2. Materials and Methods
We have developed an online self-designed questionnaire, written in the Romanian language, using the Google Forms application. After the initial pool of questionnaire items, qualified experts from the Romanian Society of Dental and Maxillofacial Prosthetics review them to evaluate content validity, make sure questions are accurate, free of item construction problems, with no content that may be perceived as offensive or biased by a particular subgroup of respondents. The prefinal version of the questionnaire was pilot tested on a small sample (20 participants), after completing the questionnaire the respondent was asked verbally by an interviewer to elaborate on what they thought each questionnaire item and their corresponding response meant. In November 2020 the questionnaire has been approved and validated.
The questionnaire was distributed via email to 190 specialists in dental prosthetics, members of the Romanian Society of Dental and Maxillofacial Prosthetics; they were invited to answer the questions, only if they have had performed fixed rehabilitation on implants by that time. Additionally, it was distributed in social media (Facebook, Instagram) professional groups of dental technique groups with a short presentation of the purpose of the study and a request for an agreement in order to process the data obtained from the answers. For two months the questionnaire had registered online answers until it reached the number of 55 doctors and 55 dental technicians (the size of the study group corresponding to the Schoenbaum’s study [
9] for doctors and technicians).
The 18 questions were structured in three sections as following: respondents’ demographic data, data regarding the design and fabricating technique of the fixed rehabilitation on implants and data regarding the complications of the fixed rehabilitation on implants. The following demographic information of the respondents was collected: years in practice, type of practice and total number of arches treated. The questions were developed with multiple answers and the possibility to detail other possible options. Where ambiguity or unique answers were expected, “other” was provided as an option, with a request for qualification from the respondent. Efforts were made to minimize the effect of response bias.
Data were downloaded as an Excel file and then submitted into a statistical analysis software (SPSS 5) where they were processed in descriptive analysis. After that, the possible correlations between the variables were tested by applying the Likelihood Ratio test and Linear by Linear association test between pairs of answers to every two questions, the Kruskal-Wallis H test for the differences between three answer groups and postdoc tests for the differences between two answer groups, looking for the significant statistic alternatives for a value of p < 0.05. The tests were applied for correlations between the questions of each questionnaire and also between the clinicians’ and dental technicians’ answers. The continuous data were tested for normality using Shapiro-Wilk test.
3. Results
The results are presented using statistic descriptive analysis of frequency, for each questionnaire partition, in comparative tables and graphics.
The average age of the doctors in the study is 36 (±9.100) and 67.3% are females, for the technicians’ lot the mean age is 28.6 (±8.59) and the sex repartition is 52.7% males (
Table 1).
Although the technicians’ study lot is young, 40% of them have already fabricated over 20 fixed prosthetic restorations with implant support and 50.9% have made less than 9. A percent of 41.8% of the doctors have made more than 20 full-arch prosthetic rehabilitations and almost the same percentage have treated less than 10 cases.
In order to test the correlation between the age of the respondent and the total number of prosthetic rehabilitations, the Kruskal-Wallis H test has been applied for the difference between the three groups of answers and the postdoc test for the difference between the two groups of answers. For the technicians’ group significant results were obtained (
Table 2).
Concerning the treatment plan responsibility, 61.2% of the dental prosthodontic specialists claimed their leading role, and 28.5% affirmed that it is a shared responsibility with the dental technicians. The dental technicians’ study group had a different opinion: half of them declared that the treatment plan is decided by both the dentist and technician, 29.1% declared that they are the leaders in the team and 5% that they manage the entire treatment plan.
When we analyze the retaining system used for fixed restorations on implants, the majority of the prosthodontic specialists prefer screw-retained restorations (80.5%). In the dental laboratory in 67.3% of cases the screw-retained restoration is the most frequently requested system for fixed prosthetic restoration on implant support.
61.8% of the dentists use the titanium abutment, followed by the custom abutment. Two respondents have chosen the “other” option, indicating the straight and the angled abutment and also the calcinable one. Regarding the most requested type of abutment in the lab, the leader is the titanium abutment (83.6%), while the customized abutment is requested only in 16.4% of the cases (
Table 3).
For implant-supported fixed restorations like crowns and bridges, the most elected type of impression is the open tray technique with connected transfer copings, 40% of the clinicians use intraoral scanning and only 1.8% use plastic transfer copings. In the doctors’ study lot 67.6% use the open tray technique with connected transfer copings for the full arch fixed implant-supported restorations
Over 50% of the implant supported fixed restoration cases that arrive in the dental laboratory have used the open tray with connected transfer copings impression technique.
The Likelihood Ratio test for full arch fixed implant impression indicates a significant difference between the ratios that correlate the clinical experience and the open tray impression technique without connecting the transfer copings; 100% of the clinicians with over 10 years of experience have chosen this option.(Test Likehood Ratio, p value = 0.030179, Test: Linear-by-Linear Association, p value = 0.396511).
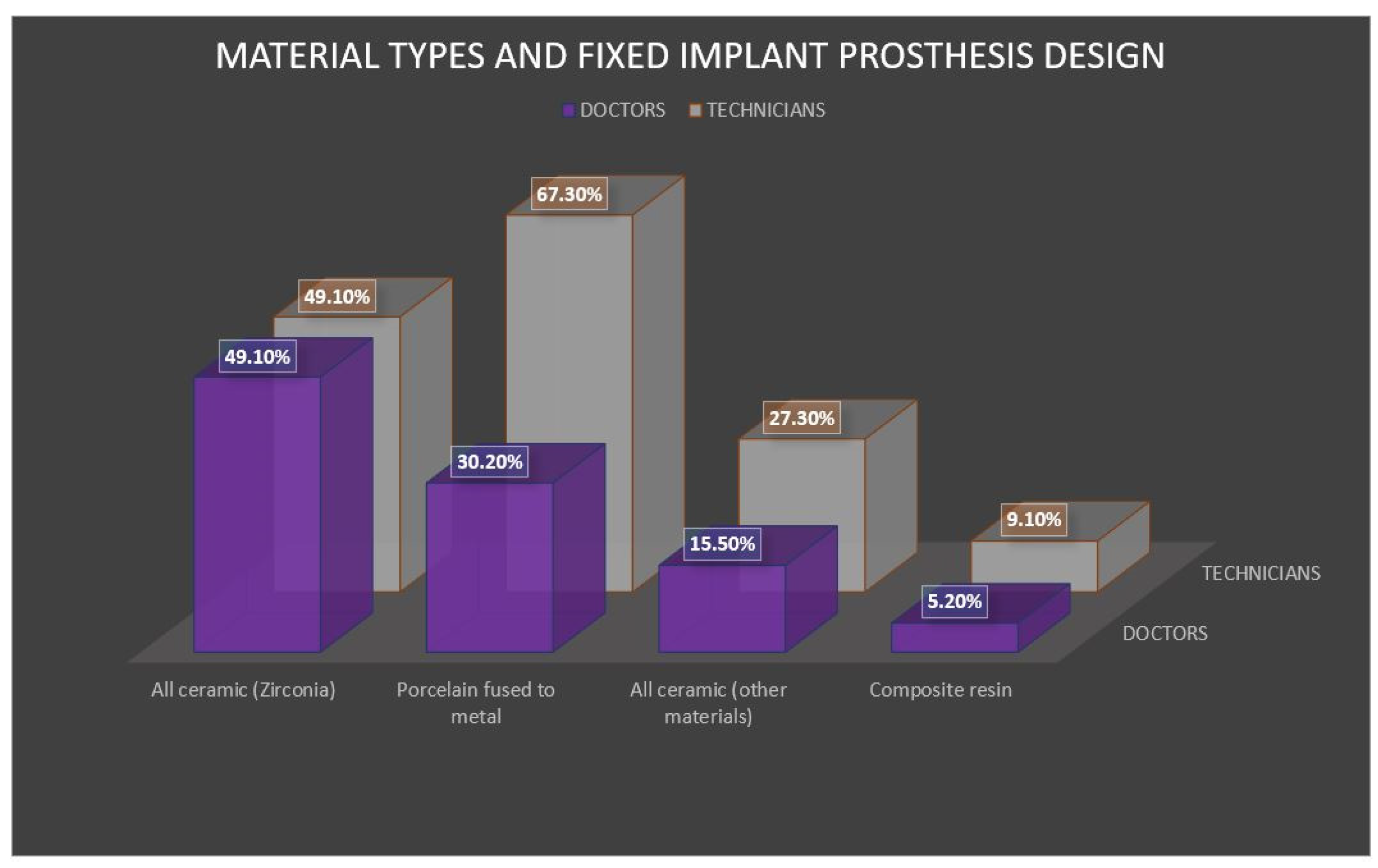
In the anterior region, the most frequently used material differs in the two study groups, according to the answers. The clinicians have chosen the all-ceramic zirconia crown as the leading restoration for the anterior, followed by the porcelain fused to metal crown, while the technicians have a reversed ratio. The results were similar to the ones from the Al Dosari study [
14]. The Japanese technicians reported 43.4% porcelain fused to metal and 27.1% full zirconia [
15] (
Figure 1 and
Figure 2).
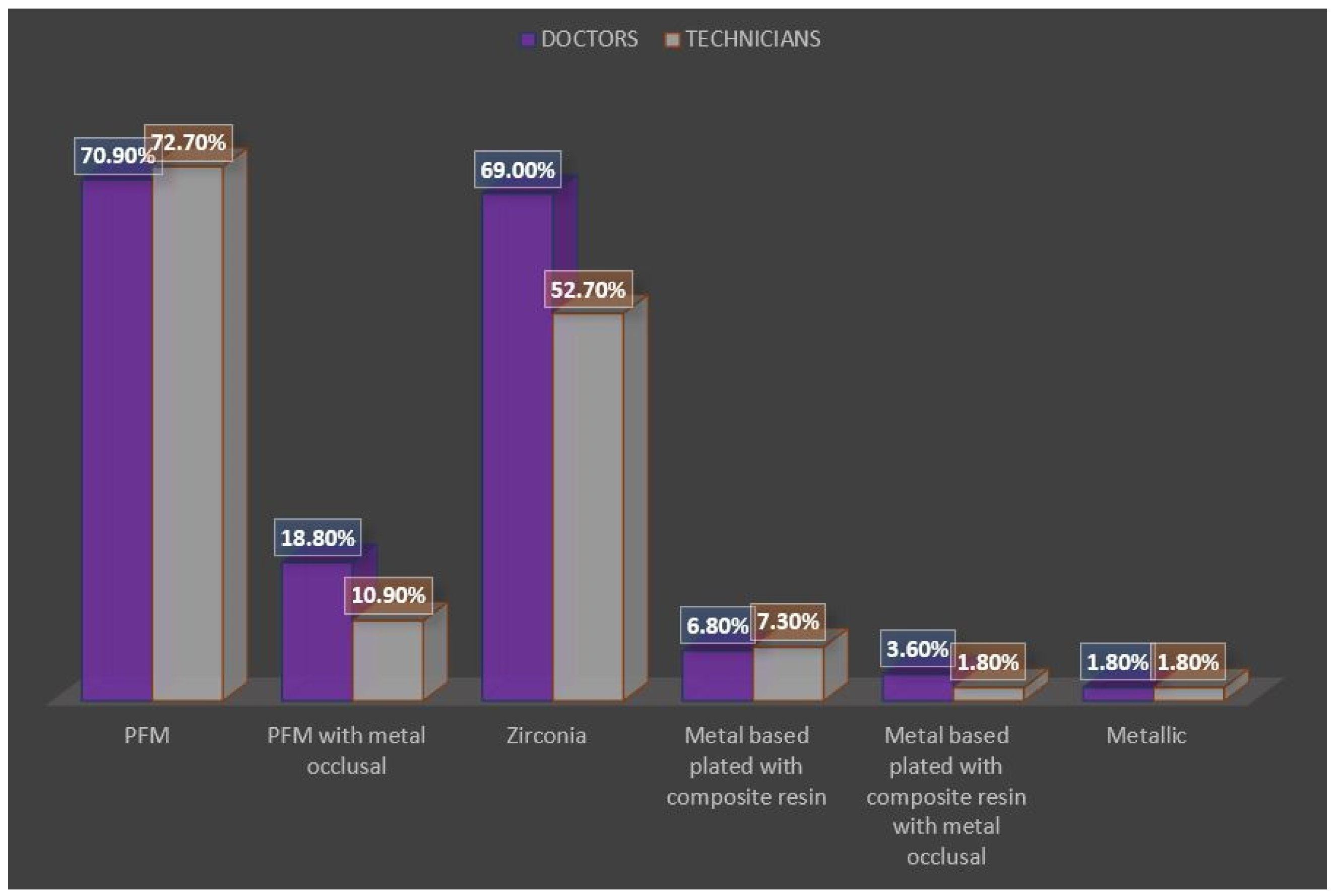
In the posterior zone, the most voted answers in both of the study groups were the porcelain fused to metal crown (72.7%), followed by the full zirconia crown (
Figure 3 and
Figure 4).
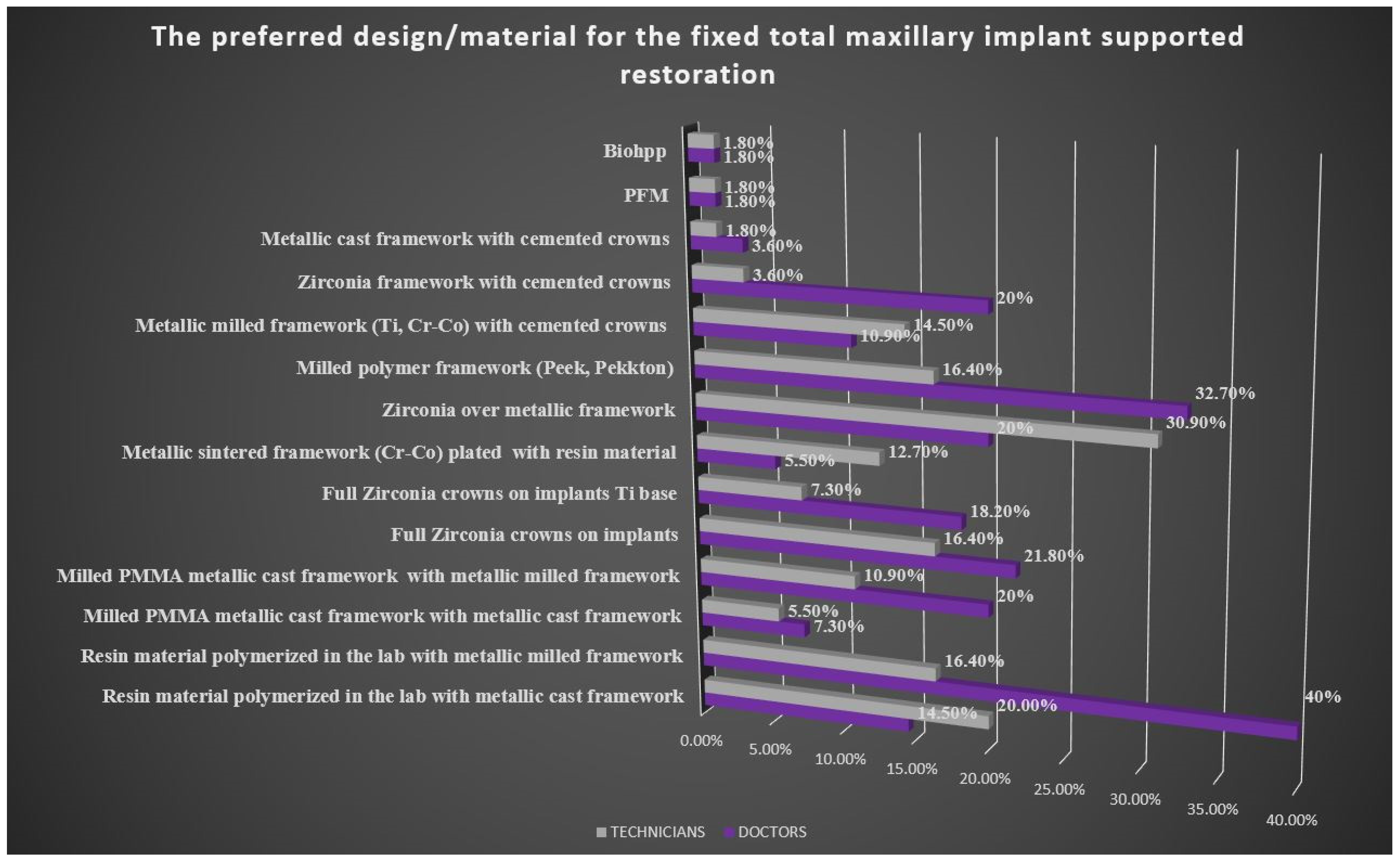
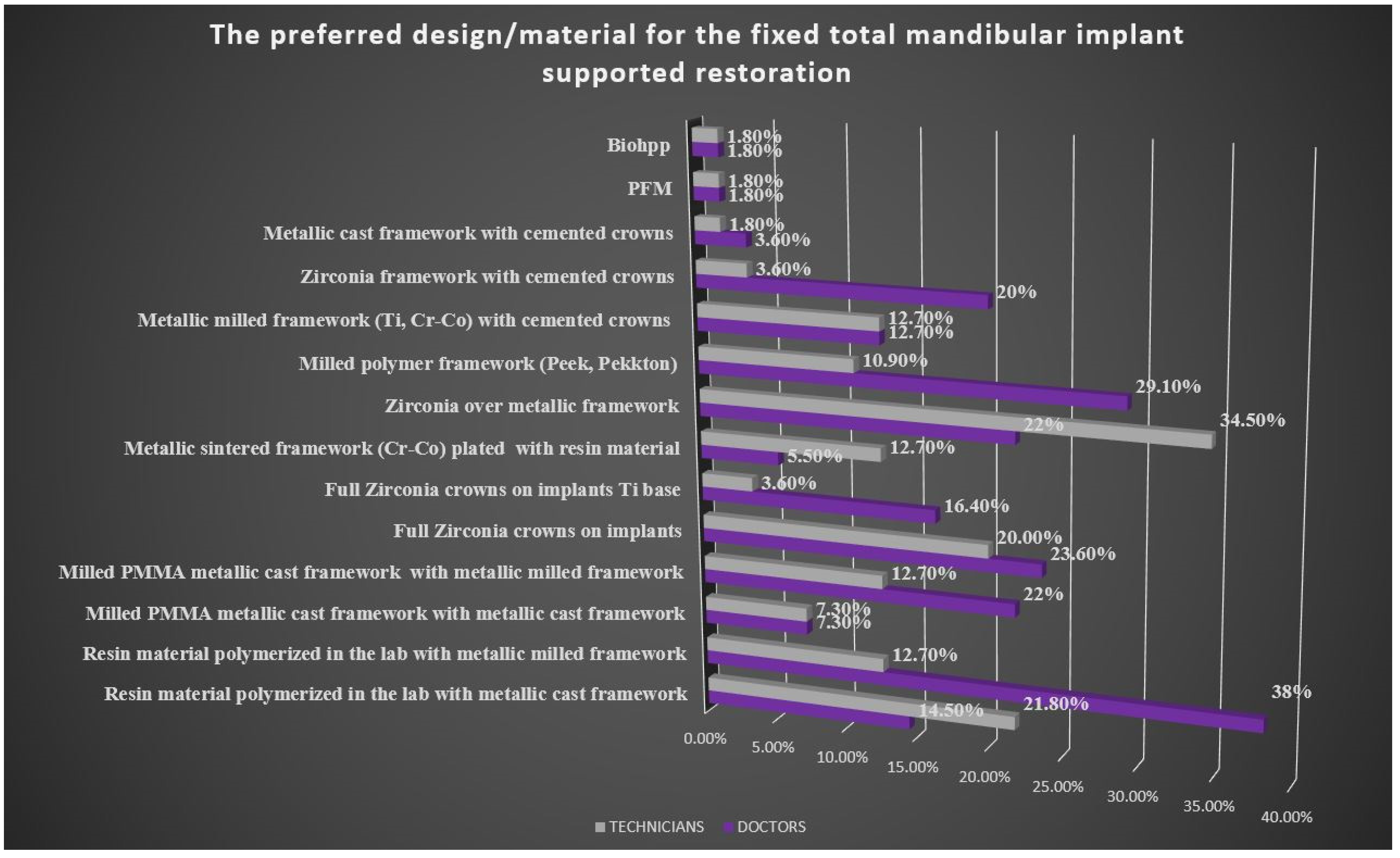
For the maxillary fixed restoration, the resin material polymerized in the laboratory, the acrylic teeth and the metallic framework gain 40% votes from the Romanian clinicians. In the mandible, both study lots voted in similar percentages the resin material polymerized in the laboratory, the acrylic teeth and the titanium framework, and, in the second place, the Romanian doctors have chosen the Cr-Co alloy milled framework. For full zirconia crowns on implants in maxillary restorations, the Likelihood Ratio test indicates a significant difference between ratios (33.3%, 28.6%, 0.0%, 0.0%), a linear tendency (a linear decrease in this case) which sometimes is statistically significant (p value = 0.025439) depending on the clinical experience. Most of the doctors who make this choice have under 10 years of clinical experience.
In the technicians’ lot, the answers for total fixed implant-supported restoration in the maxilla and in the mandible were similar, the most voted option was the milled metallic framework (Ti, Cr-Co) with cemented crowns, followed by the resin material polymerized in the laboratory, the acrylic teeth and the metallic cast framework option.
By testing the possible correlation between the design/the material preferred by the doctors for definitive total fixed implant supported maxillary prosthesis and the clinical experience, for associating the experience level and the choice of the resin material polymerized in the laboratory, the acrylic teeth and the metallic milled framework, the Likelihood Ratio indicates a significant difference in ratios (22.2%, 57.1%, 53.8%, 100%). A linear tendency (here a linear growth) is observed, sometimes depending on the clinical experience which is statistically significant (p value = 0.014189).
A linear growing tendency sometimes appears depending on the clinical experience; this combination is statistically significant (p value = 0.046517) when the restoration chosen is a milled metallic framework (Ti, Cr-Co) with cemented crowns for the maxillary definitive fixed implant supported prosthesis.
By testing the possible correlation between the design/the material preferred by the doctors for definitive total fixed implant-supported mandibular prosthesis and the clinical experience, a linear tendency (a linear growth here) has been identified, for using the resin material polymerized in the laboratory, the acrylic teeth and the metallic milled framework, depending on the clinical experience close to the significant line (p value = 0.060201).
A linear tendecy (here linear decrease) can be observed in the table, in the matter of using the material/design milled PMMA and metallic milled framework correlated with the clinical experience which is statistically significant (p value = 0.035997).
Furthermore, a linear tendency (a linear growth in this case) of using the material/design polymer milled framework (Peek, Pekkton) with cemented crowns is observed, with respect to the clinical experience which is significant statistically (
p value = 0.036145); this time most of the doctors who have chosen this option have more than 10 years of experience (
Table 4).
As to the growing linear tendency for using the material/the design metallic cast framework with cemented crowns related to the clinical experience, it proves to be significant statistically (p value = 0.013578); this is the option the experienced doctors have selected.
By testing the possible correlation between the design/the material preferred for definitive full-arch fixed mandibular prosthesis and the years of experience in the technician’s study group, the answers have revealed a linear tendency close to the significant limit: polymer milled framework (Peek, Pekkton) with cemented crowns and zirconia milled framework with cemented crowns in correlation with the years of experience.
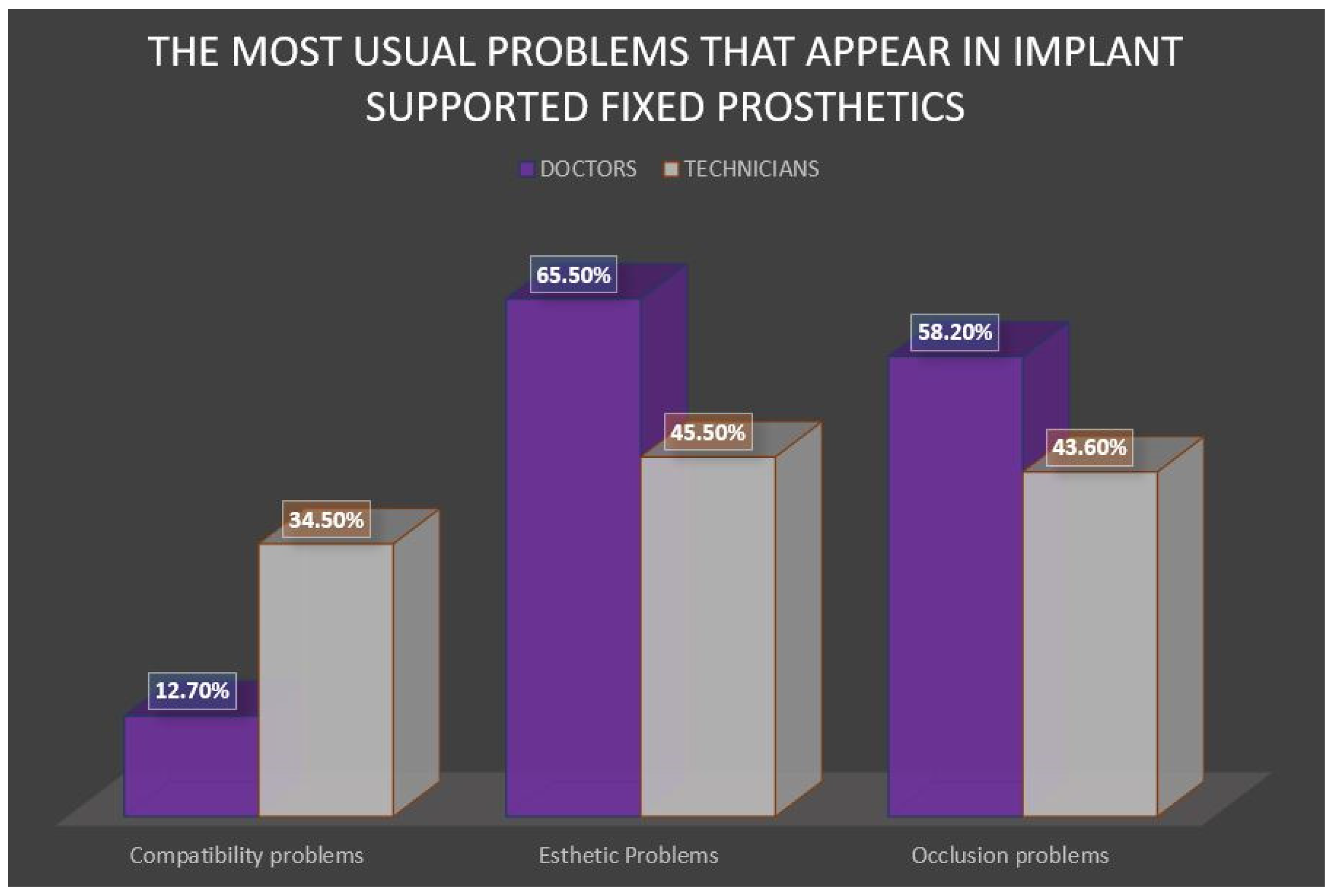
The most frequent complications (
Figure 5) reported by the doctors in the fixed prosthetic treatment with implant support are esthetic issues (65.6%), followed by occlusion problems (58.2%-more than a half of the doctors voted for it). The technicians reported in almost the same percent occlusion and esthetics complications, and in 12.7% problems related to implant compatibility.
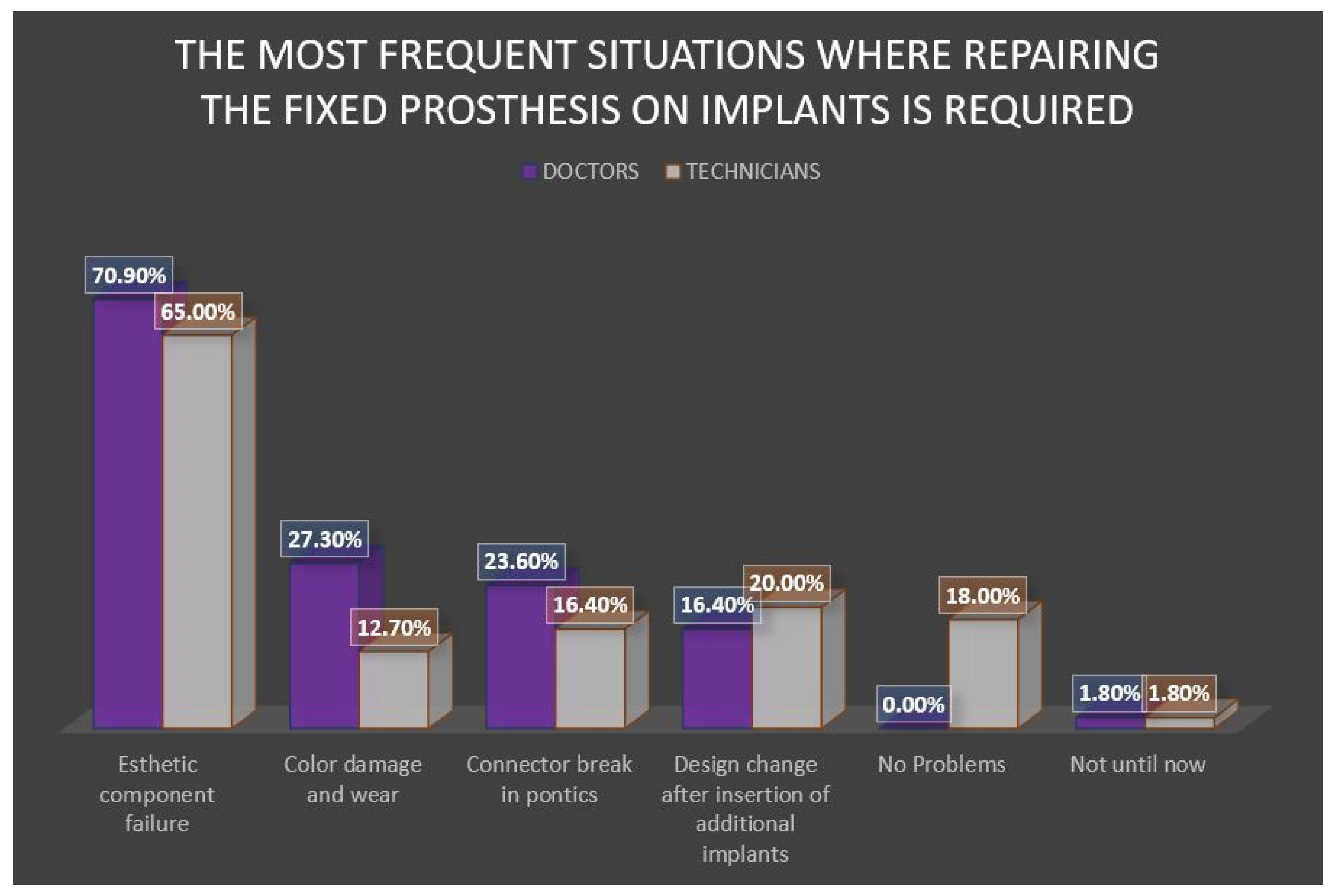
Regarding the repair request (
Figure 6) the first place in the doctor’s lot is taken by the esthetic component failure (70.9%). The result seems to correspond to the one from the technician’s study group; they have voted the failure of the esthetic component as the most common request for repairing/remaking the fixed partial prosthesis (65.6%), followed by a change of design associated to inserting additional implants (20%).
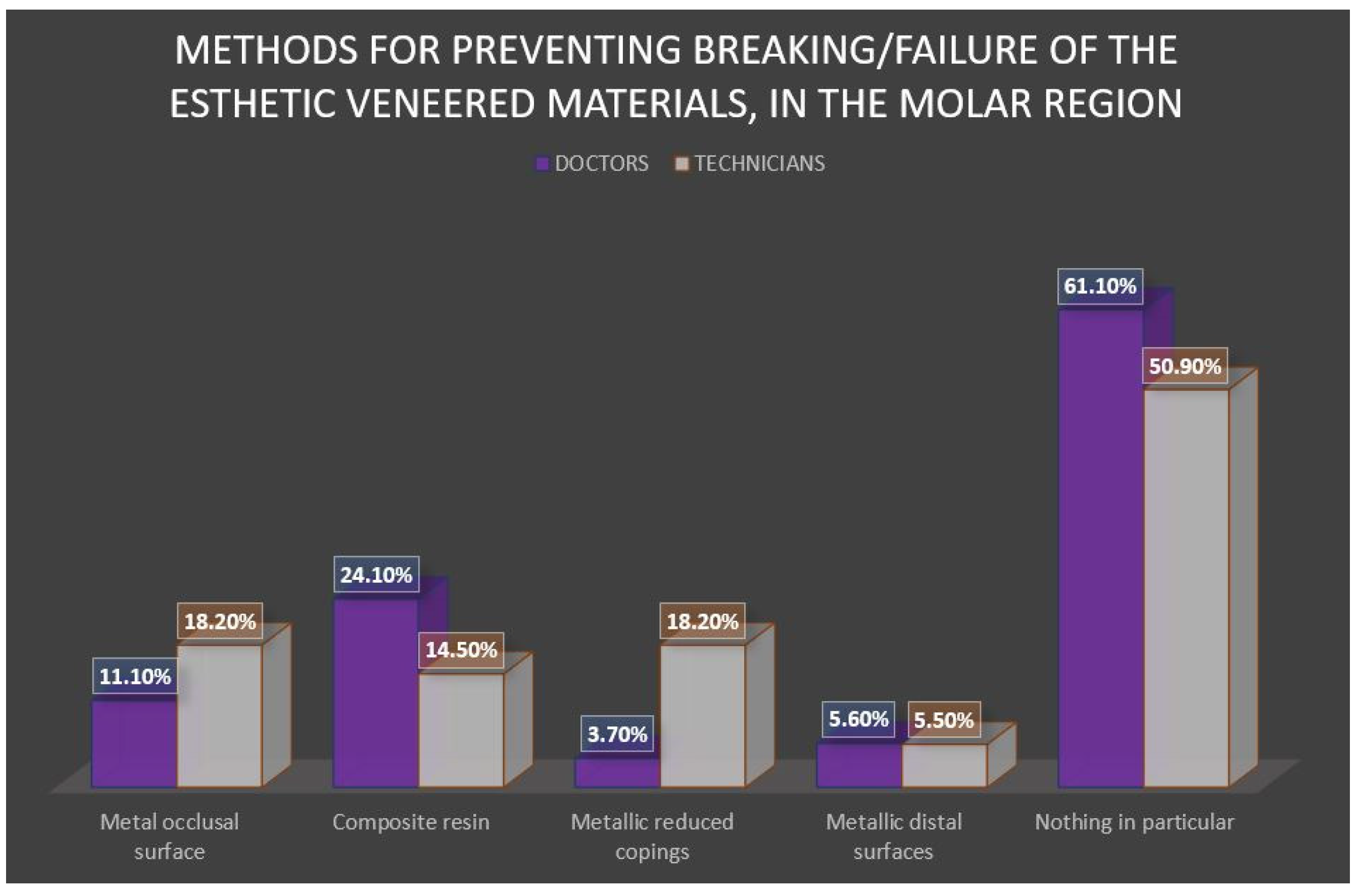
Nevertheless, 61.1% of the doctors don’t take any measures for preventing the fracture/failure of the esthetic component in the molar region. (
Figure 7) and 50.9% of the Romanian dental technicians don’t adopt any methods for preventing this in the posterior zone.
By testing the possible correlation between the design/the material preferred for full-arch fixed maxillary prosthesis with implant support and the most frequent situations the doctors request repairing the restoration, the significant statistical association has been observed between the reparation due to failure of the esthetic component and the metallic casted framework with cemented crowns used at the maxilla (
Table 5).
To determine how much the two professionals’ perspectives correspond, the Pearson Chi-Square test and the Fisher’s Exact test were applied, translating the statistical relevance at 0.05. The pairs of answers and the comparative statistical relevance that were significant have been exposed in
Table 6.
4. Discussion
Our study lot has an over-average experience in fabricating the fixed prosthetic treatment with implant support. In the attempt to find a correlation between the age of the respondent and the total number of implant-supported prosthetic restorations, we found that age was a significant variable in terms of the number of full-arch prosthetic restorations. The biggest difference has appeared between the group that made 1–9 restorations and the one with more than 20 restorations, a larger experience to approach these complex rehabilitations being obvious.
The treatment leading role item offered a different clinic versus lab perspective. While more than half of Romanian dentists claim the responsibility for the design decision, half of the dental technicians declare the common contribution of the two specialists. The situation is quite different from the study from Saudi Arabia, wherein 49% of the cases the dentist is managing the treatment plan [
14]. In Hagiwara ’s study from 2015 [
13] 39.3% assign the doctor as a leader, whereas 28.9% of the respondents’ report that there is a doctor- technician teamwork. However, due to the fact that dental technicians have claimed in this study also that in 14.5% of the cases they step forward, some problems concerning the doctor’s training in implant restoration treatment planning arise. Repercussions involve prosthetic complications that occur during the treatment plan.
Analyzing results for the type of the preferred retaining system, the screw-retained restorations were the most voted in both groups. This result is similar with Al Saleh’s study [
15] but opposite to Chowdhary’s study [
10] where the cement-retained prosthesis was the favorite restoration of most of the dentists across the countries surveyed. Furthermore, the percent obtained for the lab Romanian professionals is different from the Japanese study [
13] where 61.4% of the technicians declare a higher demand for cement-retained restorations.
Regarding the most used type of abutment, the answers are different in the two groups, the chosen options being titanium and custom abutment, but in different quantum. There is a statistically significant difference between the two categories of answers: the technicians declared a higher percent of titanium abutment 83.6% versus 61.8% in doctor’s options) while clinicians declare that they request custom abutment in 32.7% of cases (versus 16.4% percent of technicians’ reports). The custom abutment using precious metals is an excellent option for the healing phase of the soft tissue in the implant treatment and the final restoration fits perfectly. Therefore, this disparity needs to be addressed in dental and technical education curricula. Results obtained are different from a similar study from Saudi Arabia in 2018 [
14], where a technician’s study lot stated they use equally titanium abutments (37%) and custom abutments (34%), while the CAD/CAM abutments were more than a half. The percentage for titanium abutment is fairly high compared to a third stated by Hagiwara et al. (2015) in a study from Japan [
13].
The elected technique for the full and partial arch implant impression was open tray technique with connected transfer copings, results which are similar to Schoenbaum’s research [
8] A study from Israel (2017) [
9] states that prosthodontic specialists used custom open tray, whereas the generalist dentist used the stock tray impression. In our analysis, statistical tests show a positive correlation be-tween dentists’ experience and open tray impression technique without connecting the transfer copings for full arch implant impression. However, there is a statistical difference regarding the digital impression technique for implant-supported crowns or bridges and the open tray technique with connected transfer copings for full arch impression. Even that doctors vote for them, technicians report that they are not sent so often to the dental laboratory.
A disagreement between the two specialists was raised also in the matter of favor-ite anterior implant restoration, all-ceramic zirconia crown (similar to the results of Al Dosari’s study [
14], and porcelain fused to the metal crown being the chosen options for dentists versus technicians. Japanese technicians reported 43.4% porcelain fused to metal and 27.1% full zirconia [
13]. Full zirconia crowns on implants were a solution that statistically showed a correlation with the clinical experience, most of the doctors making this choice having under 10 years of clinical experience. This result may be explained by the rising interest in digital dentistry and tendency of young doctors to try new technologies.
For the posterior restoration solution, the choice of the two members of the team was porcelain fused to metal crown followed by the full zirconia crown. The answers were compared to Al Dosari’s study [
14], where the percentages registered for the full zirconia crown and for the porcelain fused to the metal crown with the metallic occlusal surface were equal. In the Asian dental laboratory [
13] 31.4% is attributed to the porcelain fused to metal crown, and the second place is taken by the metal-based plated with composite resin full esthetic crown, which in our study only takes 9.1%.
Regarding the maxillary and mandibular full-arch fixed implant restoration, the resin material polymerized in the lab, acrylic teeth, and metallic milled framework solution gained votes from the Romanian clinicians. This prosthetic option was statistically associated with clinical experience. Besides their physical property’s improvement from the last years, as the wear resistance and the discoloration, the indirect composite resin has become one of the main choices for plating materials that bonds chemically to titanium; this happens because of the increased number of CAD/CAM designed titanium framework and the porcelain, in this case, is not reliable. This option offers the advantage of direct intraoral repair if needed, in case of fissures or fractures of esthetic components and can absorb a bigger shock from an occlusal force compared to porcelain [
16]. However, the resin material polymerized in the laboratory, acrylic teeth, and metallic milled framework solution was reported in only 18% percent in an American study [
8] for the maxilla. They have preferred zirconia crowns on a titanium framework (33%). These differences came from the content of education prosthodontic curricula and also depend on the technological level of dental laboratories. Another explanation for this difference could be the price of the abovementioned prosthodontic solutions because Romanian health insurance in dentistry is very limited.
Regarding favorite full arch implant restoration solutions, technicians’ vote went to the milled metallic framework (Ti, Cr-Co) with cemented crowns. The analysis of our two groups of the study shows a disagreement between members of the prosthodontic team concerning the selection of the option resin material polymerized in the lab, acrylic teeth, and metallic milled framework option (doctors declare to use it in 40% of the cases, whereas the technicians declare to receive re-quests for it in 18.2% of the cases) and zirconia crowns on titanium base (preferred by some doctors, and ignored by all the technicians, in both upper and lower jaw).
Statistical data revealed that the clinical experience is correlated with maxillary prosthetic options like milled metallic framework (Ti, Cr-Co) with cemented crowns and polymer milled framework (Peek, Pekkton) with cemented crowns, metallic cast framework with cemented crowns. These solutions were chosen by dentists with more years of practice, while option like resin material polymerized in the lab, acrylic teeth, and metallic milled framework for the mandible is chosen by young doctors. In the technicians’ group for full arch years of experience were a significant factor as well for fixed mandibular prosthesis, in choosing polymer milled framework (Peek, Pekkton) with cemented crowns and zirconia milled framework with cemented crowns solutions.
A similar frequent complication and repair request report has been registered in the two groups of the study, esthetic issues being most reported, as some other studies concluded [
13,
14]. Technicians also declared in similar percent occlusion problems, which are in the second place in the doctor’s ranking- complications that needs specific research about the technique, material and lab transfer of mandibular- maxillary relations in Romanian dental practice. In the matter of the most usual problems encountered in the fixed prosthetics with implant support, the technicians voted the compatibility matter more than the doctors. This situation is explained by the fact that the technological procedures request different materials with similar processing indices [
16,
17].
Despite the possible failure of the esthetic component, neither of the two members of the prosthodontic team take any measures for preventing the fracture/failure of the esthetic component in the posterior region. This is a result that explained the esthetic issues complications and failures and has to be addressed in future research and dental education. While only 18.2% of Romanian technicians chose to use the metallic occlusal surfaces or the reduced metallic frames, in the Arabic study [
14], in 30% of the cases they use reduced metallic frames and composite resin, and in the Japanese one [
13], 36% of them use reduced metallic frames or the metallic distal half of the prosthetic restoration. Searching correlations between prosthetic options and complications, our data show a statistically significant as-sociation between repairing requests due to failure of the esthetic component and the metallic casted framework with cemented crowns used at the maxilla. A lot of variables like type and quality of cementation, design and technologic workflow of the metal framework, vertical prosthetic space needs to be analyzed in future re-search to find the answer for this association.
Communication and a uniform updated level of knowledge in the prosthodontic team is very important for a predictable workflow [
18,
19]. Dental technicians’ education varies from a country to another, and there is a variety of methods used to train their practical abilities. For example, a poll amongst Great Britain dental technicians made by Bower et al. [
20] uncovers the fact that while subjects are reading commercial magazines edited for dental technicians, their subscriptions to academic journals in the prosthodontics field are not so frequent and two-thirds of the respondents have never attended a training course regarding the fabrication technique. As opposed to this, the Japanese dental technicians are compelled to be enrolled in an academic society, participate in its meetings, and have a subscription to its journal [
13]. The variety in doctor’s answers also show the need of clinical training improvement in dental schools [
21,
22,
23] and we stress the importance of increasing the educational exposure and training in dental laboratory procedures [
24,
25].
Our study has a limited number of participants (110), with a prosthodontic specialized sample of doctors, from one organization in one geographic area, in a limited period of time. A limit of our research is also the heterogeneity of the technicians’ group with diversity in expertise and dental lab equipment.
In future research, we intend to develop the questionnaire items to include patients’ preferences in the selection of fixed prosthodontics appliances into consideration. The patient opinion is of great value for the dentist and makes changes in the selection of prothesis, especially in the aesthetic area.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}