
Excision of Lower Lip Mucocele Using Injection of Hydrocolloid Dental Impression Material in a Pediatric Patient: A Case Report

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case History
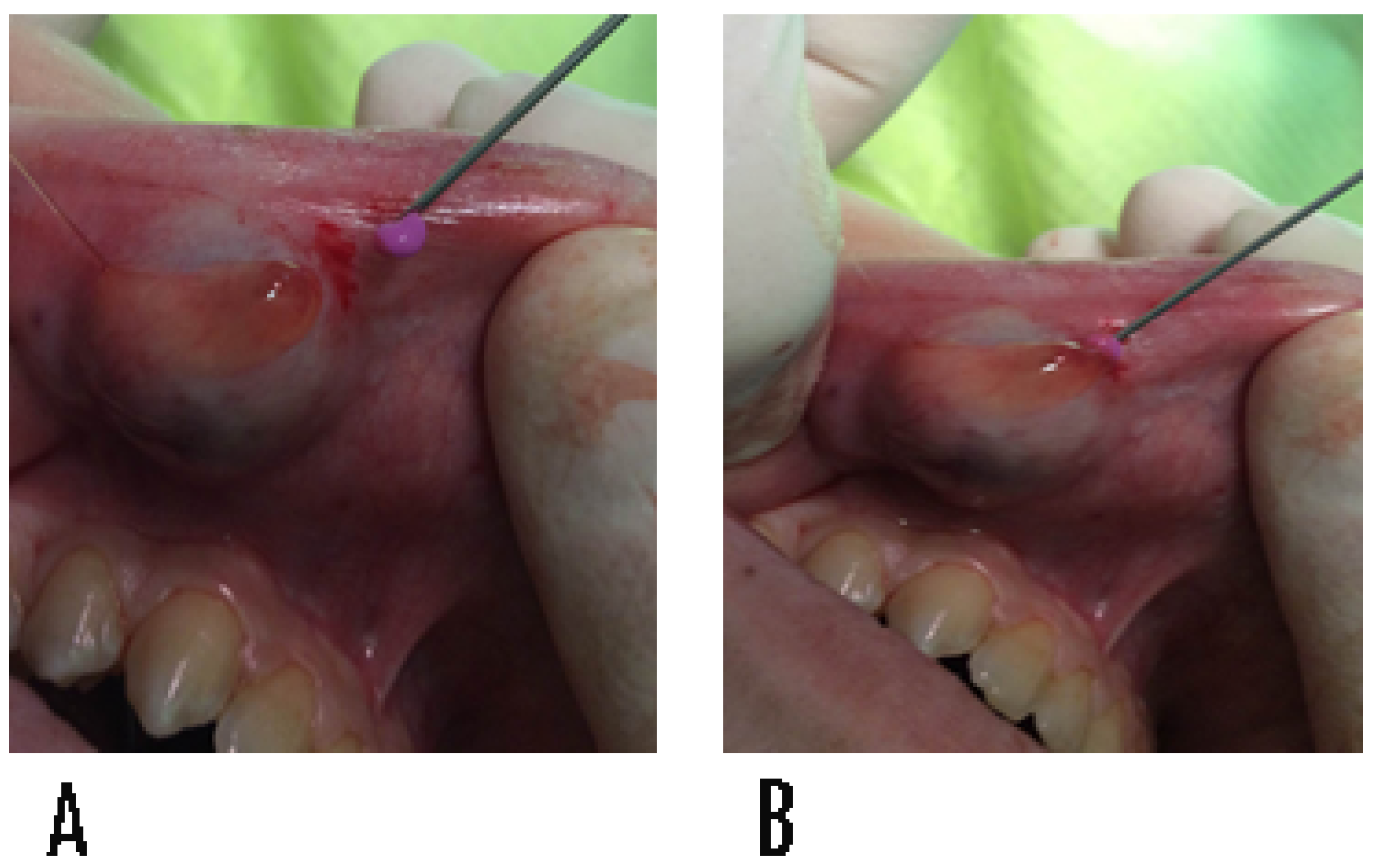
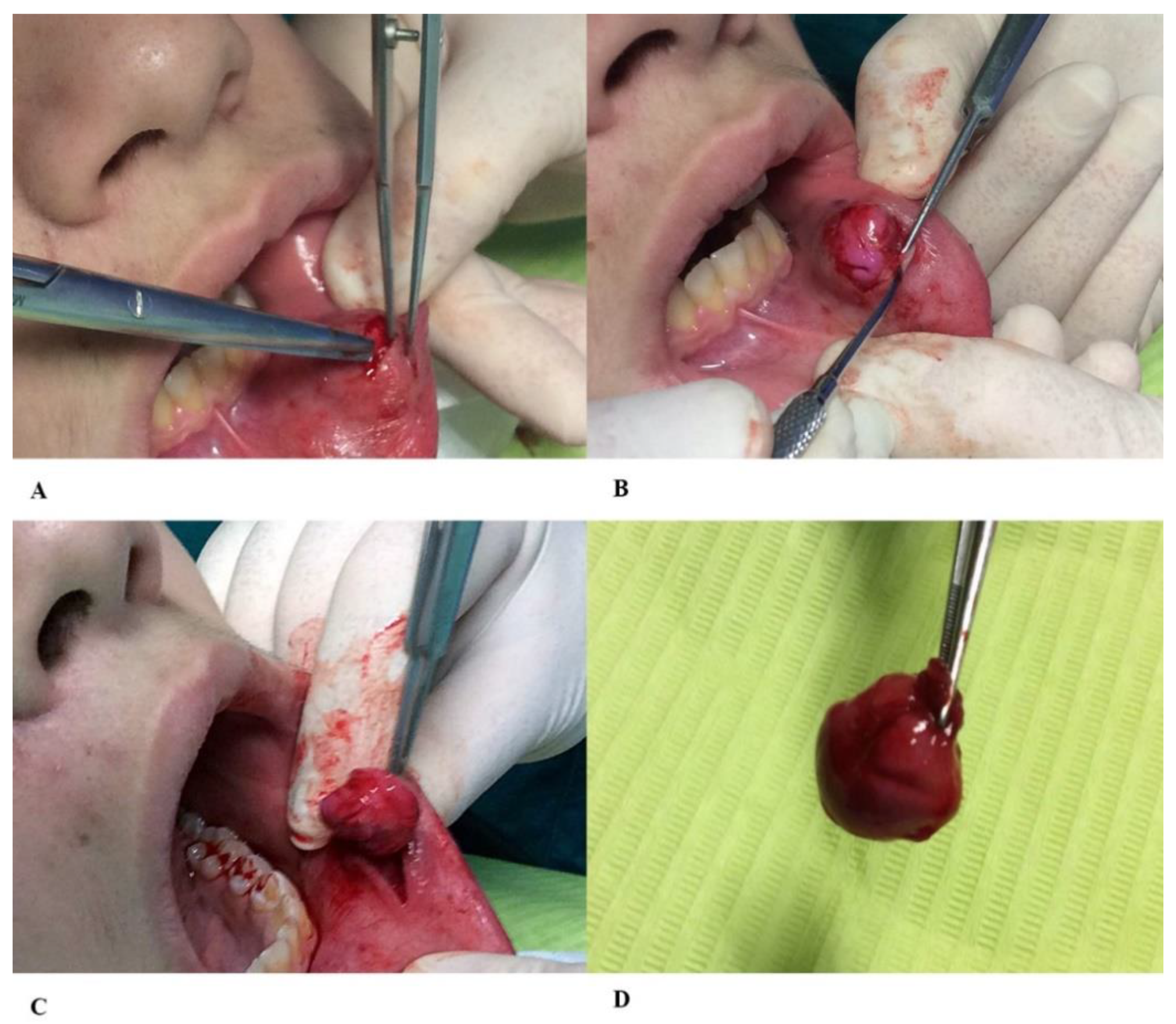
Surgical Procedure
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baurmash, H.D. Mucoceles and ranulas. J. Oral. Maxillofac. Surg. 2003, 61, 369–378. [Google Scholar] [CrossRef]
- Ozturk, K.; Yaman, H.; Arbag, H.; Koroglu, D.; Toy, H. Submandibular gland mucocele: Report of two cases. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2005, 100, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Re Cecconi, D.; Achilli, A.; Tarozzi, M.; Lodi, G. Mucoceles of the oral cavity: A large case series (1994–2008) and a literature review. Med. Oral. Pathol. Oral. Cir. Bucal. 2010, 15, e551–e556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- More, C.B.; Bhavsar, K.; Varma, S.; Tailor, M. Oral mucocele: A clinical and histopathological study. J. Oral. Maxillofac. Pathol. 2014, 18 (Suppl. 1), S72–S77. [Google Scholar] [CrossRef] [Green Version]
- Graillon, N.; Mage, C.; Le Roux, M.K.; Scemama, U.; Chossegros, C.; Foletti, J.M. Mucoceles of the anterior ventral surface of the tongue and the glands of Blandin-Nuhn: 5 cases. J. Stomatol. Oral. Maxillofac. Surg. 2019, 120, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Ata-Ali, J.; Carrillo, C.; Bonet, C.; Balaguer, J. Oral mucocele: Review of literature. J. Clin. Exp. Dent. 2010, 2, e18–e21. [Google Scholar] [CrossRef]
- Hong, C.; Dean, D.R.; Hull, K.; Hu, S.J.; Sim, Y.F.; Nadeau, C.; Gonçalves, S.; Lodi, G.; Hodgson, T.A. World Workshop on Oral Medicine VII: Relative frequency of oral mucosal lesions in children, a scoping review. Oral. Dis. 2019, 25 (Suppl. 1), 193–203. [Google Scholar] [CrossRef]
- Jensen, J.L. Superficial mucoceles of the oral mucosa. Am. J. Dermatopathol. 1990, 12, 88–92. [Google Scholar] [CrossRef]
- Harrison, J.D. Salivary mucoceles. Oral. Surg. Oral. Med. Oral. Pathol. 1975, 39, 268–278. [Google Scholar] [CrossRef]
- Bhaskar, S.N.; Bolden, T.E.; Weinmann, J.P. Pathogenesis of mucoceles. J. Dent. Res. 1956, 35, 863–874. [Google Scholar] [CrossRef]
- Jinbu, Y.; Kusama, M.; Itoh, H.; Matsumoto, K.; Wang, J.; Noguchi, T. Mucocele of the glands of Blandin-Nuhn: Clinical and histopathologic analysis of 26 cases. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2003, 95, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Sfasciotti, M.; Perfetti, G.; Annibali, S.; Pippi, R. Il mucocele delle ghiandole salivari minori. Parte I: Eziopatogenesi e istopatologia. Dental. Cadmos 1991, 11, 66–78. [Google Scholar]
- Sagari, S.K.; Vamsi, K.C.; Shah, D.; Singh, V.; Patil, G.B.; Saawarn, S. Micromarsupialization: A minimally invasive technique for mucocele in children and adolescents. J. Indian Soc. Pedod. Prev. Dent. 2012, 30, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Byun, J.S.; Choi, J.K.; Jung, J.K. Identification of predictive variables for the recurrence of oral mucocele. Med. Oral. Pathol. Oral. Cir. Bucal 2019, 24, e231–e235. [Google Scholar] [CrossRef]
- Anastassov, G.E.; Haiavy, J.; Solodnik, P.; Lee, H.; Lumerman, H. Submandibular gland mucocele: Diagnosis and management. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2000, 89, 159–163. [Google Scholar] [CrossRef]
- Johnson-Jahangir, H.; Agrawal, N. Perioperative Antibiotic Use in Cutaneous Surgery. Dermatol Clin. 2019, 37, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Dinoi, M.T.; Marchetti, E.; Garagiola, U.; Caruso, S.; Mummolo, S.; Marzo, G. Orthodontic treatment of an unerupted mandibular canine tooth in a patient with mixed dentition: A case report. J. Med. Case Rep. 2016, 10, 170. [Google Scholar] [CrossRef] [Green Version]
- Paglia, L.; Gallusi, S.; de Giorgio, S.; Cianetti, S.; Lupatelli, E.; Lombardo, G.; Montedori, A.; Eusebi, P.; Gatto, R.; Caruso, S. Reliability and validity of the Italian versions of the Children’s Fear Survey Schedule—Dental Subscale and the Modified Child Dental Anxiety Scale. Eur. J. Paediatr. Dent. 2017, 18, 305–312. [Google Scholar]
- Delbem, A.; Cunha, R.; Vieira, A.; Ribeiro, L. Treatment of mucus retention phenomena in children by the micro-marsupialization technique: Case reports. Pediatr. Dent. 2000, 22, 1558. [Google Scholar]
- Bernardi, S.; Mummolo, S.; Zeka, K.; Pajewski, L.; Continenza, M.A.; Marzo, G. Use and Evaluation of a Cooling Aid in Laser-Assisted Dental Surgery: An Innovative Study. Photomed. Laser. Surg. 2016, 34, 258–262. [Google Scholar] [CrossRef]
- Sinha, R.; Soumyabrata, S.; Khaitan, T.; Kabiraj, A.; Maji, A. Nonsurgical Management of Oral Mucocele by Intralesional Corticosteroid Therapy. Int. J. Dent. 2016, 2896748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, I.Y.; Chen, C.M.; Kao, Y.H.; Worthington, P. Treatment of mucocele of the lower lip with carbon dioxide laser. J. Oral. Maxillofac. Surg. 2007, 65, 855–858. [Google Scholar] [CrossRef] [PubMed]
- Shira, R.B. Simplified technic for the management of mucoceles and ranulas. J. Oral. Surg (Chic) 1962, 20, 374–379. [Google Scholar]
- De Santana Santos, T.; Martins, V.B.; Frota, R.; Karam, F.K. Excision of ranula using injection of hydrocolloid dental impression material. J. Craniofac. Surg. 2013, 24, 1859–1860. [Google Scholar] [CrossRef]
- Bernardi, S.; Marzo, G.; Continenza, M.A. Dorzalna površina jezika i halitoza: Morfološki aspekti Dorsal Lingual Surface and Halitosis: A Morphological Point of View. Acta Stomatol. Croat. 2016, 50, 151–157. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botticelli, G.; Severino, M.; Ferrazzano, G.F.; Vittorini Velasquez, P.; Franceschini, C.; Di Paolo, C.; Gatto, R.; Falisi, G. Excision of Lower Lip Mucocele Using Injection of Hydrocolloid Dental Impression Material in a Pediatric Patient: A Case Report. Appl. Sci. 2021, 11, 5819. https://0-doi-org.brum.beds.ac.uk/10.3390/app11135819
Botticelli G, Severino M, Ferrazzano GF, Vittorini Velasquez P, Franceschini C, Di Paolo C, Gatto R, Falisi G. Excision of Lower Lip Mucocele Using Injection of Hydrocolloid Dental Impression Material in a Pediatric Patient: A Case Report. Applied Sciences. 2021; 11(13):5819. https://0-doi-org.brum.beds.ac.uk/10.3390/app11135819
Chicago/Turabian StyleBotticelli, Gianluca, Marco Severino, Gianmaria Fabrizio Ferrazzano, Pedro Vittorini Velasquez, Carlo Franceschini, Carlo Di Paolo, Roberto Gatto, and Giovanni Falisi. 2021. "Excision of Lower Lip Mucocele Using Injection of Hydrocolloid Dental Impression Material in a Pediatric Patient: A Case Report" Applied Sciences 11, no. 13: 5819. https://0-doi-org.brum.beds.ac.uk/10.3390/app11135819