Impact of Antibiotic Prescribing Patterns on Susceptibilities of Uropathogens in Children below 24 Months Old

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
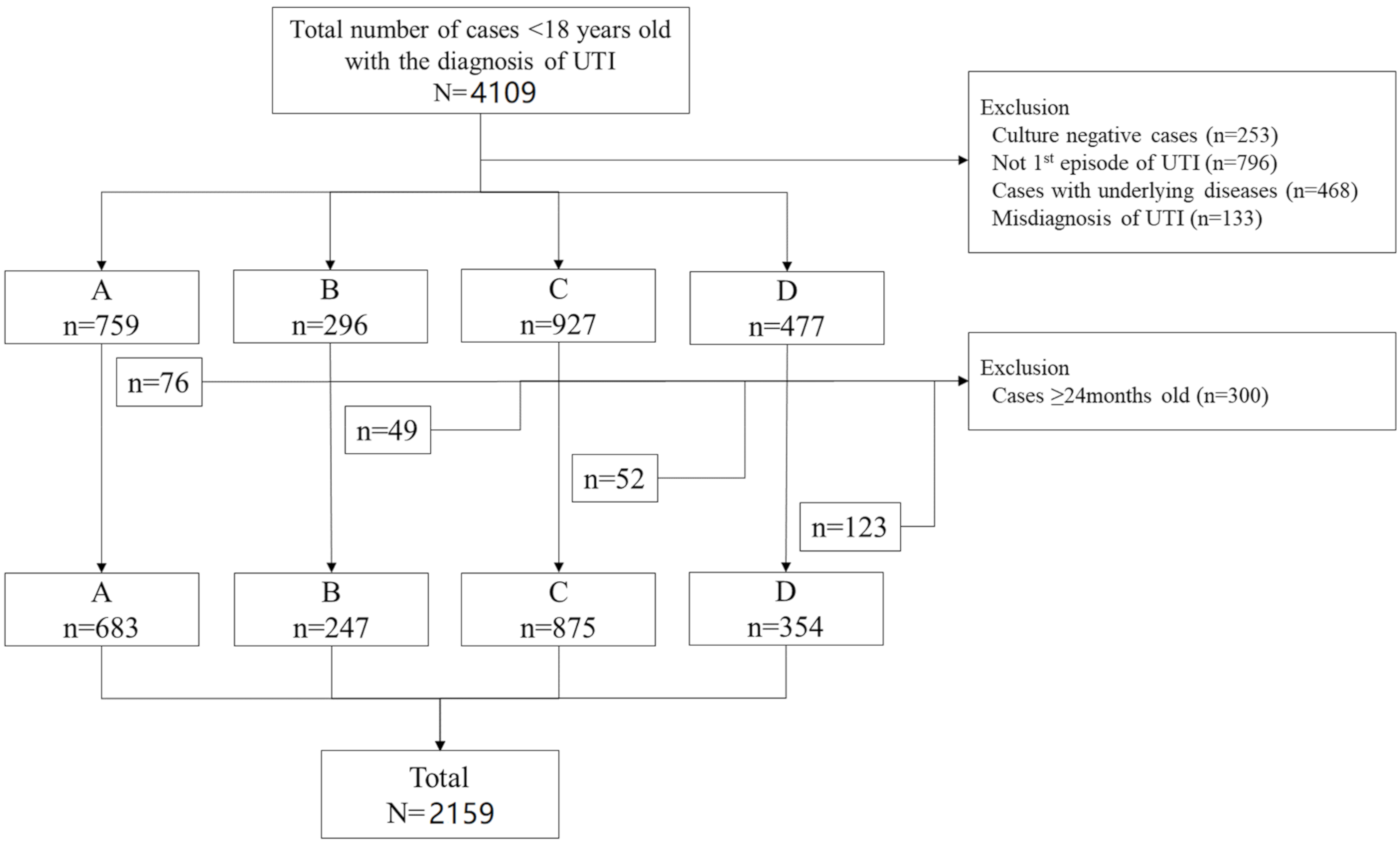
2.1. Demographics and Etiology
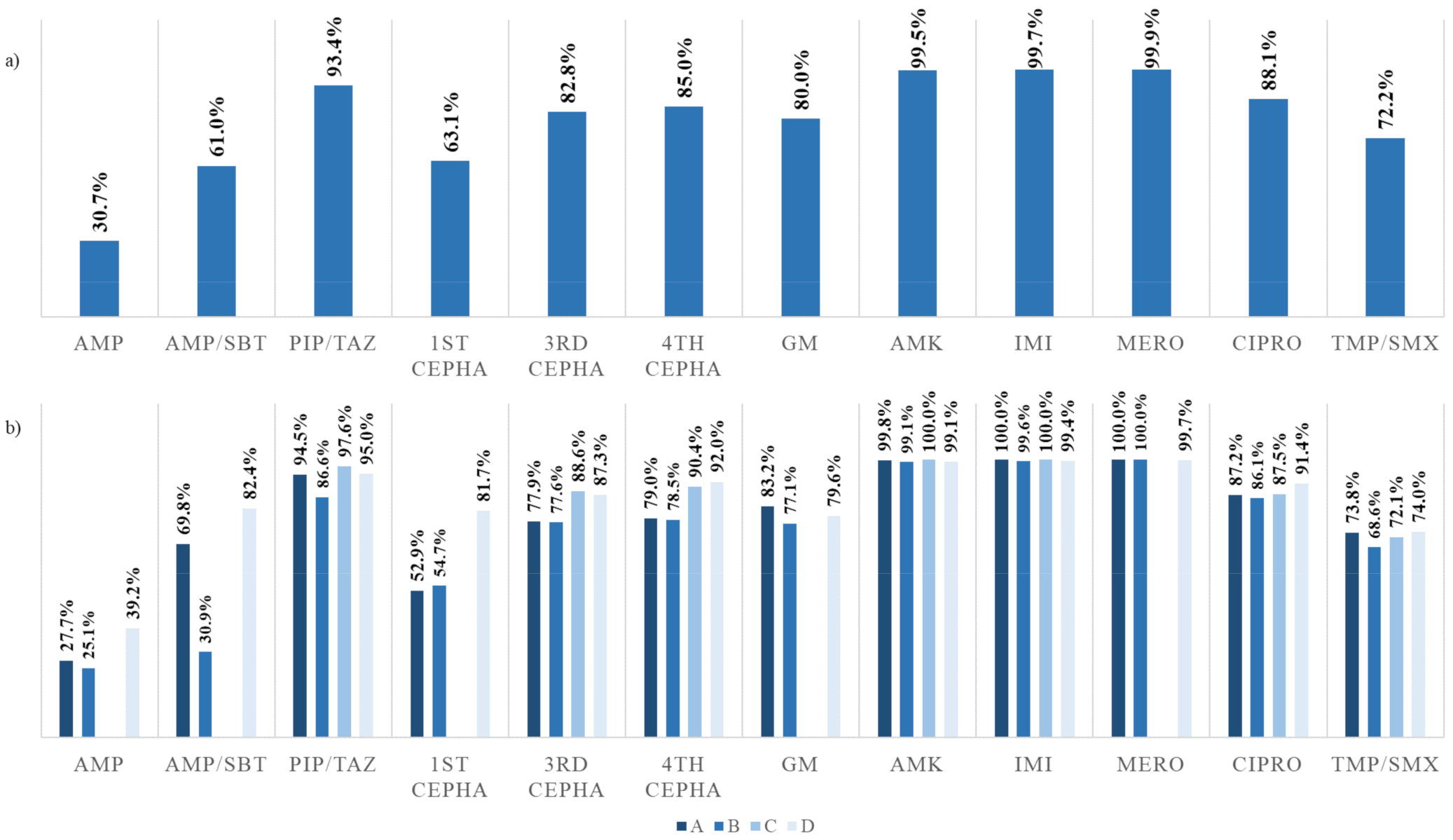
2.2. Antimicrobial Susceptibility
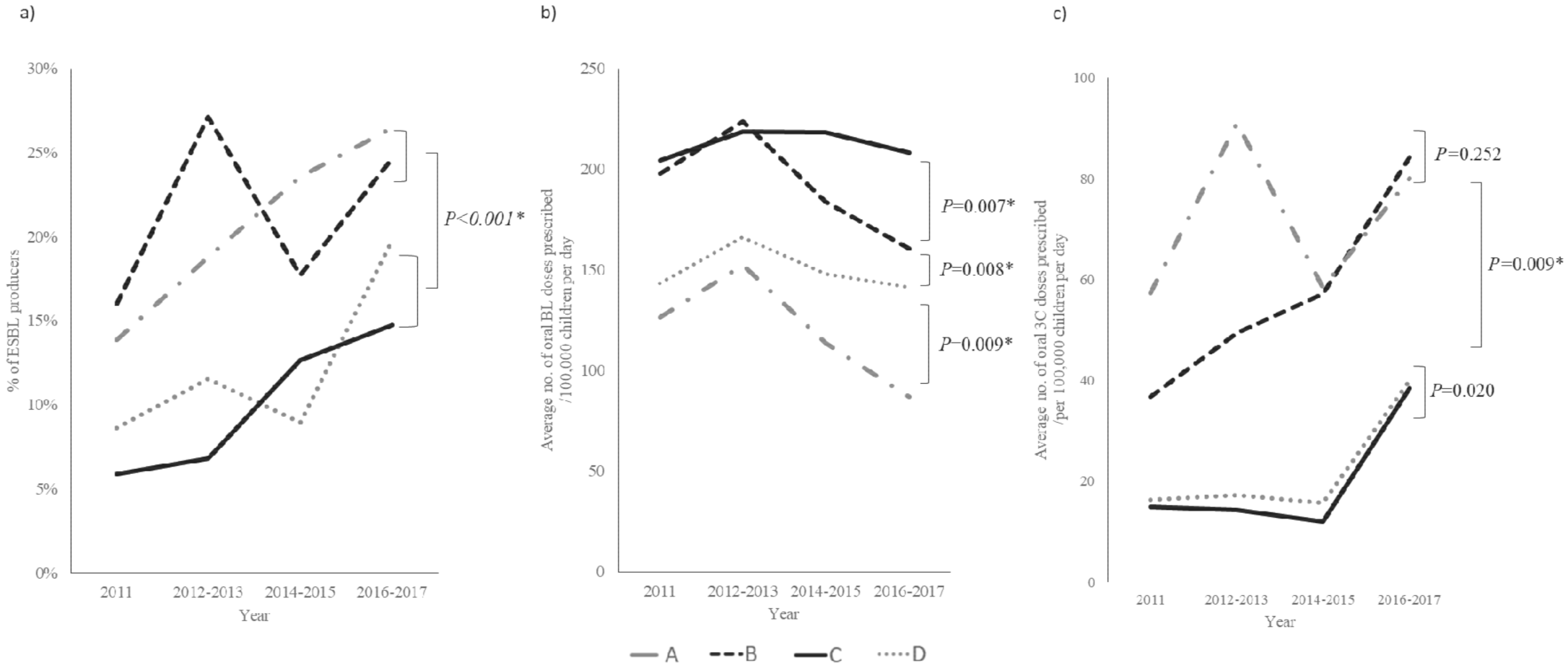
2.3. Multidrug Resistance and ESBL-Producing Enteric Gram-Negative Rods
2.4. Factors Associated with an Increased Risk for UTIs with ESBL-Producing Pathogens
2.5. Total Amount of Antibiotics Prescribed in Each of the Regions That the Four Hospitals Are Located
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Study Protocol and Data Collection
4.3. Microbiology and Antimicrobial Susceptibility
4.4. Regional Population and Antibiotics Prescribing Patterns in CHILDREN below 24 Months Old
4.5. Ethical Consideration Statement
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Jakobsson, B.; Svensson, L. Transient pyelonephritic changes on 99mTechnetium-dimercaptosuccinic acid scan for at least five months after infection. Acta Paediatr. 1997, 86, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, M.G.; Lambert, H.J.; Vernon, S.J.; Hunter, E.W.; Keir, M.J.; Matthews, J.N.S. Does prompt treatment of urinary tract infection in preschool children prevent renal scarring: Mixed retrospective and prospective audits. Arch. Dis. Child. 2014, 99, 342–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, N.; Morone, N.E.; Bost, J.E.; Farrell, M.H. Prevalence of urinary tract infection in childhood: A meta-analysis. Pediatr. Infect. Dis. J. 2008, 27, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Jayaweera, J.A.A.S.; Reyes, M. Antimicrobial misuse in pediatric urinary tract infections: Recurrences and renal scarring. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 27. [Google Scholar] [CrossRef] [Green Version]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [Green Version]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Fitzgerald, A.; Mori, R.; Lakhanpaul, M.; Tullus, K. Antibiotics for treating lower urinary tract infection in children. Cochrane Database Syst. Rev. 2012, 8, CD006857. [Google Scholar] [CrossRef]
- Harada, K.; Asai, T. Role of antimicrobial selective pressure and secondary factors on antimicrobial resistance prevalence in Escherichia coli from food-producing animals in Japan. J. Biomed. Biotechnol. 2010, 2010, 180682. [Google Scholar] [CrossRef] [Green Version]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef] [Green Version]
- Montini, G.; Toffolo, A.; Zucchetta, P.; Dall’Amico, R.; Gobber, D.; Calderan, A.; Maschio, F.; Pavanello, L.; Molinari, P.P.; Scorrano, D.; et al. Antibiotic treatment for pyelonephritis in children: Multicentre randomised controlled non-inferiority trial. BMJ 2007, 335, 386. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.; Goldman, J.L. Safety Concerns Surrounding Quinolone Use in Children. J. Clin. Pharmacol. 2016, 56, 1060–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, M.A.; Schutze, G.E. Committee on Infectious Diseases the Use of Systemic and Topical Fluoroquinolones. Pediatrics 2016, 138, e20162706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsammani, M.A.; Ahmed, M.I.; Abdelatif, N.F. Bacterial Uropathogens Isolates and Antibiograms in Children Under 5 Years of Age. Med. Arch. 2014, 68, 239–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasfi, R.; Hamed, S.M.; Amer, M.A.; Fahmy, L.I. Proteus mirabilis Biofilm: Development and Therapeutic Strategies. Front. Cell. Infect. Microbiol. 2020, 10, 414. [Google Scholar] [CrossRef]
- Mittal, R.; Aggarwal, S.; Sharma, S.; Chhibber, S.; Harjai, K. Urinary tract infections caused by Pseudomonas aeruginosa: A minireview. J. Infect. Public Health 2009, 2, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Lukac, P.J.; Bonomo, R.A.; Logan, L.K. Extended-spectrum β-lactamase-producing Enterobacteriaceae in children: Old foe, emerging threat. Clin. Infect. Dis. 2015, 60, 1389–1397. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.Y.; Lee, S.-J.; Lee, D.S.; Yoo, J.M.; Choe, H.-S. Microbiological Characteristics of Unresolved Acute Uncomplicated Cystitis. Microb. Drug Resist. 2016, 22, 387–391. [Google Scholar] [CrossRef]
- Kim, W.B.; Cho, K.H.; Lee, S.W.; Yang, H.J.; Yun, J.H.; Lee, K.W.; Kim, J.M.; Kim, Y.H.; Jeon, Y.S.; Kim, M.E. Recent Antimicrobial Susceptibilities for Uropathogenic Escherichia coli in Patients with Community Acquired Urinary Tract Infections: A Multicenter Study. Urogenit. Tract Infect. 2017, 12, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Roberts, K.B. Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [Green Version]
- National Collaborating Centre for Women’s and Children’s Health (UK). Urinary Tract Infection in Children: Diagnosis, Treatment and Long-Term Management; RCOG Press: London, UK, 2007. [Google Scholar]
- Flokas, M.E.; Detsis, M.; Alevizakos, M.; Mylonakis, E. Prevalence of ESBL-producing Enterobacteriaceae in paediatric urinary tract infections: A systematic review and meta-analysis. J. Infect. 2016, 73, 547–557. [Google Scholar] [CrossRef]
- Kolář, M.; Urbánek, K.; Látal, T. Antibiotic selective pressure and development of bacterial resistance. Int. J. Antimicrob. Agents 2001, 17, 357–363. [Google Scholar] [CrossRef]
- Lee, J.; Pai, H.; Kim, Y.K.; Kim, N.H.; Eun, B.W.; Kang, H.J.; Park, K.H.; Choi, E.H.; Shin, H.Y.; Kim, E.C.; et al. Control of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae in a children’s hospital by changing antimicrobial agent usage policy. J. Antimicrob. Chemother. 2007, 60, 629–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bantar, C.; Vesco, E.; Heft, C.; Salamone, F.; Krayeski, M.; Gomez, H.; Coassolo, M.A.; Fiorillo, A.; Franco, D.; Arango, C.; et al. Replacement of broad-spectrum cephalosporins by piperacillin-tazobactam: Impact on sustained high rates of bacterial resistance. Antimicrob. Agents Chemother. 2004, 48, 392–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Round, J.L.; Mazmanian, S.K. The gut microbiota shapes intestinal immune responses during health and disease. Nat. Rev. Immunol. 2009, 9, 313–323. [Google Scholar] [CrossRef]
- Herindrainy, P.; Rabenandrasana, M.A.N.; Andrianirina, Z.Z.; Rakotoarimanana, F.M.J.; Padget, M.; De Lauzanne, A.; Ndir, A.; Kermorvant-Duchemin, E.; Garin, B.; Piola, P.; et al. Acquisition of extended spectrum beta-lactamase-producing enterobacteriaceae in neonates: A community based cohort in Madagascar. PLoS ONE 2018, 13, e0193325. [Google Scholar] [CrossRef] [Green Version]
- Mughini-Gras, L.; Dorado-García, A.; van Duijkeren, E.; van den Bunt, G.; Dierikx, C.M.; Bonten, M.J.M.; Bootsma, M.C.J.; Schmitt, H.; Hald, T.; Evers, E.G.; et al. Attributable sources of community-acquired carriage of Escherichia coli containing β-lactam antibiotic resistance genes: A population-based modelling study. Lancet Planet. Health 2019, 3, e357–e369. [Google Scholar] [CrossRef] [Green Version]
- Birgy, A.; Cohen, R.; Levy, C.; Bidet, P.; Courroux, C.; Benani, M.; Thollot, F.; Bingen, E. Community faecal carriage of extended-spectrum beta-lactamase-producing Enterobacteriaceae in french children. BMC Infect. Dis. 2012, 12, 315. [Google Scholar] [CrossRef] [Green Version]
- Kaarme, J.; Molin, Y.; Olsen, B.; Melhus, A. Prevalence of extended-spectrum beta-lactamase-producing Enterobacteriaceae in healthy Swedish preschool children. Acta Paediatr. 2013, 102, 655–660. [Google Scholar] [CrossRef]
- Fernández-Reyes, M.; Vicente, D.; Gomariz, M.; Esnal, O.; Landa, J.; Oñate, E.; Pérez-Trallero, E. High Rate of Fecal Carriage of Extended-Spectrum-β-Lactamase-Producing Escherichia coli in Healthy Children in Gipuzkoa, Northern Spain. Antimicrob. Agents Chemother. 2014, 58, 1822–1824. [Google Scholar] [CrossRef] [Green Version]
- Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Fifth Informational Supplement; [CLSI document M100-S25]; Clinical and Laboratory Standards Institue: Annapolis Junction, MD, USA, 2019.




{kind=link}
{kind=link}
{kind=link}
| No. of Cases (%) | ||||||
|---|---|---|---|---|---|---|
| A | B | C | D | Total | P * | |
| (N = 683) | (N = 247) | (N = 875) | (N = 354) | (N = 2159) | ||
| Sex, male | 457 (66.9) | 166 (67.2) | 628 (71.8) | 254 (71.8) | 1505 (69.7) | 0.126 |
| Median age, months (IQR) | 4 (2–6) | 4.6 (2.9–6.6) | 3 (2–5) | 10.8 (7.4–14.8) | 4 (2.3–7.3) | <0.001 |
| Year of diagnosis | ||||||
| 2011 | 97 (14.2) | 25 (10.1) | 115 (13.1) | 44 (12.4) | 281 (13.0) | 0.424 |
| 2012 | 64 (9.3) | 25 (10.1) | 130 (14.9) | 53 (15.0) | 272 (12.6) | 0.003 |
| 2013 | 103 (15.1) | 28 (11.3) | 89 (10.2) | 45 (12.7) | 265 (12.3) | 0.031 |
| 2014 | 95 (13.9) | 34 (13.8) | 117 (13.4) | 50 (14.1) | 296 (13.7) | 0.984 |
| 2015 | 113 (16.5) | 43 (17.4) | 133 (15.2) | 56 (15.8) | 345 (16.0) | 0.815 |
| 2016 | 83 (12.2) | 50 (20.2) | 156 (17.8) | 50 (14.1) | 339 (15.7) | 0.003 |
| 2017 | 128 (18.7) | 42 (17.0) | 135 (15.4) | 56 (15.8) | 361 (16.7) | 0.352 |
| Pathogen | ||||||
| Escherichia coli | 614 (89.9) | 210 (85.0) | 813 (92.9) | 336 (94.9) | 1973 (91.4) | <0.001 |
| Klebsiella spp. | 28 (4.1) | 13 (5.3) | 27 (3.1) | 3 (0.8) | 71 (3.3) | 0.011 |
| Enterobacter spp. | 25 (3.7) | 0 | 19 (2.2) | 3 (0.8) | 47 (2.2) | 0.001 |
| Enterococcus spp. | 5 (0.7) | 14 (5.7) | 5 (0.6) | 9 (2.5) | 33 (1.5) | <0.001 |
| Proteus mirabilis | 3 (0.4) | 2 (0.8) | 2 (0.2) | 0 | 7 (0.3) | - |
| Streptococcus spp. | 2 (0.3) | 1 (0.4) | 2 (0.2) | 1 (0.3) | 6 (0.3) | 0.973 |
| Serratia spp. | 2 (0.3) | 2 (0.8) | 2 (0.2) | 0 | 6 (0.3) | - |
| Citrobacter spp. | 0 | 1 (0.4) | 4 (0.5) | 0 | 5 (0.2) | - |
| Morganella morganii | 2 (0.3) | 1 (0.4) | 0 | 0 | 3 (0.1) | - |
| Staphylococcus spp. | 1 (0.1) | 2 (0.8) | 0 | 0 | 3 (0.1) | - |
| Raoultella planticola | 1 (0.1) | 0 | 1 (0.1) | 1 (0.3) | 3 (0.1) | - |
| Pseudomonas aeruginosa | 0 | 0 | 0 | 1 (0.3) | 1 (0.0) | - |
| Yersinia enterocolitica | 0 | 1 (0.4) | 0 | 0 | 1 (0.0) | - |
| Year | Total (N = 2044) | ESBL (N = 310) | % of ESBL | OR | 95% CI | P |
|---|---|---|---|---|---|---|
| 2011 | 258 | 26 | 10.1 | R | ||
| 2012–2013 | 517 | 61 | 11.8 | 1.2 | 0.7–1.9 | 0.475 |
| 2014–2015 | 595 | 95 | 16.0 | 1.7 | 1.1–2.7 | 0.025 |
| 2016–2017 | 674 | 128 | 19.0 | 2.2 | 1.4–3.5 | 0.001 |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | OR (95% CI) | P | OR | OR (95% CI) | P | |||
| Lower | Upper | Lower | Upper | |||||
| Sex | 1.0 | 0.8 | 1.3 | 0.858 | ||||
| Age | 1.0 | 1.0 | 1.0 | 0.206 | ||||
| Hospital | ||||||||
| A | 1.8 | 1.3 | 2.7 | 0.001 | 1.8 | 1.2 | 2.6 | 0.002 |
| B | 1.6 | 1.0 | 2.6 | 0.035 | 1.6 | 1.0 | 2.5 | 0.054 |
| C | 0.8 | 0.6 | 1.2 | 0.304 | ||||
| D | R | |||||||
| Year | 1.1 | 1.1 | 1.2 | <0.001 | 1.1 | 1.1 | 1.2 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.Y.; Kang, H.M.; Kwak, E.M.; Rhim, J.-W.; Ahn, Y.H.; Lee, H.; Jeong, D.C.; Kang, J.H. Impact of Antibiotic Prescribing Patterns on Susceptibilities of Uropathogens in Children below 24 Months Old. Antibiotics 2020, 9, 915. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120915
Park JY, Kang HM, Kwak EM, Rhim J-W, Ahn YH, Lee H, Jeong DC, Kang JH. Impact of Antibiotic Prescribing Patterns on Susceptibilities of Uropathogens in Children below 24 Months Old. Antibiotics. 2020; 9(12):915. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120915
Chicago/Turabian StylePark, Ji Young, Hyun Mi Kang, Eun Min Kwak, Jung-Woo Rhim, Yo Han Ahn, Hyunju Lee, Dae Chul Jeong, and Jin Han Kang. 2020. "Impact of Antibiotic Prescribing Patterns on Susceptibilities of Uropathogens in Children below 24 Months Old" Antibiotics 9, no. 12: 915. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9120915