
Effects of Metronidazole as an Adjunct to Non-Surgical Periodontal Therapy on Insulin Resistance in Type 2 Diabetics


Abstract
:1. Introduction
2. Results
2.1. Baseline Associations with the HOMA-IR before Random Allocation
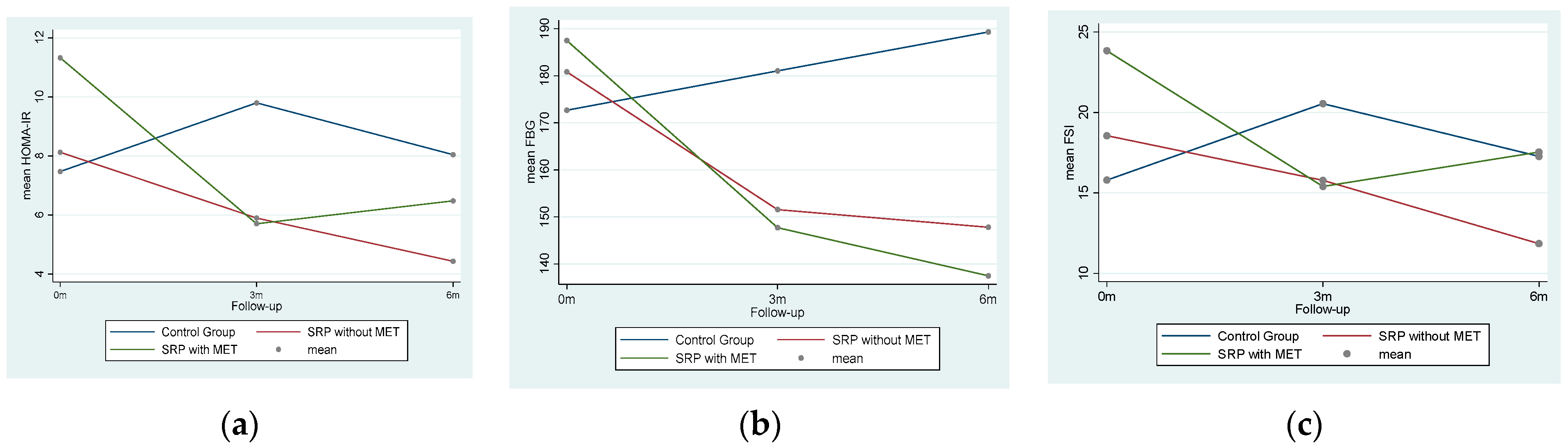
2.2. Mean Changes in the HOMA-IR in the Three Arms over Time
2.3. Intra-Group FSI and HOMA-IR Changes
2.4. Inter-Group FSI and HOMA-IR Changes
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Way, K.L.; Hackett, D.A.; Baker, M.K.; Johnson, N.A. The effect of regular exercise on insulin sensitivity in type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Metab. J. 2016, 40, 253–269. [Google Scholar] [CrossRef]
- Keshel, T.E. Exercise training and insulin resistance: A current review. J. Obes. Weight Loss Ther. 2015, 5, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Demmer, R.T.; Squillaro, A.; Papapanou, P.N.; Rosenbaum, M.; Friedewald, W.T.; Jacobs, D.R.; Desvarieux, M. Periodontal infection, systemic inflammation, and insulin resistance results from the continuous national health and nutrition examination survey (NHANES) 1999–2004. Diabetes Care 2012, 35, 2235–2242. [Google Scholar] [CrossRef] [Green Version]
- Gutch, M.; Kumar, S.; Razi, S.M.; Gupta, K.K.; Gupta, A. Assessment of insulin sensitivity/resistance. Indian J. Endocrinol. Metab. 2015, 19, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.K.; Seo, M.; Lee, Y.S.; Moon, S.S. Association of periodontitis with insulin resistance, β-cell function, and impaired fasting glucose before onset of diabetes. Endocr. J. 2015, 62, 981–989. [Google Scholar] [CrossRef] [Green Version]
- Kuo, L.C.; Polson, A.M.; Kang, T. Associations between periodontal diseases and systemic diseases: A review of the inter-relationships and interactions with diabetes, respiratory diseases, cardiovascular diseases and osteoporosis. Public Health 2008, 122, 417–433. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Mahmood, A.K.; Ismail, A.A.; Rashid, F.A.; Wan Bebakar, W.M. Insulin sensitivity and secretory status of a healthy Malay population. Malays. J. Med. Sci. 2006, 13, 37–44. [Google Scholar]
- Lim, S.G.; Han, K.; Kim, H.; Pyo, S.W.; Cho, Y.; Kim, K.; Yim, H.W.; Lee, W.; Park, Y.G.; Park, Y. Association between insulin resistance and periodontitis in Korean adults. J. Clin. Periodontol. 2014, 41, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Grossi, S.G.; Ho, A.; Nishimura, F.; Murayama, Y. A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J. Periodontol. 2005, 76, 2075–2084. [Google Scholar] [CrossRef]
- Benguigui, C.; Bongard, V.; Ruidavets, J.; Chamontin, B.; Sixou, M.; Ferrieres, J.; Amar, J. Metabolic syndrome, insulin resistance, and periodontitis: A cross-sectional study in a middle-aged French population. J. Clin. Periodontol. 2010, 37, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Timonen, P.; Suominen-Taipale, L.; Jula, A.; Niskanen, M.; Knuuttila, M.; Ylostalo, P. Insulin sensitivity and periodontal infection in a non-diabetic, non-smoking adult population. J. Clin. Periodontol. 2011, 38, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Allen, E.M.; Matthews, J.B.; O’Halloran, D.J.; Griffiths, H.R.; Chapple, I.L. Oxidative and inflammatory status in Type 2 diabetes patients with periodontitis. J. Clin. Periodontol. 2011, 38, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.P.; Bullon, P.; Morillo, J.M.; Battino, M.; Quiles, J.L.; Ramirez-Tortosa, M.C. The relationship between insulin resistance and periodontitis is not affected by Mediterranean diet in a Spanish population. Arch. Oral Biol. 2017, 77, 62–67. [Google Scholar] [CrossRef]
- Qureshi, A.; Haque, Z.; Bokhari, S.A.H.; Baloch, A.A. Evaluation of HbA1c in type-2 diabetes mellitus patients with periodontitis: Preliminary findings of three-arm clinical trial. J. Pak. Med. Assoc. 2020, 70, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, K. Periodontal study on patients with type 2 diabetes. Jpn. Periodontal Soc. J. 2005, 47, 178–185. [Google Scholar] [CrossRef]
- Sun, W.L.; Chen, L.L.; Zhang, S.Z.; Wu, Y.M.; Ren, Y.Z.; Qin, G.M. Inflammatory cytokines, adiponectin, insulin resistance and metabolic control after periodontal intervention in patients with type 2 diabetes and chronic periodontitis. Intern. Med. 2011, 50, 1569–1574. [Google Scholar] [CrossRef] [Green Version]
- Nishioka, S.; Maruyama, K.; Tanigawa, T.; Miyoshi, N.; Eguchi, E.; Nishida, W.; Osawa, H.; Saito, I. Effect of non-surgical periodontal therapy on insulin resistance and insulin sensitivity among individuals with borderline diabetes: A randomized controlled trial. J. Dent. 2019, 85, 18–24. [Google Scholar] [CrossRef]
- Engebretson, S.P.; Hyman, L.G.; Michalowicz, B.S.; Schoenfeld, E.R.; Gelato, M.C.; Hou, W.; Seaquist, E.R.; Reddy, M.S.; Lewis, C.E.; Oates, T.W.; et al. The effect of nonsurgical periodontal therapy on hemoglobin A1c levels in persons with type 2 diabetes and chronic periodontitis: A randomized clinical trial. J. Am. Med. Assoc. 2013, 310, 2523–2532. [Google Scholar] [CrossRef] [Green Version]
- ClinicalTrials.gov: National Library of Medicine (US). (2000 Feb 29-). Identifier NCT03343366. Glycemic Control in T2DM through Non-Surgical Periodontal Therapy [Last Updated on August 20, 2020]. Available online: https://clinicaltrials.gov/ct2/show/NCT03343366 (accessed on 6 September 2021).
- Qureshi, A.; Bokhari, S.A.H.; Haque, Z.; Baloch, A.A.; Zaheer, S. Clinical efficacy of scaling and root planing with and without metronidazole on glycemic control: Three arm randomized controlled trial. BMC Oral Health 2021, 21, 253. [Google Scholar] [CrossRef]
- Mealey, B.L. Periodontal disease and diabetes: A two-way street. J. Am. Dent. Assoc. 2006, 137, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Luchian, I.; Goriuc, A.; Martu, M.A.; Covasa, M. Clindamycin as an alternative option in optimizing periodontal therapy. Antibiotics 2021, 10, 814. [Google Scholar] [CrossRef]
- Yoshida, N.; Saito, Y.; Tsujimoto, Y.; Taito, S.; Banno, M.; Kataoka, Y.; Yamashita, T.; Hirata, K.-I. The impact of antibiotics on the metabolic status of obese adults without bacterial infection: A systematic review and meta-analysis. Ann. Transl. Med. 2020, 8, 1059. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, H.; Mahmood, N.; Kumar, M.; Varikuti, S.R.; Challa, H.R.; Myakala, S.P. Effect of Probiotic (VSL#3) and Omega-3 on Lipid Profile, Insulin Sensitivity, Inflammatory Markers, and Gut Colonization in Overweight Adults: A Randomized, Controlled Trial. Mediat. Inflamm. 2014, 2014, 348959. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Chen, L.; Ni, K. The effect of tinidazole in the treatment of adult periodontitis. Zhonghua Kou Qiang Yi Xue Za Zhi 1996, 31, 303–306. (In Chinese) [Google Scholar] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care 2013, 36, S11–S66. [Google Scholar] [CrossRef] [Green Version]
- Katagiri, S.; Nitta, H.; Nagasawa, T.; Uchimura, I.; Izumiyama, H.; Inagaki, K.; Kikuchi, T.; Noguchi, T.; Kanazawa, M.; Matsuo, A.; et al. Multi-center intervention study on glycohemoglobin (HbA1c) and serum, high-sensitivity CRP (hs-CRP) after local anti-infectious periodontal treatment in type 2 diabetic patients with periodontal disease. Diabetes Res. Clin. Pract. 2009, 83, 308–315. [Google Scholar] [CrossRef]
- Kocher, T.; König, J.; Borgnakke, W.; Pink, C.; Meisel, P. Periodontal complications of hyperglycemia/diabetes mellitus: Epidemiologic complexity and clinical challenge. Periodontology 2018, 78, 59–97. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Preda, C.; Chiesa, A.; Esposito, F.; Pascadopoli, M.; Scribante, A. Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial. Appl. Sci. 2021, 11, 8586. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Singh, S.; Kumar, V.; Kumar, S.; Subbappa, A. The effect of periodontal therapy on the improvement of glycaemic control in patients with type 2 diabetes mellitus: A randomized controlled clinical trial. Int. J. Diab. Dev. Count 2008, 28, 38–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalachew, A.; Mitchell, G.; Nikles, J. Barriers for conducting trials in developing countries—A systematic review. Int. J. Equal. Health 2018, 17, 37. [Google Scholar]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 world workshop on classification of periodontal and prei-implant diseases and conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundergan, W.P.; Essex, G. Ultrasonic debridement versus hand scaling and root planing. In Hall’s Critical Decisions in Periodontology and Dental Implantology, 5th ed.; Harpenau, L.A., Kao, R.T., Sanz, M., Eds.; People’s Medical Publishing House: Shelton, CT, USA, 2013; p. 177. [Google Scholar]
- Preus, H.R.; Gunleiksrud, T.M.; Sandvik, L.; Gjermo, P.; Baelum, V. A randomized, double-masked clinical trial comparing four periodontitis treatment strategies: 1-year clinical results. J. Periodontol. 2013, 84, 1075–1086. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The efficacy of powered oscillating heads vs. Powered sonic action heads toothbrushes to maintain periodontal and peri-implant health: A narrative review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef]
- Diagnostics, ARCHITECT ci System Specification. Available online: http://www.corelaboratory.abbott/sal/specSheet/ADD-00058823-RI_ARCHITECT%20Soecifications.pdf (accessed on 11 August 2018).
- HOMA-IR Calculator. MD Calc (2005–2019). Available online: https://www.mdcalc.com/homa-ir-homeostatic-model-assessment-insulin-resistance#evidence (accessed on 11 August 2018).


{kind=link}
| Variables | Categories | n (%) | HOMA-IR Coef. (p-Value *) |
|---|---|---|---|
| Gender | Female | 68 (45.3) | -- |
| Male | 82 (54.6) | −0.05 (0.962) | |
| BMI Status | Underweight | 5 (3.3) | -- |
| Normal | 44 (29.3) | 3.47 (0.292) | |
| Overweight | 80 (53.3) | 3.65 (0.255) | |
| Obese | 21 (14) | 1.80 (0.603) | |
| Living Standard (n = 125) | Low | 61 (48.8) | -- |
| Middle | 35 (28) | 1.30 (0.256) | |
| High | 29 (23.2) | 0.34 (0.775) | |
| Smokers (n = 144) | No | 136 (94.4) | -- |
| Yes | 8 (5.5) | 0.75 (0.756) | |
| Substance Abuse (n = 144) | No | 130 (90.2) | -- |
| Yes | 14 (9.7) | 0.79 (0.673) | |
| Co-morbidities (n = 147) | None | 80 (54.4) | -- |
| Hypertension | 33 (22.4) | 1.66 (0.255) | |
| CVD | 9 (6.1) | 1.21 (0.624) | |
| CVD + hypertension | 4 (2.7) | −2.5 (0.489) | |
| Others | 21 (14.2) | 0.02 (0.990) | |
| Diabetes management | Hypoglycemic | 106 (70.6) | -- |
| Insulin | 19 (12.6) | 4.70 (0.006) | |
| Both | 25 (16.6) | 3.47 (0.021) | |
| Regular Exercise | No | 66 (44) | -- |
| Yes | 84 (56) | −1.46 (0.200) | |
| Healthy Diet | No | 38 (25.3) | -- |
| Yes | 112 (74.6) | 0.98 (0.452) | |
| Age (years) | 0.14 (0.046) | ||
| Formal education (years) | 0.09 (0.384) | ||
| Bleeding on probing (%) | 0.00 (0.961) | ||
| Mean Periodontal pocket depth (mm) | 0.90 (0.162) | ||
| Mean Clinical attachment loss (mm) | 0.59 (0.277) | ||
| Variables | SRP + MET + OHI | ∆ | p-Value * | SRP + OHI | ∆ | p-Value * | DT + OHI | ∆ | p-Value * |
|---|---|---|---|---|---|---|---|---|---|
| FSI (F0) | 23.83 ± 16.41 | -- | 0.041 | 18.55 ± 14.44 | -- | 0.046 | 15.80 ± 9.80 | -- | 0.107 |
| FSI (F3) | 15.40 ± 6.55 | −8.43 | 15.77 ± 12.53 | −2.78 | 20.55 ± 16.78 | 4.75 | |||
| FSI (F6) | 17.53 ± 10.98 | −6.3 | 11.85 ± 5.99 | −6.7 | 17.26 ± 6.75 | 1.46 | |||
| F-value = 4.97; MSE (df) = 49.0(29) | F-value = 4.48; MSE (df) = 23.75(32) | F-value = 2.51; MSE (df) = 46.85 (34) | |||||||
| HOMA-IR (F0) | 11.32 ± 9.72 | -- | 0.022 | 8.12 ± 6.46 | -- | 0.013 | 7.47 ± 7.21 | -- | 0.070 |
| HOMA-IR (F3) | 5.70 ± 3.03 | −5.62 | 5.89 ± 4.42 | −2.23 | 9.79 ± 8.78 | 2.32 | |||
| HOMA-IR (F6) | 6.47 ± 4.77 | −4.85 | 4.43 ± 2.26 | −3.69 | 8.04 ± 4.27 | 0.57 | |||
| F-value = 5.63; MSE (df) = 24.08(29) | F-value = 6.87; MSE (df) = 9.25 (32) | F-value = 3.24; MSE (df) = 9.63 (34) | |||||||
| At 3-Months Follow-Up | At 6-Months Follow-Up | |||||
|---|---|---|---|---|---|---|
| Glycemic Variables v/s Intervention | ∆ | p-Value * | p-Value ** | ∆ | p-Value * | p-Value ** |
| FSI (mlU/L) | ||||||
| ∆ SRP + MET + OHI–DT + OHI | −5.14 | 0.371 | 0.437 | 0.26 | 0.108 | 0.995 |
| ∆ SRP + OHI–DT + OHI | −4.77 | 0.441 | −5.41 | 0.163 | ||
| ∆ SRP + MET + OHI–SRP + OHI | −0.37 | 0.995 | 5.68 | 0.155 | ||
| HOMA-IR | ||||||
| ∆ SRP + MET + OHI–DT + OHI | −4.08 | 0.081 | 0.130 | −1.56 | 0.046 | 0.523 |
| ∆ SRP + OHI–DT + OHI | −3.89 | 0.119 | −3.61 | 0.036 | ||
| ∆ SRP + MET + OHI–SRP + OHI | −0.19 | 0.995 | 2.04 | 0.346 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qureshi, A.; Haque, Z.; Qureshi, H.; Farooqui, W.A. Effects of Metronidazole as an Adjunct to Non-Surgical Periodontal Therapy on Insulin Resistance in Type 2 Diabetics. Antibiotics 2021, 10, 1400. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111400
Qureshi A, Haque Z, Qureshi H, Farooqui WA. Effects of Metronidazole as an Adjunct to Non-Surgical Periodontal Therapy on Insulin Resistance in Type 2 Diabetics. Antibiotics. 2021; 10(11):1400. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111400
Chicago/Turabian StyleQureshi, Ambrina, Zeba Haque, Hina Qureshi, and Waqas Ahmed Farooqui. 2021. "Effects of Metronidazole as an Adjunct to Non-Surgical Periodontal Therapy on Insulin Resistance in Type 2 Diabetics" Antibiotics 10, no. 11: 1400. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111400