
Relationship between Physical Activity, Oxidative Stress, and Total Plasma Antioxidant Capacity in Spanish Children from the GENOBOX Study

 , ,
, ,  , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Clinical and Anthropometric Examination
2.3. Blood Sampling
2.4. Accelerometry
2.5. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- García-Hermoso, A.; Ezzatvar, Y.; Ramírez-Vélez, R.; Olloquequi, J.; Izquierdo, M. Is device-measured vigorous-intensity physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis. J. Sport Health Sci. 2020. [Google Scholar] [CrossRef]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef] [Green Version]
- Watson, T.A.; MacDonald-Wicks, L.K.; Garg, M.L. Oxidative stress and antioxidants in athletes undertaking regular exercise training. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Sies, H. Oxidative stress: Concept and some practical aspects. Antioxidants 2020, 9, 852. [Google Scholar] [CrossRef]
- Basu, S. F2-isoprostanes in human health and diseases: From molecular mechanisms to clinical implications. Antioxid. Redox Signal. 2008, 10, 1405–1434. [Google Scholar] [CrossRef]
- Roberts, L.J.; Morrow, J.D. Measurement of F2-isoprostanes as an index of oxidative stress in vivo. Free Radic. Biol. Med. 2000, 28, 505–513. [Google Scholar] [CrossRef]
- Kasai, H.; Crain, P.F.; Kuchino, Y.; Nishimura, S.; Ootsuyama, A.; Tanooka, H. Formation of 8-hydroxyguanine moiety in cellular dna by agents producing oxygen radicals and evidence for its repair. Carcinogenesis 1986, 7, 1849–1851. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Yamauchi, H.; Hasui, Y.; Kurashige, J.; Ochi, H.; Yoshida, K. Quantitative determination of urinary 8-hydroxydeoxyguanosine (8-OH-dg) by using ELISA—PubMed. Res. Commun. Mol. Pathol. Pharmacol. 2000, 107, 39–44. [Google Scholar] [PubMed]
- Urso, M.L.; Clarkson, P.M. Oxidative stress, exercise, and antioxidant supplementation. Toxicology 2003, 189, 41–54. [Google Scholar] [CrossRef]
- Morandi, A.; Corradi, M.; Piona, C.; Fornari, E.; Puleo, R.; Maffeis, C. Systemic anti-oxidant capacity is inversely correlated with systolic blood pressure and pulse pressure in children with obesity. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 508–513. [Google Scholar] [CrossRef]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 6, CD012651. [Google Scholar] [CrossRef] [Green Version]
- Al-Khudairy, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 6, CD012691. [Google Scholar] [CrossRef] [Green Version]
- de Sousa, C.V.; Sales, M.M.; Rosa, T.S.; Lewis, J.E.; de Andrade, R.V.; Simões, H.G. The Antioxidant Effect of Exercise: A Systematic Review and Meta-Analysis. Sport. Med. 2017, 47, 277–293. [Google Scholar] [CrossRef]
- Rupérez, A.I.; Mesa, M.D.; Anguita-Ruiz, A.; González-Gil, E.M.; Vázquez-Cobela, R.; Moreno, L.A.; Gil, Á.; Gil-Campos, M.; Leis, R.; Bueno, G.; et al. Antioxidants and oxidative stress in children: Influence of puberty and metabolically unhealthy status. Antioxidants 2020, 9, 618. [Google Scholar] [CrossRef]
- Avloniti, A.; Chatzinikolaou, A.; Deli, C.K.; Vlachopoulos, D.; Marco, L.G.; Leontsini, D.; Draganidis, D.; Jamurtas, A.Z.; Mastorakos, G.; Fatouros, I.G. Exercise-induced oxidative stress responses in the pediatric population. Antioxidants 2017, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020; ISBN 9789241550536. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br. Med. J. 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sport. Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Treuth, M.S.; Schmitz, K.; Catellier, D.J.; McMurray, R.G.; Murray, D.M.; Almeida, M.J.; Going, S.; Norman, J.E.; Pate, R. Defining accelerometer thresholds for activity intensities in adolescent girls. Med. Sci. Sports Exerc. 2004, 36, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]
- Llorente-Cantarero, F.J.; Gil-Campos, M.; Benitez-Sillero, J.D.; Muñoz-Villanueva, M.C.; Túnez, I.; Pérez-Navero, J.L. Prepubertal children with suitable fitness and physical activity present reduced risk of oxidative stress. Free Radic. Biol. Med. 2012, 53, 415–420. [Google Scholar] [CrossRef]
- Llorente-Cantarero, F.J.; Gil-Campos, M.; de Benitez-Sillero, J.D.; Muñoz-Villanueva, M.C.; Tasset, I.; Pérez-Navero, J.L. Profile of oxidant and antioxidant activity in prepubertal children related to age, gender, exercise, and fitness. Appl. Physiol. Nutr. Metab. 2013, 38, 421–426. [Google Scholar] [CrossRef]
- Paltoglou, G.; Fatouros, I.G.; Valsamakis, G.; Schoina, M.; Avloniti, A.; Chatzinikolaou, A.; Kambas, A.; Draganidis, D.; Mantzou, A.; Papagianni, M.; et al. Antioxidation improves in puberty in normal weight and obese boys, in positive association with exercise-stimulated growth hormone secretion. Pediatric Res. 2015, 78, 158–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghadir, A.H.; Gabr, S.A.; Iqbal, Z.A.; Al-Eisa, E. Association of physical activity, vitamin E levels, and total antioxidant capacity with academic performance and executive functions of adolescents. BMC Pediatrics 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nasca, M.M.; Zhang, R.; Super, D.M.; Hazen, S.L.; Hall, H.R. Increased oxidative stress in healthy children following an exercise program: A pilot study. J. Dev. Behav. Pediatrics 2010, 31, 386–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youssef, H.; Groussard, C.; Lemoine-Morel, S.; Jacob, C.; Moussa, E.; Fazah, A.; Pineau, J.C.; Pincemail, J.; Cillard, J.; Delamarche, A. Aerobic training suppresses exercise-induced lipid peroxidation and inflammation in overweight/obese adolescent girls. Pediatric Exerc. Sci. 2015, 27, 67–76. [Google Scholar] [CrossRef]
- Paltoglou, G.; Schoina, M.; Valsamakis, G.; Salakos, N.; Avloniti, A.; Chatzinikolaou, A.; Margeli, A.; Skevaki, C.; Papagianni, M.; Kanaka-Gantenbein, C.; et al. Interrelations among the adipocytokines leptin and adiponectin, oxidative stress and aseptic inflammation markers in pre- and early-pubertal normal-weight and obese boys. Endocrine 2017, 55, 925–933. [Google Scholar] [CrossRef]
- Vehapoglu, A.; Turkmen, S.; Goknar, N.; Özer, Ö.F. Reduced antioxidant capacity and increased subclinical inflammation markers in prepubescent obese children and their relationship with nutritional markers and metabolic parameters. Redox Rep. 2016, 21, 271–280. [Google Scholar] [CrossRef]
- Rowicka, G.; Dyląg, H.; Ambroszkiewicz, J.; Riahi, A.; Weker, H.; Chełchowska, M. Total Oxidant and Antioxidant Status in Prepubertal Children with Obesity. Oxid. Med. Cell. Longev. 2017, 2017. [Google Scholar] [CrossRef] [Green Version]
- Chaki, B.; Pal, S.; Chattopadhyay, S.; Bandyopadhyay, A. High-intensity exercise-induced oxidative stress in sedentary pre-pubertal & post-pubertal boys: A comparative study. Indian J. Med. Res. 2019, 150, 167–174. [Google Scholar] [CrossRef]
- Yilmaz, N.; Erel, Ö.; Hazer, M.; Baǧci, C.; Namiduru, E.; Gül, E. Biochemical assessments of retinol, α-tocopherol, pyridoxal—5-phosphate oxidative stress index and total antioxidant status in adolescent professional basketball players and sedentary controls. Int. J. Adolesc. Med. Health 2007, 19, 177–186. [Google Scholar] [CrossRef]
- Teixeira, V.; Valente, H.; Casal, S.; Pereira, L.; Marques, F.; Moreira, P. Antioxidant status, oxidative stress, and damage in elite kayakers after 1 year of training and competition in 2 seasons. Appl. Physiol. Nutr. Metab. 2009, 34, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Abed, K.; Rebai, H.; Bloomer, R.J.; Trabelsi, K.; Masmoudi, L.; Zbidi, A.; Sahnoun, Z.; Hakim, A.; Tabka, Z. Antioxidant status and oxidative stress at rest and in response to acute exercise in judokas and sedentary men. J. Strength Cond. Res. 2011, 25, 2400–2409. [Google Scholar] [CrossRef] [PubMed]
- Wayner, D.D.; Burton, G.W.; Ingold, K.U.; Barclay, L.R.; Locke, S.J. The relative contributions of vitamin E, urate, ascorbate and proteins to the total peroxyl radical-trapping antioxidant activity of human blood plasma. Biochim. Biophys. Acta 1987, 924, 408–419. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Participants (216) | Prepubertal (105) | Pubertal (111) | p-Value |
|---|---|---|---|---|
| Age (years) | 10.8 ± 2.2 | 9.4 ± 1.7 | 12.1 ± 1.7 | <0.001 |
| Weight (kg) | 50.3 ± 17.3 | 41.8 ± 12 | 58.2 ± 17.9 | <0.001 |
| Height (m) | 1.47 ± 0.13 | 1.38 ± 0.10 | 1.55 ± 0.10 | <0.001 |
| BMI (kg/m2) | 22.9 ± 5.2 | 21.7 ± 4.5 | 23.9 ± 5.6 | 0.003 |
| BMI z-score | 1.15 ± 2.14 | 1.11 ± 2.38 | 1.15 ± 2.18 | 0.886 |
| FM (kg) | 15.2 ± 9.3 | 12.8 ± 7 | 17.3 ± 10.6 | 0.001 |
| FM (%) | 27.8 ± 9.9 | 27.9 ± 9.3 | 27.6 ± 10.4 | 0.836 |
| FFM (kg) | 35.1 ± 10.2 | 29.4 ± 6.4 | 40.4 ± 10.3 | <0.001 |
| FFM (%) | 71.6 ± 11.1 | 71.5 ± 10.4 | 71.7 ± 11.8 | 0.887 |
| Normal weight (%) | 34.9 | 14.9 | 20.2 | 0.342 * |
| Overweight (%) | 23 | 11.5 | 11.5 | 0.342 * |
| Obesity (%) | 42.1 | 22.6 | 19.2 | 0.342 * |
| HOMA-IR | 2.91 ± 1.81 | 2.32 ± 1.54 | 3.40 ± 1.83 | <0.001 |
| ST (min/d) | 482 ± 97 | 467 ± 103 | 495 ± 89 | 0.018 |
| PA Moderate (min/d) | 38 ± 14 | 40 ± 13 | 36 ± 15 | 0.050 |
| PA Vigorous (min/d) | 15 ± 10 | 14 ± 8 | 16 ± 11 | 0.251 |
| MVPA (min/d) | 53 ± 21 | 54 ± 20 | 52 ± 23 | 0.494 |
| Variables | Component matrix a | ||
|---|---|---|---|
| Factor * | |||
| Metabolic Risk | Oxidative Stress | Physical Activity | |
| HOMA-IR | 0.831 | ||
| FM (kg) | 0.804 | ||
| FFM (kg) | 0.798 | 0.388 | |
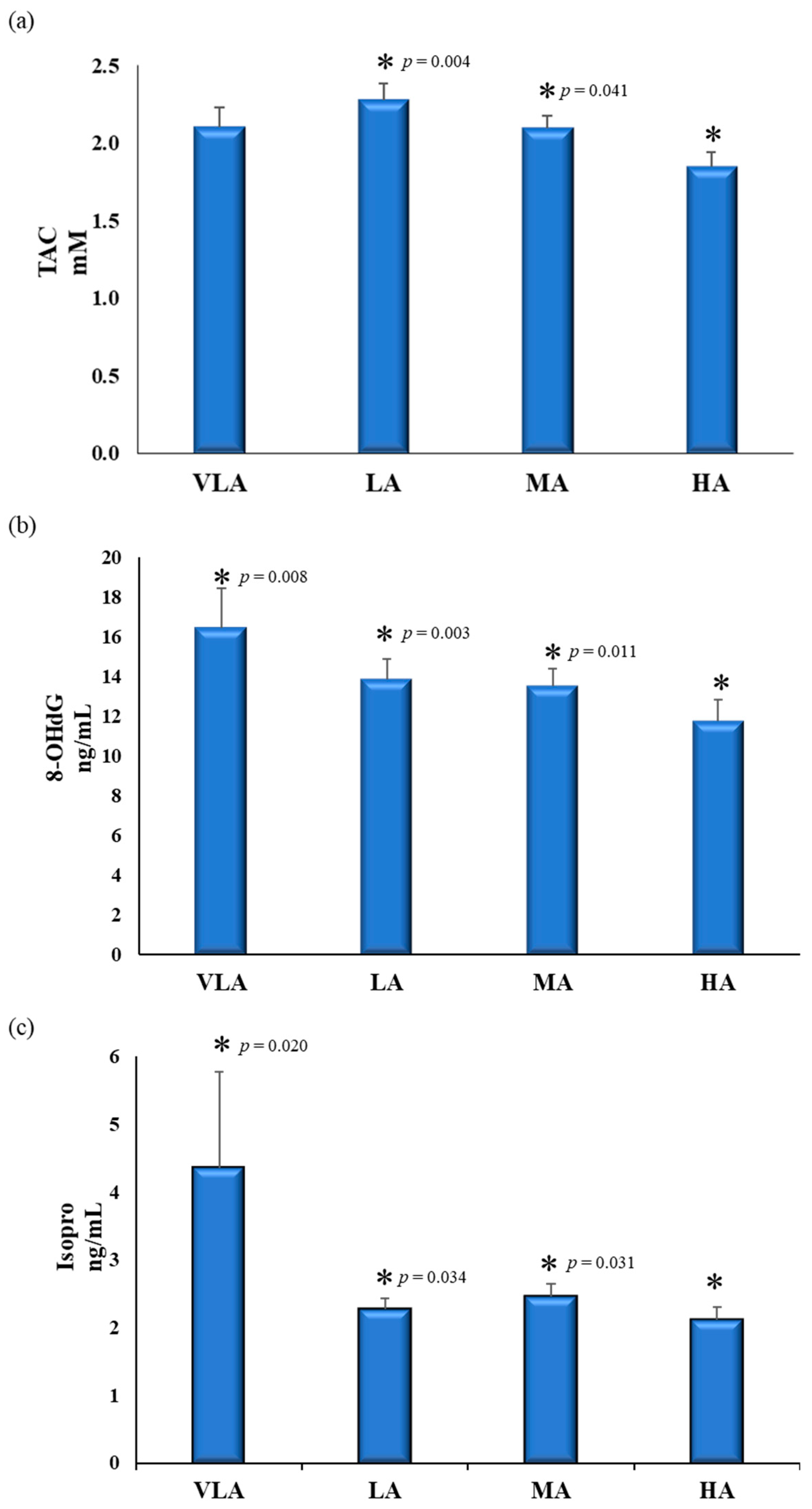
| TAC (mM) | 0.356 | ||
| 8-OHdG (ng/mL) | 0.859 | ||
| F2-IsoPs (ng/mL) | 0.831 | ||
| MVPA (min/d) | −0.377 | 0.771 | |
| ST (min/d) | 0.366 | 0.387 | −0.422 |
| Component | Total Variance Explained | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Initial Eigenvalues | Sums of Loads Squared from Extraction | Sums of Loads Squared of Rotation | |||||||
| Total | % of variance | % Accumulated | Total | % of Variance | % Accumulated | Total | % of Variance | % Accumulated | |
| 1 | 2.402 | 30.029 | 30.029 | 2.402 | 30.029 | 30.029 | 2.232 | 27.901 | 27.901 |
| 2 | 1.694 | 21.175 | 51.204 | 1.694 | 21.175 | 51.204 | 1.634 | 20.424 | 48.325 |
| 3 | 1.063 | 13.293 | 64.496 | 1.063 | 13.293 | 64.496 | 1.294 | 16.171 | 64.496 |
| Variables | Physical Activity-Sedentarism Score Levels | p-Value | p-Value for Trend | |||
|---|---|---|---|---|---|---|
| Very Low Active (12) | Low Active (65) | Moderate Active (82) | High Active (57) | |||
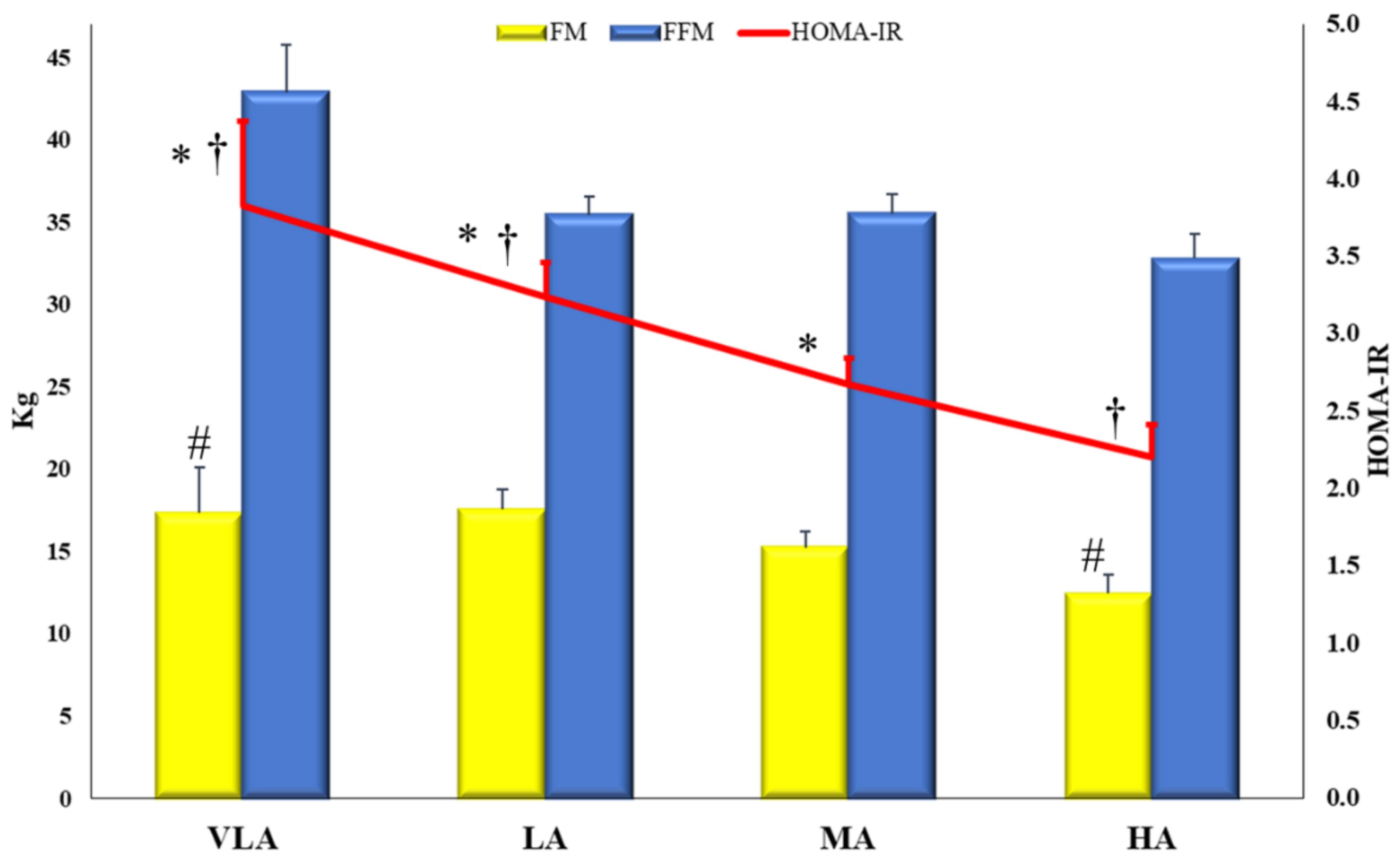
| BMI z-score | 1.25 ± 1.4 a,b | 1.57 ± 2.1 a,b | 1.41 ± 1.9 a,b | 0.51 ± 2.9 a,c | 0.046 | 0.029 |
| PASS | 3 a | 5.27 ± 0.78 b | 8 ± 0.84 c | 10.88 ± 0.81 d | <0.001 | <0.001 |
| MVPA (min/d) | 22 ± 5 a | 34 ± 11 b | 55 ± 12 c | 76 ± 17 d | <0.001 | <0.001 |
| ST (min/d) | 601 ± 70 a | 517 ± 92 b | 471 ± 95 c | 397 ± 54 d | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llorente-Cantarero, F.J.; Aguilar-Gómez, F.J.; Leis, R.; Bueno, G.; Rupérez, A.I.; Anguita-Ruiz, A.; Vázquez-Cobela, R.; Mesa, M.D.; Moreno, L.A.; Gil, Á.; et al. Relationship between Physical Activity, Oxidative Stress, and Total Plasma Antioxidant Capacity in Spanish Children from the GENOBOX Study. Antioxidants 2021, 10, 320. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10020320
Llorente-Cantarero FJ, Aguilar-Gómez FJ, Leis R, Bueno G, Rupérez AI, Anguita-Ruiz A, Vázquez-Cobela R, Mesa MD, Moreno LA, Gil Á, et al. Relationship between Physical Activity, Oxidative Stress, and Total Plasma Antioxidant Capacity in Spanish Children from the GENOBOX Study. Antioxidants. 2021; 10(2):320. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10020320
Chicago/Turabian StyleLlorente-Cantarero, Francisco Jesús, Francisco Javier Aguilar-Gómez, Rosaura Leis, Gloria Bueno, Azahara I. Rupérez, Augusto Anguita-Ruiz, Rocío Vázquez-Cobela, María Dolores Mesa, Luis A. Moreno, Ángel Gil, and et al. 2021. "Relationship between Physical Activity, Oxidative Stress, and Total Plasma Antioxidant Capacity in Spanish Children from the GENOBOX Study" Antioxidants 10, no. 2: 320. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10020320