
Robust Automatic Segmentation of Inflamed Appendix from Ultrasonography with Double-Layered Outlier Rejection Fuzzy C-Means Clustering


Abstract
:1. Introduction
- We propose Double-layered Outlier Rejection Fuzzy C-Means (DORFCM) as the quantization algorithm that mitigates the outlier sensitivity of FCM.
2. Appendix Segmentation with Double-Layered Outlier Rejection FCM
2.1. Outlier Rejection
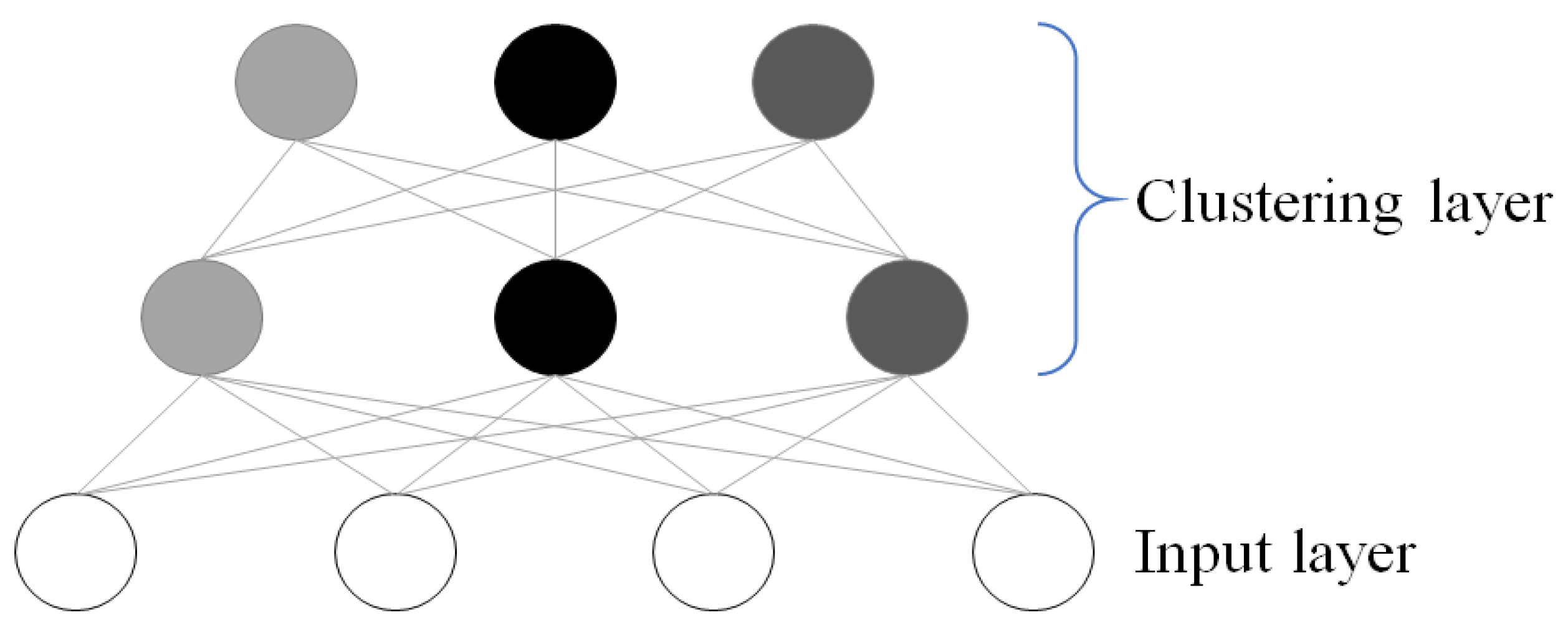
2.2. Double-Layered Pixel Clustering
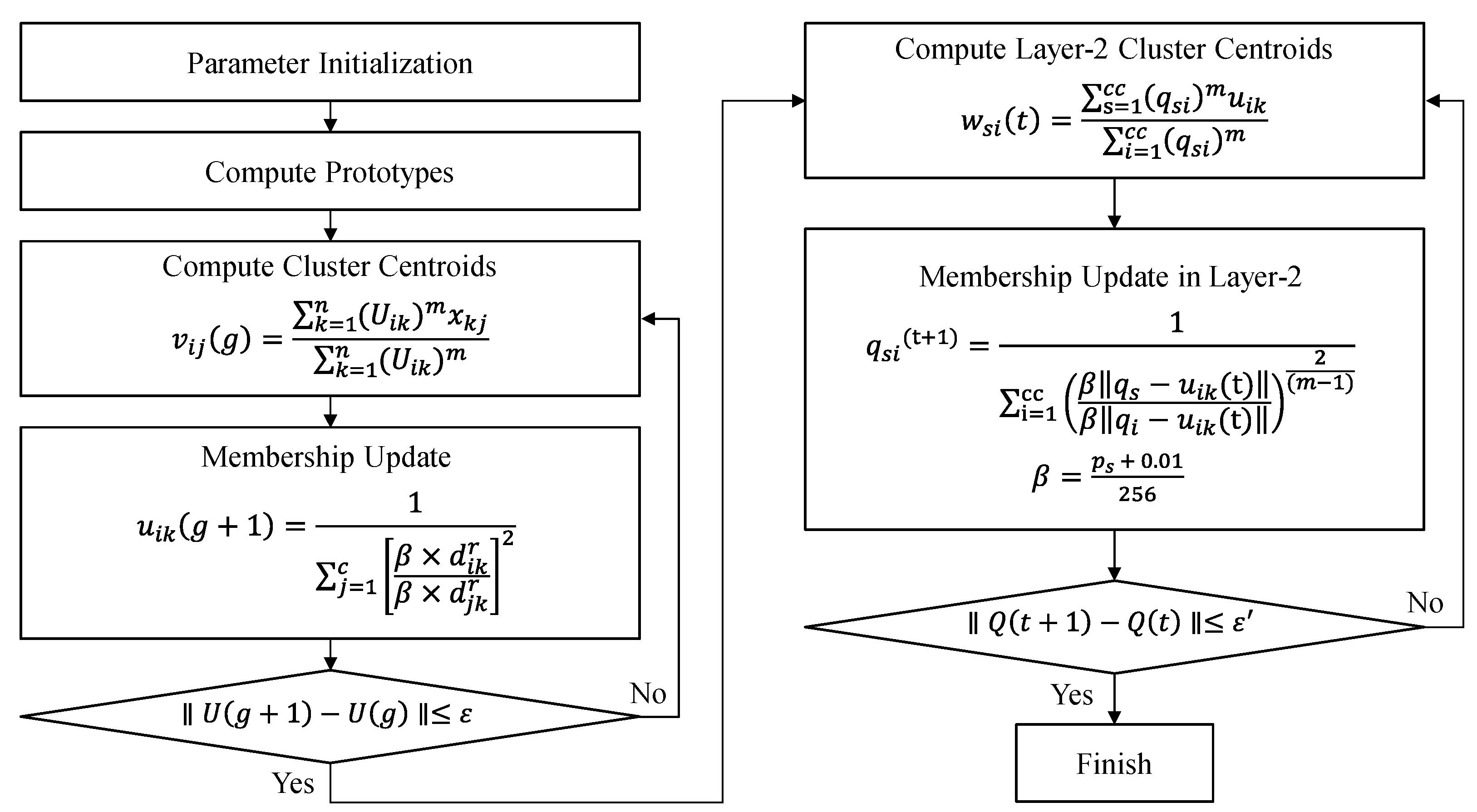
2.3. Double-Layered Outlier Rejection FCM (DORFCM)
2.3.1. Layer-1 Learning (Step 1 to Step 4)
2.3.2. Layer-2 Learning (Step 5 to Step 7)
| Algorithm 1. The proposed method algorithm |
| Procedure DORFCM (x) returns prototypes and partition matrix Input data x = {, , …, } Local fuzzification parameter: m threshold: , norm: INITALIZE-PARTITION-MATRIX g , t repeat for i = 1:c do compute prototypes for i = 1:c do for k = 1:n do update partition matrix g g + 1 until repeat for s = 1:cc do Layer compute prototypes for s = 1:cc do for i = 1:c do update Layer-2 partition matrix where is the intensity in a cluster of layer-2. t t + 1 until return w, q |
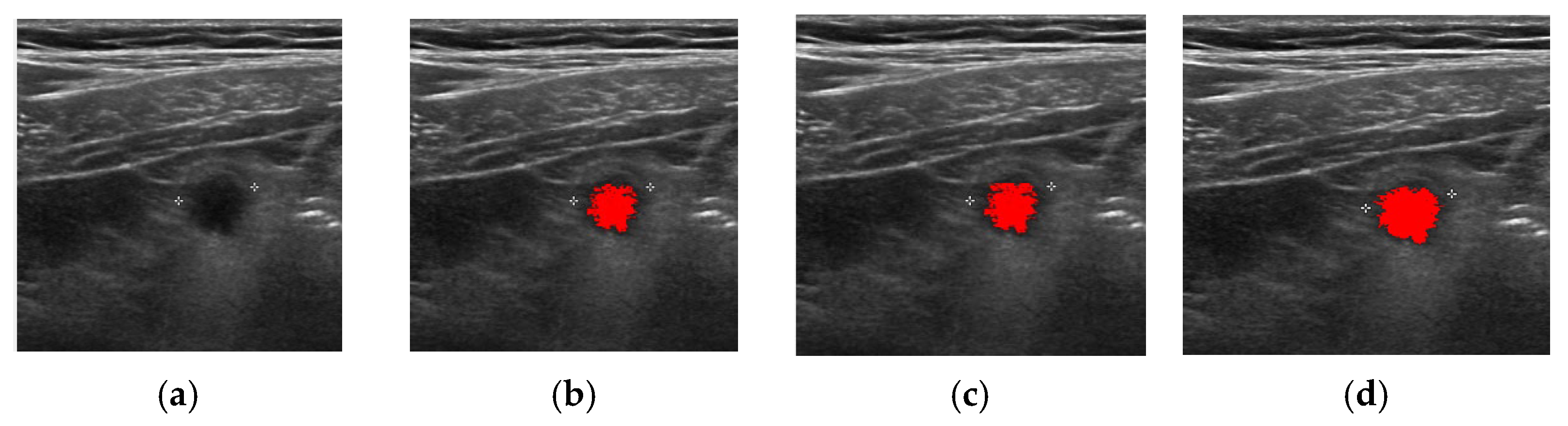
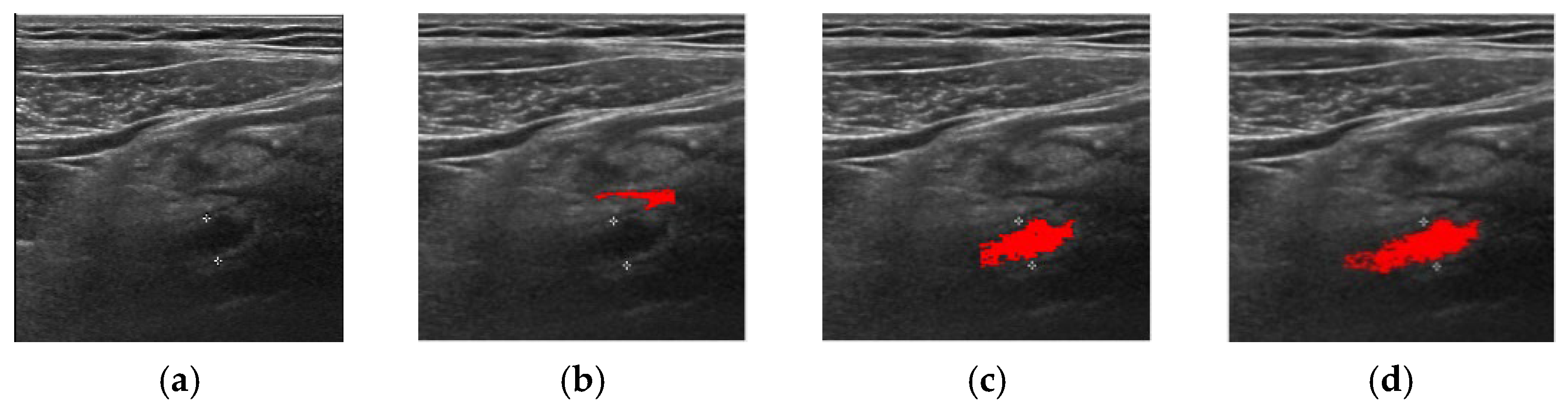
3. Experiment and Analysis
- Precision = TP/(TP + FP)
- Recall or Sensitivity = TP/(TP + FN)
- Accuracy = (TP + TN)/all area
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stewart, B.; Khanduri, P.; McCord, C.; Ohene-Yeboah, M.; Uranues, S.; Vega Rivera, F.; Mock, C. Global disease burden of conditions requiring emergency surgery. J. Br. Surg. 2014, 101, e9–e22. [Google Scholar] [CrossRef]
- Longo, D.L.; Fauci, A.S.; Kasper, D.L.; Hauser, S.L.; Jameson, J.; Loscalzo, J. Harrison's Principles of Internal Medicine, 18th ed.; McGraw-Hill: New York, NY, USA, 2012; pp. 2516–2519. [Google Scholar]
- Dissanayake, S.; Hohnen, A.; Lo, G.; Herron, J. Beyond appendicitis: Clinical and radiological manifestations of appendiceal neoplasms. Eur. Congr. Radiol. ECR 2018, 28, 2018. [Google Scholar]
- Alari, F.S.; Gutierrez, I.; Pérez, J.G. Case Report: Familial history aggregation on acute appendicitis. BMJ Case Rep. 2017, 1–4. [Google Scholar] [CrossRef]
- Doherty, G.M. CURRENT Diagnosis and Treatment: Surgery, 13th ed.; McGraw-Hill: New York, NY, USA, 2010; pp. 615–620. [Google Scholar]
- Israel, G.M.; Malguria, N.; McCarthy, S.; Copel, J.; Weinreb, J. MRI vs. ultrasound for suspected appendicitis during pregnancy. J. Magn. Reson. Imaging 2008, 28, 428–433. [Google Scholar] [CrossRef]
- Di Saverio, S.; Birindelli, A.; Kelly, M.D.; Catena, F.; Weber, D.G.; Sartelli, M.; Sugrue, M.; Moya, M.D.; Gomes, C.A.; Bhangu, A.; et al. WSES Jerusalem guidelines for diagnosis and treatment of acute appendicitis. World J. Emerg. Surg. 2016, 11, 34. [Google Scholar] [CrossRef]
- Gaitini, D. Imaging acute appendicitis: State of the art. J. Clin. Imaging Sci. 2011, 1, 49. [Google Scholar] [CrossRef]
- Jang, K.M.; Lee, K.; Kim, M.J.; Yoon, H.S.; Jeon, E.Y.; Koh, S.H.; Choi, D. What is the complementary role of ultrasound evaluation in the diagnosis of acute appendicitis after CT. Eur. J. Radiol. 2010, 74, 71–76. [Google Scholar] [CrossRef]
- Tomizawa, M.; Shinozaki, F.; Hasegawa, R.; Shirai, Y.; Motoyoshi, Y.; Sugiyama, T.; Yamamoto, S.; Ishige, N. Abdominal ultrasonography for patients with abdominal pain as a first-line diagnostic imaging modality. Exp. Ther. Med. 2017, 13, 1932–1936. [Google Scholar] [CrossRef] [Green Version]
- Reddan, T. Statistical Modelling of Paediatric Appendix Ultrasonography and the Predictive Value of Secondary Sonographic Signs. Ph.D. Thesis, Queensland University of Technology, Brisbane, Australia, 2019. [Google Scholar]
- Estey, A.; Poonai, N.; Lim, R. Appendix not seen: The predictive value of secondary inflammatory sonographic signs. Pediatr. Emerg. Care 2013, 29, 435–439. [Google Scholar] [CrossRef]
- Ruseckaitė, V.; Dūdėnas, V. Ultrasonography Guidelines for Imaging Acute Appendicitis; Medicinos mokslai. Med. Sci. 2018, 6, 7. [Google Scholar]
- Zacharzewska-Gondek, A.; Szczurowska, A.; Guziński, M.; Sąsiadek, M.; Bladowska, J. How to ultrasound an appendicitis? In Proceedings of the European Congress of Radiology, Vienna, Austria, 27 February–3 March 2019.
- Wider, M.; Myint, Y.; Supriyanto, E. Comparison of histogram thresholding methods for ultrasound appendix image extraction. NAUN Int. J. Comput. 2011, 5, 542–549. [Google Scholar]
- Lam, J.; Pahl, C.; Abduljabbar, H.N.; Supriyanto, E. Measurement and analysis of the diameter of appendix based on ultrasound images. Int. J. Biosci. Biochem. Bioinform. 2014, 4, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Tashfeen, S.H.; Abrar, A.; Tondra, T.T. Inflamed Appendix Detection from Laparoscopic Video Footage Using Edge Detection and Morphological Image Processing. Ph.D. Thesis, BRAC University, Dhaka, Bangladesh, 2017. [Google Scholar]
- Kim, K.B.; Song, D.H.; Lee, W.J. Flaw detection in ceramics using sigma fuzzy binarization and gaussian filtering method. Int. J. Multimed. Ubiquitous Eng. 2014, 9, 403–414. [Google Scholar] [CrossRef]
- Lee, H.J.; Song, D.H.; Kim, K.B. Effective computer-assisted automatic cervical vertebrae extraction with rehabilitative ultrasound imaging by using K-means clustering. Int. J. Electr. Comput. Eng. 2016, 6, 2810–2817. [Google Scholar]
- Park, J.; Song, D.H.; Nho, H.; Choi, H.M.; Kim, K.A.; Park, H.J.; Kim, K.B. Automatic segmentation of brachial artery based on fuzzy C-means pixel clustering from ultrasound images. Int. J. Electr. Comput. Eng. 2018, 8, 638–643. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.B.; Song, D.H. Intelligent automatic extraction of canine cataract object with dynamic controlled fuzzy C-means based quantization. Int. J. Electr. Comput. Eng. 2018, 8, 666–672. [Google Scholar] [CrossRef]
- Kim, K.B.; Song, D.H.; Cho, J.H.; Kim, C.; Woo, Y.W. Detection and recognition of uterine cervical carcinoma cells in pap-smears using kapur method and morphological features. Inf. Int. Interdiscip. J. 2009, 12, 731–741. [Google Scholar]
- Park, S.I.; Park, H.J.; Kim, K.B. Appendix analysis from ultrasonography with cubic spline interpolation and K-means clustering. Int. J. Bio-Sci. Bio-Technol. 2015, 7, 1–10. [Google Scholar] [CrossRef]
- Kim, K.B.; Park, H.J.; Song, D.H.; Han, S.S. Developing an intelligent automatic appendix extraction method from ultrasonography based on fuzzy ART and image processing. Comput. Math. Methods Med. 2015, 2015, 389057. [Google Scholar] [CrossRef]
- Kim, K.B.; Song, D.H.; Park, H.J. Automatic Extraction of Appendix from Ultrasonography with Self-Organizing Map and Shape-Brightness Pattern Learning. BioMed Res. Int. 2016, 2016, 5206268. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.B.; Park, H.J.; Song, D.H. Semi-dynamic Control of FCM Initialization for Automatic Extraction of Inflamed Appendix from Ultrasonography. Curr. Med. Imaging Rev. 2019, 15, 810. [Google Scholar] [CrossRef]
- Kim, K.B.; Song, Y.S.; Park, H.J.; Song, D.H.; Choi, B.K. A fuzzy C-means quantization based automatic extraction of rotator cuff tendon tears from ultrasound images. J. Intell. Fuzzy Syst. 2018, 35, 149–158. [Google Scholar] [CrossRef]
- Razavi, M.; Wang, L.; Gubern-Mérida, A.; Ivanovska, T.; Laue, H.; Karssemeijer, N.; Hahn, H.K. Towards accurate segmentation of fibroglandular tissue in breast MRI using fuzzy c-means and skin-folds removal. In Proceedings of the International Conference on Image Analysis and Processing, Genova, Italy, 7–11 September 2015; pp. 528–536. [Google Scholar]
- Hassan, M.; Chaudhry, A.; Khan, A.; Iftikhar, M.A. Robust information gain based fuzzy c-means clustering and classification of carotid artery ultrasound images. Comput. Methods Programs Biomed. 2014, 113, 593–609. [Google Scholar] [CrossRef]
- Hong, J.S.; Kaneko, T.; Sekiguchi, R.; Park, K.H. Automatic liver tumor detection from CT. IEICE Trans. Inf. Syst. 2001, 84, 741–748. [Google Scholar]
- Ceylan, R.; Ceylan, M.; Özbay, Y.; Kara, S. Fuzzy clustering complex-valued neural network to diagnose cirrhosis disease. Expert Syst. Appl. 2011, 38, 9744–9751. [Google Scholar] [CrossRef]
- Li, K.; Zhang, C.; Chen, Z.; Chen, Y. Development of a weighted fuzzy c-means clustering algorithm based on JADE. Int. J. Numer. Anal. Model. 2014, 5, 113–122. [Google Scholar]
- Fu, H.; Elmisery, A.M. A new feature weighted fuzzy c-means clustering algorithm. In Proceedings of the Multi Conference on Computer Science and Information Systems (MCCSIS 2009), Algarve, Portugal, 17–23 June 2009; pp. 11–18. Available online: http://www.iadisportal.org/digital-library/a-new-feature-weighted-fuzzy-c-means-clustering-algorithm (accessed on 1 March 2022).
- Wu, K.L.; Yang, M.S. Alternative c-means clustering algorithms. Pattern Recognit. 2002, 35, 2267–2278. [Google Scholar] [CrossRef]
- Siddiqui, F.U.; Isa, N.A.M.; Yahya, A. Outlier rejection fuzzy c-means (ORFCM) algorithm for image segmentation. Turk. J. Electr. Eng. Comput. Sci. 2013, 21, 1801–1819. [Google Scholar] [CrossRef]
- Kim, K.B.; Kim, G.H.; Song, D.H.; Park, H.J.; Kim, C.W. Automatic segmentation of liver/kidney area with double-layered fuzzy C-means and the utility of hepatorenal index for fatty liver severity classification. J. Intell. Fuzzy Syst. 2020, 39, 925–936. [Google Scholar] [CrossRef]
- Bezdek, J.C. Pattern Recognition with Fuzzy Objective Function Algorithms; Plenum Press: New York, NY, USA, 1981. [Google Scholar]
- Abderrezak, M.Z.; Chibane, M.B.; Mansour, K. A new segmentation method of cerebral MRI images based on the fuzzy c-means algorithm. Turk. J. Electr. Eng. Comput. Sci. 2017, 25, 3215–3226. [Google Scholar] [CrossRef]
- Mekhmoukh, A.; Mokrani, K. MR brain image segmentation using an improved kernel fuzzy local information c-means based wavelet, particle swarm optimization (PSO) initialization and outlier rejection with level set methods. Int. Arab. J. Inf. Technol 2018, 15, 683–692. [Google Scholar]
- Chowdhary, C.L.; Mittal, M.; Pattanaik, P.A.; Marszalek, Z. An efficient segmentation and classification system in medical images using intuitionist possibilistic fuzzy C-mean clustering and fuzzy SVM algorithm. Sensors 2020, 20, 3903. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Successful Images/Total Images |
|---|---|
| FCM | 83/100 |
| ORFCM | 88/100 |
| DFCM | 91/100 |
| DORFCM | 98/100 |
| Accuracy | Precision | Recall | |
|---|---|---|---|
| DORFCM | 84.20% | 83.40% | 85.80% |
| DFCM | 80.80% | 80.90% | 80.20% |
| Accuracy | Precision | Recall | |
|---|---|---|---|
| DORFCM | 84.82% | 83.78% | 86.04% |
| ORFCM | 81.23% | 78.56% | 80.53% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.B.; Song, D.H.; Park, H.J. Robust Automatic Segmentation of Inflamed Appendix from Ultrasonography with Double-Layered Outlier Rejection Fuzzy C-Means Clustering. Appl. Sci. 2022, 12, 5753. https://0-doi-org.brum.beds.ac.uk/10.3390/app12115753
Kim KB, Song DH, Park HJ. Robust Automatic Segmentation of Inflamed Appendix from Ultrasonography with Double-Layered Outlier Rejection Fuzzy C-Means Clustering. Applied Sciences. 2022; 12(11):5753. https://0-doi-org.brum.beds.ac.uk/10.3390/app12115753
Chicago/Turabian StyleKim, Kwang Baek, Doo Heon Song, and Hyun Jun Park. 2022. "Robust Automatic Segmentation of Inflamed Appendix from Ultrasonography with Double-Layered Outlier Rejection Fuzzy C-Means Clustering" Applied Sciences 12, no. 11: 5753. https://0-doi-org.brum.beds.ac.uk/10.3390/app12115753