
Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Randomized Clinical Trial
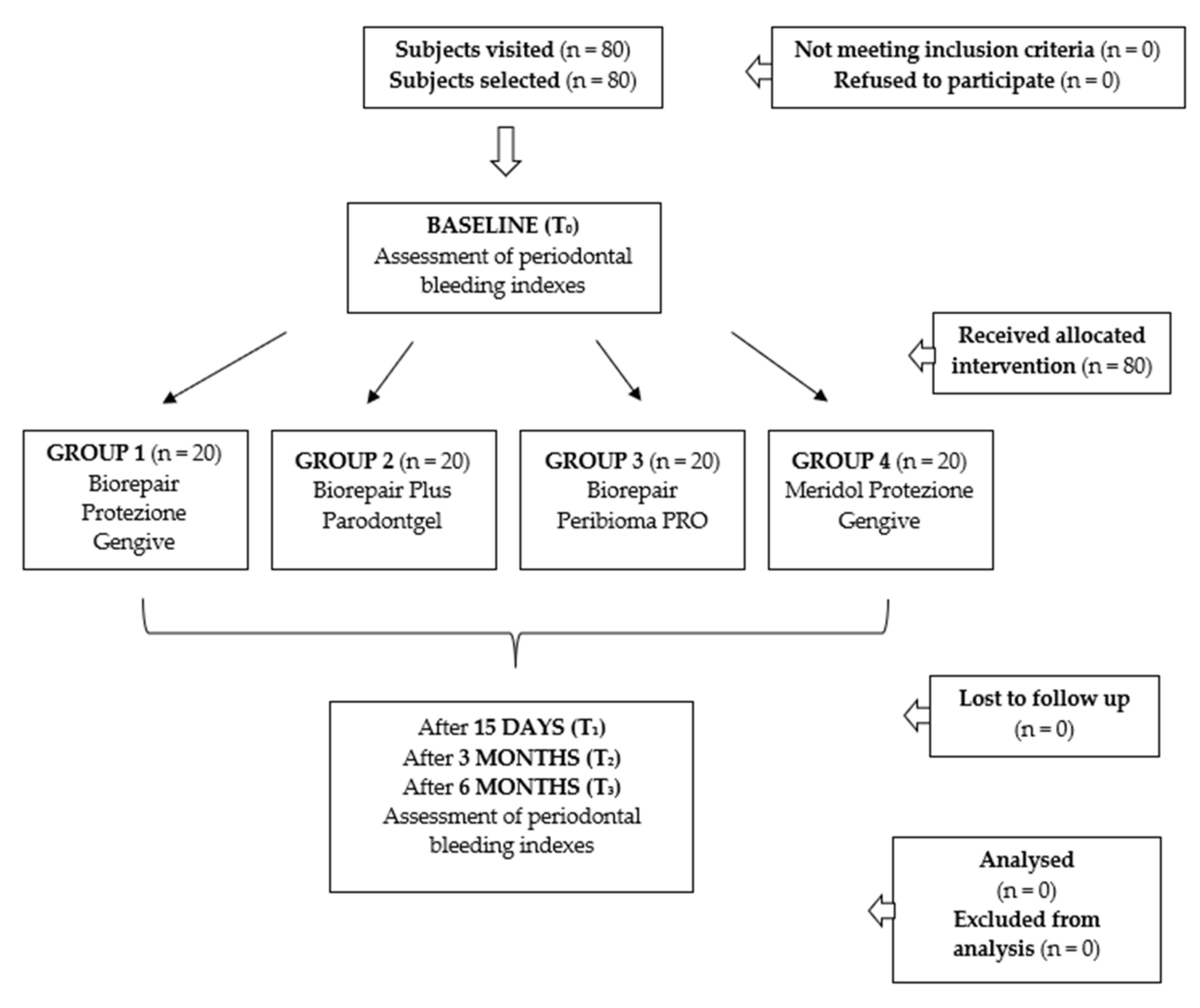
2.2.1. Trial Design
2.2.2. Participants
2.2.3. Interventions and Outcomes
2.2.4. Sample Size
2.2.5. Randomization and Blinding
2.2.6. Statistical Methods
3. Results
3.1. Bleeding on Probing (BoP, %)
3.2. Full-Mouth Bleeding Score (FMBS, 0–3)
3.3. Modified Sulcus Bleeding Index (mSBI, 0–3)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baelum, V.; Lopez, R. Periodontal disease epidemiology—Learned and unlearned? Periodontology 2000 2013, 62, 37–58. [Google Scholar] [CrossRef] [PubMed]
- Checchi, V.; Pascolo, G. Microbiological Response to Periodontal Therapy: A Retrospective Study. Open Dent. J. 2018, 12, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Berezow, A.B.; Darveau, R.P. Microbial shift and periodontitis. Periodontology 2000 2011, 55, 36–47. [Google Scholar] [CrossRef]
- Mombelli, A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontology 2000 2018, 76, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Checchi, L.; Montevecchi, M.; Gatto, R.M.; Moreschi, A.; Checchi, V. Clinical efficacy of two toothbrushes with different bristles. Int. J. Dent. Hyg. 2007, 5, 242–246. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Mombelli, A.; van Oosten, M.A.; Schurch, E., Jr.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Bertoldi, C.; Forabosco, A.; Lalla, M.; Generali, L.; Zaffe, D.; Cortellini, P. How Intraday Index Changes Influence Periodontal Assessment: A Preliminary Study. Int. J. Dent. 2017, 2017, 7912158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlemann, H.R.; Son, S. Gingival sulcus bleeding—A leading symptom in initial gingivitis. Helv. Odontol. Acta 1971, 15, 107–113. [Google Scholar]
- Farhadian, N.; Bidgoli, M.; Jafari, F.; Mahmoudzadeh, M.; Yaghobi, M.; Miresmaeili, A. Comparison of Electric Toothbrush, Persica and Chlorhexidine Mouthwashes on Reduction of Gingival Enlargement in Orthodontic Patients: A Randomised Clinical Trial. Oral Health Prev Dent. 2015, 13, 301–307. [Google Scholar]
- Scribante, A.; Poggio, C.; Gallo, S.; Riva, P.; Cuocci, A.; Carbone, M.; Arciola, C.R.; Colombo, M. In Vitro Re-Hardening of Bleached Enamel Using Mineralizing Pastes: Toward Preventing Bacterial Colonization. Materials 2020, 13, 818. [Google Scholar] [CrossRef] [Green Version]
- Deng, Z.L.; Szafrański, S.P.; Jarek, M.; Bhuju, S.; Wagner-Döbler, I. Dysbiosis in chronic periodontitis: Key microbial players and interactions with the human host. Sci. Rep. 2017, 7, 3703–3715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, F.O.; Cortelli, S.C.; Costa, A.A.; Cyrino, R.M.; Cortelli, J.R.; Miranda Cota, L.O. Impact of compliance during periodontal maintenance therapy on oral health-related quality of life: A 6-year follow-up. J. Dent. 2019, 83, 50–55. [Google Scholar] [CrossRef]
- Cosola, S.; Giammarinaro, E.; Genovesi, A.M.; Pisante, R.; Poli, G.; Covani, U.; Marconcini, S. A short-term study of the effects of ozone irrigation in an orthodontic population with fixed appliances. Eur. J. Paediatr. Dent. 2019, 20, 15–18. [Google Scholar] [PubMed]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Iauk, L.; Lo Bue, A.M.; Milazzo, I.; Rapisarda, A.; Blandino, G. Antibacterial activity of medicinal plant extracts against periodontopathic bacteria. Phytother. Res. 2003, 17, 599–604. [Google Scholar] [CrossRef]
- Mahendra, J.; Mahendra, L.; Muthu, J.; John, L.; Romanos, G.E. Clinical effects of subgingivally delivered spirulina gel in chronic periodontitis cases: A placebo controlled clinical trial. J. Clin. Diagn. Res. 2013, 7, 2330–2333. [Google Scholar] [CrossRef]
- Palombo, E.A. Traditional Medicinal Plant Extracts and Natural Products with Activity against Oral Bacteria: Potential Application in the Prevention and Treatment of Oral Diseases. Evid. Based Complement. Alternat. Med. 2011, 2011, 680354. [Google Scholar] [CrossRef] [Green Version]
- Maniyar, R.; Umashankar, G.K. Effectiveness of Spirulina Mouthwash on Reduction of Dental Plaque and Gingivitis: A Clinical Study. Int. J. Pharm. Pharm. Sci. 2017, 9, 136–139. [Google Scholar] [CrossRef]
- Lima, M.D.R.; Lopes, A.P.; Martins, C.; Brito, G.A.C.; Carneiro, V.C.; Goes, P. The Effect of Calendula officinalis on Oxidative Stress and Bone Loss in Experimental Periodontitis. Front. Physiol. 2017, 8, 440. [Google Scholar] [CrossRef] [Green Version]
- Berlutti, F.; Pilloni, A.; Pietropaoli, M.; Polimeni, A.; Valenti, P. Lactoferrin and oral diseases: Current status and perspective in periodontitis. Ann. Stomatol. 2011, 2, 10–18. [Google Scholar]
- Varela-López, A.; Navarro-Hortal, M.D.; Giampieri, F.; Bullón, P.; Battino, M.; Quiles, J.L. Nutraceuticals in Periodontal Health: A Systematic Review on the Role of Vitamins in Periodontal Health Maintenance. Molecules 2018, 23, 1226. [Google Scholar] [CrossRef] [Green Version]
- Joint FAO/WHO Working Group. Working Group Report on Drafting Guidelines for the Evaluation of Probiotics in Food; Joint FAO/WHO Working Group: London, ON, Canada, 2002. [Google Scholar]
- İnce, G.; Gürsoy, H.; İpçi, Ş.D.; Cakar, G.; Emekli-Alturfan, E.; Yılmaz, S. Clinical and Biochemical Evaluation of Lozenges Containing Lactobacillus reuteri as an Adjunct to Non-Surgical Periodontal Therapy in Chronic Periodontitis. J. Periodontol. 2015, 86, 746–754. [Google Scholar] [CrossRef]
- De Almada, C.N.; Almada, C.N.; Martinez, R.C.R.; Sant’Ana, A.S. Paraprobiotics: Evidences on their ability to modify biological responses, inactivation methods and perspectives on their application in foods. Trends Food Sci. Technol. 2016, 58, 96–114. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Celmare, R.L.; D’Antò, V.; Grippaudo, C.; Gandini, P.; Sfondrini, M.F. Orthodontic debonding and tooth sensitivity of anterior and posterior teeth. Angle Orthod. 2020, 90, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Product | Manufacturer | Ingredients |
|---|---|---|
| Biorepair Gum Protection | Coswell SPA, 40050 Funo di Argelato, Bologna, Italy | Aqua, Zinc Hydroxyapatite (microRepair®) 15%, Glycerin, Sorbitol, Silica, Cellulose Gum, Cocamidopropyl Betaine, Aroma, Sodium Myristoyl Sarcosinate, Sodium Methyl Cocoyl Taurate, Hamamelis Virginiana Leaf Extract, Spirulina Platensis Extract, Calendula Officinalis Flower Extract, Sodium Hyaluronate, Sodium Saccharin, Phenoxyethanol, Benzyl Alcohol, Sodium Benzoate, Potassium Sorbate, Limonene, Eugenol, Cl 16255. |
| Biorepair Plus Parodontgel | Coswell SPA, 40050 Funo di Argelato, Bologna, Italy | Aqua, Zinc Hydroxyapatite (microRepair®) 20%, Glycerin, Sorbitol, Hydrated Silica, Silica, Cocamidopropyl Betaine, Cellulose Gum, Aroma, Lactoferrin, Sodium Myristoyl Sarcosinate, Sodium Methyl Cocoyl Taurate, Hamamelis Virginiana Leaf Extract, Spirulina Platensis Extract, Calendula Officinalis Flower Extract, Zinc PCA, Sodium Hyaluronate, Tocopheryl Acetate, Retinyl Palmitate, Sodium Saccharin, Phenoxyethanol, Benzyl Alcohol, Sodium Benzoate, Potassium Sorbate, Limonene, CI 77891. |
| Biorepair Peribioma PRO | Coswell SPA, 40050 Funo di Argelato, Bologna, Italy | Aqua, Zinc Hydroxyapatite *, Sorbitol, Glycerin, Hydrated Silica, Silica, Cocamidopropyl Betaine, Cellulose Gum, Aroma, Pistacia Lentiscus (Mastic) Gum Oil, Ascorbic Acid, Tocopheryl Acetate, Retynil Palmitate, Sodium Hyaluronate, Hamamelis Virginiana Leaf Extract, Spirulina Platensis Extract, Calendula Officinalis Flower Extract, Eucaliptus Globulus Leaf Oil, Bifidobacterium Breve *, Lactobacillus Acidophilus *, Sodium Myristoyl Sarcosinate, Sodium Methyl Cocoyl Taurate, Phenoxyethanol, Benzyl Alcohol, Sodium Benzoate, Sodium Saccharin, Potassium Sorbate, Maltodextrin, Citric Acid, Helianthus Annuus Seed Oil, BHT, Limonene, Eugenol, CI 77891, CI 73360. |
| Meridol Gum Protection | Colgate-Palmolive, 00148 Roma, Italy | Aqua, Sorbitol, Hydrated Silica, siliva Dimethyl Silylate, Hydroxyethylcellulose, Cocamidopropyl Betaine, PEG-40 Hydrogenated Castor Oil, Aroma, Sodium Gluconate, Limonene, PEG-3 Tallow Aminoproprylamine, Olafur, Stannous Fluoride, Sodium Saccharin, Potassium Hydroxide, Hydrochloric Acid, CI 74160. |
| Appointment | Procedures |
|---|---|
| Baseline (T0) |
Group 2: Biorepair Plus Parodontgel Group 3: Biorepair Peribioma PRO Group 4: Meridol Gum Protection |
| After 15 days (T1) After 3 months (T2) After 6 months (T3) |
|
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| 1—15%MR | T0 | 91.85 | 12.42 | 55 | 100 | 100 | A |
| T1 | 50.75 | 13.70 | 25 | 52 | 75 | B | |
| T2 | 47.95 | 12.77 | 23 | 49.5 | 67 | B | |
| T3 | 44.85 | 13.39 | 20 | 43.5 | 65 | B | |
| 2—20%MR | T0 | 89.45 | 14.21 | 55 | 97.5 | 100 | A |
| T1 | 29.75 | 8.17 | 15 | 27.5 | 50 | C | |
| T2 | 28.30 | 8.89 | 13 | 28 | 48 | C | |
| T3 | 25.55 | 8.11 | 10 | 25 | 43 | C | |
| 3—20%MR+Paraprobiotics | T0 | 77.00 | 21.30 | 40 | 80 | 100 | A |
| T1 | 24.00 | 17.59 | 0 | 20 | 60 | C | |
| T2 | 20.40 | 14.56 | 0 | 10 | 48 | C | |
| T3 | 13.15 | 11.94 | 0 | 10 | 37 | D | |
| 4—Control | T0 | 81.25 | 17.23 | 50 | 80 | 100 | A |
| T1 | 69.25 | 18.157 | 40 | 67.5 | 100 | E | |
| T2 | 68.15 | 16.468 | 43 | 69 | 98 | E | |
| T3 | 57.95 | 9.8434 | 40 | 58 | 75 | E |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| 1—15%MR | T0 | 1.54 | 0.52 | 0.5 | 1.5 | 3 | A |
| T1 | 1.11 | 0.48 | 0.5 | 1 | 2.3 | B | |
| T2 | 1.05 | 0.51 | 0.4 | 0.8 | 2.1 | B | |
| T3 | 0.84 | 0.53 | 0.3 | 0.5 | 2 | B | |
| 2—20%MR | T0 | 1.53 | 0.66 | 0.5 | 1.5 | 3 | A |
| T1 | 0.93 | 0.50 | 0 | 0.9 | 2 | B | |
| T2 | 0.92 | 0.67 | 0 | 0.65 | 2 | B | |
| T3 | 0.76 | 0.63 | 0 | 0.5 | 1.8 | B | |
| 3—20%MR+Paraprobiotics | T0 | 1.52 | 0.56 | 0.9 | 1.4 | 2.9 | A |
| T1 | 0.38 | 0.33 | 0 | 0.4 | 1.2 | C | |
| T2 | 0.38 | 0.21 | 0 | 0.4 | 0.8 | C | |
| T3 | 0.26 | 0.17 | 0 | 0.2 | 0.5 | C | |
| 4—Control | T0 | 1.83 | 0.78 | 0.5 | 2 | 3 | A |
| T1 | 1.675 | 0.7482 | 0.5 | 1.75 | 3 | A | |
| T2 | 1.665 | 0.7372 | 0.8 | 1.5 | 3 | A | |
| T3 | 1.49 | 0.7333 | 0 | 1.45 | 2.8 | A |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| 1—15%MR | T0 | 1.69 | 0.38 | 1 | 1.75 | 2.3 | A |
| T1 | 1.12 | 0.49 | 0 | 1 | 2 | B | |
| T2 | 1.10 | 0.45 | 0.2 | 1 | 1.8 | B | |
| T3 | 0.90 | 0.47 | 0.2 | 1 | 1.7 | B | |
| 2—20%MR | T0 | 1.67 | 0.66 | 0.5 | 1.8 | 3 | A |
| T1 | 0.83 | 0.51 | 0 | 0.9 | 2 | B | |
| T2 | 0.72 | 0.57 | 0 | 0.65 | 2 | B | |
| T3 | 0.53 | 0.51 | 0 | 0.5 | 1.8 | B | |
| 3—20%MR+Paraprobiotics | T0 | 1.96 | 0.76 | 0 | 2 | 3 | A |
| T1 | 0.84 | 0.63 | 0 | 0.8 | 2.75 | B | |
| T2 | 0.82 | 0.74 | 0 | 0.65 | 2.54 | B | |
| T3 | 0.60 | 0.62 | 0 | 0.55 | 2.3 | B | |
| 4—Control | T0 | 2.03 | 0.78 | 1 | 1.8 | 3 | A |
| T1 | 1.85 | 0.7037 | 1 | 1.6 | 3 | A | |
| T2 | 1.835 | 0.6907 | 0.7 | 1.65 | 3 | A | |
| T3 | 1.67 | 0.6449 | 0.6 | 1.5 | 2.8 | A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, A.; Gallo, S.; Maiorani, C.; Preda, C.; Chiesa, A.; Esposito, F.; Pascadopoli, M.; Scribante, A. Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial. Appl. Sci. 2021, 11, 8586. https://0-doi-org.brum.beds.ac.uk/10.3390/app11188586
Butera A, Gallo S, Maiorani C, Preda C, Chiesa A, Esposito F, Pascadopoli M, Scribante A. Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial. Applied Sciences. 2021; 11(18):8586. https://0-doi-org.brum.beds.ac.uk/10.3390/app11188586
Chicago/Turabian StyleButera, Andrea, Simone Gallo, Carolina Maiorani, Camilla Preda, Alessandro Chiesa, Francesca Esposito, Maurizio Pascadopoli, and Andrea Scribante. 2021. "Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial" Applied Sciences 11, no. 18: 8586. https://0-doi-org.brum.beds.ac.uk/10.3390/app11188586