
Characterizing the Mechanical Performance of a Bare-Metal Stent with an Auxetic Cell Geometry



 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
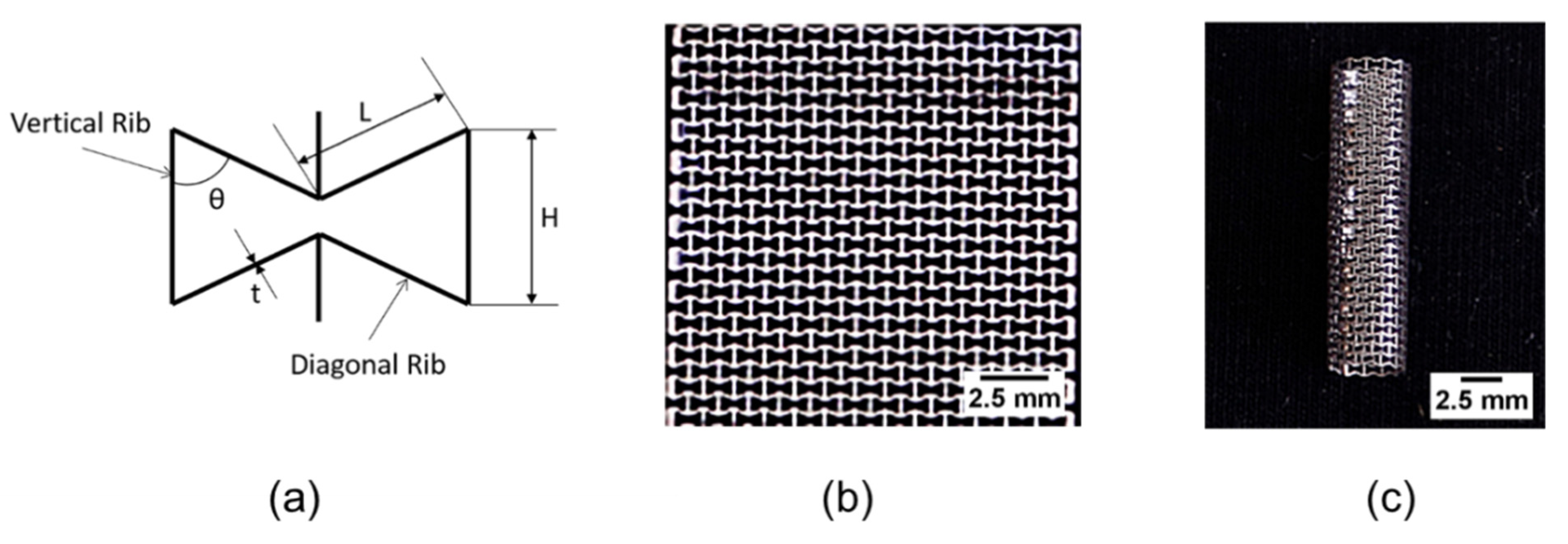
2.1. Production of the Stents
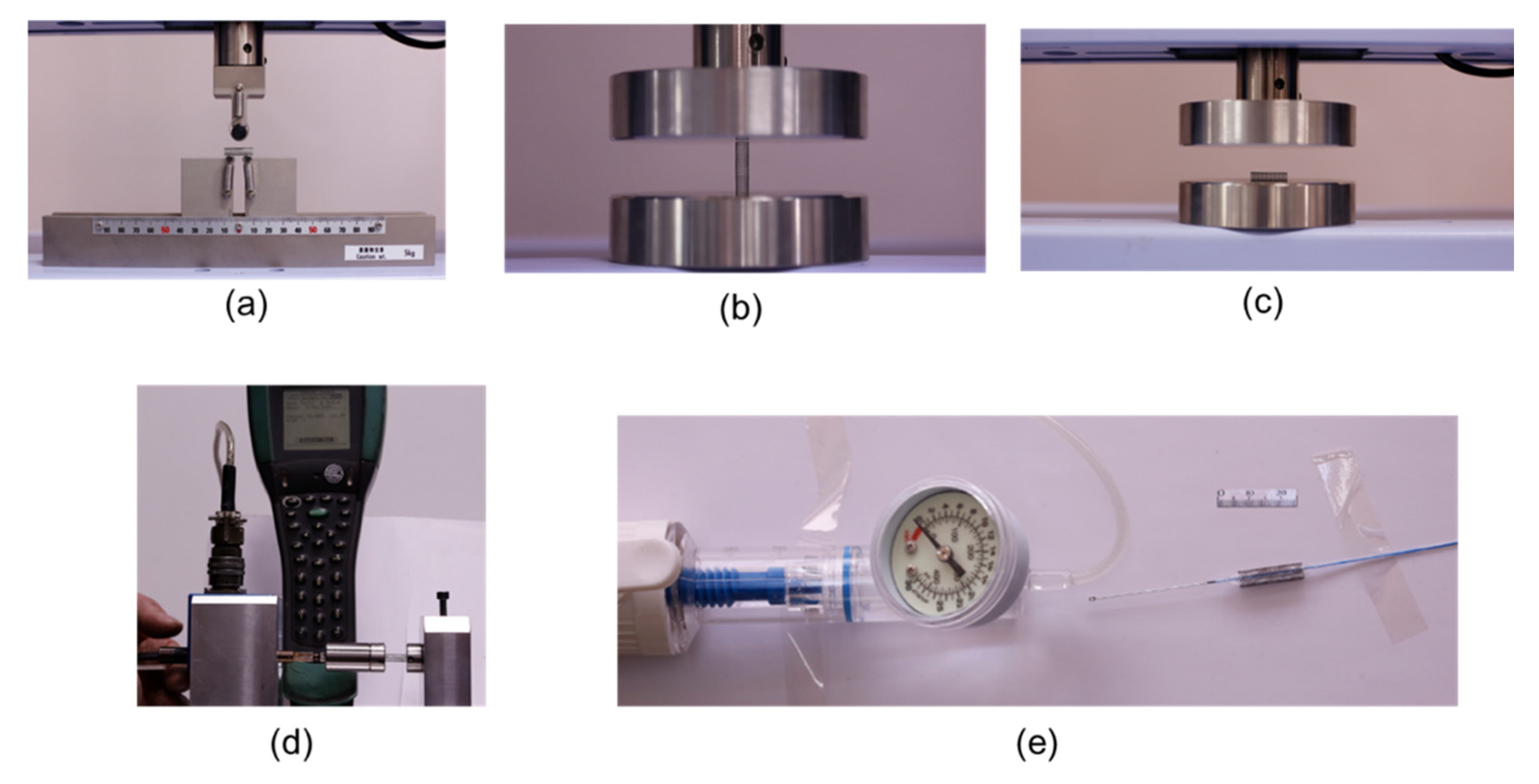
2.2. Mechanical Testings
2.2.1. Three-Point Bending
2.2.2. Radial Strength
2.2.3. Torsion
2.2.4. Radial Expansion Testing
2.3. Finite Element Analysis-Simulations
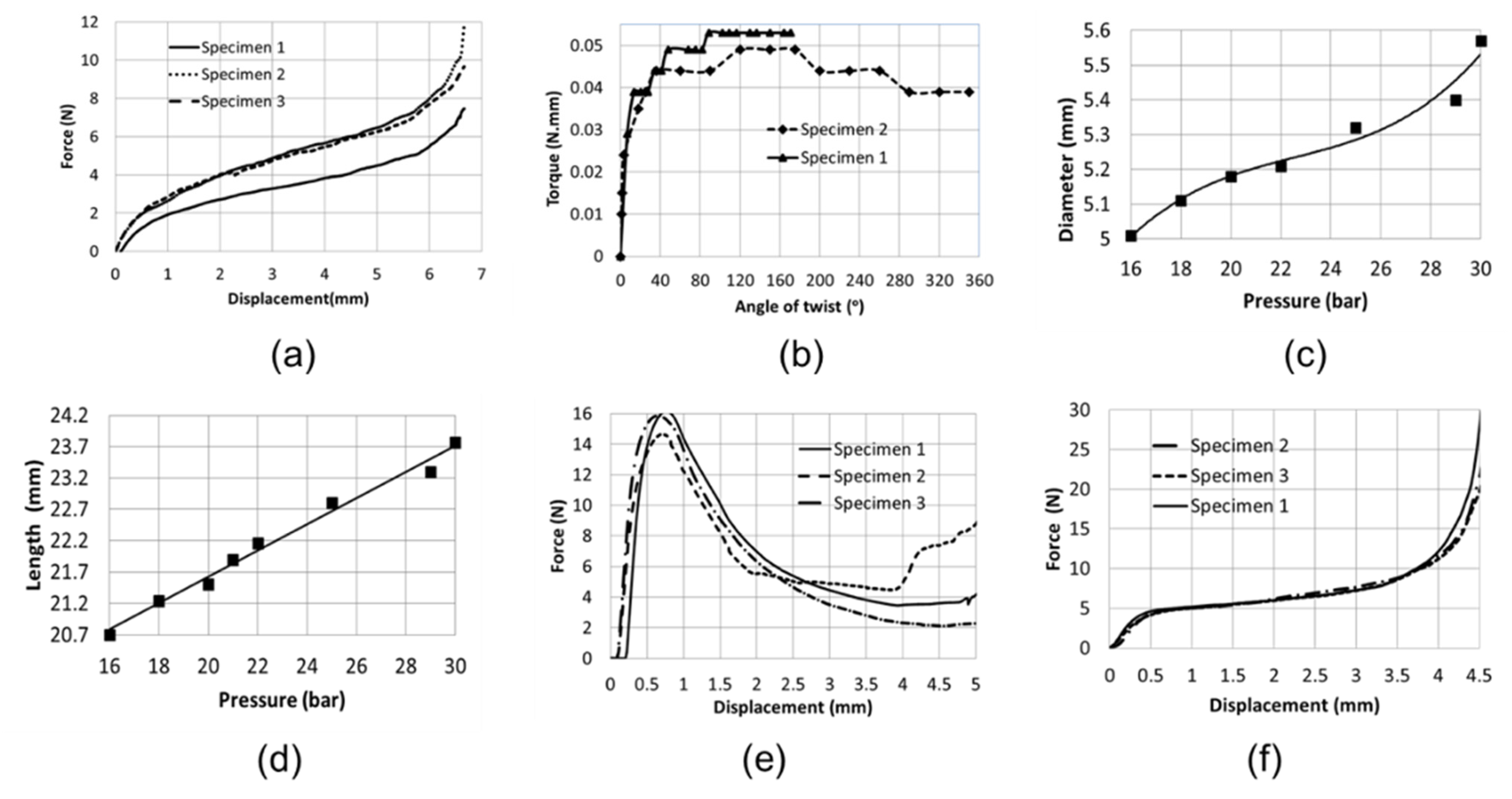
3. Results
3.1. Three-Point Bending
3.2. Torsion
3.3. Radial Expansion/Catheter Testing
3.4. Longitudinal/Lateral Compression
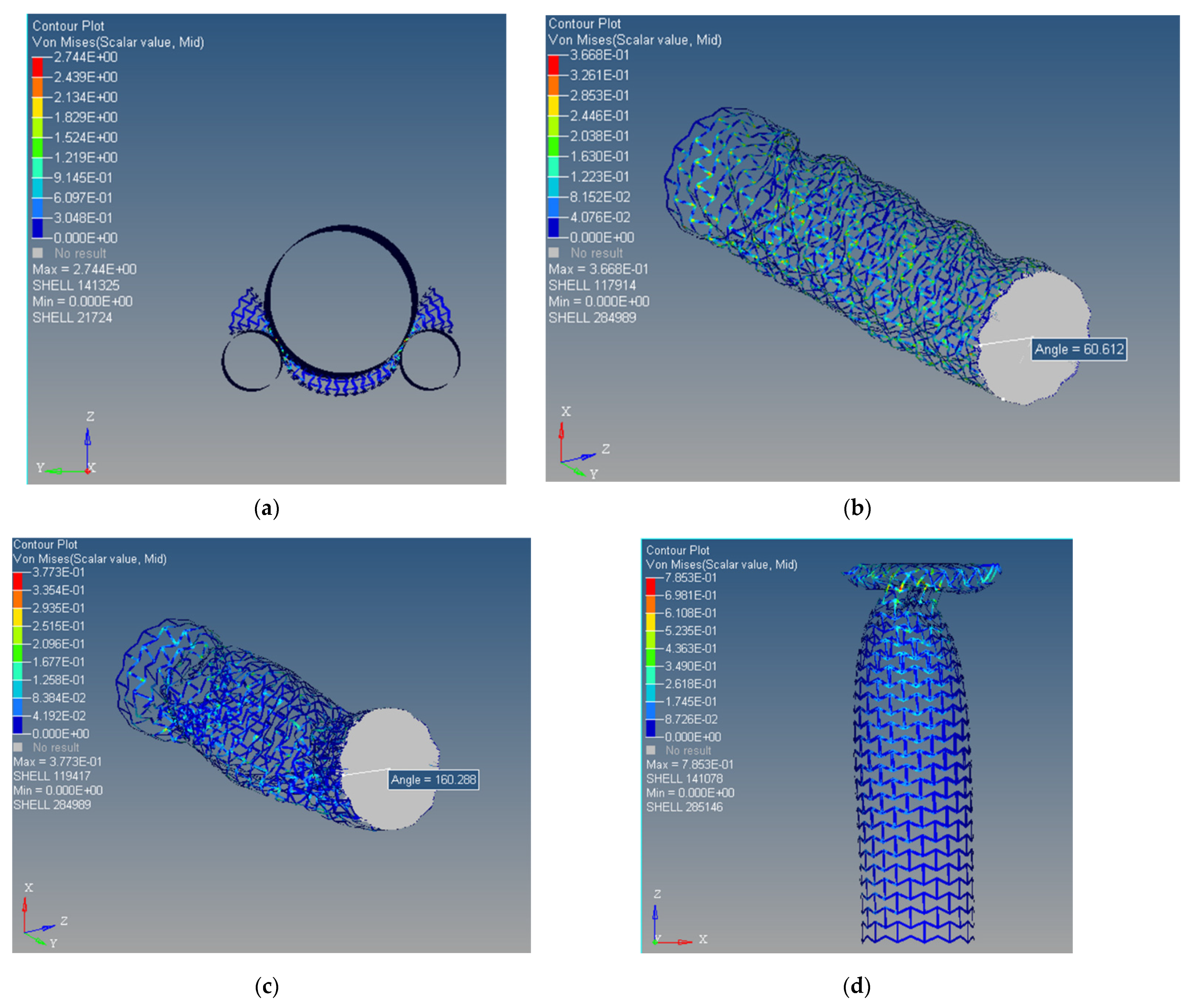
3.5. Finite Element Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dobrin, P.B. Mechanical properties of arteries. Physiol. Rev. 1978, 58, 397–460. [Google Scholar] [CrossRef] [Green Version]
- Roy, C.S. The elastic properties of the arterial wall. J. Physiol. 2008, 3, 125–159. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.Y.; Han, B.; Lamm, S.D.; Fierro, C.A.; Han, H.C. Effects of elastin degradation and surrounding matrix support on artery stability. Am. J. Physiol. Circ. Physiol. 2012, 302, H873–H884. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Han, H.C. Mechanical buckling of artery under pulsatile pressure. J. Biomech. 2012, 45, 1192–1198. [Google Scholar] [CrossRef] [Green Version]
- Chesnutt, J.K.W.; Han, H.C. Tortuosity triggers platelet activation and thrombus formation in microvessels. J. Biomech. Eng. 2011, 133, 121004. [Google Scholar] [CrossRef] [PubMed]
- Driver, M. Coatings for cardiovascular devices: Coronary stents. In Coatings for Biomedical Applications; Woodhead Publishing: Cambridge, UK, 2012; pp. 223–250. [Google Scholar]
- Duda, S.H.; Wiskirchen, J.; Tepe, G.; Bitzer, M.; Kaulich, T.W.; Stoeckel, D.; Claussen, C.D. Physical properties of endovascular stents: An experimental comparison. J. Vasc. Interv. Radiol. 2000, 11, 645–654. [Google Scholar] [CrossRef]
- Dyet, J.F.; Watts, W.G.; Ettles, D.F.; Nicholson, A.A. Mechanical properties of metallic stents: How do these properties influ-ence the choice of stent for specific lesions? Cardiovasc. Interv. Radiol. 2000, 23, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.; Serruys, P.W. Coronary stents: Current status. J. Am. Coll. Cardiol. 2010, 56, S1–S42. [Google Scholar] [CrossRef] [Green Version]
- Maleckis, K.; Deegan, P.; Poulson, W.; Sievers, C.; Desyatova, A.; MacTaggart, J.; Kamenskiy, A. Comparison of femoropopliteal artery stents under axial and radial compression, axial tension, bending, and torsion deformations. J. Mech. Behav. Biomed. Mater. 2017, 75, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Borhani, S.; Hassanajili, S.; Tafti, S.H.A.; Rabbani, S. Cardiovascular stents: Overview, evolution, and next generation. Prog. Biomater. 2018, 7, 175–205. [Google Scholar] [CrossRef] [Green Version]
- Fischman, D.L.; Leon, M.B.; Baim, D.S.; Schatz, R.A.; Savage, M.P.; Penn, I.; Detre, K.; Veltri, L.; Ricci, D.; Nobuyoshi, M.; et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N. Engl. J. Med. 1994, 331, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.R.; O’Sullivan, M. Mechanisms of angioplasty and stent restenosis: Implications for design of rational therapy. Pharmacol. Ther. 2001, 91, 149–166. [Google Scholar] [CrossRef]
- Vos, N.S.; Fagel, N.D.; Amoroso, G.; Herrman, J.-P.R.; Patterson, M.S.; Piers, L.H.; van der Schaaf, R.J.; Slagboom, T.; Vink, M.A. Paclitaxel-coated balloon angioplasty versus drug-eluting stent in acute myocardial infarction: The REVELATION Ran-domized Trial. JACC Cardiovasc. Interv. 2019, 12, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Bezrouk, A.; Hosszu, T.; Hromadko, L.; Olmrova, Z.; Kopecek, M.; Smutny, M.; Selke Krulichova, I.; Macak, J.M.; Kremlacek, J. Mechanical properties of a biodegradable self-expandable polydioxanone monofilament stent: In vitro force relaxation and its clinical relevance. PLoS ONE 2020, 15, e0235842. [Google Scholar] [CrossRef]
- Zilberman, M.; Eberhart, R.C. Drug-eluting bioresorbable stents for various applications. Annu. Rev. Biomed. Eng. 2006, 8, 153–180. [Google Scholar] [CrossRef] [Green Version]
- Charpentier, E.; Barna, A.; Guillevin, L.; Juliard, J.M. Fully bioresorbable drug-eluting coronary scaffolds: A review. Arch. Car-Diovasc. Dis. 2015, 108, 385–397. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, W.; Behrens, P.; Brandt, W.C.; Siewert, S.; Grabow, N.; Schmitz, K.P. In vitro performance investigation of bioresorb-able scaffolds–standard tests for vascular stents and beyond. Cardiovasc. Revasc. Med. 2016, 17, 375–383. [Google Scholar] [CrossRef]
- Available online: https://med.stanford.edu/news/all-news/2019/11/invasive-heart-treatments.html (accessed on 15 March 2020).
- Canfield, J.; Totary-Jain, H. 40 years of percutaneous coronary intervention: History and future directions. J. Pers. Med. 2018, 8, 33. [Google Scholar] [CrossRef] [Green Version]
- Yelamanchili, V.S.; Hajouli, S. Coronary Artery Stents, StatPearls. 2020. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK559287/ (accessed on 15 March 2020).
- Chaparro-Rico, B.D.M.; Sebastiano, F.; Cafolla, D. A smart stent for monitoring eventual restenosis: Computational fluid dynamic and finite element analysis in descending thoracic aorta. Machines 2020, 8, 81. [Google Scholar] [CrossRef]
- Javaid, I.; Julian, G.; Patrick, W.S. Coronary stents: Historical development, current status and future directions. Br. Med. Bull. 2013, 106, 193–211. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Phil, J. Drug-Eluting Bioresorbable Stents, Med-Tech Innovation, The Communication Hub for the UK and Irish Medical Device Industry. Available online: http://www.med-techinnovation.com (accessed on 10 March 2020).
- Colombo, A.; Giannini, F.; Briguori, C. Should We Still Have Bare-metal stents available in our catheterization laboratory? J. Am. Coll. Cardiol. 2017, 70, 607–619, Erratum in J. Am. Coll. Cardiol. 2017, 70, 1541. [Google Scholar] [CrossRef]
- Meraj, P.M.; Jauhar, R.; Singh, A. Bare metal stents versus drug eluting stents: Where do we stand in 2015? Curr. Treat. Options Cardiovasc. Med. 2015, 17, 393. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; van Hout, B.; Bonnier, H.; Legrand, V.; Garcia, E.; Macaya, C.; Sousa, E.; van der Giessen, W.; Colombo, A.; Sea-bra-Gomes, R.; et al. Randomised comparison of implantation of heparin-coated stents with balloon angioplasty in selected patients with coronary artery disease (Benestent II). Lancet 1998, 352, 673–681. [Google Scholar] [CrossRef]
- Biswas, S.; Duffy, S.J.; Lefkovits, J.; Andrianopoulos, N.; Brennan, A.; Walton, A.; Chan, W.; Noaman, S.; Shaw, J.A.; Dawson, L.; et al. Australian trends in procedural characteristics and outcomes in patients undergoing percutaneous coronary intervention for ST-elevation myocardial infarction. Am. J. Cardiol. 2018, 121, 279–288. [Google Scholar] [CrossRef]
- Rymer, J.A.; Harrison, R.W.; Dai, D.; Roe, M.T.; Messenger, J.C.; Anderson, H.V.; Peterson, E.D.; Wang, T.Y. Trends in bare-metal stent use in the United States in patients aged ≥65 years (from the CathPCI Registry). Am. J. Cardiol. 2016, 118, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Choubey, R.K.; Pradhan, S.K. Prediction of strength and radial recoil of various stents using FE analysis. Mater. Today Proc. 2020, 27, 2254–2259. [Google Scholar] [CrossRef]
- Cockerill, I.; See, C.W.; Young, M.L.; Wang, Y.; Zhu, D. Designing better cardiovascular stent materials: A learning curve. Adv. Funct. Mater. 2021, 31, 2005361. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.; Mintz, G.S.; Dussaillant, G.R.; Popma, J.J.; Pichard, A.D.; Satler, L.F.; Kent, K.M.; Griffin, J.; Leon, M.B. Patterns and mechanisms of in-stent restenosis. A serial intravascular ultrasound study. Circulation 1996, 94, 1247–1254. [Google Scholar] [CrossRef]
- Kastrati, A.; Mehilli, J.; Dirschinger, J.; Pache, J.; Ulm, K.; Schühlen, H.; Seyfarth, M.; Schmitt, C.; Blasini, R.; Neumann, F.J.; et al. Restenosis after coronary placement of various stent types. Am. J. Cardiol. 2001, 87, 34–39. [Google Scholar] [CrossRef]
- Nuhn, H.; Blanco, C.E.; Desai, T.A. Nanoengineered stent surface to reduce in-stent restenosis in vivo. ACS Appl. Mater. Interfaces 2017, 9, 19677–19686. [Google Scholar] [CrossRef]
- Guildford, A.; Santin, M.; Phillips, G.J. Cardiovascular stents. In Biomaterials and Devices for the Circulatory System; Woodhead Publishing: Cambridge, UK, 2010; pp. 173–216. [Google Scholar]
- Udriște, A.S.; Niculescu, A.-G.; Grumezescu, A.M.; Badila, E. Cardiovascular stents: A review of past, current, and emerging devices. Materials 2021, 14, 2498. [Google Scholar] [CrossRef] [PubMed]
- Bhullar, S.K. Influence of Negative Poisson′s Ratio on Stent Applications. Adv. Mater. 2013, 2, 42. [Google Scholar] [CrossRef]
- Ren, X.; Shen, J.; Ghaedizadeh, A.; Tian, H.; Xie, Y.M. A simple auxetic tubular structure with tuneable mechanical properties. Smart Mater. Struct. 2016, 25, 65012. [Google Scholar] [CrossRef]
- Liu, R.; Xu, S.; Luo, X.; Liu, Z. Theoretical and numerical analysis of mechanical behaviors of a metamaterial-based shape memory polymer stent. Polymers 2020, 12, 1784. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Song, X.; Liang, J.; Xia, R.; Qian, G.; Fang, D. Mechanical properties of anti-tetrachiral auxetic stents. Compos. Struct. 2018, 185, 381–392. [Google Scholar] [CrossRef]
- Ruan, X.L.; Wu, W.W.; Song, X.K.; Li, J.J.; Xia, R. Design and characterization of the 3D antichiral-reentrant hybrid structure for intravascular stent. Int. J. Appl. Mech. 2018, 10, 1850105. [Google Scholar] [CrossRef]
- Ning, X.; Yu, X.; Wang, H.; Sun, R.; Corman, R.E.; Li, H.; Lee, C.M.; Xue, Y.; Chempakasseril, A.; Yao, Y. Mechanically active materials in three-dimensional mesostructures. Sci. Adv. 2018, 4, eaat8313. [Google Scholar] [CrossRef] [Green Version]
- Wojciechowski, K.W. Two-dimensional isotropic system with a negative Poisson ratio. Phys. Lett. A 1989, 137, 60–64. [Google Scholar] [CrossRef]
- Wu, W.; Qi, M.; Liu, X.P.; Yang, D.Z.; Wang, W.Q. Delivery and release of nitinol stent in carotid artery and their interactions: A finite element analysis. J. Biomech. 2007, 40, 3034–3040. [Google Scholar] [CrossRef]
- Timmins, L.H.; Miller, M.W.; Clubb, F.J., Jr.; Moore, J.E., Jr. Increased artery wall stress post-stenting leads to greater intimal thickening. Lab. Investig. 2011, 91, 955–967. [Google Scholar] [CrossRef] [Green Version]
- Dumoulin, C.; Cochelin, B. Mechanical behaviour modelling of balloon-expandable stents. J. Biomech. 2000, 33, 1461–1470. [Google Scholar] [CrossRef]
- Lakes, R.S. Advances in negative Poisson’s ratio materials. Adv. Mater. 1993, 5, 293–296. [Google Scholar] [CrossRef]
- Evans, K.E.; Alderson, A. Auxetic materials: Functional materials and structures from lateral thinking! Adv. Mater. 2000, 12, 617–628. [Google Scholar] [CrossRef]
- Lakes, R.S. Negative Poisson’s ratio materials. Science 1987, 238, 551. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Li, Z.M.; Shi, W.; Xie, B.H.; Yang, M.B. Review on auxetic materials. J. Mater. Sci. 2004, 39, 3269–3279. [Google Scholar] [CrossRef]
- Lekesiz, H.; Bhullar, S.K.; Karaca, A.A.; Jun, M.B.G. Mechanical characterization of auxetic stainless steel thin sheets with reentrant structure. Smart Mater. Struct. 2017, 26, 085022. [Google Scholar] [CrossRef]
- Gatt, R.; Caruana-Gauci, R.; Attard, D.; Casha, A.R.; Wolak, W.; Dudek, K.; Mizzi, L.; Grima, J.N. On the properties of real fi-nite-sized planar and tubular stent-like auxetic structures. Phys. Status Solidi Basic Res. 2014, 251, 321–327. [Google Scholar] [CrossRef]
- Mizzi, L.; Attard, D.; Casha, A.; Grima, J.N.; Gatt, R. On the suitability of hexagonal honeycombs as stent geometries. Phys. Status Solidi Basic Res. 2014, 251, 328–337. [Google Scholar] [CrossRef]
- Amin, F.; Ali, M.N.; Ansari, U.; Mir, M.; Minhas, M.A.; Shahid, W. Auxetic coronary stent endoprosthesis: Fabrication and structural analysis. J. Appl. Biomater. Funct. Mater. 2015, 13, E127–E135. [Google Scholar] [CrossRef]
- Geng, L.C.; Ruan, X.L.; Wu, W.W.; Xia, R.; Fang, D.N. Mechanical properties of selective laser sintering (SLS) additive manu-factured chiral auxetic cylindrical stent. Exp. Mech. 2019, 59, 913–925. [Google Scholar] [CrossRef]
- Bhullar, S.K.; Ko, J.; Cho, Y.; Jun, M.B.G. Fabrication and characterization of nonwoven auxetic polymer stent. Polym.-Plast. Technol. Eng. 2015, 54, 1553–1559. [Google Scholar] [CrossRef]
- Wu, W.; Hu, W.; Qian, G.; Liao, H.; Xu, X.; Berto, F. Mechanical design and multifunctional applications of chiral mechanical metamaterials: A review. Mater. Des. 2019, 180, 107950. [Google Scholar] [CrossRef]
- Xue, H.; Luo, Z. Design of auxetic coronary stents by topology optimization. In Computational Biomechanics for Medicine; Springer: Cham, Switzerland, 2019; pp. 17–31. [Google Scholar]
- Prithipaul, P.K.M.; Kokkolaras, M.; Pasini, D. Assessment of structural and hemodynamic performance of vascular stents modelled as periodic lattices. Med. Eng. Phys. 2018, 57, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liulan, L.; Qingxi, H.; Xianxu, H.; Gaochun, X. Design and fabrication of bone tissue engineering scaffolds via rapid prototyping and CAD. J. Rare Earths 2007, 25, 379–383. [Google Scholar] [CrossRef]
- Snowhill, P.B.; Nosher, J.L.; Siegel, R.L.; Silver, F.H. Characterization of radial forces in Z stents. Investig. Radiol. 2001, 36, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, T.M.; Ainsworth, S.D.; Langan, E.M.; Taylor, S.; Snyder, B.; Cull, D.; Youkey, J.; Laberge, M. Effect of endovascular stent strut geometry on vascular injury, myointimal hyperplasia, and restenosis. J. Vasc. Surg. 2002, 36, 143–149. [Google Scholar] [CrossRef]
- De Bock, S.; Iannaccone, F.; De Beule, M.; Van Loo, D.; Vermassen, F.; Verhegghe, B.; Segers, P. Filling the void: A coalescent numerical and experimental technique to determine aortic stent graft mechanics. J. Biomech. 2013, 46, 2477–2482. [Google Scholar] [CrossRef]
- Prendergast, P.J.; Lally, C.; Daly, S.; Reid, A.J.; Lee, T.C.; Quinn, D.; Dolan, F. Analysis of prolapse in cardiovascular stents: A constitutive equation for vascular tissue and finite-element modelling. J. Biomech. Eng. 2003, 125, 692–699. [Google Scholar] [CrossRef]
- Jedwab, M.R.; Clerc, C.O. A study of the geometrical and mechanical properties of a self-expanding metallic stent-theory and experiment. J. Appl. Biomater. 1993, 4, 77–85. [Google Scholar] [CrossRef]
- Kalmar, G.; Hubner, F.; Voelker, W.; Hutzenlaub, J.; Teubner, J.; Poerner, T.; Suselbeck, T.; Borggrefe, M.; Haase, K.K. Radial force and wall apposition of balloon-expandable vascular stents in eccentric stenosis: An in vitro evaluation in a curved vessel model. J. Vasc. Interv. Radiol. 2002, 13, 499–508. [Google Scholar] [CrossRef]
- Fortier, A.; Gullapalli, V.; Mirshams, R.A. Review of biomechanical studies of arteries and their effect on stent performance. IJC Heart Vessel. 2014, 4, 12–18. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhullar, S.K.; Lekesiz, H.; Karaca, A.A.; Cho, Y.; Willerth, S.M.; Jun, M.B.G. Characterizing the Mechanical Performance of a Bare-Metal Stent with an Auxetic Cell Geometry. Appl. Sci. 2022, 12, 910. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020910
Bhullar SK, Lekesiz H, Karaca AA, Cho Y, Willerth SM, Jun MBG. Characterizing the Mechanical Performance of a Bare-Metal Stent with an Auxetic Cell Geometry. Applied Sciences. 2022; 12(2):910. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020910
Chicago/Turabian StyleBhullar, Sukhwinder K., Huseyin Lekesiz, Ahmet Abdullah Karaca, Yonghyun Cho, Stephanie Michelle Willerth, and Martin B. G. Jun. 2022. "Characterizing the Mechanical Performance of a Bare-Metal Stent with an Auxetic Cell Geometry" Applied Sciences 12, no. 2: 910. https://0-doi-org.brum.beds.ac.uk/10.3390/app12020910