
The Association between Influenza Vaccination and Stroke Risk in Patients with Hypertension: A Nationwide Population-Based Study

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
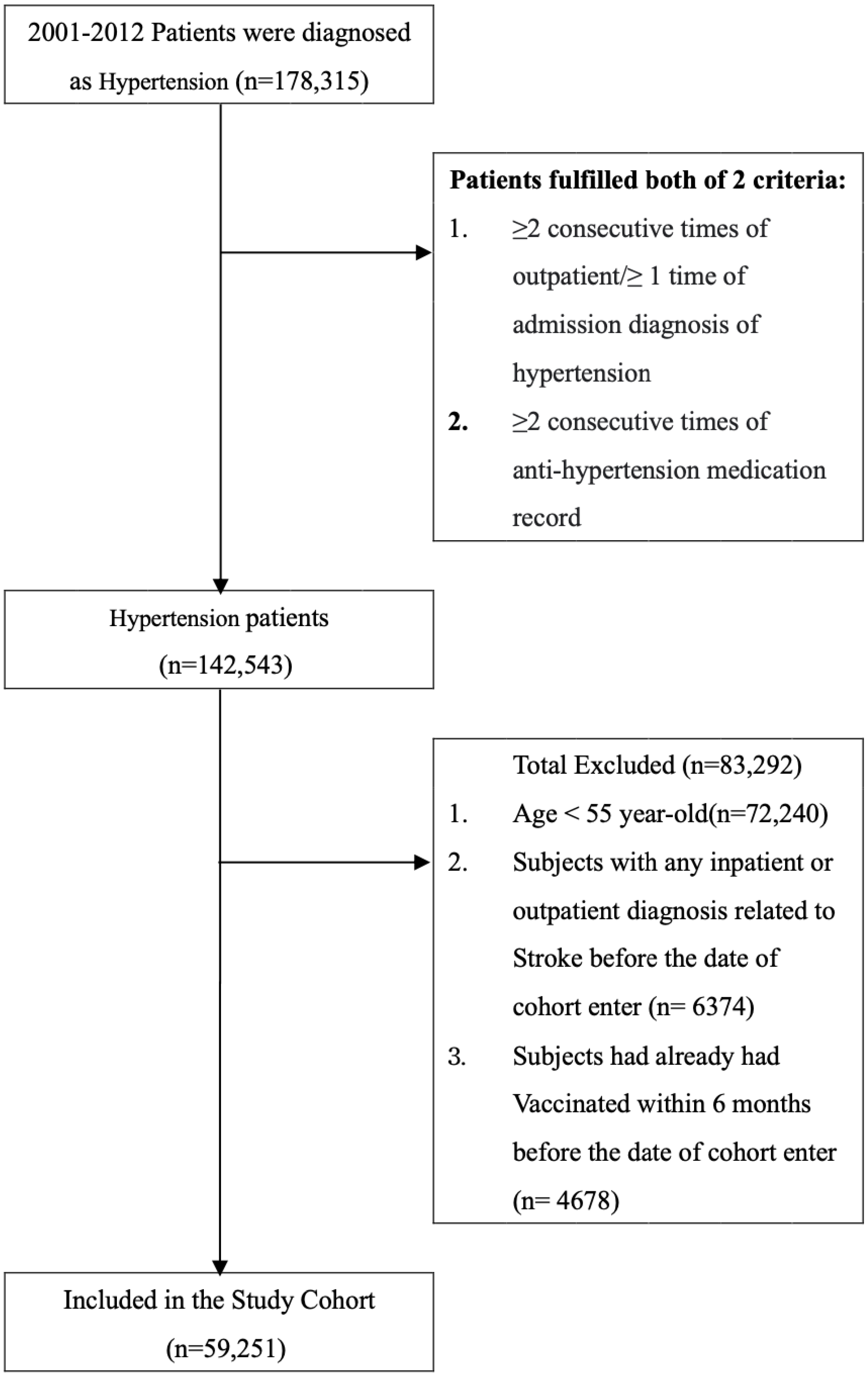
2.1. Study Population and Data Collection
2.2. Potential Confounders
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. The Association between the Risk of Stroke and the Influenza Vaccination for Different Age and Sex
3.3. Sensitivity Analysis of Stroke Risk Reduction after Different Times of Vaccination during Influenza Season, Non-Influenza Season and All Seasons
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardiovascular Diseases (CVDs). World Health Organization Web Site. 2015. Available online: http://www.who.int/mediacentre/factsheets/fs317/en/ (accessed on 10 January 2018).
- Kunst, A.E.; Amiri, M.; Janssen, F. The decline in stroke mortality: Exploration of future trends in 7 Western European countries. Stroke 2011, 42, 2126–2130. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Straus, S.E.; Majumdar, S.R.; McAlister, F.A. New evidence for stroke prevention: Scientific review. JAMA 2002, 288, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Wong, N.D. Epidemiological studies of CHD and the evolution of preventive cardiology. Nat. Rev. Cardiol. 2014, 11, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Hernu, R.; Cour, M.; Casalegno, J.S.; Lina, B.; Argaud, L. Fatal influenza A(H1N1)pdm09 encephalopathy in immunocompetent man. Emerg. Infect. Dis. 2013, 19, 1005–1007. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Chan, P.K.; Lui, G.C.; Wong, B.C.; Sin, W.W.; Choi, K.W.; Wong, R.Y.; Lee, E.L.; Yeung, A.C.; Ngai, K.L.; et al. Complications and outcomes of pandemic 2009 influenza A (H1N1) virus infection in hospitalized adults: How do they differ from those in seasonal influenza? J. Infect. Dis. 2011, 203, 1739–1747. [Google Scholar] [CrossRef] [PubMed]
- Bautista, E.; Chotpitayasunondh, T.; Gao, Z.; Harper, S.A.; Shaw, M.; Uyeki, T.M. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N. Engl. J. Med. 2010, 362, 1708–1719. [Google Scholar] [PubMed] [Green Version]
- Warren-Gash, C.; Smeeth, L.; Hayward, A.C. Influenza as a trigger for acute myocardial infarction or death from cardiovascular disease: A systematic review. Lancet Infect. Dis. 2009, 9, 601–610. [Google Scholar] [CrossRef]
- Bova, I.Y.; Bornstein, N.M.; Korczyn, A.D. Acute infection as a risk factor for ischemic stroke. Stroke 1996, 27, 2204–2206. [Google Scholar] [CrossRef]
- Lavallée, P.; Perchaud, V.; Gautier-Bertrand, M.; Grabli, D.; Amarenco, P. Association between influenza vaccination and reduced risk of brain infarction. Stroke 2002, 33, 513–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siriwardena, A.N.; Gwini, S.M.; Coupland, C.A. Influenza vaccination, pneumococcal vaccination and risk of acute myocardial infarction: Matched case-control study. CMAJ 2010, 182, 1617–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, M.H.; Wu, H.H.; Shih, C.J.; Chen, Y.T.; Kuo, S.C.; Chen, T.L. Association between influenza vaccination and reduced risks of major adverse cardiovascular events in elderly patients. Am. Heart J. 2017, 193, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wolf, P.A.; D’Agostino, R.B.; Belanger, A.J.; Kannel, W.B. Probability of stroke: A risk profile from the Framingham study. Stroke 1991, 22, 312–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannel, W.B.; Dawber, T.R.; Sorlie, P.; Wolf, P.A. Components of blood pressure and risk of atherothrombotic brain infarction: The Framingham study. Stroke 1976, 7, 327–331. [Google Scholar] [CrossRef] [Green Version]
- Domanski, M.J.; Davis, B.R.; Pfeffer, M.A.; Kastantin, M.; Mitchell, G.F. Isolated systolic hypertension: Prognostic information provided by pulse pressure. Hypertension 1999, 34, 375–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.C.; Wang, T.J.; Sung, L.C.; Kao, P.F.; Yang, T.Y.; Hao, W.R.; Chen, C.C.; Hsu, Y.P.; Wu, S.Y. Influenza vaccination reduces hemorrhagic stroke risk in patients with atrial fibrillation: A population-based cohort study. Int. J. Cardiol. 2017, 232, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Cooper, N.J.; Sutton, A.J.; Lu, G.; Khunti, K. Mixed comparison of stroke prevention treatments in individuals with nonrheumatic atrial fibrillation. Arch. Intern. Med. 2006, 166, 1269–1275. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Yarmohammadi, H.; Varr, B.C.; Puwanant, S.; Lieber, E.; Williams, S.J.; Klostermann, T.; Jasper, S.E.; Whitman, C.; Klein, A.L. Role of CHADS2 score in evaluation of thromboembolic risk and mortality in patients with atrial fibrillation undergoing direct current cardioversion (from the ACUTE trial substudy). Am. J. Cardiol. 2012, 110, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.I.; Kuan, C.F.; Fang, Y.A.; Liu, S.H.; Liu, J.C.; Wu, L.-L.; Chang, C.-J.; Yang, H.-C.; Hwang, J.; Miser, J.S.; et al. Cancer risk in HBV patients with statin and metformin use: A population-based cohort study. Med. Baltim. 2015, 94, e462. [Google Scholar] [CrossRef]
- Liu, J.C.; Hsu, Y.P.; Kao, P.F.; Hao, W.R.; Liu, S.H.; Lin, C.F.; Sung, S.C.; Wu, S.Y. Influenza vaccination reduces dementia risk in chronic kidney disease patients: A population-based cohort study. Med. Baltim. 2016, 95, e2868. [Google Scholar] [CrossRef] [PubMed]
- Sung, L.C.; Chen, C.I.; Fang, Y.A.; Lai, C.H.; Hsu, Y.P.; Cheng, T.H.; Miser, J.S.; Liu, J.C. Influenza vaccination reduces hospitalization for acute coronary syndrome in elderly patients with chronic obstructive pulmonary disease: A population-based cohort study. Vaccine 2014, 32, 3843–3849. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deb, S.; Austin, P.C.; Tu, J.V.; Ko, D.T.; Mazer, C.D.; Kiss, A.; Fremes, S.E. A Review of Propensity-Score Methods and Their Use in Cardiovascular Research. Can. J. Cardiol. 2016, 32, 259–265. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Kiri, V.A.; Mackenzie, G. Re: “immortal time bias in pharmacoepidemiology”. Am. J. Epidemiol. 2009, 170, 667–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneeweiss, S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiol. Drug Saf. 2006, 15, 291–303. [Google Scholar]
- Elkind, M.S.V.; Boehme, A.K.; Smith, C.J.; Meisel, A.; Buckwalter, M.S. Infection as a Stroke Risk Factor and Determinant of Outcome after Stroke. Stroke 2020, 51, 3156–3168. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.; Williams, O.A. A decade of racial and ethnic stroke disparities in the United States. Neurology 2014, 82, 1080–1082. [Google Scholar] [CrossRef] [Green Version]
- Corrales-Medina, V.F.; Madjid, M.; Musher, D.M. Role of acute infection in triggering acute coronary syndromes. Lancet Infect. Dis. 2010, 10, 83–92. [Google Scholar] [CrossRef]
- Stokes, K.Y.; Granger, D.N. Platelets: A critical link between inflammation and microvascular dysfunction. J. Physiol. 2012, 590, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Noriega, L.M.; Verdugo, R.J.; Araos, R.; Munita, J.M.; Diaz, V.; Marcotti, A.; Perez, J.; Gonzalez, P.; Thompson, L.; Canals, M.; et al. Pandemic influenza A (H1N1) 2009 with neurological manifestations, a case series. Influenza Other Respir Viruses 2010, 4, 117–120. [Google Scholar] [CrossRef]
- Liu, I.F.; Huang, C.C.; Chan, W.L.; Huang, P.H.; Chung, C.M.; Lin, S.J.; Chen, J.-W.; Leu, H.-B. Effects of annual influenza vaccination on mortality and hospitalization in elderly patients with ischemic heart disease: A nationwide population-based study. Prev. Med. 2012, 54, 431–433. [Google Scholar] [CrossRef]
- Lau, D.; Eurich, D.T.; Majumdar, S.R.; Katz, A.; Johnson, J.A. Effectiveness of influenza vaccination in working-age adults with diabetes: A population-based cohort study. Thorax 2013, 68, 658–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodds, L.; McNeil, S.A.; Fell, D.B.; Allen, V.M.; Coombs, A.; Scott, J.; MacDonald, N. Impact of influenza exposure on rates of hospital admissions and physician visits because of respiratory illness among pregnant women. CMAJ 2007, 176, 463–468. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.B.; Hodgson, A.; Robinson, D.P. Mechanisms of sex disparities in influenza pathogenesis. J. Leukoc. Biol. 2012, 92, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zia, E.; Hedblad, B.; Pessah-Rasmussen, H.; Berglund, G.; Janzon, L.; Engstrom, G. Blood pressure in relation to the incidence of cerebral infarction and intracerebral hemorrhage. Hypertensive hemorrhage: Debated nomenclature is still relevant. Stroke 2007, 38, 2681–2685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karapanayiotides, T.; Piechowski-Jozwiak, B.; van Melle, G.; Bogousslavsky, J.; Devuyst, G. Stroke patterns, etiology, and prognosis in patients with diabetes mellitus. Neurology 2004, 62, 1558–1562. [Google Scholar] [CrossRef] [PubMed]
- Elgebaly, M.M.; Prakash, R.; Li, W.; Ogbi, S.; Johnson, M.H.; Mezzetti, E.M.; Fagan, S.C.; Ergul, A. Vascular protection in diabetic stroke: Role of matrix metalloprotease-dependent vascular remodeling. J. Cereb. Blood Flow Metab. 2010, 30, 1928–1938. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.C.; Tung, H.J.; Hsu, S.W.; Chen, L.S.; Kung, P.T.; Huang, K.H.; Chiou, S.J.; Tsai, W.C. Use of seasonal influenza vaccination and its associated factors among elderly people with disabilities in Taiwan: A population-based study. PLoS ONE 2016, 11, e0158075. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.C.; Chou, Y.L.; Lee, P.L.; Yang, Y.C.; Chen, K.T. Influenza vaccination coverage and factors affecting adherence to influenza vaccination among patients with diabetes in Taiwan. Hum. Vaccines Immunother. 2014, 10, 1028–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, S.F.; Hsieh, C.Y.; Lin, H.J.; Chen, Y.W.; Yang, Y.H.K.; Li, C.Y. Validation of algorithms to identify stroke risk factors in patients with acute ischemic stroke, transient ischemic attack, or intracerebral hemorrhage in an administrative claims database. Int. J. Cardiol. 2016, 215, 277–282. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Whole Cohort (n = 59,521) | Unvaccinated (n = 33,985) | Vaccinated (n = 25,266) | p | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age, years (Mean ± SD) | 66.24 (8.24) | 64.08 (8.19) | 69.14 (7.37) | <0.001 | |||
| 55–64 | 30,531 | 51.53 | 22,205 | 65.34 | 8326 | 32.95 | <0.001 |
| 65–74 | 19,122 | 32.27 | 7661 | 22.54 | 11,461 | 45.36 | |
| ≥75 | 9598 | 16.20 | 4119 | 12.12 | 5479 | 21.69 | |
| Gender | |||||||
| Female | 30,106 | 50.81 | 16,819 | 49.49 | 13,287 | 52.59 | <0.001 |
| Male | 29,145 | 49.19 | 17,166 | 50.51 | 11,979 | 47.41 | |
| CCI | |||||||
| 0 | 24,501 | 41.35 | 14,208 | 41.81 | 10,293 | 40.74 | 0.003 |
| 1 | 15,333 | 25.88 | 8699 | 25.60 | 6634 | 26.26 | |
| 2 | 9613 | 16.22 | 5394 | 15.87 | 4219 | 16.70 | |
| ≥3 | 9804 | 16.55 | 5684 | 16.73 | 4120 | 16.31 | |
| Comorbidities | |||||||
| Diabetes | 13,422 | 22.65 | 7725 | 22.73 | 5697 | 22.55 | 0.600 |
| Dyslipidemia | 15,062 | 25.42 | 9087 | 26.74 | 5975 | 23.65 | <0.001 |
| Atrial fibrillation | 3726 | 6.29 | 1636 | 4.81 | 2090 | 8.27 | <0.001 |
| Anti-hypertension medications | |||||||
| Antihypertenives | 12,255 | 20.68 | 5343 | 15.72 | 6912 | 27.36 | <0.001 |
| Diuretics | 33,998 | 57.38 | 17,076 | 50.25 | 16,922 | 66.98 | <0.001 |
| Beta blocking agents | 31,978 | 53.97 | 16,696 | 49.13 | 15,282 | 60.48 | <0.001 |
| Calcium channel blockers | 44,966 | 75.89 | 24,277 | 71.43 | 20,689 | 81.88 | <0.001 |
| RAA | 40,146 | 67.76 | 21,659 | 63.73 | 18,487 | 73.17 | <0.001 |
| Co-medications | |||||||
| Statin drugs | |||||||
| <28 days | 38,564 | 65.09 | 22,849 | 67.23 | 15,715 | 62.20 | <0.001 |
| 28–365 days | 10,204 | 17.22 | 5829 | 17.15 | 4375 | 17.32 | |
| >365 days | 10,483 | 17.69 | 5307 | 15.62 | 5176 | 20.49 | |
| Metformin drug | |||||||
| <28 days | 45,017 | 75.98 | 26,178 | 77.03 | 18,839 | 74.56 | <0.001 |
| 28–365 days | 4335 | 7.32 | 2677 | 7.88 | 1658 | 6.56 | |
| >365 days | 9899 | 16.71 | 5130 | 15.09 | 4769 | 18.88 | |
| Aspirin drug | |||||||
| <28 days | 34,022 | 57.42 | 21,900 | 64.44 | 12,122 | 47.98 | <0.001 |
| 28–365 days | 12,351 | 20.85 | 6419 | 18.89 | 5932 | 23.48 | |
| >365 days | 12,878 | 21.73 | 5666 | 16.67 | 7212 | 28.54 | |
| Level of Urbanization | |||||||
| Urban | 41,015 | 69.22 | 25,268 | 74.35 | 15,747 | 62.32 | <0.001 |
| Suburban | 12,129 | 20.47 | 6158 | 18.12 | 5971 | 23.63 | |
| Rural | 6107 | 10.31 | 2559 | 7.53 | 3548 | 14.04 | |
| Monthly income (NT$) | |||||||
| 0 | 5709 | 9.64 | 2818 | 8.29 | 2891 | 11.44 | <0.001 |
| 1–20,100 | 19,825 | 33.46 | 10,282 | 30.25 | 9543 | 37.77 | |
| 20,100–30,300 | 19,665 | 33.19 | 10,363 | 30.49 | 9302 | 36.82 | |
| ≥30,301 | 14,052 | 23.72 | 10,522 | 30.96 | 3530 | 13.97 | |
| All Group (n = 59,521) | Unvaccinated (Total Follow-Up 177,838.0 Person Years) | Vaccinated (Total Follow-Up 201,118.5 Person Years) | Adjusted HR † (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No. of Patients with Stroke | Incidence Rate (per 105 Person Years) (95% CI) | No. of Patients with Stroke | Incidence Rate (per 105 Person Years) (95% CI) | ||||||
| Whole cohort | |||||||||
| Influenza season | 2579 | 1450.2 | (1394.2, | 1506.2) | 2809 | 1396.7 | (1345.0, | 1448.3) | 0.60 (0.56, 0.63) *** |
| Non-influenza season | 1779 | 1000.3 | (953.9, | 1046.8) | 1649 | 819.9 | (780.3, | 859.5) | 0.56 (0.52, 0.60) *** |
| All seasons | 4358 | 2450.5 | (2377.8, | 2523.3) | 4458 | 2216.6 | (2151.5, | 2281.7) | 0.58 (0.56, 0.61) *** |
| Age, 55–64 a | |||||||||
| Influenza season | 1374 | 1127.7 | (1068.1, | 1187.4) | 668 | 895.6 | (827.7, | 963.6) | 0.53 (0.48, 0.58) *** |
| Non-influenza season | 886 | 727.2 | (679.3, | 775.1) | 298 | 399.5 | (354.2, | 444.9) | 0.44 (0.38, 0.50) *** |
| All seasons | 2260 | 1854.9 | (1778.5, | 1931.4) | 966 | 1295.2 | (1213.5, | 1376.9) | 0.49 (0.46, 0.53) *** |
| Age, ≥65 b | |||||||||
| Influenza season | 1205 | 2151.8 | (2030.3, | 2273.3) | 2141 | 1692.0 | (1620.4, | 1763.7) | 0.61 (0.57, 0.66) *** |
| Non-influenza season | 893 | 1594.6 | (1490.0, | 1699.2) | 1351 | 1067.7 | (1010.8, | 1124.6) | 0.58 (0.53, 0.63) *** |
| All seasons | 2098 | 3746.4 | (3586.1, | 3906.7) | 3492 | 2759.7 | (2668.2, | 2851.3) | 0.60 (0.57, 0.63) *** |
| Female c | |||||||||
| Influenza season | 1104 | 1195.8 | (1125.3, | 1266.4) | 1321 | 1218.6 | (1152.9, | 1284.4) | 0.63 (0.58, 0.68) *** |
| Non-influenza season | 807 | 874.1 | (813.8, | 934.4) | 797 | 735.2 | (684.2, | 786.3) | 0.58 (0.52, 0.64) *** |
| All seasons | 1911 | 2069.9 | (1977.1, | 2162.7) | 2118 | 1953.9 | (1870.7, | 2037.1) | 0.61 (0.57, 0.65) *** |
| Male d | |||||||||
| Influenza season | 1475 | 1724.8 | (1636.8, | 1812.8) | 1488 | 1604.9 | (1523.3, | 1686.4) | 0.57 (0.53, 0.62) *** |
| Non-influenza season | 972 | 1136.6 | (1065.2, | 1208.1) | 852 | 918.9 | (857.2, | 980.6) | 0.53 (0.48, 0.59) *** |
| All seasons | 2447 | 2861.5 | (2748.1, | 2974.8) | 2340 | 2523.8 | (2421.5, | 2626.0) | 0.56 (0.52, 0.59) *** |
| Unvaccinated | Vaccinated | p for Trend | |||
|---|---|---|---|---|---|
| 1 | 2–3 | ≥4 | |||
| Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | ||
| Main model † | 1.00 | 0.85 (0.78, 0.92) *** | 0.69 (0.64, 0.75) *** | 0.41 (0.38, 0.45) *** | <0.001 |
| Subgroup effects | |||||
| Age, years | |||||
| 55–64 | 1.00 | 0.67 (0.59, 0.77) *** | 0.53 (0.46, 0.60) *** | 0.41 (0.35, 0.48) *** | <0.001 |
| ≥65 | 1.00 | 0.95 (0.86, 1.05) | 0.77 (0.70, 0.84) *** | 0.41 (0.37, 0.45) *** | <0.001 |
| Sex | |||||
| Female | 1.00 | 0.86 (0.76, 0.97) * | 0.73 (0.66, 0.82) *** | 0.45 (0.41, 0.51) *** | <0.001 |
| Male | 1.00 | 0.84 (0.76, 0.94) ** | 0.66 (0.60, 0.73) *** | 0.38 (0.34, 0.42) *** | <0.001 |
| Diabetes | |||||
| No | 1.00 | 0.86 (0.79, 0.94) ** | 0.72 (0.66, 0.78) *** | 0.43 (0.39, 0.47) *** | <0.001 |
| Yes | 1.00 | 0.81 (0.69, 0.95) ** | 0.63 (0.54, 0.74) *** | 0.37 (0.32, 0.44) *** | <0.001 |
| Dyslipidemia | |||||
| No | 1.00 | 0.87 (0.80, 0.95) ** | 0.70 (0.65, 0.76) *** | 0.42 (0.38, 0.45) *** | <0.001 |
| Yes | 1.00 | 0.74 (0.62, 0.89) ** | 0.66 (0.56, 0.77) *** | 0.40 (0.34, 0.48) *** | <0.001 |
| AF | |||||
| No | 1.00 | 0.85 (0.78, 0.93) *** | 0.69 (0.64, 0.75) *** | 0.41 (0.38, 0.44) *** | <0.001 |
| Yes | 1.00 | 0.79 (0.63, 1.00) | 0.68 (0.54, 0.84) *** | 0.44 (0.36, 0.54) *** | <0.001 |
| Antihypertensive | |||||
| No (<28 days) | 1.00 | 0.82 (0.74, 0.90) *** | 0.66 (0.60, 0.72) *** | 0.38 (0.34, 0.42) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.98 (0.84, 1.14) | 0.82 (0.71, 0.95) ** | 0.51 (0.45, 0.59) *** | <0.001 |
| Diuretics | |||||
| No (<28 days) | 1.00 | 0.89 (0.78, 1.02) | 0.65 (0.56, 0.74) *** | 0.35 (0.30, 0.41) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.84 (0.76, 0.92) *** | 0.72 (0.66, 0.79) *** | 0.44 (0.40, 0.48) *** | <0.001 |
| Beta blocking agents | |||||
| No (<28 days) | 1.00 | 0.84 (0.74, 0.94) ** | 0.64 (0.56, 0.72) *** | 0.37 (0.33, 0.43) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.85 (0.77, 0.95) ** | 0.73 (0.67, 0.81) *** | 0.44 (0.40, 0.48) *** | <0.001 |
| Calcium channel blockers | |||||
| No (<28 days) | 1.00 | 0.81 (0.67, 0.97) * | 0.66 (0.55, 0.80) *** | 0.36 (0.29, 0.44) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.86 (0.79, 0.94) ** | 0.70 (0.65, 0.76) *** | 0.43 (0.39, 0.46) *** | <0.001 |
| RAA | |||||
| No (<28 days) | 1.00 | 0.98 (0.84, 1.14) | 0.72 (0.62, 0.84) *** | 0.39 (0.33, 0.47) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.81 (0.74, 0.89) *** | 0.69 (0.63, 0.75) *** | 0.42 (0.39, 0.46) *** | <0.001 |
| Statin drugs | |||||
| <28 days | 1.00 | 0.89 (0.80, 0.98) * | 0.72 (0.66, 0.80) *** | 0.42 (0.38, 0.46) *** | <0.001 |
| 28–365 days | 1.00 | 0.76 (0.64, 0.90) ** | 0.63 (0.53, 0.75) *** | 0.39 (0.32, 0.46) *** | <0.001 |
| >365 days | 1.00 | 0.82 (0.69, 0.99) * | 0.67 (0.57, 0.79) *** | 0.45 (0.38, 0.53) *** | <0.001 |
| Metformin drug | |||||
| <28 days | 1.00 | 0.85 (0.77, 0.93) *** | 0.71 (0.65, 0.77) *** | 0.41 (0.37, 0.45) *** | <0.001 |
| 28–365 days | 1.00 | 0.88 (0.68, 1.16) | 0.68 (0.52, 0.88) ** | 0.42 (0.32, 0.57) *** | <0.001 |
| >365 days | 1.00 | 0.85 (0.71, 1.01) | 0.68 (0.57, 0.81) *** | 0.45 (0.38, 0.53) *** | <0.001 |
| Aspirin drug | |||||
| <28 days | 1.00 | 0.85 (0.73, 0.98) * | 0.76 (0.66, 0.88) *** | 0.40 (0.34, 0.47) *** | <0.001 |
| 28–365 days | 1.00 | 0.88 (0.77, 1.01) | 0.64 (0.56, 0.73) *** | 0.37 (0.32, 0.43) *** | <0.001 |
| >365 days | 1.00 | 0.84 (0.74, 0.96) ** | 0.70 (0.62, 0.79) *** | 0.45 (0.41, 0.51) *** | <0.001 |
| Unvaccinated | Vaccinated | p for Trend | |||
|---|---|---|---|---|---|
| 1 | 2–3 | ≥4 | |||
| Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | ||
| Main model † | 1.00 | 0.83 (0.75, 0.91) *** | 0.63 (0.57, 0.69) *** | 0.35 (0.32, 0.39) *** | <0.001 |
| Subgroup effects | |||||
| Age, years | |||||
| 55–64 | 1.00 | 0.58 (0.48, 0.70) *** | 0.48 (0.39, 0.58) *** | 0.27 (0.20, 0.34) *** | <0.001 |
| ≥65 | 1.00 | 0.94 (0.83, 1.05) | 0.67 (0.60, 0.75) *** | 0.35 (0.31, 0.39) *** | <0.001 |
| Sex | |||||
| Female | 1.00 | 0.87 (0.76, 1.00) | 0.65 (0.57, 0.75) *** | 0.36 (0.31, 0.42) *** | <0.001 |
| Male | 1.00 | 0.79 (0.69, 0.90) *** | 0.60 (0.53, 0.69) *** | 0.34 (0.29, 0.39) *** | <0.001 |
| Diabetes | |||||
| No | 1.00 | 0.80 (0.72, 0.90) *** | 0.59 (0.53, 0.66) *** | 0.34 (0.30, 0.38) *** | <0.001 |
| Yes | 1.00 | 0.89 (0.74, 1.08) | 0.72 (0.60, 0.86) *** | 0.39 (0.32, 0.47) *** | <0.001 |
| Dyslipidemia | |||||
| No | 1.00 | 0.82 (0.74, 0.92) *** | 0.62 (0.56, 0.69) *** | 0.36 (0.32, 0.40) *** | <0.001 |
| Yes | 1.00 | 0.83 (0.67, 1.03) | 0.63 (0.51, 0.78) *** | 0.33 (0.26, 0.41) *** | <0.001 |
| AF | |||||
| No | 1.00 | 0.82 (0.74, 0.91) *** | 0.62 (0.56, 0.69) *** | 0.35 (0.31, 0.39) *** | <0.001 |
| Yes | 1.00 | 0.85 (0.64, 1.13) | 0.63 (0.48, 0.83) ** | 0.38 (0.29, 0.50) *** | <0.001 |
| Antihypertensive | |||||
| No (<28 days) | 1.00 | 0.88 (0.79, 0.99) * | 0.65 (0.58, 0.72) *** | 0.33 (0.29, 0.38) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.69 (0.57, 0.85) *** | 0.59 (0.49, 0.70) *** | 0.38 (0.32, 0.45) *** | <0.001 |
| Diuretics | |||||
| No (<28 days) | 1.00 | 0.87 (0.74, 1.02) | 0.63 (0.53, 0.74) *** | 0.33 (0.27, 0.40) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.81 (0.72, 0.91) *** | 0.62 (0.55, 0.70) *** | 0.35 (0.31, 0.40) *** | <0.001 |
| Beta blocking agents | |||||
| No (<28 days) | 1.00 | 0.78 (0.67, 0.91) ** | 0.65 (0.56, 0.75) *** | 0.31 (0.26, 0.37) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.85 (0.75, 0.96) * | 0.61 (0.54, 0.69) *** | 0.37 (0.33, 0.42) *** | <0.001 |
| Calcium channel blockers | |||||
| No (<28 days) | 1.00 | 0.87 (0.70, 1.08) | 0.56 (0.44, 0.71) *** | 0.33 (0.25, 0.43) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.81 (0.73, 0.91) *** | 0.64 (0.57, 0.71) *** | 0.35 (0.32, 0.39) *** | <0.001 |
| RAA | |||||
| No (<28 days) | 1.00 | 0.70 (0.58, 0.85) *** | 0.52 (0.43, 0.63) *** | 0.25 (0.20, 0.32) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.88 (0.79, 0.99) * | 0.67 (0.60, 0.75) *** | 0.39 (0.34, 0.43) *** | <0.001 |
| Statin drugs | |||||
| <28 days | 1.00 | 0.83 (0.73, 0.93) ** | 0.64(0.57, 0.72) *** | 0.33 (0.29, 0.37) *** | <0.001 |
| 28–365 days | 1.00 | 0.72 (0.58, 0.89) ** | 0.55(0.44, 0.68) *** | 0.37 (0.30, 0.46) *** | <0.001 |
| >365 days | 1.00 | 0.95 (0.73, 1.24) | 0.66(0.51, 0.86) ** | 0.44 (0.35, 0.57) *** | <0.001 |
| Metformin drug | |||||
| <28 days | 1.00 | 0.83 (0.74, 0.93) ** | 0.62 (0.55, 0.69) *** | 0.34 (0.30, 0.38) *** | <0.001 |
| 28–365 days | 1.00 | 0.72 (0.53, 0.99) * | 0.51 (0.37, 0.70) *** | 0.31 (0.22, 0.44) *** | <0.001 |
| >365 days | 1.00 | 0.88 (0.70, 1.10) | 0.72 (0.58, 0.90) ** | 0.42 (0.34, 0.53) *** | <0.001 |
| Aspirin drug | |||||
| <28 days | 1.00 | 0.87 (0.74, 1.02) | 0.59 (0.49, 0.70) *** | 0.27 (0.22, 0.34) *** | <0.001 |
| 28–365 days | 1.00 | 0.76 (0.64, 0.89) *** | 0.54 (0.46, 0.64) *** | 0.36 (0.30, 0.42) *** | <0.001 |
| >365 days | 1.00 | 0.90 (0.76, 1.08) | 0.78 (0.66, 0.92) ** | 0.41 (0.35, 0.49) *** | <0.001 |
| Unvaccinated | Vaccinated | p for Trend | |||
|---|---|---|---|---|---|
| 1 | 2–3 | ≥4 | |||
| Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | Adjusted HR (95% CI) | ||
| Main model † | 1.00 | 0.84 (0.79, 0.89) *** | 0.67 (0.63, 0.71) *** | 0.39 (0.37, 0.41) *** | <0.001 |
| Subgroup effects | |||||
| Age, years | |||||
| 55–64 | 1.00 | 0.64 (0.57, 0.71) *** | 0.51 (0.45, 0.57) *** | 0.36 (0.31, 0.41) *** | <0.001 |
| ≥65 | 1.00 | 0.94 (0.87, 1.02) | 0.72 (0.67, 0.78) *** | 0.39 (0.36, 0.41) *** | <0.001 |
| Sex | |||||
| Female | 1.00 | 0.87 (0.79, 0.95) ** | 0.70 (0.64, 0.76) *** | 0.42 (0.38, 0.45) *** | <0.001 |
| Male | 1.00 | 0.82 (0.76, 0.89) *** | 0.64 (0.59, 0.69) *** | 0.36 (0.33, 0.40) *** | <0.001 |
| Diabetes | |||||
| No | 1.00 | 0.84 (0.78, 0.90) *** | 0.67 (0.62, 0.71) *** | 0.39 (0.37, 0.42) *** | <0.001 |
| Yes | 1.00 | 0.84 (0.75, 0.95) ** | 0.67 (0.59, 0.75) *** | 0.38 (0.33, 0.43) *** | <0.001 |
| Dyslipidemia | |||||
| No | 1.00 | 0.85 (0.80, 0.91) *** | 0.67 (0.63, 0.72) *** | 0.39 (0.37, 0.42) *** | <0.001 |
| Yes | 1.00 | 0.78 (0.68, 0.89) *** | 0.65 (0.57, 0.74) *** | 0.37 (0.33, 0.43) *** | <0.001 |
| AF | |||||
| No | 1.00 | 0.84 (0.79, 0.90) *** | 0.67 (0.63, 0.71) *** | 0.38 (0.36, 0.41) *** | <0.001 |
| Yes | 1.00 | 0.82 (0.68, 0.98) * | 0.66 (0.55, 0.78) *** | 0.42 (0.35, 0.49) *** | <0.001 |
| Antihypertensive | |||||
| No (<28 days) | 1.00 | 0.84 (0.78, 0.90) *** | 0.65 (0.61, 0.70) *** | 0.36 (0.34, 0.39) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.86 (0.76, 0.97) * | 0.72 (0.65, 0.81) *** | 0.46 (0.41, 0.51) *** | <0.001 |
| Diuretics | |||||
| No (<28 days) | 1.00 | 0.88 (0.80, 0.98) * | 0.64 (0.57, 0.71) *** | 0.34 (0.31, 0.39) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.83 (0.76, 0.89) *** | 0.68 (0.64, 0.73) *** | 0.40 (0.38, 0.43) *** | <0.001 |
| Beta blocking agents | |||||
| No (<28 days) | 1.00 | 0.81 (0.74, 0.90) *** | 0.64 (0.58, 0.71) *** | 0.35 (0.32, 0.39) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.85 (0.79, 0.92) *** | 0.68 (0.63, 0.74) *** | 0.41 (0.38, 0.44) *** | <0.001 |
| Calcium channel blockers | |||||
| No (<28 days) | 1.00 | 0.83 (0.73, 0.96) * | 0.62 (0.54, 0.72) *** | 0.34 (0.29, 0.41) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.84 (0.79, 0.90) *** | 0.68 (0.63, 0.72) *** | 0.40 (0.37, 0.42) *** | <0.001 |
| RAA | |||||
| No (<28 days) | 1.00 | 0.85 (0.76, 0.96) ** | 0.63 (0.56, 0.71) *** | 0.33 (0.29, 0.38) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.84 (0.78, 0.90) *** | 0.68 (0.64, 0.73) *** | 0.41 (0.38, 0.44) *** | <0.001 |
| Statin drugs | |||||
| <28 days | 1.00 | 0.86 (0.80, 0.93) *** | 0.69 (0.64, 0.74) *** | 0.38 (0.35, 0.41) *** | <0.001 |
| 28–365 days | 1.00 | 0.74 (0.65, 0.85) *** | 0.60 (0.52, 0.68) *** | 0.38 (0.33, 0.44) *** | <0.001 |
| >365 days | 1.00 | 0.86 (0.74, 1.00) * | 0.67 (0.58, 0.77) *** | 0.45 (0.39, 0.51) *** | <0.001 |
| Metformin drug | |||||
| <28 days | 1.00 | 0.84 (0.78, 0.90) *** | 0.67 (0.63, 0.72) *** | 0.38 (0.35, 0.41) *** | <0.001 |
| 28–365 days | 1.00 | 0.81 (0.66, 0.99) * | 0.60 (0.49, 0.73) *** | 0.37 (0.30, 0.46) *** | <0.001 |
| >365 days | 1.00 | 0.86 (0.75, 0.99) * | 0.70 (0.61, 0.80) *** | 0.44 (0.39, 0.51) *** | <0.001 |
| Aspirin drug | |||||
| <28 days | 1.00 | 0.86 (0.77, 0.96) ** | 0.69 (0.61, 0.77) *** | 0.35 (0.31, 0.40) *** | <0.001 |
| 28–365 days | 1.00 | 0.83 (0.74, 0.92) *** | 0.60 (0.54, 0.66) *** | 0.36 (0.33, 0.41) *** | <0.001 |
| >365 days | 1.00 | 0.86 (0.78, 0.96) ** | 0.73 (0.66, 0.80) *** | 0.44 (0.40, 0.48) *** | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Chiu, C.-C.; Yang, T.-Y.; Fang, Y.-A.; Lei, M.-H.; Yeh, H.-T.; Chen, C.-C.; Hao, W.-R.; Kuo, C.-H.; Liu, J.-C. The Association between Influenza Vaccination and Stroke Risk in Patients with Hypertension: A Nationwide Population-Based Study. Appl. Sci. 2022, 12, 4074. https://0-doi-org.brum.beds.ac.uk/10.3390/app12084074
Lin C-H, Chiu C-C, Yang T-Y, Fang Y-A, Lei M-H, Yeh H-T, Chen C-C, Hao W-R, Kuo C-H, Liu J-C. The Association between Influenza Vaccination and Stroke Risk in Patients with Hypertension: A Nationwide Population-Based Study. Applied Sciences. 2022; 12(8):4074. https://0-doi-org.brum.beds.ac.uk/10.3390/app12084074
Chicago/Turabian StyleLin, Cheng-Hsin, Chun-Chih Chiu, Tsung-Yeh Yang, Yu-Ann Fang, Meng-Huan Lei, Hsien-Tang Yeh, Chun-Chao Chen, Wen-Rui Hao, Chung-Hsien Kuo, and Ju-Chi Liu. 2022. "The Association between Influenza Vaccination and Stroke Risk in Patients with Hypertension: A Nationwide Population-Based Study" Applied Sciences 12, no. 8: 4074. https://0-doi-org.brum.beds.ac.uk/10.3390/app12084074