Antibiotic Use: A Cross-Sectional Study Evaluating the Understanding, Usage and Perspectives of Medical Students and Pathfinders of a Public Defence University in Malaysia

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
1.1. Prescribing Skills and Medical Students
1.2. Malaysia and Antibiotic Use
1.3. Pathogenic Microbes, Antimicrobials, Mode of Actions, Antimicrobials Resistance Situations
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Study Period
2.4. Sampling Method and Sample Size
2.5. Techniques of Data Collection
- Section 1: To gather socio-demographic data, including age, gender, year of birth, religion, year of study and type of admission.
- Section 2: To evaluate the students’ use of antibiotics over the previous year.
- Section 3: To assess knowledge regarding antibiotic and related adverse reactions.
- Section 4: To gather information about respondents’ awareness of antibiotic resistance.
- Section 5: Focusing on attitudes and behaviors towards antibiotic use.
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Socio-Demographic Profile of the Study Respondents
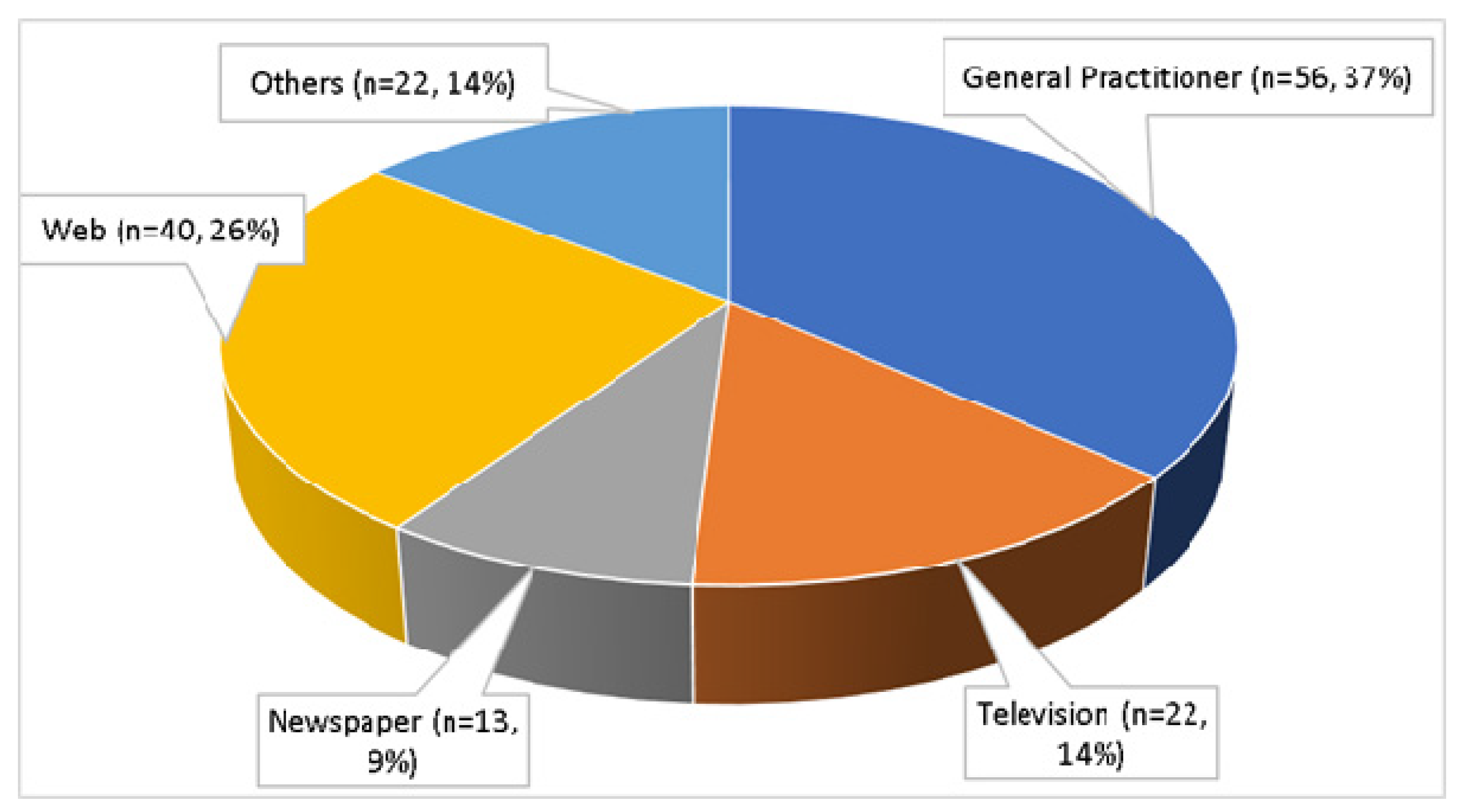
3.2. Usage of Antibiotics
3.3. Knowledge, Awareness, and Attitude Regarding Antibiotics
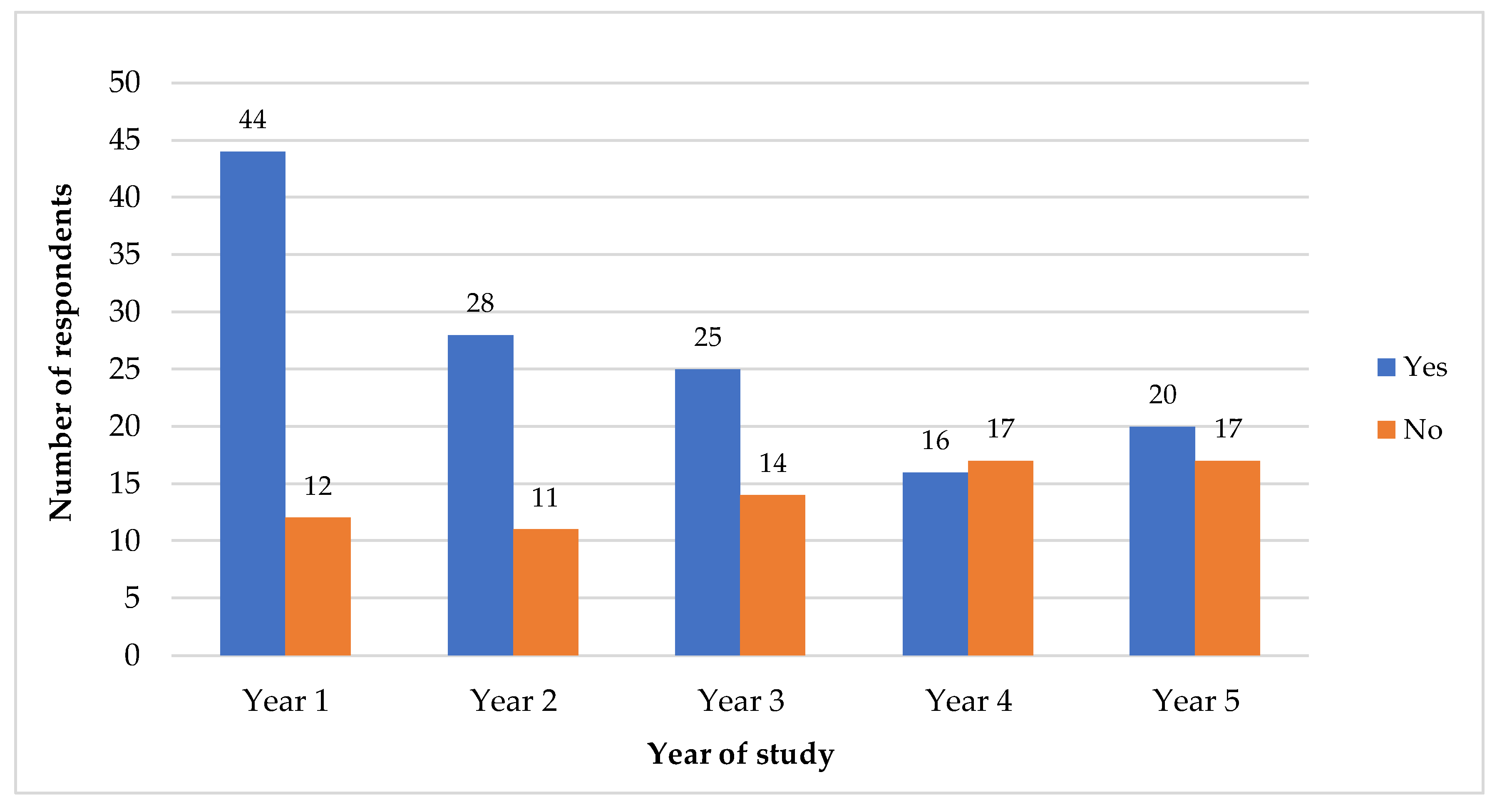
3.4. Factors Associated with Usage of Antibiotics
3.5. Factors Associated with Total Knowledge and Attitude Scores Regarding Antibiotics
3.6. Factors Associated with Stopping Antibiotics When Feeling Better, Keeping Leftover Antibiotics for Future Use and Using Leftover Antibiotics without Doctor’s Consultation
4. Discussion
4.1. Socio-Demographic Profile of the Study Respondents
4.2. Use of Antibiotics and Its Associated Factors
4.3. Knowledge, Awareness, and Attitude Regarding Antibiotics and Its Associated Factors
4.3.1. Knowledge Regarding Antibiotics
4.3.2. Awareness of Antibiotic Resistance
4.3.3. Attitudes Regarding Personal Consumption of Antibiotics
4.3.4. Factors Associated with Knowledge, Awareness, and Attitude Regarding Antibiotics
4.4. Factors Associated with Stopping Antibiotics When Feeling Better, Keeping Leftover Antibiotics for Future Use and Using Leftover Antibiotics without Doctor’s Consultation
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, C.R.; Cho, I.H.; Jeong, B.C.; Lee, S.H. Strategies to Minimize Antibiotic Resistance. Int. J. Environ. Res. Public Health 2013, 10, 4274–4305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantas, L.; Shah, S.Q.; Cavaco, L.M.; Manaia, C.M.; Walsh, F.; Popowska, M.; Garelick, H.; Bürgmann, H.; Sørum, H. A brief multi-disciplinary review on antimicrobial resistance in medicine and its linkage to the global environmental microbiota. Front. Microbiol. 2013, 4, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminov, R. History of antimicrobial drug discovery: Major classes and health impact. Biochem. Pharmacol. 2017, 133, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Powers, J.H.; Brass, E.P.; Miller, L.G.; Edwards, J.E. Trends in Antimicrobial Drug Development: Implications for the Future. Clin. Infect. Dis. 2004, 38, 1279–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dye, C. After 2015: Infectious diseases in a new era of health and development. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2014, 369, 20130426. [Google Scholar] [CrossRef]
- O’Neill, J. Review on Antimicrobial Resistance Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; Review on Antimicrobial Resistance: London, UK, 2014; Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 22 April 2018).
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Littmann, J.; Viens, A.M. The Ethical Significance of Antimicrobial Resistance. Public Health Ethic 2015, 8, 209–224. [Google Scholar] [CrossRef] [Green Version]
- Stewardson, A.J.; Allignol, A.; Beyersmann, J.; Graves, N.; Schumacher, M.; Meyer, R.; Tacconelli, E.; De Angelis, G.; Farina, C.; Pezzoli, F.; et al. TIMBER Study Group. The health and economic burden of bloodstream infections caused by antimicrobial-susceptible and non-susceptible Enterobacteriaceae and Staphylococcus aureus in European hospitals, 2010 and 2011: A multicenter retrospective cohort study. Eurosurveillance 2016, 21, 30319. [Google Scholar] [CrossRef]
- The Conversation. No, You Don’t Have to Finish all Your Antibiotics. 2015. Available online: https://theconversation.com/no-you-dont-have-to-finish-all-your-antibiotics-38774 (accessed on 22 April 2018).
- Ventola, C.L. The Antibiotic Resistance Crisis: Part 1: Causes and Threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Gould, I.M.; Bal, A.M. New antibiotic agents in the pipeline and how they can help overcome microbial resistance. Virulence 2013, 4, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Wright, G.D. Something old, something new: Revisiting natural products in antibiotic drug discovery. Can. J. Microbiol. 2014, 60, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Chattopadhyay, M.K.; Grossart, H.-P. The multifaceted roles of antibiotics and antibiotic resistance in nature. Front. Microbiol. 2013, 4, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piddock, L.J. The crisis of no new antibiotics—What is the way forward? Lancet Infect. Dis. 2012, 12, 249–253. [Google Scholar] [CrossRef]
- United Nations. High-level Meeting on Antimicrobial Resistance. 2016. Available online: https://www.un.org/pga/71/event-latest/high-level-meeting-on-antimicrobial-resistance/ (accessed on 22 April 2018).
- World Health Organization. Global Action Plan on Antimicrobial Resistance; WHO Press: Geneva, Switzerland, 2015; Available online: http://www.wpro.who.int/entity/drug resistance/resources/global_action_plan_eng.pdf (accessed on 22 April 2018).
- Brinkman, D.J.; Tichelaar, J.; Schutte, T.; Benemei, S.; Böttiger, Y.; Chamontin, B.; Christiaens, T.; Likic, R.; Maciulaitis, R.; Marandi, T.; et al. Working Group Research on CPT Education of the European Association for Clinical Pharmacology and Therapeutics (EACPT). Essential competencies in prescribing: A first European cross-sectional study among 895 final-year medical students. Clin. Pharmacol. Ther. 2017, 101, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.; Rahman, N.I.A.; Zulkifli, Z.; Ismail, S. Antibiotic prescribing and resistance: Knowledge level of medical students of clinical years of University Sultan Zainal Abidin, Malaysia. Ther. Clin. Risk Manag. 2016, 12, 413–426. [Google Scholar] [CrossRef] [PubMed]
- Hoque, R.; Mostafa, A.; Haque, M. Insight of Medical Students of Clinical Years to Antimicrobials Prescribing and Resistance in Private Medical School, Chittagong, Bangladesh. J. Young- Pharm. 2016, 8, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Hoque, R.; Mostafa, A.; Haque, M. Intern doctors’ views on the current and future antibiotic resistance situation of Chattagram Maa O Shishu Hospital Medical College, Bangladesh. Ther. Clin. Risk Manag. 2015, 11, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- P&T Community. The Five Most Over-Prescribed Antibiotics Overuse in Medicine and Agriculture Has Led to Slew of ‘Superbugs’ 2018. Available online: https://www.ptcommunity.com/news/2015-05-28-000000/five-most-over-prescribed-antibiotics (accessed on 22 April 2018).
- Weier, N.; Thursky, K.; Zaidi, S.T.R. Antimicrobial knowledge and confidence amongst final year medical students in Australia. PLoS ONE 2017, 12, e0182460. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, S.; Potgieter, S.; Shoul, E.; Constant, D.; Stewart, A.; Mendelson, M.; Boyles, T.H. South African medical students’ perceptions and knowledge about antibiotic resistance and appropriate prescribing: Are we providing adequate training to future prescribers? S. Afr. Med. J. 2017, 107, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Pulcini, C.; Howard, P.; Nathwani, D. ESGAP (ESCMID Study Group for Antibiotic Policies). European medical students: A first multicenter study of knowledge, attitudes, and perceptions of antibiotic prescribing and antibiotic resistance. J. Antimicrob. Chemother. 2014, 69, 842–846. [Google Scholar] [CrossRef]
- Abbo, L.M.; Cosgrove, S.E.; Pottinger, P.S.; Pereyra, M.; Sinkowitz-Cochran, R.; Srinivasan, A.; Webb, D.J.; Hooton, T.M. Medical Students’ Perceptions and Knowledge About Antimicrobial Stewardship: How Are We Educating Our Future Prescribers? Clin. Infect. Dis. 2013, 57, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, D.J.; Tichelaar, J.; Graaf, S.; Otten, R.H.J.; Richir, M.C.; Van Agtmael, M.A. Do final-year medical students have sufficient prescribing competencies? A systematic literature review. Br. J. Clin. Pharmacol. 2018, 84, 615–635. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance. 2018. Available online: http://www.who.int/en/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 27 April 2018).
- Alothman, A.; Algwizani, A.; Alsulaiman, M.; Alalwan, A.; Binsalih, S.; Bosaeed, M. Knowledge and Attitude of Physicians Toward Prescribing Antibiotics and the Risk of Resistance in Two Reference Hospitals. Infect. Dis. Res. Treat. 2016, 9, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Pizzuto, M.A.; Camilleri, L.; Serracino-Inglott, A.; Azzopardi, L.M. Practices and perceptions of medical practitioners on potential antibiotic prescribing by pharmacists. J. Pharm. Health Serv. Res. 2016, 7, 157–164. [Google Scholar] [CrossRef]
- Doctors in the US Incorrectly Prescribe Antibiotics in Nearly a Third of Cases. The Guardian. 2016. Available online: https://www.theguardian.com/society/2016/may/03/us-doctors-antibiotic-prescriptions-study#top (accessed on 27 April 2018).
- Alhomoud, F.; AlJamea, Z.; Almahasnah, R.; Alkhalifah, K.; Basalelah, L.; Alhomoud, F.K. Self-medication and self-prescription with antibiotics in the Middle East—Do they really happen? A systematic review of the prevalence, possible reasons, and outcomes. Int. J. Infect. Dis. 2017, 57, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Lago, J.M.; Lopez-Vazquez, P.; López-Durán, A.; Taracido-Trunk, M.; Figueiras, A. Attitudes of primary care physicians to the prescribing of antibiotics and antimicrobial resistance: A qualitative study from Spain. Fam. Pract. 2012, 29, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Vijayananthan, A.; Nawawi, O. The importance of Good Clinical Practice guidelines and its role in clinical trials. Biomed. Imaging Interv. J. 2008, 4, e5. [Google Scholar] [CrossRef] [PubMed]
- The Patient Safety Education Study Group. Patient Safety in Health Care Professional Educational Curricula: Examining the Learning Experience. 2009. Available online: https://www.birmingham.ac.uk/Documents/college-mds/haps/projects/cfhep/psrp/finalreports/PS030PSRPReportFINAL0609.pdf (accessed on 27 April 2018).
- Leach, J.; Cross, V.; Fawkes, C.; Mandy, A.; Hankins, M.; Fiske, A.; Bottomley, L.; Moore, A. Investigating Osteopathic Patients’ Expectations of Osteopathic Care: The Open Project. 2011. The University of Brighton. Full Research Report. Available online: https://www.ncor.org.uk/wp-content/uploads/2013/02/open_full_research_report_public.pdf (accessed on 27 April 2018).
- World Health Organization. Guidelines for Good Clinical Practice (GCP) for Trials on Pharmaceutical Products. WHO Technical Report Series; No. 850, Annex 3; 1995; Available online: http://apps.who.int/medicinedocs/pdf/whozip13e/whozip13e.pdf (accessed on 27 April 2018).
- Awad, A.I.; Aboud, E.A. Knowledge, Attitude and Practice towards Antibiotic Use among the Public in Kuwait. PLoS ONE 2015, 10, e0117910. [Google Scholar] [CrossRef] [PubMed]
- Havens, L.; Schwartz, M. Identification of Parents Perceptions of Antibiotic Use for Individualized Community Education. Glob. Pediatr. Health 2016, 3, 1–7. [Google Scholar] [CrossRef]
- Tan, W.L.; Siti, R.; Shahfini, I.; Zuraidah, A. Knowledge, attitude and practice of antibiotics prescribing among medical officers of public health care facilities in the state of Kedah, Malaysia. Med. J. Malays. 2015, 70, 307–311. [Google Scholar]
- Chan, G.C.; Tang, S.F. Parental knowledge, attitudes and antibiotic use for acute upper respiratory tract infection in children attending a primary healthcare clinic in Malaysia. Singap. Med. J. 2006, 47, 266–270. [Google Scholar]
- Lim, K.K.; Teh, C.C. A Cross Sectional Study of Public Knowledge and Attitude towards Antibiotics in Putrajaya, Malaysia. South. Med. Rev. 2012, 5, 26–33. [Google Scholar] [PubMed]
- Ling Oh, A.; Hassali, M.A.; Al-Haddad, M.S.; Syed Sulaiman, S.A.; Shafie, A.A.; Awaisu, A. Public knowledge and attitudes towards antibiotic usage: A cross-sectional study among the general public in the state of Penang, Malaysia. J. Infect. Dev. Ctries. 2011, 5, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Islahudin, F.; Tamezi, A.M.A.; Shah, N.M. Knowledge, attitudes and practices about antibiotic use among the general public in Malaysia. Southeast Asian J. Trop. Med. Public Health 2014, 45, 1474–1482. [Google Scholar]
- Fatokun, O. Exploring antibiotic use and practices in a Malaysian community. Int. J. Clin. Pharm. 2014, 36, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Cheong, Y.M.; Lim, V.K.; Jegathesan, M.; Suleiman, A.B. Antimicrobial resistance in 6 Malaysian general hospitals. Med. J. Malays. 1994, 49, 317–326. [Google Scholar]
- Nicholson, A.; Tennant, I.; White, L.; Thoms-Rodriguez, C.A.; Cook, L.; Johnson, S.; Thompson, T.; Barnett, J.; Richards, L. The knowledge, attitudes and practices of doctors regarding antibiotic resistance at a tertiary care institution in the Caribbean. Antimicrob. Resist. Infect. Control 2018, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Thakolkaran, N.; Shetty, A.V.; D’Souza, N.D.R.; Shetty, A.K. Antibiotic prescribing knowledge, attitudes, and practice among physicians in teaching hospitals in South India. J. Fam. Med. Prim. Care 2017, 6, 526–532. [Google Scholar]
- McNulty, C.A.M.; Cookson, B.D.; Lewis, M.A.O. Education of healthcare professionals and the public. J. Antimicrob. Chemother. 2012, 67, 11–18. [Google Scholar] [CrossRef]
- Wei, X.; Zhang, Z.; Walley, J.D.; Hicks, J.P.; Zeng, J.; Deng, S.; Zhou, Y.; Yin, J.; Newell, J.N.; Sun, Q.; et al. Effect of a training and educational intervention for physicians and caregivers on antibiotic prescribing for upper respiratory tract infections in children at primary care facilities in rural China: A cluster-randomized controlled trial. Lancet Glob. Health 2017, 5, e1258–e1267. [Google Scholar] [CrossRef]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef]
- Shehadeh, M.B.; Suaifan, G.A.; Hammad, E.A. Active educational intervention as a tool to improve safe and appropriate use of antibiotics. Saudi Pharm. J. 2016, 24, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Cheesman, M.J.; Ilanko, A.; Blonk, B.; Cock, I.E. Developing New Antimicrobial Therapies: Are Synergistic Combinations of Plant Extracts/Compounds with Conventional Antibiotics the Solution? Pharmacogn. Rev. 2017, 11, 57–72. [Google Scholar] [PubMed]
- Kapoor, G.; Saigal, S.; Elongavan, A. Action and resistance mechanisms of antibiotics: A guide for clinicians. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Davies, J. Microbes have the last word. A drastic re-evaluation of antimicrobial treatment is needed to overcome the threat of antibiotic-resistant bacteria. EMBO Rep. 2007, 8, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Davies, D. Origins and Evolution of Antibiotic Resistance. Microbiol. Mol. Boil. Rev. 2010, 74, 417–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fair, R.J.; Tor, Y. Antibiotics and Bacterial Resistance in the 21st Century. Perspect. Med. Chem. 2014, 6, S14459. [Google Scholar] [CrossRef]
- Wright, G.D. Q&A: Antibiotic resistance: Where does it come from and what can we do about it? BMC Boil. 2010, 8, 123. [Google Scholar]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiol. Spectr. 2016, 4, 481–511. [Google Scholar]
- Karakonstantis, S.; Kalemaki, D. Antimicrobial overuse and misuse in the community in Greece and link to antimicrobial resistance using methicillin-resistant S. aureus as an example. J. Infect. Public Health 2019, 12, 460–464. [Google Scholar] [CrossRef]
- Coculescu, B.-I. Antimicrobial resistance induced by genetic changes. J. Med. Life 2009, 2, 114–123. [Google Scholar]
- Holmes, R.K.; Jobling, M.G. Genetics. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TA, USA, 1996; Chapter 5; Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK7908/ (accessed on 8 September 2019).
- Van Duijkeren, E.; Schink, A.-K.; Roberts, M.C.; Wang, Y.; Schwarz, S. Mechanisms of Bacterial Resistance to Antimicrobial Agents. Microbiol. Spectr. 2018, 6, 51–82. [Google Scholar] [CrossRef] [PubMed]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [PubMed]
- Scaioli, G.; Gualano, M.R.; Gili, R.; Masucci, S.; Bert, F.; Siliquini, R. Antibiotic Use: A Cross-Sectional Survey Assessing the Knowledge, Attitudes and Practices amongst Students of a School of Medicine in Italy. PLoS ONE 2015, 10, e0122476. [Google Scholar] [CrossRef] [PubMed]
- Losby, J.; Wetmore, A. CDC Coffee Break: Using Likert Scale in Evaluation Survey Work. 2012. Available online: https://www.cdc.gov/dhdsp/pubs/docs/cb_february_14_2012.pdf (accessed on 30 April 2018).
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Barman, M.P.; Hazarika, J.; Kalita, A. Reliability and validity of Assamese version of EORTC QLQ-C30 Questionnaire for Studying the Quality of Life of Cancer Patients of Assam. World Appl. Sci. J. 2012, 17, 672–678. [Google Scholar]
- Keown, O.P.; Warburton, W.; Davies, S.C.; Darzi, A. Antimicrobial Resistance: Addressing The Global Threat Through Greater Awareness And Transformative Action. Health Aff. 2014, 33, 1620–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shallcross, L.J.; Howard, S.J.; Fowler, T.; Davies, S.C. Tackling the threat of antimicrobial resistance: From policy to sustainable action. Philos. Trans. R. Soc. B: Boil. Sci. 2015, 370, 20140082. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Day, 2011. Urgent Action Necessary to Safeguard Drug Treatments. 2011. Available online: http://www.who.int/mediacentre/news/releases/2011/whd_20110406/en/ (accessed on 5 May 2018).
- Haque, M.; Lutf, S.N.; Othman, N.S.; Lugova, H.; Abdullah, S.L. Empathy level among the medical students of the National Defence University of Malaysia consuming Toronto empathy scale. Acta Med. Int. 2018, 5, 24. [Google Scholar] [CrossRef]
- Haque, M.; Othman, N.S.A.O.; Lutfi, S.N.N.B.; Islam, M.Z.; Rahman, N.A.A.; Kibria, G.M.; Haque, A.T.M.E.; Majumder, M.A.A.; Gnanou, J.V. Evaluation of Out-Patient Care Educational Environment of National Defense University, Malaysia utilizing the ACLEEM Inventory. J. Basic Clin. Health Sci. 2018, 2, 45–52. [Google Scholar] [CrossRef]
- Fincham, J.E. Response Rates and Responsiveness for Surveys, Standards, and the Journal. Am. J. Pharm. Educ. 2008, 72, 43. [Google Scholar] [CrossRef]
- Haque, M.; Zulkifli, Z.; Haque, S.Z.; Kamal, Z.M.; Salam, A.; Bhagat, V.; Alattraqchi, A.G.; Rahman, N.I. Professionalism perspectives among medical students of a novel medical graduate school in Malaysia. Adv. Med. Educ. Pr. 2016, 7, 407–422. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, V.; Haque, M.; Bin Simbak, N.; Jaalam, K. Study on personality dimension negative emotionality affecting academic achievement among Malaysian medical students studying in Malaysia and overseas. Adv. Med. Educ. Pr. 2016, 7, 341–346. [Google Scholar] [Green Version]
- Harbarth, S.; Balkhy, H.H.; Goossens, H.; Jarlier, V.; Kluytmans, J.; Laxminarayan, R.; Saam, M.; Belkum, A.V.; Pittet, D. and for the World Healthcare-Associated Infections Resistance. Open Forum Infect. Dis. 2017, 4, S257. [Google Scholar]
- Hu, Y.; Wang, X.; Tucker, J.D.; Little, P.; Moore, M.; Zhou, X. Antibiotic Use Among Future Health Professionals: A Multicenter Cross-Sectional Study of Chinese Medical Student. Open Forum Infect. Dis. 2017, 4, S257. [Google Scholar] [CrossRef]
- Rathish, D.; Wijerathne, B.; Bandara, S.; Piumanthi, S.; Senevirathna, C.; Jayasumana, C.; Siribaddana, S. Pharmacology education and antibiotic self-medication among medical students: A cross-sectional study. BMC Res. Notes 2017, 10, 337. [Google Scholar] [CrossRef] [PubMed]
- Sakeena, M.H.F.; Bennett, A.A.; Jamshed, S.; Mohamed, F.; Herath, D.R.; Gawarammana, I.; McLachlan, A.J. Investigating knowledge regarding antibiotics and antimicrobial resistance among pharmacy students in Sri Lankan universities. BMC Infect. Dis. 2018, 18, 209. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Petty, R.E.; Smith, S.M.; Crites, S.L. Understanding knowledge effects on attitude-behavior consistency: The role of relevance, complexity, and amount of knowledge. J. Pers. Soc. Psychol. 2006, 90, 556–577. [Google Scholar] [CrossRef]
- Albarracin, D.; Wyer, R.S. The cognitive impact of past behavior: Influences on beliefs, attitudes, and future behavioral decisions. J. Pers. Soc. Psychol. 2000, 79, 5–22. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; MacDonald, T.K.; Wegener, D.T. The Structure of Attitudes from. In The Handbook of Attitudes; Albarracín, D., Johnson, B.T., Zanna, M.P., Eds.; Psychology Press: Hove, UK, 2014; pp. 79–124. Available online: https://www.routledgehandbooks.com/doi/10.4324/9781410612823.ch3 (accessed on 9 May 2018).
- Ajzen, I. Nature and operation of attitudes. Annu. Rev. Psychol. 2001, 52, 27–58. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Division of Behavioral and Social Sciences and Education; Board on Children, Youth, and Families; Committee on Supporting the Parents of Young Children. 2. Parenting Knowledge, Attitudes, and Practices. In Parenting Matters: Supporting Parents of Children Ages 0–8; Breiner, H., Ford, M., Gadsden, V.L., Eds.; National Academies Press: Washington, DC, USA, 21 November 2016; Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK402020/ (accessed on 9 May 2018).
- Institute of Medicine. 5. Individuals and Families: Models and Interventions. In Committee on Health and Behavior: Research, Practice, and Policy. Health and Behavior: The Interplay of Biological, Behavioral, and Societal Influences; National Academies Press: Washington, DC, USA, 2001; Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK43749/ (accessed on 9 May 2018).
- McKay, R.; Mah, A.; Law, M.R.; McGrail, K.; Patrick, D.M. Systematic Review of Factors Associated with Antibiotic Prescribing for Respiratory Tract Infections. Antimicrob. Agents Chemother. 2016, 60, 4106–4118. [Google Scholar] [CrossRef] [Green Version]
- Rademacher, J.; Welte, T. New antibiotics—standstill or progress. Med. Klin. Intensivmed. Notfmed. 2017, 112, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Projan, S.J. Why is big Pharma getting out of antibacterial drug discovery? Curr. Opin. Microbiol. 2003, 6, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Projan, S.J.; Shlaes, D.M. Antibacterial drug discovery: Is it all downhill from here? Clin. Microbiol. Infect. 2004, 10, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Shlaes, D. The abandonment of antibacterials: Why and wherefore? Curr. Opin. Pharmacol. 2003, 3, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Shlaes, D.M.; Sahm, D.; Opiela, C.; Spellberg, B. The FDA Reboot of Antibiotic Development. Antimicrob. Agents Chemother. 2013, 57, 4605–4607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spellberg, B.; Guidos, R.; Gilbert, D.; Bradley, J.; Boucher, H.W.; Scheld, W.M.; Bartlett, J.G.; Edwards, J.; America, T.I.D.S.O. The Epidemic of Antibiotic-Resistant Infections: A Call to Action for the Medical Community from the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Wellcome Trust. New Antibiotic Approved for Drug-Resistant Infections. 2018. Available online: https://wellcome.ac.uk/news/new-antibiotic-approved-drug-resistant-infections (accessed on 3 August 2019).
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious diseases society of America and the society for healthcare epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Bettiol, E.; Harbarth, S. Development of new antibiotics: Taking off finally? Swiss Med. Wkly. 2015, 145, w14167. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Hills, H.; Seitz, L.-T.; Perry, A.; Ashiru-Oredope, D. Assessing the Knowledge, Attitudes and Behaviors of Human and Animal Health Students towards Antibiotic Use and Resistance: A Pilot Cross-Sectional Study in the UK. Antibiotics 2018, 7, 10. [Google Scholar] [CrossRef]
- Topor, G.; Grosu, I.-A.; Ghiciuc, C.M.; Strat, A.L.; Lupuşoru, C.E. Awareness about antibiotic resistance in a self-medication user group from Eastern Romania: A pilot study. PeerJ 2017, 5, e3803. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.L. Medical Students’ Attitude towards Antibiotics Misuse in Hong Kong. Master’s Thesis, Public Health, the University of Hong Kong, Hong Kong, China, 2012. [Google Scholar]
- Mazinska, B.; Strużycka, I.; Hryniewicz, W. Surveys of public knowledge and attitudes with regard to antibiotics in Poland: Did the European Antibiotic Awareness Day campaigns change attitudes? PLoS ONE 2017, 12, e0172146. [Google Scholar] [CrossRef] [PubMed]
- Horvat, O.J.; Tomas, A.D.; Kusturica, M.M.P.; Savkov, A.V.; Bukumirić, D.U.; Tomić, Z.S.; Sabo, A.J. Is the level of knowledge a predictor of rational antibiotic use in Serbia? PLoS ONE 2017, 12, e0180799. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.K.; Banu, G.K.K.R. Antibiotic Resistance and Usage—A Survey on the Knowledge, Attitude, Perceptions and Practices among the Medical Students of a Southern Indian Teaching Hospital. J. Clin. Diagn. Res. 2013, 7, 1613–1616. [Google Scholar]
- World Health Organization. How to Stop Antibiotic Resistance? Here’s a WHO Prescription. 2015. Available online: http://www.who.int/mediacentre/commentaries/stop-antibiotic-resistance/en/ (accessed on 9 May 2018).
- Leekha, S.; Terrell, C.L.; Edson, R.S. General Principles of Antimicrobial Therapy. Mayo Clin. Proc. 2011, 86, 156–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De With, K.; Allerberger, F.; Amann, S.; Apfalter, P.; Brodt, H.-R.; Eckmanns, T.; Fellhauer, M.; Geiss, H.K.; Janata, O.; Krause, R.; et al. Strategies to enhance rational use of antibiotics in hospital: A guideline by the German Society for Infectious Diseases. Infection 2016, 44, 395–439. [Google Scholar] [CrossRef]
- Cornaglia, G.; Hryniewicz, W.; Jarlier, V.; Kahlmeter, G.; Mittermayer, H.; Stratchounski, L.; Baquero, F. ESCMID Study Group for Antimicrobial Resistance Surveillance. European recommendations for antimicrobial resistance surveillance. Clin. Microbiol. Infect. 2004, 10, 349–383. [Google Scholar] [CrossRef] [PubMed]
- Llewelyn, M.J.; Fitzpatrick, J.M.; Darwin, E.; Crine, S.T.; Gorton, C.; Paul, J.; Peto, T.; Yardley, L.; Hopkins, S.; Walker, A.S. The antibiotic course has had its day. BMJ 2017, 358, j3418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Health 2016, 9, 211–217. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Frequency | Percentage | |
|---|---|---|
| Gender | ||
| Male | 110 | 53.9 |
| Female | 94 | 46.1 |
| Race | ||
| Malay | 140 | 68.9 |
| Chinese | 18 | 8.8 |
| Indian | 41 | 20.1 |
| Others | 5 | 2.5 |
| Had relatives working in health field | ||
| Yes | 57 | 27.9 |
| No | 147 | 72.1 |
| Year of study | ||
| 1 | 56 | 27.5 |
| 2 | 39 | 19.1 |
| 3 | 39 | 19.1 |
| 4 | 33 | 16.2 |
| 5 | 37 | 18.1 |
| Type of admission a | ||
| Cadet officer | 100 | 49.3 |
| Territorial army | 28 | 13.8 |
| Civil student | 75 | 36.9 |
| Latest academic grade | ||
| A | 20 | 9.8 |
| B | 150 | 73.5 |
| C | 34 | 16.7 |
| Questions on Knowledge about Antibiotic | Totally Disagree n (%) | Disagree n (%) | Agree n (%) | Totally Agree n (%) |
|---|---|---|---|---|
| ● Penicillin or Amoxicillin are antibiotics a | 9 (4.4) | 14 (6.9) | 31 (15.3) | 149 (73.4) |
| ● Aspirin is an antibiotic | 142 (69.6) | 24 (11.8) | 29 (14.2) | 9 (4.4) |
| ● Paracetamol is an antibiotic | 157 (77.0) | 16 (7.8) | 15 (7.4) | 16 (7.8) |
| ● Antibiotics are useful for bacterial infections (e.g., tuberculosis) | 11 (5.4) | 13 (6.4) | 31 (15.2) | 149 (73.0) |
| ● Antibiotics are useful for viral infections (e.g., flu) | 108 (52.9) | 26 (12.7) | 29 (14.2) | 41 (20.1) |
| ● Antibiotics are indicated to reduce any kind of pain and inflammation | 102 (50.0) | 42 (20.6) | 37 (18.1) | 23 (11.3) |
| ● Antibiotics can kill “good bacteria” present in our system | 29 (14.2) | 53 (26.0) | 54 (26.5) | 68 (33.3) |
| ● Antibiotics can cause secondary infections after killing good bacteria present in our system | 26 (12.7) | 63 (30.9) | 59 (28.9) | 56 (27.5) |
| ● Antibiotics can cause allergic reactions | 5 (2.5) | 19 (9.3) | 57 (27.9) | 123 (60.3) |
| Totally Disagree n (%) | Disagree n (%) | Agree n (%) | Totally Agree n (%) | |
|---|---|---|---|---|
| ● Antibiotic resistance is a phenomenon for which a bacterium loses its sensitivity to an antibiotic. | 6 (2.9) | 20 (9.8) | 41 (20.1) | 137 (67.2) |
| ● Misuse of antibiotics can lead to a loss of sensitivity of an antibiotic to a specific pathogen. | 5 (2.5) | 24 (11.8) | 52 (25.5) | 123 (60.3) |
| ● If symptoms improve the full course of antibiotics is completed, you can stop taking it. | 137 (67.2) | 22 (10.8) | 25 (12.3) | 20 (9.8) |
| Questionnaire on Attitudes Regarding Antibiotic Consumption | Yes n (%) | No n (%) |
|---|---|---|
| ● Do you usually take antibiotics for cold or sore throat? | 46 (22.5) | 158 (77.5) |
| ● Do you usually take antibiotics for fever? | 80 (39.2) | 124 (60.8) |
| ● Do you usually stop taking antibiotics when you start feeling better? | 67 (32.8) | 137 (67.2) |
| ● Do you take antibiotic only when prescribed by the doctor? | 179 (87.7) | 25 (12.3) |
| ● Do you keep leftovers antibiotics at home because they might be useful in the future? | 68 (33.3) | 136 (66.7) |
| ● Do you use leftovers antibiotics when you have a cold, sore throat or flu without consulting your doctor? | 46 (22.5) | 158 (77.5) |
| ● Do you buy antibiotics without a medical receipt? | 23 (11.3) | 181 (88.7) |
| ● Have you ever started an antibiotic therapy after a simple doctor call, without a proper medical examination? | 34 (16.7) | 170 (83.3) |
| Variables | Use Antibiotic in the Previous Year | Chi-Square Value (df a) | p-Value | |
|---|---|---|---|---|
| Yes n (%) | No n (%) | |||
| Gender | ||||
| Male | 75 (56.4) | 35 (49.3) | 0.938 | 0.333 |
| Female | 58 (43.6) | 36 (50.7 | (1) | |
| Race | ||||
| Malay | 88 (66.2) | 52 (73.2) | 1.076 | 0.300 |
| Others b | 45 (33.8) | 19 (26.8) | (1) | |
| Had relatives working in the health field | ||||
| Yes | 39 (29.3) | 18 (25.4) | 0.363 | 0.547 |
| No | 94 (70.7) | 53 (74.6) | (1) | |
| Year of study | ||||
| 1 | 44 (33.1) | 12 (16.9) | 11.270 | 0.024 |
| 2 | 28 (21.1) | 11 (15.5) | (4) | |
| 3 | 25 (18.8) | 14 (19.7) | ||
| 4 | 16 (12.0) | 17 (23.9) | ||
| 5 | 20 (15.0) | 17 (23.9) | ||
| Type of admission c | ||||
| Cadet officer | 57 (43.2) | 43 (60.6) | 5.996 | 0.050 |
| Territorial army | 19 (14.4) | 9 (12.7) | (2) | |
| Civil student | 56 (42.4) | 19 (26.8) | ||
| Latest academic grade | ||||
| A | 13 (9.8) | 7 (9.9) | 2.770 | 0.250 |
| B | 102 (76.7) | 48 (67.6) | (2) | |
| C | 18 (13.5) | 16 (22.5) | ||
| Variables | Total Knowledge Score | Total Attitude Score | ||
|---|---|---|---|---|
| r-Value | p-Value | r-Value | p-Value | |
| Age | 0.568 | <0.001 | 0.252 | <0.001 |
| Year of Study | 0.572 | <0.001 | 0.258 | <0.001 |
| Grade | 0.038 | 0.591 | −0.112 | 0.109 |
| Variables | Total Knowledge Score | Total Attitude Score | ||
|---|---|---|---|---|
| Mean (SD *) | p-Value | Mean (SD) | p-Value | |
| Gender | ||||
| Male (n = 110) | 39.7 (5.59) | 0.598 | 14.0 (1.89) | 0.348 |
| Female (n = 94) | 39.2 (6.43) | 14.2 (1.75) | ||
| Had relatives working in health field | ||||
| Yes (n = 57) | 39.7 (5.50) | 0.688 | 14.1 (1.81) | 0.819 |
| No (n = 147) | 39.4 (6.17) | 14.1 (1.84) | ||
| Variables | Stopping Antibiotic when Feeling Better | Keeping Leftover Antibiotics for Future Use | Using Leftover Antibiotics without a Doctor’s Consultation | |||
|---|---|---|---|---|---|---|
| OR (95% C.I.) | p-Value | OR (95% C.I.) | p-Value | OR (95% C.I.) | p-Value | |
| Age * | 0.782 (0.636, 0.961) | 0.019 | 0.929 (0.762, 1.132) | 0.463 | 0.767 (0.606, 0.971) | 0.028 |
| Year of study * | 0.767 (0.622, 0.946) | 0.013 | 0.926 (0.758, 1.132) | 0.456 | 0.769 (0.606, 0.976) | 0.030 |
| Exam grade * | 1.228 (0.692, 2.181) | 0.483 | 1.447 (0.813, 2.576) | 0.209 | 1.515 (0.793, 2.894) | 0.208 |
| Total knowledge Score * | 0.906 (0.860, 0.954) | <0.001 ** | 0.972 (0.926, 1.021) | 0.257 | 0.880 (0.829, 0.934) | <0.001 ** |
| Gender | ||||||
| Male # | 1 | 1.000 | 1 | 1.000 | 1 | 1.000 |
| Female | 0.827 (0.460, 1.485) | 0.525 | 0.789 (0.440, 1.415) | 0.427 | 1.622 (0.826, 3.185) | 0.160 |
| Relatives working in health-related field | ||||||
| No # | 1 | 1.000 | 1 | 1.000 | 1 | 1.000 |
| Yes | 1.533 (0.777, 3.024) | 0.218 | 0.806 (0.425, 1.528) | 0.508 | 0.855 (0.416, 1.754) | 0.669 |
| Heard about antibiotic resistance | ||||||
| No # | 1 | 1.000 | 1 | 1.000 | 1 | 1.000 |
| Yes | 2.508 (1.075, 5.850) | 0.033 | 1.391 (0.589, 3.284) | 0.452 | 2.159 (0.884, 5.274) | 0.091 |
| Discussed about antibiotic resistance | ||||||
| No # | 1 | 1.000 | 1 | 1.000 | 1 | 1.000 |
| Yes | 1.538 (0.832, 2.842) | 0.170 | 1.000 (0.537, 1.863) | 1.000 | 1.662 (0.843, 3.277) | 0.142 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haque, M.; Rahman, N.A.A.; McKimm, J.; Sartelli, M.; Kibria, G.M.; Islam, M.Z.; Binti Lutfi, S.N.N.; Binti Othman, N.S.A.; Binti Abdullah, S.L. Antibiotic Use: A Cross-Sectional Study Evaluating the Understanding, Usage and Perspectives of Medical Students and Pathfinders of a Public Defence University in Malaysia. Antibiotics 2019, 8, 154. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030154
Haque M, Rahman NAA, McKimm J, Sartelli M, Kibria GM, Islam MZ, Binti Lutfi SNN, Binti Othman NSA, Binti Abdullah SL. Antibiotic Use: A Cross-Sectional Study Evaluating the Understanding, Usage and Perspectives of Medical Students and Pathfinders of a Public Defence University in Malaysia. Antibiotics. 2019; 8(3):154. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030154
Chicago/Turabian StyleHaque, Mainul, Nor Azlina A. Rahman, Judy McKimm, Massimo Sartelli, Golam Mohammad Kibria, Md Zakirul Islam, Siti Nur Najihah Binti Lutfi, Nur Syamirah Aishah Binti Othman, and Shahidah Leong Binti Abdullah. 2019. "Antibiotic Use: A Cross-Sectional Study Evaluating the Understanding, Usage and Perspectives of Medical Students and Pathfinders of a Public Defence University in Malaysia" Antibiotics 8, no. 3: 154. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8030154