Appropriate Handling, Processing and Analysis of Blood Samples Is Essential to Avoid Oxidation of Vitamin C to Dehydroascorbic Acid


Abstract
:1. Introduction
2. Materials and Methods
2.1. In Vitro Stability of Ascorbate and DHA
2.2. Stability of Ascorbate in Blood and Plasma
2.3. Long-Term Stability of Ascorbate and DHA
2.4. Detection of DHA in Clinical Samples
2.5. Sample Preparation for HPLC Analysis
2.6. Ascorbate HPLC Analysis
2.7. Statistical Analyses
3. Results
3.1. Detection of DHA in Clinical Samples
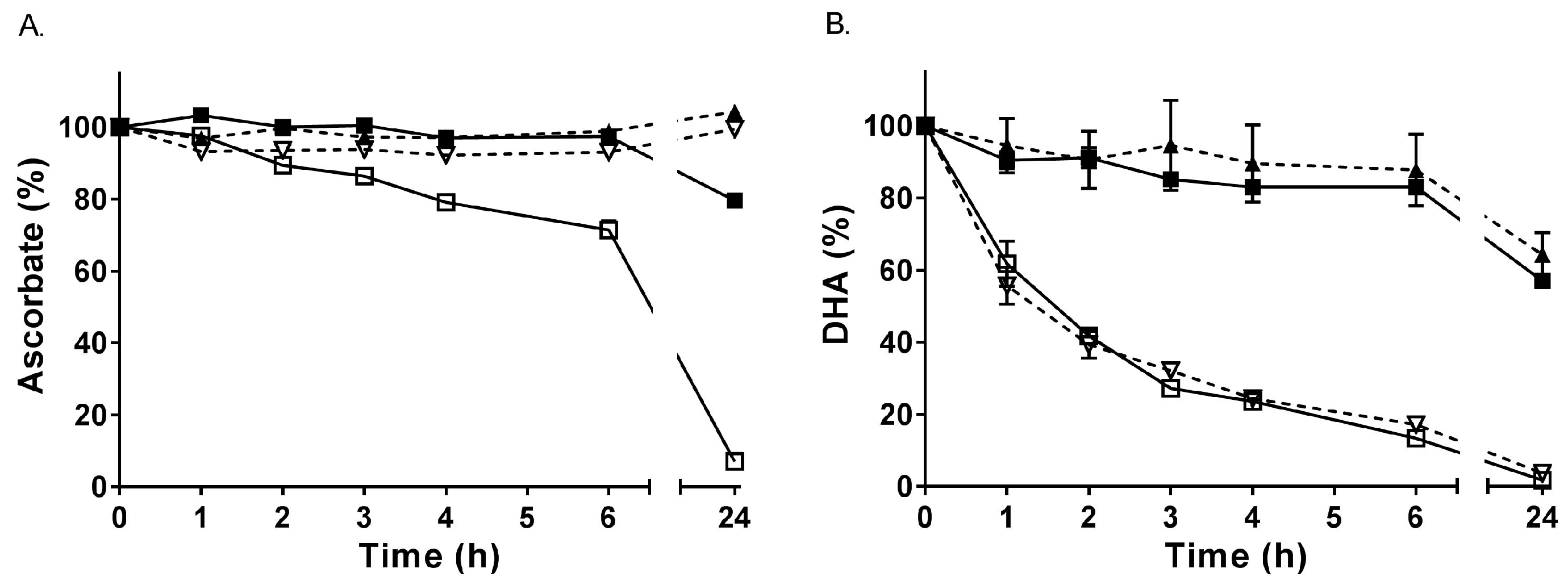
3.2. In Vitro Stability of Ascorbate and DHA
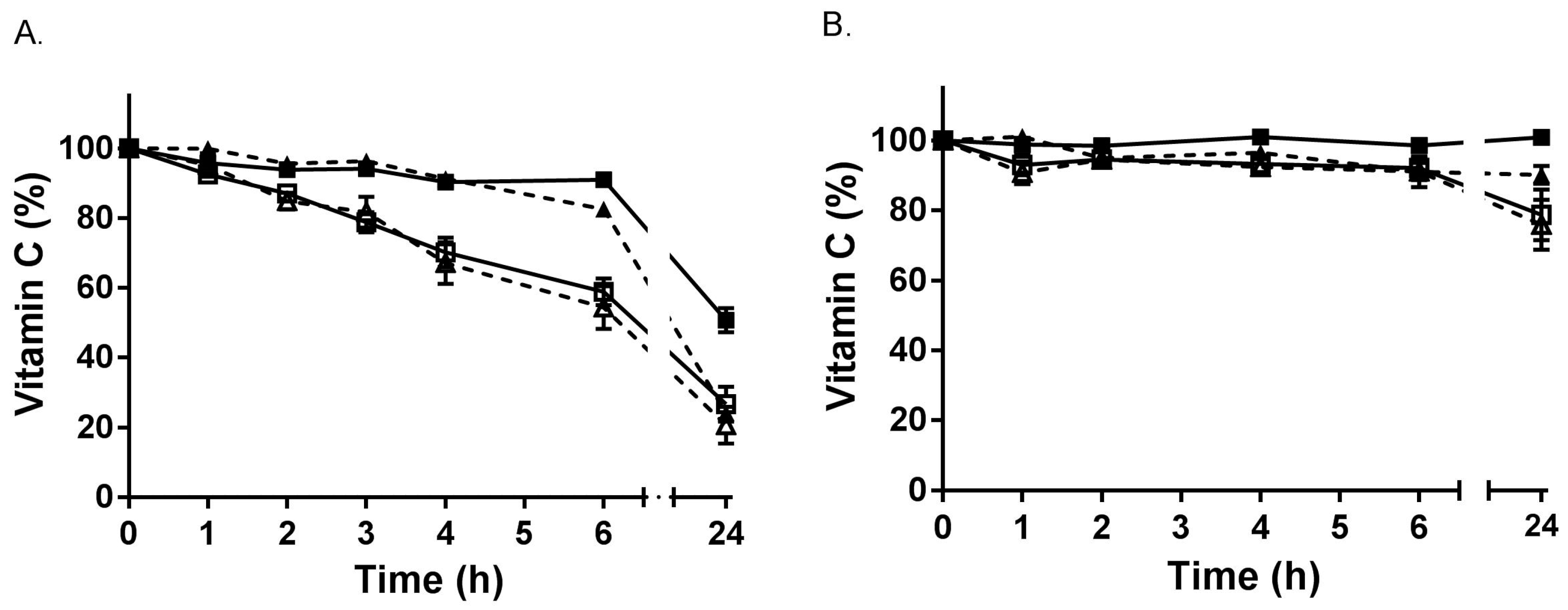
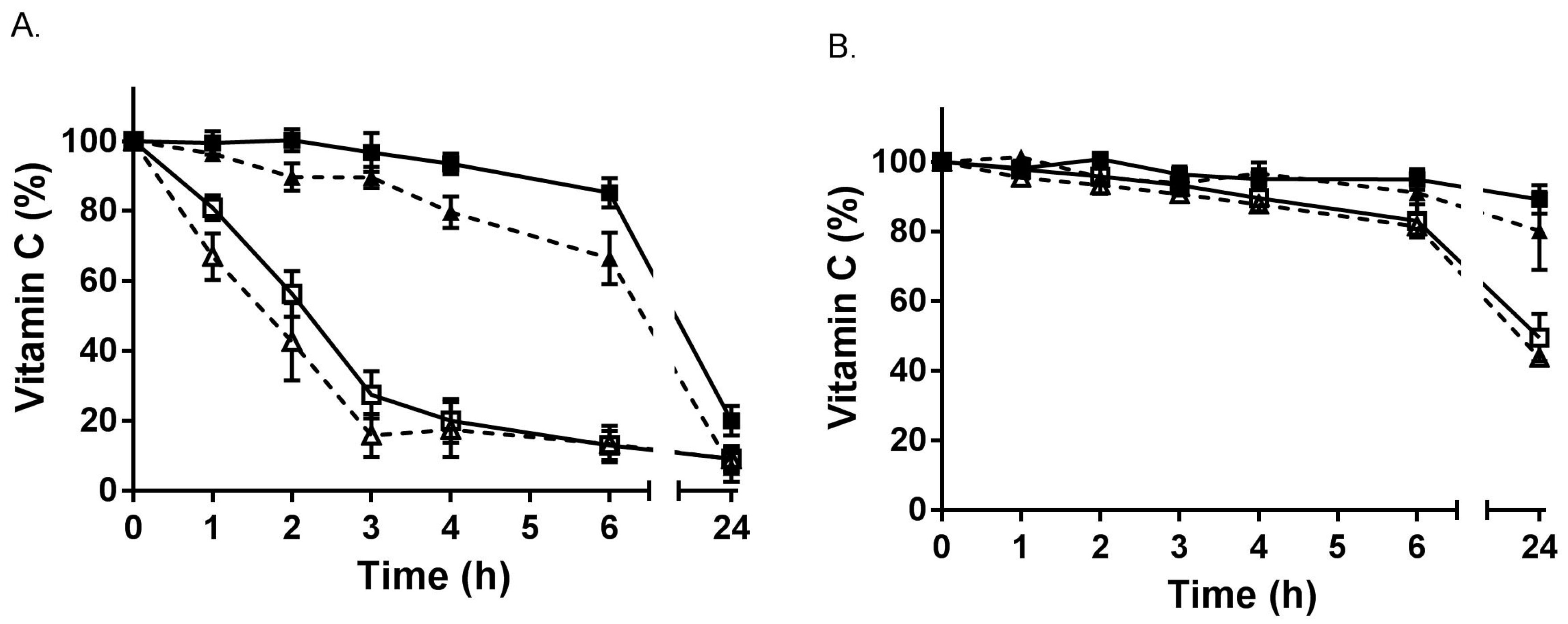
3.3. Stability of Ascorbate during Sample Collection and Processing
3.3.1. Stability in Whole Blood
3.3.2. Stability in Plasma
4. Discussion
5. Conclusions
- Plasma stored at −80 °C prior to processing for ascorbate analysis contains variable amounts of DHA, requiring treatment with a reducing agent prior to ascorbate analysis (DHA is relatively stable for at least a year at −80 °C at physiological pH).
- Haemolysis facilitates oxidation of ascorbate, likely due to the release of catalytic iron from haemoglobin following acid precipitation, requiring reduction of samples prior to ascorbate analysis (DHA is stable for at least five years at −80 °C under acidic conditions).
- EDTA anticoagulant samples need to be kept cold at all times during handling, processing and analysis as EDTA-chelated iron is redox active at physiological pH and can facilitate ascorbate oxidation via redox cycling.
- Colourimetric/fluorometric ascorbate assays appear to generate high concentrations of DHA via artefactual ex vivo oxidation of ascorbate, regardless of the anticoagulant or deproteinization method used. In comparison, analysis using HPLC with electrochemical detection does not detect appreciable DHA concentrations in clinical samples.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Svirbely, J.L.; Szent-Gyorgyi, A. The chemical nature of vitamin C. Biochem. J. 1933, 27, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.; Frei, B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999, 13, 1007–1024. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Zhu, B.Z.; Frei, B. Potential antiatherogenic mechanisms of ascorbate (vitamin C) and alpha-tocopherol (vitamin E). Circ. Res. 2000, 87, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Vissers, M.C.; Kuiper, C.; Dachs, G.U. Regulation of the 2-oxoglutarate-dependent dioxygenases and implications for cancer. Biochem. Soc. Trans. 2014, 42, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Young, J.I.; Zuchner, S.; Wang, G. Regulation of the epigenome by vitamin C. Annu. Rev. Nutr. 2015, 35, 545–564. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Cullen, J.J.; Buettner, G.R. Ascorbic acid: Chemistry, biology and the treatment of cancer. Biochim. Biophys. Acta 2012, 1826, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Shaw, G.M.; Fowler, A.A.; Natarajan, R. Ascorbate-dependent vasopressor synthesis: A rationale for vitamin C administration in severe sepsis and septic shock? Crit. Care 2015, 19, 418. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, B.; Banerjee, S. Dehydroascorbic acid level in blood of patients suffering from various infectious diseases. Proc. Soc. Exp. Biol. Med. 1955, 88, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.S.; Palodhi, G.R.; Jain, A.K. Ascorbic acid, dehydroascorbic acid and glutathione in liver disease. Indian J. Physiol. Pharmacol. 1987, 31, 279–283. [Google Scholar] [PubMed]
- Lunec, J.; Blake, D.R. The determination of dehydroascorbic acid and ascorbic acid in the serum and synovial fluid of patients with rheumatoid arthritis (RA). Free Radic. Res. Commun. 1985, 1, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, I.B.; Banerjee, A. Estimation of dehydroascorbic acid in blood of diabetic patients. Anal. Biochem. 1979, 98, 368–374. [Google Scholar] [CrossRef]
- Banerjee, A. Blood dehydroascorbic acid and diabetes mellitus in human beings. Ann. Clin. Biochem. 1982, 19 Pt 2, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.D.; Whichelow, M.J. The measurement of dehydroascorbic acid and diketogulonic acid in normal and diabetic plasma. Biochem. Med. 1975, 12, 183–193. [Google Scholar] [CrossRef]
- Schorah, C.J.; Downing, C.; Piripitsi, A.; Gallivan, L.; Al-Hazaa, A.H.; Sanderson, M.J.; Bodenham, A. Total vitamin C, ascorbic acid, and dehydroascorbic acid concentrations in plasma of critically ill patients. Am. J. Clin. Nutr. 1996, 63, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J.; Loft, S.; Nielsen, J.B.; Poulsen, H.E. Ascorbic acid and dehydroascorbic acid as biomarkers of oxidative stress caused by smoking. Am. J. Clin. Nutr. 1997, 65, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Buettner, G.R.; Jurkiewicz, B.A. Catalytic metals, ascorbate and free radicals: Combinations to avoid. Radiat. Res. 1996, 145, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Bode, A.M.; Cunningham, L.; Rose, R.C. Spontaneous decay of oxidized ascorbic acid (dehydro-L-ascorbic acid) evaluated by high-pressure liquid chromatography. Clin. Chem. 1990, 36, 1807–1809. [Google Scholar] [PubMed]
- Washko, P.W.; Welch, R.W.; Dhariwal, K.R.; Wang, Y.; Levine, M. Ascorbic acid and dehydroascorbic acid analyses in biological samples. Anal. Biochem. 1992, 204, 1–14. [Google Scholar] [CrossRef]
- Lykkesfeldt, J. Ascorbate and dehydroascorbic acid as biomarkers of oxidative stress: Validity of clinical data depends on vacutainer system used. Nutr. Res. 2012, 32, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Rosengrave, P.C.; Bayer, S.; Chambers, S.; Mehrtens, J.; Shaw, G.M. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care 2017, 21, 300. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.F.; Pullar, J.M.; Wilson, R.; Spittlehouse, J.K.; Vissers, M.C.M.; Skidmore, P.M.L.; Willis, J.; Cameron, V.A.; Carr, A.C. Vitamin C status correlates with markers of metabolic and cognitive health in 50-year-olds: Findings of the CHALICE cohort study. Nutrients 2017, 9, 831. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Willis, J.; Gearry, R.; Skidmore, P.; Fleming, E.; Frampton, C.; Carr, A. Inadequate vitamin C status in prediabetes and type 2 diabetes mellitus: Associations with glycaemic control, obesity, and smoking. Nutrients 2017, 9, 997. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Pullar, J.M.; Moran, S.; Vissers, M.C.M. Bioavailability of vitamin C from kiwifruit in non-smoking males: Determination of ‘healthy’ and ‘optimal’ intakes. J. Nutr. Sci. 2012, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wechtersbach, L.; Cigic, B. Reduction of dehydroascorbic acid at low pH. J. Biochem. Biophys. Methods 2007, 70, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Uchiki, T.; Iwama, M.; Kishimoto, Y.; Takahashi, R.; Ishigami, A. Determination of dehydroascorbic acid in mouse tissues and plasma by using tris (2-carboxyethyl) phosphine hydrochloride as reductant in metaphosphoric acid/ethylenediaminetetraacetic acid solution. Biol. Pharm. Bull. 2010, 33, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Koshiishi, I.; Mamura, Y.; Liu, J.; Imanari, T. Evaluation of an acidic deproteinization for the measurement of ascorbate and dehydroascorbate in plasma samples. Clin. Chem. 1998, 44, 863–868. [Google Scholar] [PubMed]
- Koshiishi, I.; Imanari, T. Measurement of ascorbate and dehydroascorbate contents in biological fluids. Anal. Chem. 1997, 69, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J. Ascorbate and dehydroascorbic acid as reliable biomarkers of oxidative stress: Analytical reproducibility and long-term stability of plasma samples subjected to acidic deproteinization. Cancer Epidemiol. Prev. Biomark. 2007, 16, 2513–2516. [Google Scholar] [CrossRef] [PubMed]
- Banfi, G.; Salvagno, G.L.; Lippi, G. The role of ethylenediamine tetraacetic acid (EDTA) as in vitro anticoagulant for diagnostic purposes. Clin. Chem. Lab. Med. 2007, 45, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Burkitt, M.J.; Gilbert, B.C. Model studies of the iron-catalysed Haber-Weiss cycle and the ascorbate-driven Fenton reaction. Free Radic. Res. Commun. 1990, 10, 265–280. [Google Scholar] [CrossRef] [PubMed]
- Buettner, G.R. Ascorbate oxidation: UV absorbance of ascorbate and ESR spectroscopy of the ascorbyl radical as assays for iron. Free Radic. Res. Commun. 1990, 10, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Salminen, I.; Alfthan, G. Plasma ascorbic acid preparation and storage for epidemiological studies using TCA precipitation. Clin. Biochem. 2008, 41, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Davis, K.A.; Rettmer, R.L.; Labbe, R.F. Ascorbic acid status: Biochemical and clinical considerations. Am. J. Clin. Nutr. 1988, 48, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, A.; Blomhoff, R.; Gundersen, T.E. Stability of whole blood and plasma ascorbic acid. Eur. J. Clin. Nutr. 2007, 61, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Cuerq, C.; Peretti, N.; Chikh, K.; Mialon, A.; Guillaumont, M.; Drai, J.; Blond, E. Overview of the in vitro stability of commonly measured vitamins and carotenoids in whole blood. Ann. Clin. Biochem. 2015, 52 Pt 2, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.Y.; Chung, J.K.; Szeto, Y.T.; Tomlinson, B.; Benzie, I.F. Plasma ascorbic acid: Measurement, stability and clinical utility revisited. Clin. Biochem. 2001, 34, 623–627. [Google Scholar] [CrossRef]
- Liau, L.S.; Lee, B.L.; New, A.L.; Ong, C.N. Determination of plasma ascorbic acid by high-performance liquid chromatography with ultraviolet and electrochemical detection. J. Chromatogr. B Biomed. Sci. Appl. 1993, 612, 63–70. [Google Scholar] [CrossRef]
- Ching, S.Y.; Prins, A.W.; Beilby, J.P. Stability of ascorbic acid in serum and plasma prior to analysis. Ann. Clin. Biochem. 2002, 39, 518–520. [Google Scholar] [CrossRef] [PubMed]
- Bradley, D.W.; Emery, G.; Maynard, J.E. Vitamin C in plasma: A comparative study of the vitamin stabilized with trichloroacetic acid or metaphosphoric acid and the effects of storage at −70 degrees, −20 degrees, 4 degrees, and 25 degrees on the stabilized vitamin. Clin. Chim. Acta 1973, 44, 47–52. [Google Scholar] [CrossRef]
- Kand’ar, R.; Zakova, P. Determination of ascorbic acid in human plasma with a view to stability using HPLC with UV detection. J. Sep. Sci. 2008, 31, 3503–3508. [Google Scholar] [CrossRef] [PubMed]
- Dhariwal, K.R.; Hartzell, W.O.; Levine, M. Ascorbic acid and dehydroascorbic acid measurements in human plasma and serum. Am. J. Clin. Nutr. 1991, 54, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.; Li, H.; Wang, Y.; Niyyati, M.; Wang, Y.; Leshin, J.; Levine, M. Low red blood cell vitamin C concentrations induce red blood cell fragility: A link to diabetes via glucose, glucose transporters, and dehydroascorbic acid. EBioMedicine 2015, 2, 1735–1750. [Google Scholar] [CrossRef] [PubMed]
- Rumsey, S.C.; Kwon, O.; Xu, G.W.; Burant, C.F.; Simpson, I.; Levine, M. Glucose transporter isoforms GLUT1 and GLUT3 transport dehydroascorbic acid. J. Biol. Chem. 1997, 272, 18982–18989. [Google Scholar] [CrossRef] [PubMed]
- Welch, R.W.; Wang, Y.; Crossman, A., Jr.; Park, J.B.; Kirk, K.L.; Levine, M. Accumulation of vitamin C (ascorbate) and its oxidized metabolite dehydroascorbic acid occurs by separate mechanisms. J. Biol. Chem. 1995, 270, 12584–12592. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.S.; Thompson, L.L. Vitamin C status of an outpatient population. J. Am. Coll. Nutr. 1998, 17, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Gan, R.; Eintracht, S.; Hoffer, L.J. Vitamin C deficiency in a university teaching hospital. J. Am. Coll. Nutr. 2008, 27, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Cahill, L.; Corey, P.N.; El-Sohemy, A. Vitamin C deficiency in a population of young canadian adults. Am. J. Epidemiol. 2009, 170, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L.J. Re: “Vitamin C deficiency in a population of young canadian adults”. Am. J. Epidemiol. 2010, 171, 387. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cohort | Description (n) | DHA (µmol/L) 1 |
|---|---|---|
| Community | Prediabetes (22) | 2.8 ± 4.2 |
| Infection | Pneumonia (20) | 1.2 ± 1.2 |
| Cancer | Colorectal (27) | 2.5 ± 3.3 |
| Haematological (6) | 1.0 ± 0.4 | |
| Critically ill | Septic shock (24) | 0.1 ± 2.2 |
| Surgical (15) | 0.0 ± 1.5 | |
| Excluded 2 | Heamolysed (9) | 17 ± 11 |
| Cohort (n) | DHA (µmol/L) |
|---|---|
| Community (20) | 24 ± 7 |
| Normal glucose control (32) | 10 ± 4 |
| Prediabetes (24) | 9 ± 5 |
| Type 2 diabetes mellitus (30) | 8 ± 6 |
| Cohort (n) | DHA (µmol/L) 1 | Anticoagulant, Deproteinization, and Detection | Ref. |
|---|---|---|---|
| Controls (28) Pneumonia–died (7) Pneumonia–survived (15) Convalescent (13) | 3 ± 1 39 ± 2 23 ± 1 9 ± 1 | Oxalate SSA DCPIP | [8] |
| Controls (10) Viral hepatitis (26) Liver carcinoma (11) | 5 ± 2 29 ± 8 32 ± 5 | Heparin TCA DNPH | [9] |
| Controls (20) Rheumatoid arthritis (13) | 12 ± 4 22 ± 9 | Serum MPA/EDTA PDA/HPLC | [10] |
| Controls (37) Diabetic–male (25) Diabetic–female (12) | 0 12 ± 2 12 ± 2 | Heparin MPA DNPH | [11] |
| Controls (20) Diabetic (27) | 2.0 ± 1.5 3.3 ± 3.0 | EDTA MPA/oxalate DNPH | [13] |
| Controls (34) Critically ill (62) Diabetic (24) Gastritis (21) | 2.3 (−2.9–5.8) 1.4 (−0.8–2.9) 2.8 (0.0–6.3) 2.3 (0.6–2.9) | Heparin MPA HPLC | [14] |
| Controls (124) Smokers (82) | 0.1 ± 2.4 0.8 ± 2.3 | MPA HPLC-ECD | [15] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pullar, J.M.; Bayer, S.; Carr, A.C. Appropriate Handling, Processing and Analysis of Blood Samples Is Essential to Avoid Oxidation of Vitamin C to Dehydroascorbic Acid. Antioxidants 2018, 7, 29. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox7020029
Pullar JM, Bayer S, Carr AC. Appropriate Handling, Processing and Analysis of Blood Samples Is Essential to Avoid Oxidation of Vitamin C to Dehydroascorbic Acid. Antioxidants. 2018; 7(2):29. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox7020029
Chicago/Turabian StylePullar, Juliet M., Simone Bayer, and Anitra C. Carr. 2018. "Appropriate Handling, Processing and Analysis of Blood Samples Is Essential to Avoid Oxidation of Vitamin C to Dehydroascorbic Acid" Antioxidants 7, no. 2: 29. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox7020029