Long-Term Carbapenems Antimicrobial Stewardship Program

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Adequacy of Treatment
2.2. Clinical Impact
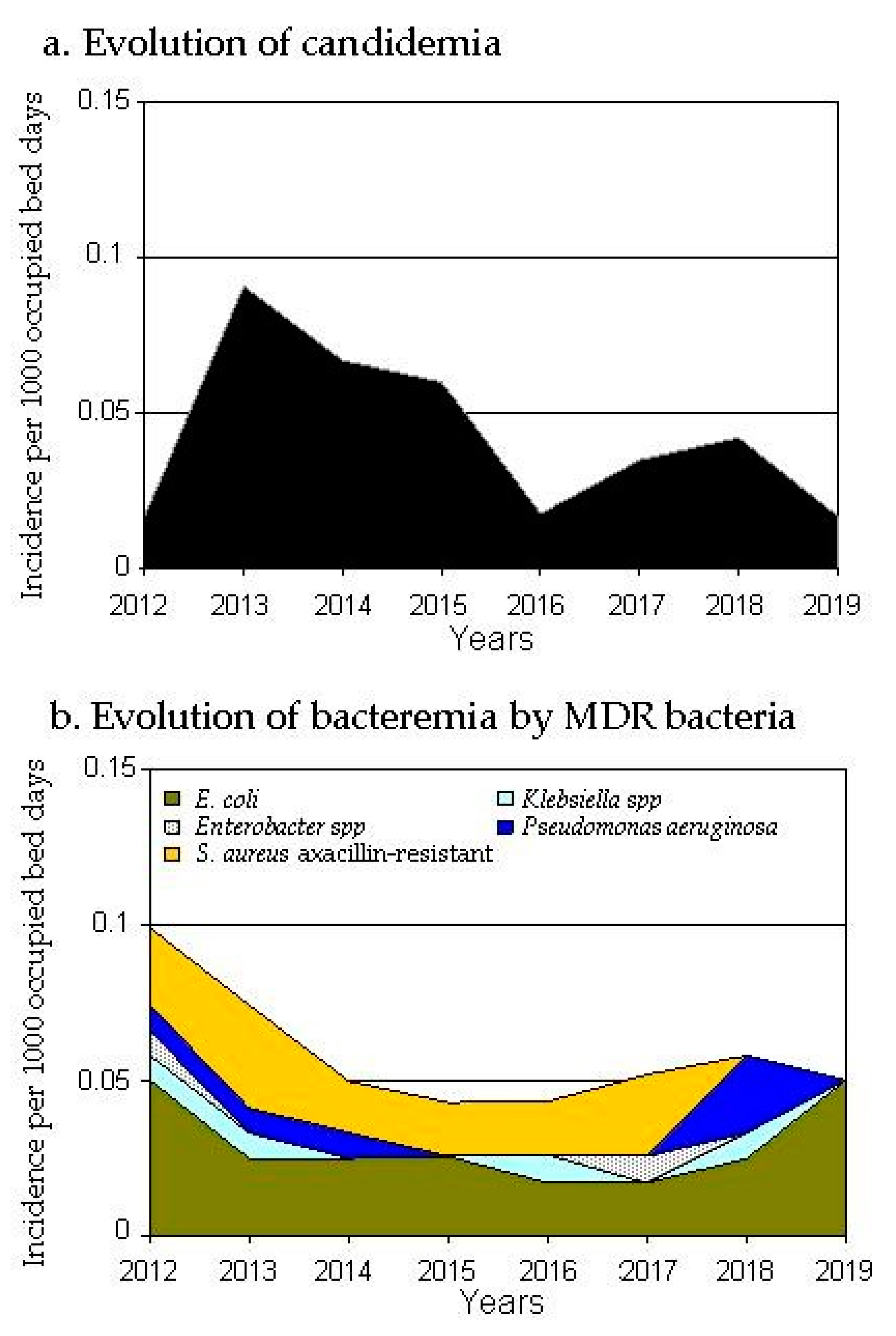
2.3. Impact on Resistance
3. Discussion
4. Materials and Methods
4.1. Adequacy of Treatment
4.2. Clinical Impact
4.3. Impact on Resistance
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. General Assembly of the United Nations: President of the 71st Session. 2016. Available online: http://www.un.org/pga/71/2016/09/21/press-release-hl-meeting-on-antimicrobial-resistance/ (accessed on 30 October 2020).
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Hamilton, C.W. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Karanika, S.; Paudel, S.; Grigoras, C.; Kalbasi, A.; Mylonakis, E. Systematic Review and Meta-analysis of Clinical and Economic Outcomes from the Implementation of Hospital-Based Antimicrobial Stewardship Programs. Antimicrob. Agents Chemother. 2016, 60, 4840–4852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuts, E.C.; Hulscher, M.E.; Mouton, J.W.; Verduin, C.M.; Stuart, J.W.C.; Overdiek, H.W.; Schouten, J.A. Current evidence on hospital antimicrobial stewardship objetives: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 847–856. [Google Scholar] [CrossRef]
- Lawes, T.; Lopez-Lozano, J.-M.; A Nebot, C.; Macartney, G.; Subbarao-Sharma, R.; Dare, C.R.; Wares, K.D.; Gould, I.M. Effects of national antibiotic stewardship and infection control strategies on hospital-associated and community-associated meticillin-resistant Staphylococcus aureus infections across a region of Scotland: A non-linear time-series study. Lancet Infect. Dis. 2015, 15, 1438–1449. [Google Scholar] [CrossRef]
- Molina, J.; Peñalva, G.; Gil-Navarro, M.V.; Praena, J.; A Lepe, J.; A Pérez-Moreno, M.; Ferrándiz, C.; Aldabó, T.; Aguilar, M.; Olbrich, P.; et al. Long-Term Impact of an Educational Antimicrobial Stewardship Program on Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections: A Quasi-Experimental Study of Interrupted Time-Series Analysis. Clin. Infect. Dis. 2017, 65, 1992–1999. [Google Scholar] [CrossRef] [Green Version]
- Lawes, T.; Lopez-Lozano, J.-M.; A Nebot, C.; Macartney, G.; Subbarao-Sharma, R.; Wares, K.D.; Sinclair, C.; Gould, I.M. Effect of a national 4C antibiotic stewardship intervention on the clinical and molecular epidemiology of Clostridium difficile infections in a region of Scotland: A non-linear time-series analysis. Lancet Infect. Dis. 2017, 17, 194–206. [Google Scholar] [CrossRef]
- Liew, Y.X.; Lee, W.; Loh, J.C.Z.; Cai, Y.; Tang, S.S.L.; Lim, C.L.L.; Chlebicki, M.P. Impact of an antimicrobial stewardship program on patient safety in Singapore General Hospital. Int. J. Antimicrob. Agents 2012, 40, 55–60. [Google Scholar] [CrossRef]
- Tedeschi, S.; Trapani, F.; Giannella, M.; Cristini, F.; Tumietto, F.; Bartoletti, M.; Liverani, A.; Pignanelli, S.; Toni, L.; Pederzini, R.; et al. An Antimicrobial Stewardship Program Based on Systematic Infectious Disease Consultation in a Rehabilitation Facility. Infect. Control. Hosp. Epidemiol. 2016, 38, 76–82. [Google Scholar] [CrossRef]
- Marcelin, J.R.; Chung, P.; Van Schooneveld, T. Antimicrobial stewardship in the outpatient setting: A review and proposed framework. Infect. Control. Hosp. Epidemiol. 2020, 41, 833–840. [Google Scholar] [CrossRef]
- Van Duin, D.; A Arias, C.; Komarow, L.; Chen, L.; Hanson, B.M.; Weston, G.; Cober, E.; Garner, O.B.; Jacob, J.T.; Satlin, M.J.; et al. Molecular and clinical epidemiology of carbapenem-resistant Enterobacterales in the USA (CRACKLE-2): A prospective cohort study. Lancet Infect. Dis. 2020, 20, 731–741. [Google Scholar] [CrossRef]
- Mathers, A.J.; Vegesana, K.; German-Mesner, I.; Ainsworth, J.; Pannone, A.; Crook, D.; Sifri, C.; Sheppard, A.; Stoesser, N.; Peto, T.; et al. Risk factors for Klebsiella pneumoniae carbapenemase (KPC) gene acquisition and clinical outcomes across multiple bacterial species. J. Hosp. Infect. 2020, 104, 456–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, K.; Bradford, P.A. Epidemiology of ß-Lactamase-Producing Pathogens. Clin. Microbiol. Rev. 2020, 33, eooo47-19. [Google Scholar] [CrossRef] [PubMed]
- Samonis, G.; Galanakis, E.; Ntaoukakis, M.; Sarchianaki, E.; Spathopoulou, T.; Dimopoulou, D.; Kofteridis, D.P.; Maraki, S. Effects of carbapenems and their combination with amikacin on murine gut colonisation byCandida albicans. Mycoses 2012, 56, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Keighley, C.; Pope, A.; Marriott, D.; Chapman, B.; Bak, N.; Daveson, K.; Sorrell, T.C. Risk factors for candidaemia: A prospective multi-centre case-control study. Mycoses 2020. [Google Scholar] [CrossRef]
- Keighley, C.; Pope, A.; Marriott, D.; Chapman, B.; Bak, N.; Daveson, K.; Sorrell, T.C. European Antimicrobial Resistance Genes Surveillance Network EURGen-Net Capacity Survey Group. Worsening epidemiological situation of carbapenemase-producing Enterobacteriaceae in Europe, assessment by national experts from 37 countries, July 2018. Euro Surveill 2019, 24. [Google Scholar] [CrossRef]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- García-Rodríguez, J.F.; Bardán-García, B.; Peña-Rodríguez, M.F.; Álvarez-Díaz, H.; Mariño-Callejo, A. Meropenem antimicrobial stewardship program: Clinical, economic, and antibiotic resistance impact. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 161–170. [Google Scholar] [CrossRef]
- Estimation of Weights and Costs of Hospital Processes in the National Health System: Methodology and Main Results. Health Information and Statistics 2019. Ministry of Health, Consumption and Social Welfare. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/docs/CMBD/Inf_proc_estim_cost_hosp_SNS2017.pdf (accessed on 30 October 2020).
- Moehring, R.W.; Anderson, D.J.; Cochran, R.L.; Hicks, L.A.; Srinivasan, A.; Ashley, E.S.D.; Structured Taskforce of Experts Working at Reliable Standards for Stewardship (STEWARDS) Panel. Expert Consensus on Metrics to Assess the Impact of Patient-Level Antimicrobial Stewardship Interventions in Acute-Care Settings. Clin. Infect. Dis. 2017, 64, 377–383. [Google Scholar] [CrossRef] [Green Version]
- Spivak, E.S.; Cosgrove, S.E.; Srinivasan, A. Measuring Appropriate Antimicrobial Use: Attempts at Opening the Black Box. Clin. Infect. Dis. 2016, 63, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-S.; Lin, I.-F.; Yen, Y.-F.; Lin, P.-C.; Shiu, Y.-C.; Hu, H.-Y.; Yang, Y.-P. Impact of an antimicrobial stewardship program with multidisciplinary cooperation in a community public teaching hospital in Taiwan. Am. J. Infect. Control. 2013, 41, 1069–1072. [Google Scholar] [CrossRef]
- Lew, K.Y.; Ng, T.M.; Tan, M.; Tan, S.H.; Lew, E.L.; Ling, L.M.; Teng, C.B. Safety and Clinical outcomes of carbapenem de-escalation as part of an antimicrobial stewardship program in an ESBL-endemic setting. J. Antimicrob. Chemother. 2015, 70, 1219–1225. [Google Scholar] [PubMed] [Green Version]
- Teng, C.B.; Ng, T.M.; Tan, M.W.; Tan, S.H.; Tay, M.; Lim, S.F.; Ling, L.M.; Brenda, A.S.P.; Lye, D.C.B. Safety and effectiveness of improving carbapenem use via prospective review and feedback in a multidisciplinary antimicrobial stewardship programme. Ann. Acad. Med. Singap. 2015, 44, 19–25. [Google Scholar] [PubMed]
- Sadyrbaeva-Dolgova, S.; Aznarte-Padial, P.; Jimenez-Morales, A.; Expósito-Ruiz, M.; Calleja-Hernández, M.Á.; Hidalgo-Tenorio, C. Pharmacist recommendations for carbapenem de-escalation in urinary tract infection within an antimicrobial stewardship program. J. Infect. Public Health 2020, 13, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.; On behalf of the San Martino Antimicrobial Stewardship Group; Del Bono, V.; Mikulska, M.; Gustinetti, G.; Marchese, A.; Mina, F.; Signori, A.; Orsi, A.; Rudello, F.; et al. Impact of a mixed educational and semi-restrictive antimicrobial stewardship project in a large teaching hospital in Northern Italy. Infection 2017, 45, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Martín-Gutiérrez, G.; Peñalva, G.; De Pipaón, M.R.-P.; Aguilar, M.; Gil-Navarro, M.V.; Pérez-Blanco, J.L.; Pérez-Moreno, M.A.; Amaya-Villar, R.; Ferrándiz-Millón, C.; Gascón, M.L.; et al. Efficacy and safety of a comprehensive educational antimicrobial stewardship program focused on antifungal use. J. Infect. 2020, 80, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Poissy, J.; Funginos, T.; Damonti, L.; Bignon, A.; Khanna, N.; Von Kietzell, M.; Boggian, K.; Neofytos, D.; Vuotto, F.; Coiteux, V.; et al. Risk factors for candidemia: A prospective matched case-control study. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Stenehjem, E.; Hyun, D.Y.; Septimus, E.; Yu, K.C.; Meyer, M.; Raj, D.; Srinivasan, A. Antibiotic Stewardship in Small Hospitals: Barriers and Potencial Solutions. Clin. Infect. Dis. 2017, 65, 691–696. [Google Scholar] [CrossRef]
- Apisarnthanarak, A.; Bhooanusas, N.; Yaprasert, A.; Mundy, L.M. Carbapenem De-escalation Therapy in a Resource-Limited Setting. Infect. Control. Hosp. Epidemiol. 2013, 34, 1310–1313. [Google Scholar] [CrossRef]
- Olesen, S.W.; Barnett, M.L.; MacFadden, D.R.; Brownstein, J.S.; Hernández-Díaz, S.; Lipsitch, M.; Grad, Y.H. The distribution of antibiotic use and its association with antibiotic resistance. eLife 2018, 7, e39435. [Google Scholar] [CrossRef]
- López-Lozano, J.-M.; THRESHOLDS Study Group; Lawes, T.; Nebot, C.; Beyaert, A.; Bertrand, X.; Hocquet, D.; Aldeyab, M.; Scott, M.; Conlon-Bingham, G.; et al. A nonlinear time-series analysis approach to identify thresholds in associations between population antibiotic use and rates of resistance. Nat. Microbiol. 2019, 4, 1160–1172. [Google Scholar] [CrossRef]
- Kazakova, S.V.; Baggs, J.; McDonald, L.C.; Yi, S.H.; Hatfield, K.M.; Guh, A.; Reddy, S.C.; A Jernigan, J. Association Between Antibiotic Use and Hospital-onset Clostridioides difficile Infection in US Acute Care Hospitals, 2006–2012: An Ecologic Analysis. Clin. Infect. Dis. 2020, 70, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meini, S.; Tascini, C.; Cei, M.; Sozio, E.; Rossolini, G.M. AmpC β-lactamase-producing Enterobacterales: What a clinician should know. Infection 2019, 47, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Tabak, Y.P.; Srinivasan, A.; Yu, K.C.; Kurtz, S.G.; Gupta, V.; Gelone, S.; Scoble, P.J.; McDonald, L.C. Hospital-level high-risk antibiotic use in relation to hospital-associated Clostridioides difficile infections: Retrospective analysis of 2016–2017 data from US hospitals. Infect. Control. Hosp. Epidemiol. 2019, 40, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; A Marwick, C.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, D.J.; Watson, S.; Moehring, R.W.; Komarow, L.; Finnemeyer, M.; Arias, R.M.; Huvane, J.; Hill, C.B.; Deckard, N.; Sexton, D.J.; et al. Feasibility of Core Antimicrobial Stewardship Interventions in Community Hospitals. JAMA Netw. Open 2019, 2, e199369. [Google Scholar] [CrossRef] [PubMed]
- Stenehjem, E.; Hersh, A.L.; Buckel, W.R.; Jones, P.; Sheng, X.; Evans, R.S.; Burke, J.P.; Lopansri, B.K.; Srivastava, R.; Greene, T.; et al. Impact of Implementing Antibiotic Stewardship Programs in 15 Small Hospitals: A Cluster-Randomized Intervention. Clin. Infect. Dis. 2018, 67, 525–532. [Google Scholar] [CrossRef]
- Zhang, D.; Hu, S.; Sun, J.; Zhang, L.; Dong, H.; Feng, W.; Lei, J.; Lu, T. Antibiotic consumption versus the prevalence of carbapenem-resistant Gram-negative bacteria at a tertiary hospital in China from 2011 to 2017. J. Infect. Public Health 2019, 12, 195–199. [Google Scholar] [CrossRef]
- Informe SOGAMIC Sobre Resistencias a Antimicrobianos en Galicia. 2019 December. Dirección Xeral de Saúde Pública da Consellería de Sanidade. Available online: http://sogamic.es/wp-content/uploads/2019/12/Informe-SOGAMIC-sobre-resistencias-2018-1.pdf (accessed on 30 October 2020).
- García-Rodríguez, J.F.; Álvarez, H.; Vilariño-Maneiro, L.; Lorenzo-García, M.V.; Canton, A.; Ordoñez-Barrosa, P.; Mariño-Callejo, A.I.; Sesma-Sánchez, P. Epidemiology and impact of a multifaceted approach in controlling central venous catheter associated blood stream infections outside the intensive care unit. BMC Infect. Dis. 2013, 13, 445. [Google Scholar] [CrossRef] [Green Version]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Osborn, T.M. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef]
- WHO Collaborating Center for Drug Statistics Methodology. DDD Definition and General Considerations. 2016. Available online: https://www.whocc.no/ddd/definition_and_general_considera/ (accessed on 8 May 2020).
- Mattner, F.; Bange, F.C.; Meyer, E.; Seifert, H.; Wichelhaus, T.A.; Chaberny, I.F. Preventing the spread of multidrug-resistant gram-negative pathogens: Recommendations of an expert panel of the German Society For Hygiene and Microbiology. Dtsch. Arztebl. Int. 2012, 109, 39–45. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Intervention Accepted n = 371 | Intervention Rejected n = 77 | p |
|---|---|---|---|
| Male gender, n (%) | 243 (65.5) | 48 (62.3) | 0.6 |
| Median age ± SD, years (range) | 67.2 ± 15.5 (10–96) | 66 ± 18.8 (6–95) | 0.6 |
| Charlson comorbidity score, Median ± SD, (range) | 5.2 ± 2.9 (0–13.6) | 4.8 ± 2.9 (0–12) | 0.4 |
| Neutropenia, <500/mL | 7 (1.9) | 3 (3.9) | 0.4 |
| Sepsis | 15 (4) | 5 (6.5) | 0.4 |
| Site of infections, n (%) | |||
| Pulmonary | 64 (17.3) | 24 (31.2) | 0.007 |
| Abdominal | 99 (26.7) | 36 (46.8) | 0.001 |
| Skin/soft tissue | 25 (6.7) | 1 (1.3) | 0.06 |
| Urinary | 131 (35.3) | 12 (15.6) | 0.001 |
| Other | 52 (14) | 4 (5.2) | 0.04 |
| Acquisition place of infection | |||
| Hospital onset | 127 (34.2) | 33 (42.8) | 0.15 |
| Healthcare-associated | 134 (36.1) | 28 (36.4) | 1 |
| Community-associated | 110 (29.6) | 16 (20.8) | 0.13 |
| Variables | Intervention Accepted n = 371 | Intervention Rejected n = 77 | p |
|---|---|---|---|
| Evolution to healing | 329 (88.7%) | 64 (83.1%) | 0.4 |
| Death caused by infection | 15 (4%) | 7 (9.1%) | 0.08 |
| All-cause crude death | 42 (11.3%) | 12 (15.6%) | 0.3 |
| Readmission in a month | 15 # (4%) | 4 * (5.2%) | 0.6 |
| Adverse effects | 42 (11.3%) | 7 (9.1%) | 0.8 |
| Phlebitis | 64 (17.3%) | 11 (14.3%) | 0.6 |
| Development of resistance to treatment | 8 (2.2%) | 0 (0%) | 0.4 |
| Diarrhea caused by C. difficile | 6 (1.6%) | 2 (2.6%) | 0.6 |
| Colonization-Infection with Candida spp. | 40 (10.8%) | 11 (14.3%) | 0.4 |
| Days of antibiotic treatment (intervention series) | 11 ± 10.2 | 12.7 ± 8.5 | 0.2 |
| Total inpatient days, X ± SD | 17.7 ± 16.7 | 25.3 ± 22.3 | 0.006 |
| Inpatient days post-intervention, X ± SD | 12.5 ± 14.2 | 16.7 ± 18.9 | 0.03 |
| Healthcare Variable. | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|---|---|
| Nº of patients admitted | 14,721 | 14,615 | 14,979 | 14,867 | 14,852 | 15,248 | 15,561 | 15,641 |
| Nº of inpatient days | 119,885 | 121,181 | 119,615 | 116,588 | 114,072 | 114,864 | 120,133 | 119,350 |
| Blood cultures performed, No. | 3242 | 3340 | 2985 | 3003 | 3419 | 3074 | 3554 | 3331 |
| Nº blood cultures/1000 OBDs * | 27.0 | 27.6 | 24.9 | 25.8 | 29.9 | 26.8 | 29.6 | 27.9 |
| Hospital-acquired BSIs per 1000 OBDs * | 0.8 | 0.9 | 0.8 | 0.8 | 0.8 | 1.0 | 1.4 | 1.0 |
| Hospital-acquired no-MDR BSIs/1000 OBDs * | 0.7 | 0.8 | 0.7 | 0.7 | 0.8 | 0.9 | 1.3 | 0.9 |
| Intravascular catheter-associated BSIs/1000 OBDs * | 0.3 | 0.4 | 0.5 | 0.4 | 0.4 | 0.5 | 0.7 | 0.4 |
| Surgical procedures, Nº/1000 OBDs *. | 74 | 77 | 74 | 78 | 82 | 80 | 76 | 79 |
| Case mix index + | 1.5 | 1.5 | 1.6 | 1.6 | 0.8 | 0.9 | 0.9 | 0.9 |
| Parenteral nutrition units, No./1000 OBDs | 29.1 | 38.7 | 39.5 | 46.1 | 41.3 | 34.0 | 28.9 | 26.5 |
| Consumption of antifungals, DDD/1000 OBDs * | 29.1 | 38.4 | 30.8 | 34.9 | 33.1 | 25.5 | 23.6 | 21.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Rodríguez, J.F.; Bardán-García, B.; Juiz-González, P.M.; Vilariño-Maneiro, L.; Álvarez-Díaz, H.; Mariño-Callejo, A. Long-Term Carbapenems Antimicrobial Stewardship Program. Antibiotics 2021, 10, 15. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010015
García-Rodríguez JF, Bardán-García B, Juiz-González PM, Vilariño-Maneiro L, Álvarez-Díaz H, Mariño-Callejo A. Long-Term Carbapenems Antimicrobial Stewardship Program. Antibiotics. 2021; 10(1):15. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010015
Chicago/Turabian StyleGarcía-Rodríguez, José Francisco, Belén Bardán-García, Pedro Miguel Juiz-González, Laura Vilariño-Maneiro, Hortensia Álvarez-Díaz, and Ana Mariño-Callejo. 2021. "Long-Term Carbapenems Antimicrobial Stewardship Program" Antibiotics 10, no. 1: 15. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010015