1. Introduction
Neutrophil gelatinase-associated lipocalin (NGAL) is a ubiquitous protein, composed of a single polypeptide chain with a molecular weight of 25 kDa [
1]. It was firstly distinguished in the granules of human granulocytes, but it is likewise expressed in low levels also in cardiomyocytes, lymphocytes, and renal tubular cells [
2,
3].
It is associated with the lipocalin superfamily, a group of proteins implicated in the organism’s defense against pathogens. Precisely, NGAL induces the activation of the innate immunity in the course of bacterial infection, furthermore, it modulates several eukaryotic cellular reactions and proliferation and differentiation processes [
2].
In the kidney, NGAL is synthesized in the distal nephron and released into the urine from the ascending limb of the loop of Henle to the collecting ducts [
4]. NGAL is a small sized molecule, is openly filtered, and is simply detected in blood, urine, and peritoneal effluent. Different studies have demonstrated its efficacy in the diagnosis of acute kidney disease (AKI) [
5]. Currently, urine NGAL concentration is a valid and effective tool to detect renal tubular injury [
6].
During bacterial infection, the pathogen and host compete for iron. In this context, NGAL binds bacterial siderophores blocking iron shuttling, thereby limiting bacterial growth [
2]. These inflammatory features underline why NGAL levels have been found in the presence of infection, inflammatory statements, and kidney insult.
Peritonitis (inflammation of the peritoneum membrane) is a frequent complication for peritoneal dialysis (PD) patients, and it is associated with catheter loss, shift to hemodialysis, temporary loss of ultrafiltration, potential membrane damage, and occasionally death. Despite progress in treatment and prevention, PD-associated peritonitis is still the main cause of morbidity and mortality in this population [
7,
8]. In this context, several studies have reported significant increases in NGAL during peritonitis [
7,
8]. In particular, our group demonstrated that peritoneal NGAL is poorly present in the peritoneal effluent of PD patients in a basal statement [
8]. On the contrary, human peritoneal mesothelial cells can release NGAL during an inflammatory state [
9].
Current clinical criteria for the diagnosis of peritonitis include clinical signs and symptoms, cloudy effluent, and positive culture [
10]. However, these features may not always be suggestive in the timely identification of peritonitis. For this reason, various biomarkers have been tested for the early diagnosis of peritonitis. Therefore, as expected, peritoneal NGAL has been revealed to be a novel biomarker for the diagnosis of peritoneal dialysis (PD) associated peritonitis [
11].
In particular, in a previous study, we confirmed that peritoneal NGAL is a great marker for the diagnosis of peritonitis, particularly combining with WBC in PDE (the gold standard for the diagnosis of peritonitis).
In our PD Unit, for these reasons, peritoneal NGAL is employed as a biomarker of peritonitis, in combination with the traditional criteria based on the International Society of Peritoneal Dialysis (ISPD) guidelines [
8,
9,
10,
11]. In Vicenza center, the quantitative evaluation of peritoneal NGAL is detected by a particle-enhanced turbidimetric immunoassay (BioPorto test) performed by the Clinical Chemistry and Hematology Laboratory at San Bortolo Hospital. Recently, a point-of-care test (POCT) for the rapid evaluation of NGAL based on semi-quantitative colorimetric test strips was introduced in our PD Unit. The POCT is currently accessible in the PD center at the bedside of the patient, and it is performed by qualified nurses, giving quick results.
The focus of this report is to compare the NGAL POCT with the laboratory-based NGAL test currently accessible in our medical routine and with other laboratory biomarkers of peritonitis, such as the dialysis effluent white cell count. A secondary aim of this study is the assessment of the NGAL POCT as an analytic instrument to aid physicians with the recognition of peritonitis.
2. Materials and Methods
2.1. Study Design
This is an observational, case control study carried out in our PD center at San Bortolo Hospital (Vicenza-Italy) between 1 January 2020 and 31 December 2020. The case group consisted of all eligible patients who came to the Vicenza center with signs and symptoms suggestive of peritonitis in the period study. The inclusion criteria were an age over 18 years, PD treatment for at least 30 days, and informed consent. We excluded patients with relapsing and recurrent peritonitis. The control group consisted of a similar number of patients who were scheduled for routine visits at our PD center during the same period. The inclusion criteria for the control group were age over 18 years, PD treatment for at least 30 days, and informed consent. The exclusion criteria were the presence of a current peritonitis episode or the presence of previous peritonitis or any history of systemic inflammation 30 days before enrollment. All patients were provided written informed consent, and the study was conducted in accordance with the principles of the Helsinki Declaration and Good Clinical Practices.
Based on the ISPD criteria, peritonitis is defined as a cloudy peritoneal dialysate effluent (PDE) with a white cell count > 100 × 10
6/L (after a dwell time of at least 2 h), of which more than 50% were polymorphonuclear cells, typically with abdominal pain and/or a positive effluent culture [
10]. All patients underwent blood and PDE analysis according to our clinical practice on the first day of peritonitis for the case group and during routine checkout visits for the control group. Medical features, laboratory parameters, and dialysis-related data were collected for all subjects at the time of enrollment. Blood urea nitrogen, serum creatinine (sCr), C-reactive protein (CRP), and other biochemistry parameters were detected by the usual laboratory techniques performed by an automatic analyzer (Dimension Vista, Siemens Healthcare, Tarrytown, NY.) White blood cells (WBC) and hemoglobin (Hb) were evaluated by the automated hematology analyzers XN 9000 (SYSMEX, KOBE, Japan). Weekly Kt/Vurea and Creatinine Clearance (wCCr) were applied as estimates of PD adequacy. Weekly Kt/Vurea and wCCr were estimated based on the 24 h drain volumes carried out before the planned visit to the PD center [
12]. The white cell count in PDE was assessed by the collection of PD effluent in all patients by the automated hematology analyzers XN 9000 (SYSMEX, KOBE, Japan). PDE culture and gram staining were performed in the case group.
2.2. NGAL Measurements
The peritoneal NGAL was measured in all PD patients with both techniques described below. Peritoneal laboratory-based NGAL was measured by the conventional BioPorto test (BioPorto Diagnostics, 2900 Hellerup, DK), using a particle-enhanced turbidimetric immunoassay for the quantitative determination. The assay range is between 50 and 3000 ng/mL. Values ≥ 200 ng/mL are indicative of peritonitis [
13].
In addition, peritoneal NGAL was tested by the novel POCT (NGAL dipstick- NGALds, BioPorto Diagnostics, 2900 Hellerup, DK). NGALds is a rapid assay for the semi-quantitative evaluation of NGAL levels in biological fluids by colorimetric strips (NGALds, BioPorto Diagnostics, 2900 Hellerup, DK). This test is an antibody sandwich lateral flow dipstick test. Color-categorized NGAL levels were 25 ng/mL–50 ng/mL–100 ng/mL–150 ng/mL–300 ng/mL–600 ng/mL and were reported in the user guide. For the reproducibility of the data, NGALds were determined by two distinct trained lab operators on all PD patients in a blinded manner.
2.3. Endpoints
As the primary endpoint, we compared the NGALds results with the laboratory-based NGAL results used in our medical routine. In addition, we evaluated the time needed to perform the two different methods. The secondary endpoint was verifying the relationship and the concordance between the already used markers of peritonitis, such as peritoneal laboratory-based NGAL and white cell count in PDE, and NGALds and standard inflammation markers, such as CRP. Finally, we compared the performance of peritoneal NGALds in patients with peritonitis and the different range of peritoneal NGALds in patients with and without peritonitis. For these points, we split patients with peritonitis into two groups based on the value of white cell count in PDE and quantitative peritoneal NGAL. We considered values of white cell count in PDE ≥100 × 106/L as an indicative cut-off point of peritonitis. We considered the peritoneal laboratory-based NGAL values ≥ 200 ng/mL as an indicative cut-off point of peritonitis.
2.4. Statistical Analysis
For the statistical analysis, the SPSS 16.0 (SPSS Inc., Chicago, IL, USA) software package was used. Categorical variables were reported as percentages; continuous variables were reported as means ± standard deviation (parametric variables) or median and interquartile range (IQR) (nonparametric variables). The Mann–Whitney U test or t-test were employed for comparison of two groups, as appropriate. Categorical variables were compared using the X2 test. Correlation coefficients were evaluated with the Spearman’s rank or Pearson’s test, as appropriate. Correlations between the two observers were calculated by Spearman’s correlation coefficient, and the agreement between the two observers was calculated by the kappa test and Bland–Altman method. A p-value of <0.05 was considered statistically significant.
3. Results
3.1. Subjects Baseline Characteristics
Finally, this scientific report investigated 30 PD patients. Seven of them were treated with continuous ambulatory PD (CAPD) and twenty-three with automated PD (APD). The average length of the PD treatment was 32.7 (IQR 11–49) months and the range was a minimum of 1 to a maximum of 88 months. In total, 9/30 PD patients had diabetes, all 30 patients had hypertension, and 12/30 had cardiovascular disease (CVD). None of the patients were treated with immunosuppressive drugs, and 86.6% of them were treated with erythropoietin.
The case group is composed of 17 patients with peritonitis. The control group is composed of 13 PD patients without peritonitis and a history of systemic inflammation in the last 3 months (as previously defined).
The medical-, laboratory- and dialysis-related parameters of all 30 patients with and without peritonitis are reported in
Table 1. The two groups were statistically similar for baseline characteristics.
In the case group, five patients were admitted to the hospital for the peritonitis and two patients required catheter removal and switching to hemodialysis. No subject died during the peritonitis treatment. The microbiological reasons for the peritonitis are recapitulated in
Table 2.
3.2. Laboratory Parameters Evaluation
We evaluated the white cell count in PDE (287.5 × 106/L, IQR 81.5–2860.5 × 106/L), quantitative peritoneal NGAL (171 ng/mL, IQR 96.2–286.7 ng/mL) and peritoneal NGALds (300 ng/mL, IQR 150–300 ng/mL) in our PD population.
We noticed a positive linear correlation between NGALds and laboratory-based NGAL values in the peritoneal dialysis effluent (Spearman’s rho = 0.88, p < 0.01). Furthermore, we observed a positive correlation between peritoneal NGALds and white cell count in PDE (Spearman’s rho = 0.82, p < 0.01). In addition, we reported a positive linear correlation between peritoneal NGALds values and CRP (Spearman’s rho = 0.54, p = 0.02).
Table 3 describes the different inflammatory profiles in the case and control groups. In particular, all standard inflammatory parameters, such as CRP, WBC count in blood, white cell count in PDE, and peritoneal laboratory-based NGAL were different in the two groups (
p = 0.01,
p = 0.03,
p = 0.01, and <0.01, respectively). Similarly, in PDE, the NGALds levels resulted in being elevated in PD patients with peritonitis (300 ng/mL, IQR 300–600) compared with patients without peritonitis (100 ng/mL, IQR 50–150) (
p < 0.01). In particular, in the peritonitis group, all subjects were characterized by peritoneal NGALds values ≥ 300 ng/mL. On the contrary, in the control group, two patients had peritoneal NGALds values equal to 300 ng/mL; no one had peritoneal NGALds values equal to 600 ng/mL (
Table 4).
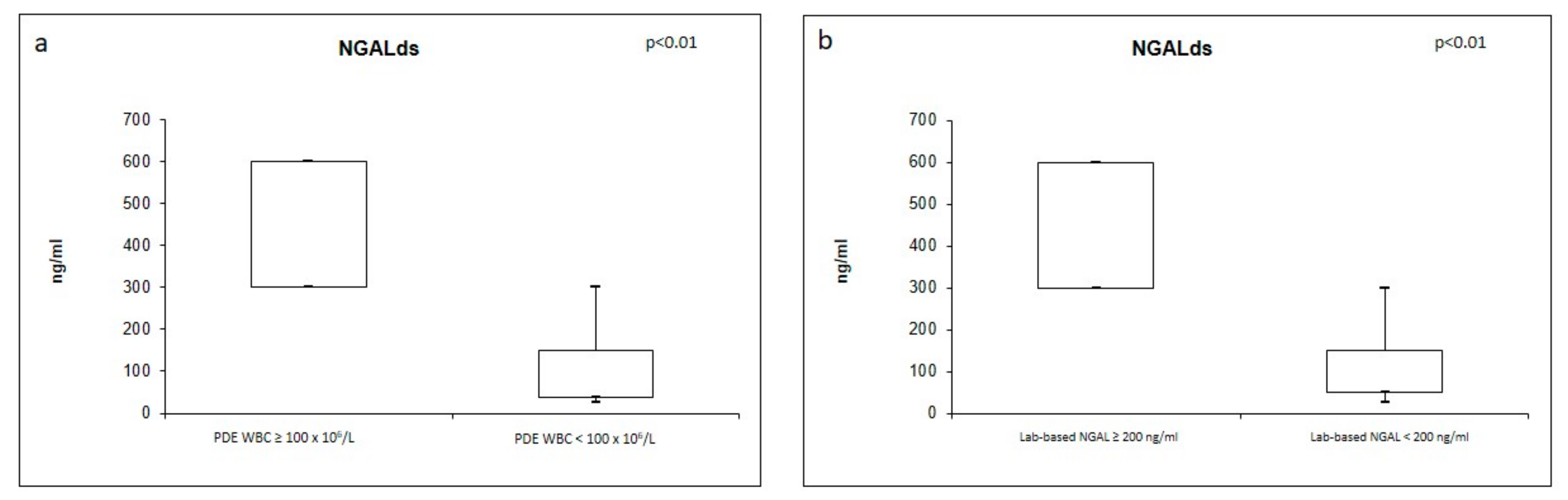
Furthermore, we split patients into two groups based on the value of white cell count in PDE. The values of peritoneal NGALds resulted in being significantly higher in PD patients (n = 17) with a peritoneal white cell count ≥ 100 × 10
6/L (300 ng/mL, IQR 300–600 versus 100 ng/mL, IQR 37.5–150) (
Figure 1a). All patients with peritoneal white cell count ≥ 100 × 10
6/L had peritoneal NGALds ≥ 300 ng/mL. Only one patient with peritoneal white cell count < 100 × 10
6/L had peritoneal NGALds equal to 300 ng/mL.
In addition, we split patients into two categories based on the value of the quantitative peritoneal NGAL. The values of the peritoneal NGALds resulted in being significantly higher in PD patients with peritoneal laboratory-based NGAL ≥ 200 ng/mL (n = 17) (300 ng/mL, IQR 300–600 versus 100 ng/mL, IQR 50–150) (
Figure 2). All patients with peritoneal laboratory-based NGAL ≥ 200 ng/mL had peritoneal NGALds ≥ 300 ng/mL. Only two patients with peritoneal laboratory-based NGAL < 200 ng/mL had peritoneal NGALds values equal to 300 ng/mL.
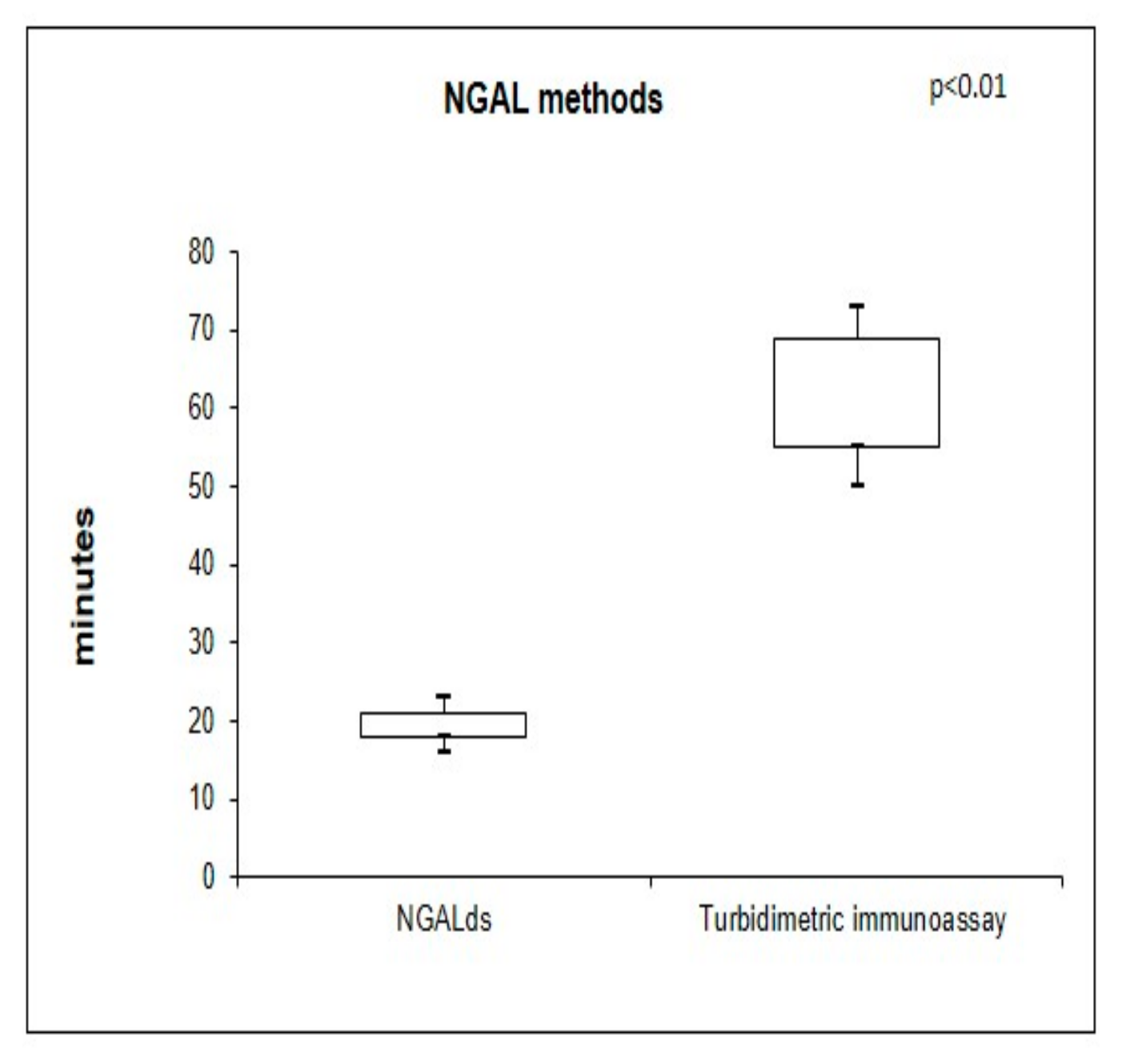
The peritoneal NGALds assay was carried out over a median time of 20 min (IQR 18–21) in comparison to the turbidimetric immunoassay performed in the median time of 65 min (IQR 55–69) (
p < 0.01) (
Figure 1).
Two different lab operators measured NGALds in a blinded mode. The reproducibility for the interoperator variability for NGALds in PDE was 0.847 (p < 0.001), and the agreement was elevated (k = 0.786, p < 0.001).
4. Discussion
In this investigation, we analyzed NGALds as a rapid NGAL assay in PDE using semi-quantitative colorimetric-category test strips. In particular, we theorized that the results of this new method could be similar to the results of the quantitative peritoneal laboratory-based NGAL test and could be coherent to the present biomarkers used to evaluate peritonitis and inflammation. In particular, we speculated that NGALds may be useful in the determination of peritonitis. In fact, it was proved that the early identification and prompt management of peritonitis is fundamental to limiting the structural and functional changes and avoiding peritoneal membrane malfunction in peritoneal dialysis patients [
14].
At the state of the art, clinical criteria for the identification of peritonitis consist of clinical signs and symptoms, cloudy effluent, and positive culture [
10]. Nevertheless, these features may not always be notable in the timely recognition of peritonitis. For this reason, numerous biomarkers have been investigated in the setting of early diagnosis of peritonitis such as adipokine [
15], matrix-metalloproteinase-9 [
16], and various cytokines [
17]. Unfortunately, none of them seems to have applicability in clinical practice.
Instead, the NGAL value in plasma and peritoneal effluent has been gaining increasing attention in the last decades and the quantitative peritoneal laboratory-based NGAL test has already been proved to be a helpful instrument for the timely and precise diagnosis of peritonitis [
7,
9].
Recently, NGALds has been developed as a POCT assay for NGAL rapid evaluation and several studies have demonstrated that it performs uniformly to the quantitative-continuous assay in urine biological fluids. These studies were all performed on patients with AKI [
18,
19,
20].
In our study, we evaluated NGALds using the peritoneal effluent as a biological sample from PD patients with and without peritonitis. In accordance with the aforementioned data reported in urine samples, the current results have confirmed that, also in peritoneal effluent, the results of the peritoneal NGALds are coherent with the laboratory-based NGAL values.
Furthermore, our results highlighted a good positive correlation between the peritoneal NGALds and laboratory parameters involved in peritonitis. In particular, we observed a robust positive correlation between peritoneal NGALds and the white cell count in PDE, the main laboratory parameter for the peritonitis diagnosis suggested by the ISPD guidelines. Furthermore, the peritoneal NGALds levels resulted in being significantly elevated in PD patients with peritonitis. These results corroborate that NGAL is implicated in the human immune response and that it is promptly measurable in PDE at the beginning of peritonitis, even if detected with a semi-quantitative color-categorized assay.
The peritoneal NGAL quantitative values fit well with the peritoneal NGALds categories. This observation confirmed that both methods can be mixed with the white cell count in PDE, as an extra tool for the diagnosis of peritonitis [
8].
In addition, we observed that all the PD patients with the diagnosis of peritonitis had peritoneal NGALds values ≥ 300 ng/dL. Similarly, all the PD patients with white cell count ≥ 100 × 106/L and with peritoneal laboratory-based NGAL ≥ 200 ng/dL had peritoneal NGALds values ≥ 300 ng/dL. Consequently, we suggest that the indicative cut-off point of NGALds for peritonitis could be the value of 300 ng/mL.
The NGALds assay is completed within a median time of 20 min, while the laboratory-based NGAL test requires a median time of 65 min. We spent significantly less time using NGALds compared to the laboratory-based test. We observed that two trained laboratory technicians in a blinded manner independently executed the NGALds test with a strong agreement between these operators. This finding confirms the high reproducibility and the user friendliness of NGALds. We supported the evidence demonstrated by Bjornstad et al. that NGALds is carried out easily and in a low-resource condition [
19]. Moreover, Lei et al. suggested that NGALds can be performed at the patient’s bedside by qualified staff (i.e., nurses), offering real-time data. In addition, several studies have demonstrated that the novel test could be a useful tool for the clinical staff at the point of care [
18,
19].
We recognize the limitations of this preliminary study: the small sample size and the single-center study design. In this preliminary study, we described the comparison between two different experimental test values in 30 PD patients. Further analysis and a bigger cohort are necessary to evaluate the sensitivities and specificities of NGALds (these points are not the focus of this report). We think that these results are the basis for multicenter, larger, and more specific studies that may prove the efficacy, helpfulness, and applicability of NGALds in stable subjects treated by PD and in patients with PD-related peritonitis. So, our preliminary results are hypothesis-generating data that can promote additional larger studies. In particular, future studies must improve the sample size, and a bigger population of patients must be included.
5. Conclusions
In conclusion, in PDE, NGALds values were coherent with the quantitative NGAL performed by the central laboratory and with the biomarkers implicated in the diagnosis of peritonitis (specifically WBC in PDE). Finally, it was an accessible method with real-time results. NGALds could be an extra novel biomarker of peritonitis, helpful at the patient’s bedside or when/if the laboratory-based NGAL test is not available.
In the future, we can speculate that this point-of-care test could be integrated into a remote monitoring program, improving medical outcomes in PD patients, thereby lowering emergency visits and hospitalizations [
20].
The NGALds might be an accurate triage tool at the bedside of the patient, shortening the length of diagnosis and distance between the patient at home and the clinical staff in the hospital.


 ,
, 


{kind=link}
{kind=link}