemical antibodies. J. Transl. Med. 2016, 14, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghebeh, H.; Barhoush, E.; Tulbah, A.; Elkum, N.; Al-Tweigeri, T.; Dermime, S. FOXP3+ Tregs and B7-H1+/PD-1+ T lymphocytes co-infiltrate the tumor tissues of high-risk breast cancer patients: Implication for immunotherapy. BMC Cancer 2008, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, K.M.; Sun, H.; Liao, X.; Hua, P.; Callea, M.; Greenfield, E.A.; Hodi, F.S.; Sharpe, A.H.; Signoretti, S.; Rodig, S.J.; et al. PD-L1 Antibodies to Its Cytoplasmic Domain Most Clearly Delineate Cell Membranes in Immunohistochemical Staining of Tumor Cells. Cancer Immunol. Res. 2015, 3, 1308–1315. [Google Scholar] [CrossRef] [Green Version]
- Watson, P.F.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [Green Version]
- Buttner, R.; Gosney, J.R.; Skov, B.G.; Adam, J.; Motoi, N.; Bloom, K.J.; Dietel, M.; Longshore, J.W.; Lopez-Rios, F.; Penault-Llorca, F.; et al. Programmed Death-Ligand 1 Immunohistochemistry Testing: A Review of Analytical Assays and Clinical Implementation in Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2017, 35, 3867–3876. [Google Scholar] [CrossRef]
- Mansfield, A.S.; Aubry, M.C.; Moser, J.C.; Harrington, S.M.; Dronca, R.S.; Park, S.S.; Dong, H. Temporal and spatial discordance of programmed cell death-ligand 1 expression and lymphocyte tumor infiltration between paired primary lesions and brain metastases in lung cancer. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. / Esmo 2016, 27, 1953–1958. [Google Scholar] [CrossRef]
- Eckstein, M.; Cimadamore, A.; Hartmann, A.; Lopez-Beltran, A.; Cheng, L.; Scarpelli, M.; Montironi, R.; Gevaert, T. PD-L1 assessment in urothelial carcinoma: A practical approach. Ann. Transl. Med. 2019, 7, 690. [Google Scholar] [CrossRef] [PubMed]
- Dapson, R.W. Macromolecular changes caused by formalin fixation and antigen retrieval. Biotech. Histochem. Off. Publ. Biol. Stain Comm. 2007, 82, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Namimatsu, S.; Ghazizadeh, M.; Sugisaki, Y. Reversing the effects of formalin fixation with citraconic anhydride and heat: A universal antigen retrieval method. J. Histochem. Cytochem. Off. J. Histochem. Soc. 2005, 53, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Bogen, S.A.; Vani, K.; Sompuram, S.R. Molecular mechanisms of antigen retrieval: Antigen retrieval reverses steric interference caused by formalin-induced cross-links. Biotech. Histochem. Off. Publ. Biol. Stain Comm. 2009, 84, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Sompuram, S.R.; Vani, K.; Hafer, L.J.; Bogen, S.A. Antibodies immunoreactive with formalin-fixed tissue antigens recognize linear protein epitopes. Am. J. Clin. Pathol. 2006, 125, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Sznol, M.; Chen, L. Antagonist antibodies to PD-1 and B7-H1 (PD-L1) in the treatment of advanced human cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2013, 19, 1021–1034. [Google Scholar] [CrossRef] [Green Version]
- Gadiot, J.; Hooijkaas, A.I.; Kaiser, A.D.; van Tinteren, H.; van Boven, H.; Blank, C. Overall survival and PD-L1 expression in metastasized malignant melanoma. Cancer 2011, 117, 2192–2201. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.H.; Kuntz, S.M.; Leibovich, B.C.; Dong, H.; Lohse, C.M.; Webster, W.S.; Sengupta, S.; Frank, I.; Parker, A.S.; Zincke, H.; et al. Tumor B7-H1 is associated with poor prognosis in renal cell carcinoma patients with long-term follow-up. Cancer Res. 2006, 66, 3381–3385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, M.S.; Kerr, K.M.; Kockx, M.; Beasley, M.B.; Borczuk, A.C.; Botling, J.; Bubendorf, L.; Chirieac, L.; Chen, G.; Chou, T.Y.; et al. PD-L1 Immunohistochemistry Comparability Study in Real-Life Clinical Samples: Results of Blueprint Phase 2 Project. J. Thorac. Oncol. 2018, 13, 1302–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Morilla, S.; McGuire, J.; Gaule, P.; Moore, L.; Acs, B.; Cougot, D.; Gown, A.M.; Yaziji, H.; Wang, W.L.; Cartun, R.W.; et al. Quantitative assessment of PD-L1 as an analyte in immunohistochemistry diagnostic assays using a standardized cell line tissue microarray. Lab Investig. 2020, 100, 4–15. [Google Scholar] [CrossRef]
- Lee, H.H.; Wang, Y.N.; Xia, W.; Chen, C.H.; Rau, K.M.; Ye, L.; Wei, Y.; Chou, C.K.; Wang, S.C.; Yan, M.; et al. Removal of N-Linked Glycosylation Enhances PD-L1 Detection and Predicts Anti-PD-1/PD-L1 Therapeutic Efficacy. Cancer Cell 2019, 36, 168–178. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Summary of Safety and Effectiveness Data (SSED) for Ventana PD-L1 (SP263) Assay. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160046B.pdf (accessed on 12 March 2020).
- U.S. Food and Drug Administration. Summary of Safety and Effectiveness Data (SSED) for Ventana PD-L1 (28-8) PharmDx. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150027b.pdf (accessed on 12 March 2020).
- Schalper, K.A.; Velcheti, V.; Carvajal, D.; Wimberly, H.; Brown, J.; Pusztai, L.; Rimm, D.L. In situ tumor PD-L1 mRNA expression is associated with increased TILs and better outcome in breast carcinomas. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 2773–2782. [Google Scholar] [CrossRef] [Green Version]
- Parsa, A.T.; Waldron, J.S.; Panner, A.; Crane, C.A.; Parney, I.F.; Barry, J.J.; Cachola, K.E.; Murray, J.C.; Tihan, T.; Jensen, M.C.; et al. Loss of tumor suppressor PTEN function increases B7-H1 expression and immunoresistance in glioma. Nat. Med. 2007, 13, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, A.A.; Ibrahim, E.M.; Raja, M.A.; Al-Sobhi, S.; Rostom, A.; Stuart, R.K. Locally advanced breast cancer in Saudi Arabia: High frequency of stage III in a young population. Med. Oncol. 1999, 16, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Al-Malki, J.S.; Al-Jaser, M.H.; Warsy, A.S. Overweight and obesity in Saudi females of childbearing age. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2003, 27, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ligibel, J. Obesity and breast cancer. Oncology 2011, 25, 994–1000. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD-L1 (SP263) | PD-L1 (MIH1) | |||||
|---|---|---|---|---|---|---|
| − | + | *p | − | + | *p | |
| Estrogen Receptor Status | ||||||
| Positive | 44 (94) | 3 (6) | 37 (79) | 10 (21) | ||
| Negative | 16 (73) | 6 (27) | 0.025 | 12 (55) | 10 (45) | 0.039 |
| Progesterone Receptor Status | ||||||
| Positive | 33 (97) | 1 (3) | 28 (82) | 6 (18) | ||
| Negative | 27 (77) | 8 (23) | 0.028 | 21 (67) | 14 (33) | 0.041 |
| E1L3N | 28-8 | |||||
|---|---|---|---|---|---|---|
| FR | FFPE | ↓Drop | FR | FFPE | ↓Drop | |
| ♣ R. Sensitivity | 67 | 33 | 34 | 89 | 22 | 67 |
| R. Specificity | 100 | 100 | 0 | 95 | 100 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghebeh, H.; Mansour, F.A.; Colak, D.; Alfuraydi, A.A.; Al-Thubiti, A.A.; Monies, D.; Al-Alwan, M.; Al-Tweigeri, T.; Tulbah, A. Higher PD-L1 Immunohistochemical Detection Signal in Frozen Compared to Matched Paraffin-Embedded Formalin-Fixed Tissues. Antibodies 2021, 10, 24. https://0-doi-org.brum.beds.ac.uk/10.3390/antib10030024
Ghebeh H, Mansour FA, Colak D, Alfuraydi AA, Al-Thubiti AA, Monies D, Al-Alwan M, Al-Tweigeri T, Tulbah A. Higher PD-L1 Immunohistochemical Detection Signal in Frozen Compared to Matched Paraffin-Embedded Formalin-Fixed Tissues. Antibodies. 2021; 10(3):24. https://0-doi-org.brum.beds.ac.uk/10.3390/antib10030024
Chicago/Turabian StyleGhebeh, Hazem, Fatmah A. Mansour, Dilek Colak, Akram A. Alfuraydi, Amal A. Al-Thubiti, Dorota Monies, Monther Al-Alwan, Taher Al-Tweigeri, and Asma Tulbah. 2021. "Higher PD-L1 Immunohistochemical Detection Signal in Frozen Compared to Matched Paraffin-Embedded Formalin-Fixed Tissues" Antibodies 10, no. 3: 24. https://0-doi-org.brum.beds.ac.uk/10.3390/antib10030024