Regional Inhaled Deposited Dose of Urban Aerosols in an Eastern Mediterranean City

 , , , and
, , , and
Abstract
:1. Introduction
2. Methodology
2.1. Regional Inhaled Deposited Dose Rate
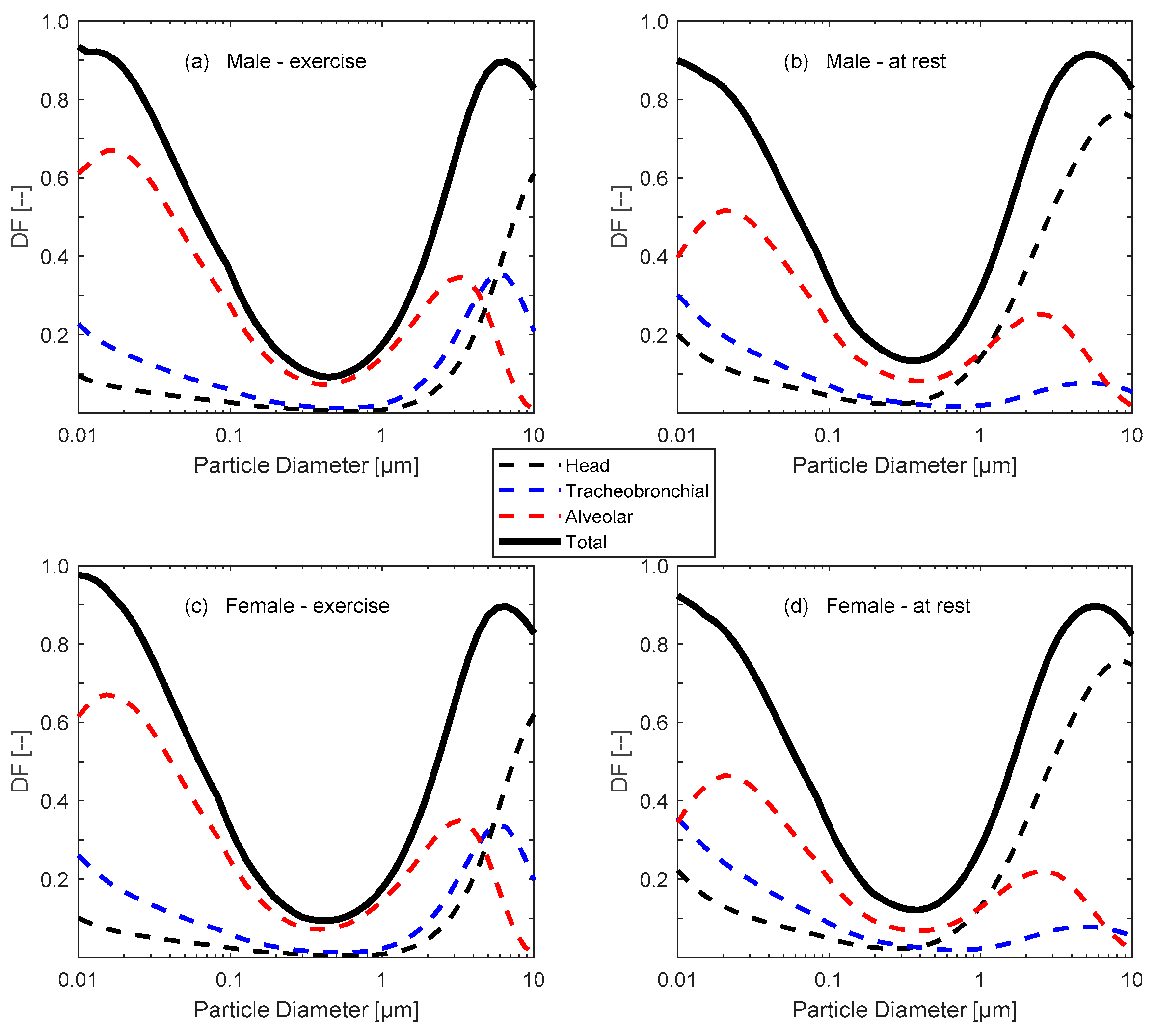
2.2. Respiratory Tract Parameters
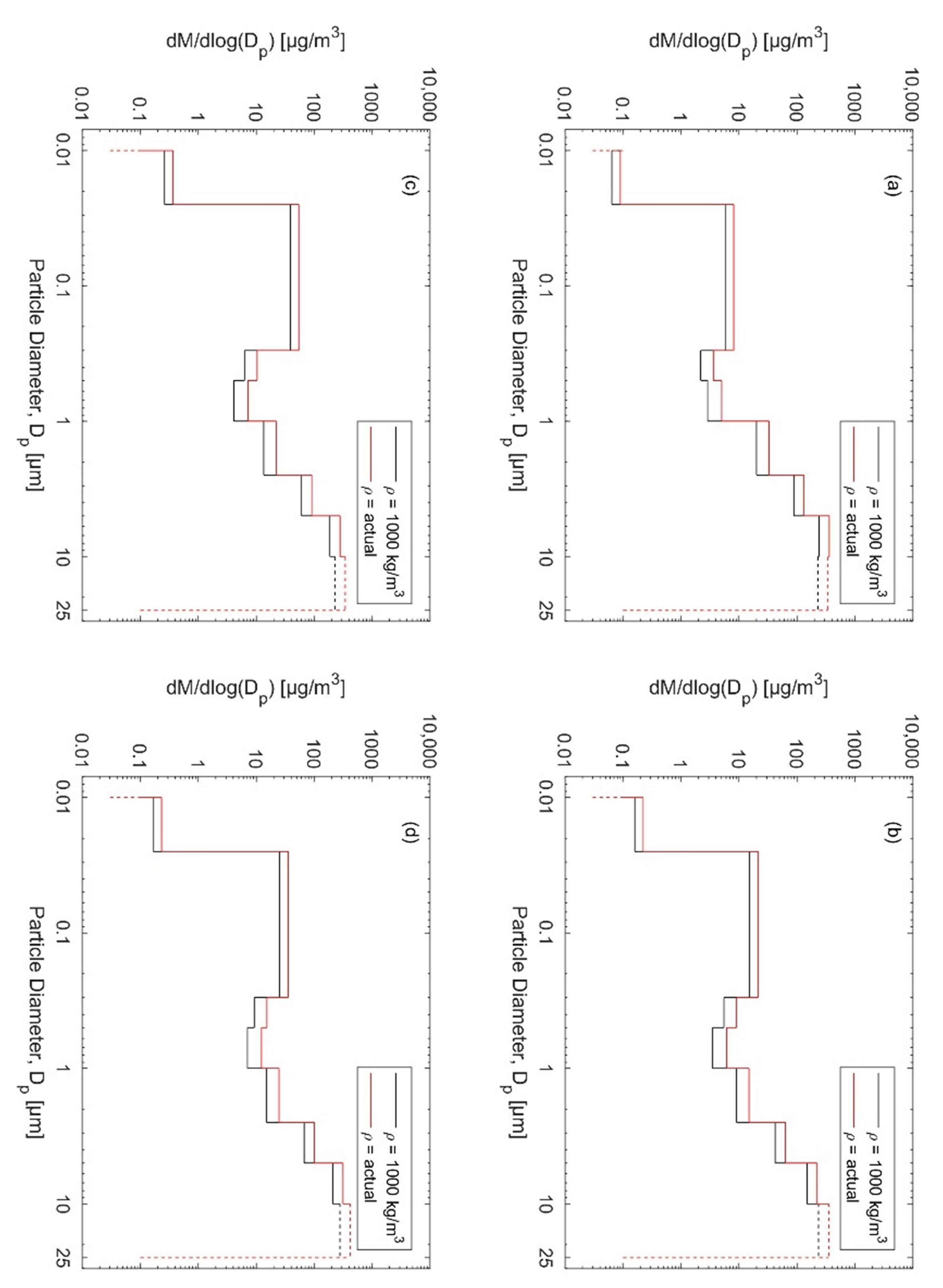
2.3. Particle Size Distributions
3. Results and Discussion
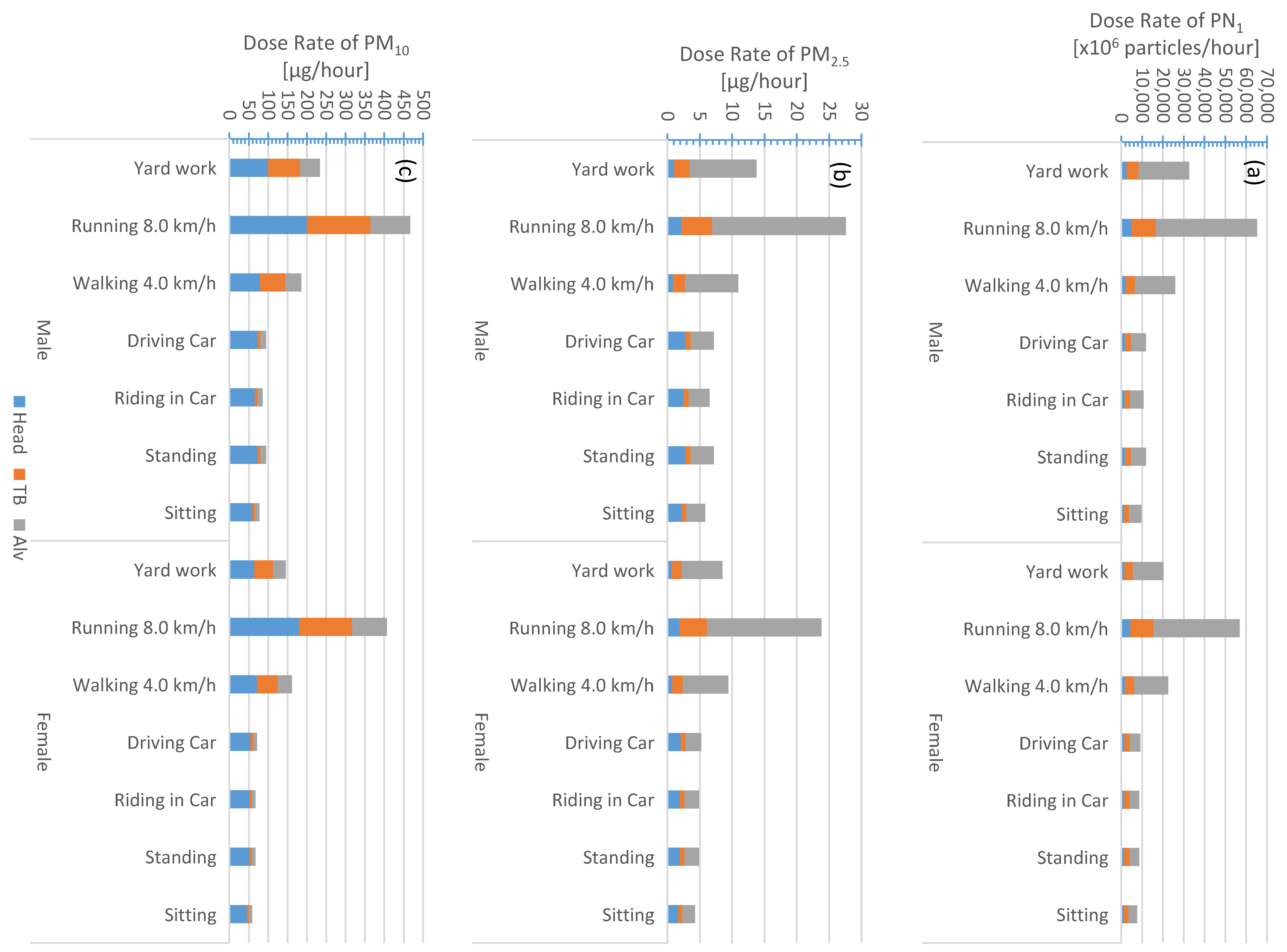
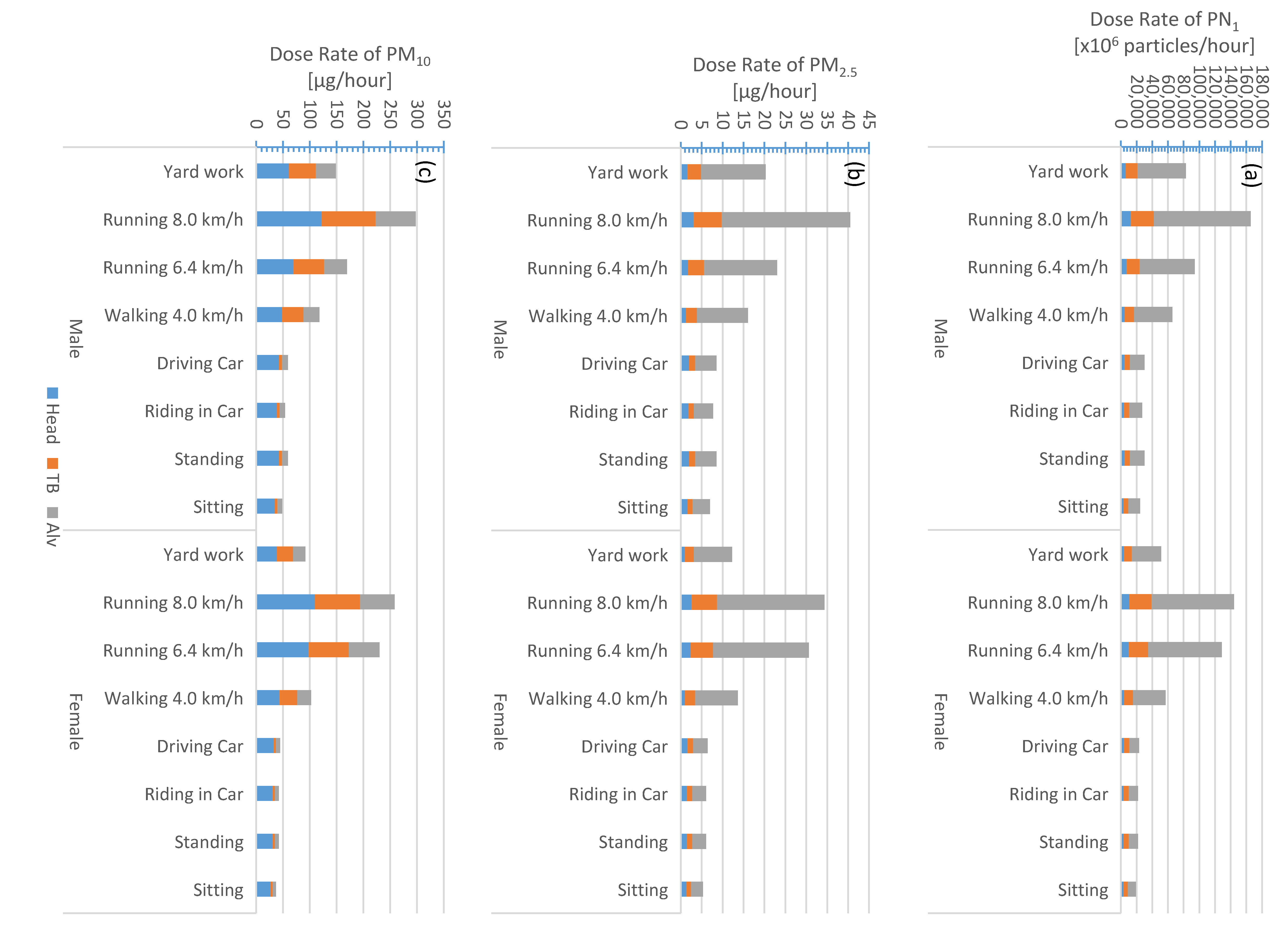
3.1. Regional and Total Inhaled Dose Rate
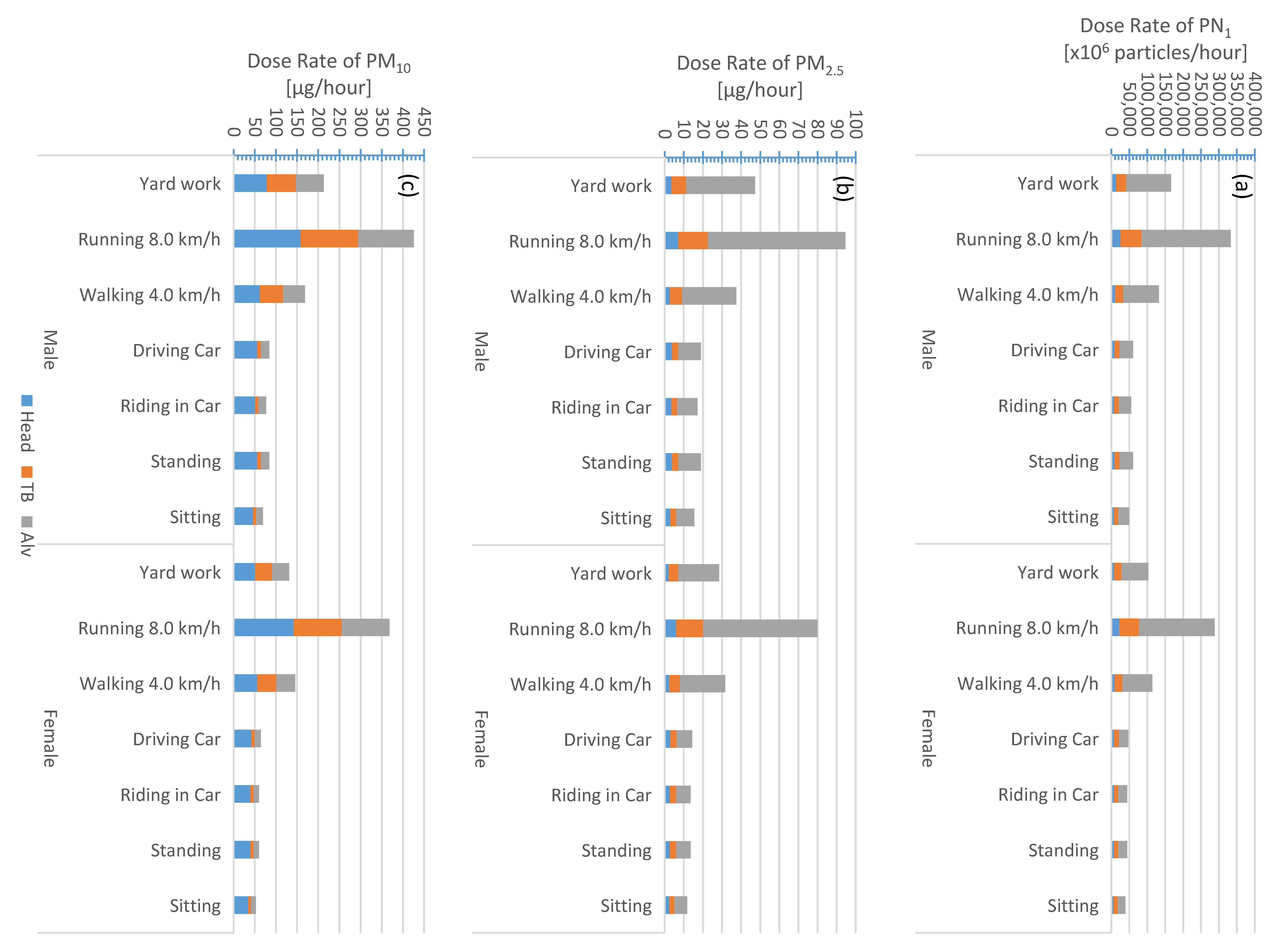
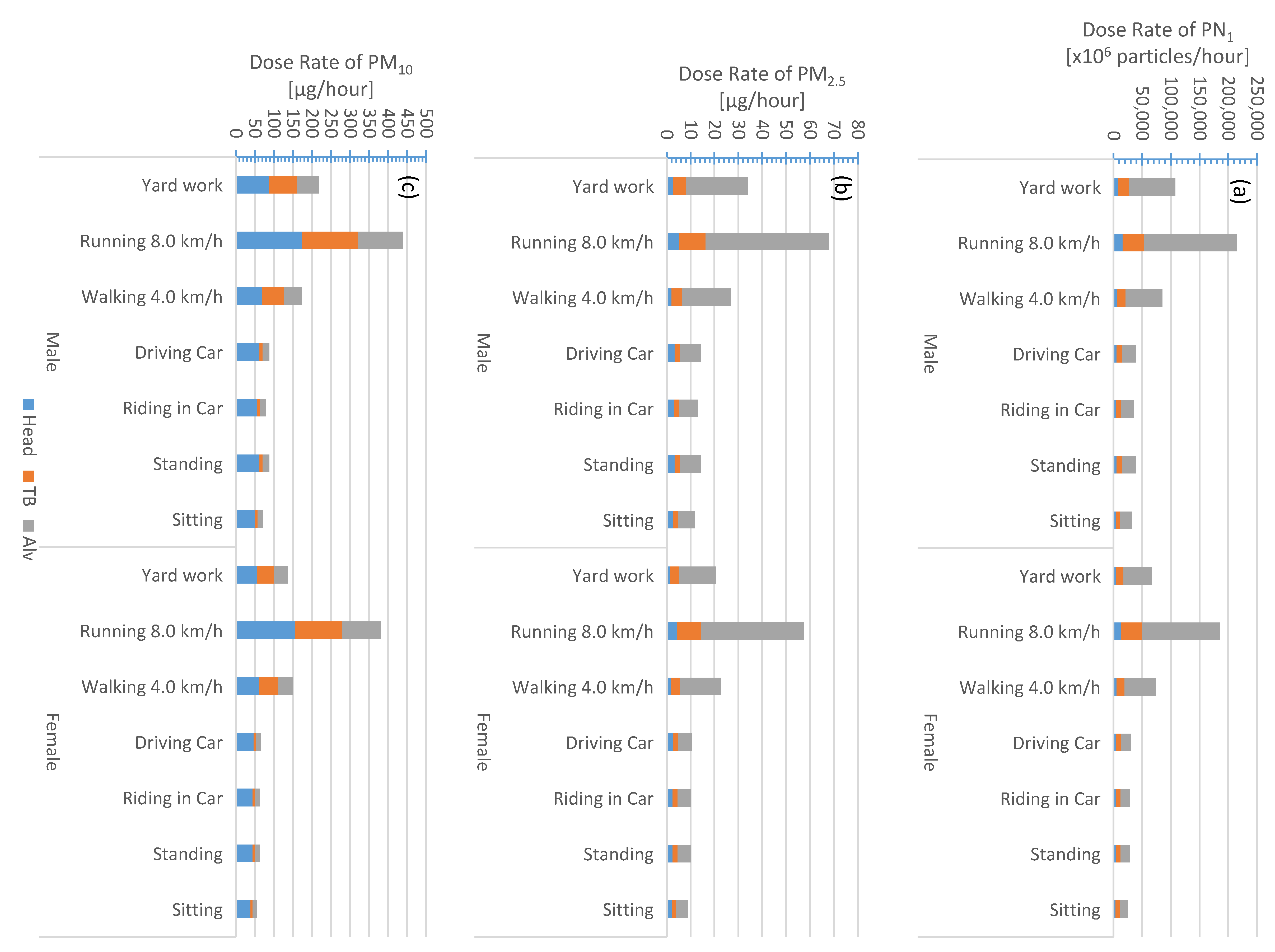
3.2. Scenarios of Exposure and Correspinding Dose Rate
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fenger, J. Urban air quality. Atmos. Environ. 1999, 33, 4877–4900. [Google Scholar] [CrossRef]
- Anderson, H.R. Air pollution and mortality: A history. Atmos. Environ. 2009, 43, 142–152. [Google Scholar] [CrossRef]
- Dockery, D.W.; Luttmann-Gibson, H.; Rich, D.Q.; Link, M.S.; Mittleman, M.A.; Gold, D.R.; Koutrakis, P.; Schwartz, J.D.; Verrier, R.L. Association of Air Pollution with Increased Incidence of Ventricular Tachyarrhythmias Recorded by Implanted Cardioverter Defibrillators. Environ. Health Perspect. 2005, 113, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohmann, U.; Feichter, J. Global indirect aerosol effects: A review. Atmos. Chem. Phys. 2005, 5, 715–737. [Google Scholar] [CrossRef]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. Am. Med. Assoc. 2002, 287, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Künzli, N.; Kaiser, R.; Medina, S.; Studnicka, M.; Chanel, O.; Filliger, P.; Herry, M.; Horak, F., Jr.; Puybonnieux-Texier, V.; Quénel, P.; et al. Public-health impact of outdoor and traffic-related airpollution: A European assessment. Lancet 2000, 356, 795–801. [Google Scholar]
- Jones, A.P. Indoor air quality and health. Atmos. Environ. 1999, 33, 4535–4564. [Google Scholar] [CrossRef]
- Pope, C.A.; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. 2006, 56, 709–742. [Google Scholar] [CrossRef]
- Hänninen, O.; Knol, A.; Jantunen, M.; Lim, T.A.; Conrad, A.; Rappolder, M.; Carrer, P.; Fanetti, A.-C.; Kim, R.; Buekers, J.; et al. Environmental burden of disease in Europe: Asessing nine risk factors in six countries. Environ. Health Perspect. 2014, 122, 439–446. [Google Scholar] [CrossRef]
- WHO. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks; WHO: Geneva, Switzerland, 2018; ISBN 978 92 4 156519 6. [Google Scholar]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Downward, G.S.; van Nunen, E.J.H.M.; Kerckhoffs, J.; Vineis, P.; Brunekreef, B.; Boer, J.M.A.; Messier, K.P.; Roy, A.; Monique, W.; Verschuren, M.; et al. Long-Term Exposure to Ultrafine Particles and Incidence of Cardiovascular and Cerebrovascular Disease in a Prospective Study of a Dutch Cohort. Environ. Health Perspect. 2018, 126, 127007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rönkkö, T.J.; Jalava, P.I.; Happo, M.S.; Kasurinen, S.; Sippula, O.; Leskinen, A.; Koponen, H.; Kuuspalo, K.; Ruusunen, J.; Väisänen, O.; et al. Emissions and atmospheric processes influence the chemical composition and toxicological properties of urban air particulate matter in Nanjing, China. Sci. Total Environ. 2018, 639, 1290–1310. [Google Scholar] [CrossRef]
- Allen, J.L.; Oberdorster, G.; Morris-Schaffer, K.; Wong, C.; Klocke, C.; Sobolewski, M.; Conrad, K.; Mayer-Proschel, M.; Cory-Slechta, D.A. Developmental neurotoxicity of inhaled ambient ultrafine particle air pollution: Parallels with neuropathological and behavioral features of autism and other neurodevelopmental disorders. Neurotoxicology 2017, 59, 140–154. [Google Scholar] [CrossRef] [PubMed]
- Pieters, N.; Koppen, G.; Van Poppel, M.; de Prins, S.; Cox, B.; Dons, E.; Nelen, V.; Panis, L.I.; Plusquin, M.; Schoeters, G.; et al. Blood Pressure and Same-Day Exposure to Air Pollution at School: Associations with Nano-Sized to Coarse PM in Children. Environ. Health Perspect. 2015, 123, 0737–0742. [Google Scholar] [CrossRef] [PubMed]
- Osunsanya, T.; Prescott, G.; Seaton, A. Acute respiratory effects of ultrafine particles: Mass or number? J. Occup. Environ. Med. 2001, 58, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Stoeger, T.; Reinhard, C.; Takenaka, S.; Schroeppel, A.; Karg, E.; Ritter, B.; Heyder, J.; Schulz, H. Instillation of six different ultrafine carbon particles indicates a surface area threshold dose for acute lung inflammation in mice. Environ. Health Perspect. 2005, 114, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Cassee, F.R.; Héroux, M.E.; Gerlofs-Nijland, M.E.; Kelly, F.J. Particulate matter beyond mass: Recent health evidence on the role of fractions, chemical constituents and sources of emission. Inhal. Toxicol. 2013, 25, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Fussell, J.C. Size, source and chemical composition as determinants of toxicity attributable to ambient particulate matter. Atmos. Environ. 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Nethery, E.; Leckie, S.E.; Teschke, K.; Brauer, M. From measures to models: An evaluation of air pollution exposure assessment for epidemiological studies of pregnant women. J. Occup. Environ. Med. 2008, 65, 579–586. [Google Scholar] [CrossRef]
- Gerharz, L.E.; Pebesma, E. Using geostatistical simulation to disaggregate air quality model results for individual exposure estimation on GPS tracks. Stoch. Res. Risk Assess. 2013, 27, 223–234. [Google Scholar] [CrossRef]
- Löndahl, J.; Massling, A.; Pagels, J.; Swietlicki, E.; Vaclavik, E.; Loft, S. Size-resolved respiratory-tract deposition of fine and ultrafine hydrophobic and hygroscopic aerosol particles during rest and exercise. Inhal. Toxicol. 2007, 19, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Hussein, T.; Wierzbicka, A.; Löndahl, J.; Lazaridis, M.; Hänninen, O. Indoor Aerosol Modeling for Assessment of Exposure and Respiratory Tract Deposited Dose. Atmos. Environ. 2015, 106, 402–411. [Google Scholar] [CrossRef]
- Ferron, G.A.; Gebhart, J. Estimation of the lung deposition of aerosol particles produced with medical nebulizers. J. Aerosol Sci. 1988, 19, 1083–1086. [Google Scholar] [CrossRef]
- Choi, H.S.; Ashitate, Y.; Lee, J.H.; Kin, S.H.; Matsui, A.; Insin, N.; Bawendi, M.G.; Semmler-Behnke, M.; Frangioni, J.V.; Tsuda, A. Rapid translocation of nanoparticles from the lung airspaces to the body. Nat. Biotechnol. 2010, 28, 1300–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, V.; Miller, M.R.; Clift, M.J.D.; Elder, A.; Mills, N.L.; Møller, P.; Schins, R.P.F.; Vogel, U.; Kreyling, W.G.; Alstrup Jensen, K.; et al. Nanomaterials Versus Ambient Ultrafine Particles: An Opportunity to Exchange Toxicology Knowledge. Environ. Health Perspect. 2017, 125, 106002. [Google Scholar] [CrossRef] [PubMed]
- Daigle, C.C.; Chalupa, D.C.; Gibb, F.R.; Morrow, P.E.; Oberdörster, G.; Utell, M.J.; Frampton, M.W. Ultrafine Particle Deposition in Humans During Rest and Exercise. Inhal. Toxicol. 2003, 15, 539–552. [Google Scholar] [CrossRef] [PubMed]
- ICRP. Annals of the International Commission on Radiological Protection ICRP Publication 66: Human Respiratory Tract Model for Radiological Protection; International Commission on Radiological Protection: Ottawa, ON, Canada, 1994; Pergamon 1994. [Google Scholar]
- Anjilvel, S.; Asgharian, B. A multiple-path model of particle deposition in the rat lung. Fundam. Appl. Toxicol. 1995, 28, 41–50. [Google Scholar] [CrossRef]
- Löndahl, J.; Swietlicki, E.; Rissler, J.; Bengtsson, A.; Boman, C.; Blomberg, A.; Sandström, T. Experimental determination of the respiratory tract deposition of diesel combustion particles in patients with chronic obstructive pulmonary disease. Part. Fibre Toxicol. 2012, 9, 1–8. [Google Scholar] [CrossRef]
- Chalupa, D.C.; Morrow, P.E.; Oberdörster, G.; Utell, M.J.; Frampton, M.W. Ultrafine Particle Deposition in Subjects with Asthma. Environ. Health Perspect. 2004, 112, 879–882. [Google Scholar] [CrossRef]
- Anderson, P.J.; Wilson, J.D.; Hiller, F.C. Respiratory tract deposition of ultrafine particles disease in subjects with obstructive or restrictive lung. Chest 1990, 97, 1115–1120. [Google Scholar] [CrossRef]
- Zeman, W.D.B.K.L. Deposition of fine particles in children spontaneously breathing at rest. Inhal. Toxicol. 1998, 10, 831–842. [Google Scholar]
- Rissler, J.; Gudmundsson, A.; Nicklasson, H.; Swietlicki, E.; Wollmer, P.; Löndahl, J. Deposition efficiency of inhaled particles (15–5000 nm) related to breathing pattern and lung function: An experimental study in healthy children and adults. Part. Fibre Toxicol. 2017, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Löndahl, J.; Massling, A.; Swietlicki, E.; Bräuner, E.V.; Ketzel, M.; Pagels, J.; Loft, S. Experimentally determined human respiratory tract deposition of airborne particles at a busy street. Environ. Sci. Technol. 2009, 43, 4659–4664. [Google Scholar] [CrossRef] [PubMed]
- Oberdörster, G.; Oberdörster, E.; Oberdörster, J. Nanotoxicology: An emerging discipline evolving from studies of ultrafine particles. Environ. Health Perspect. 2005, 113, 823–839. [Google Scholar] [CrossRef] [PubMed]
- Stoeger, T.; Schmid, O.; Takenaka, S.; Schulz, H. Inflammatory response to TiO2 and carbonaceous particles scales best with BET surface area. Environ. Health Perspect. 2007, 115, A290–A291. [Google Scholar] [CrossRef] [PubMed]
- Stoeger, T.; Takenaka, S.; Frankenberger, B.; Ritter, B.; Karg, E.; Maier, K.; Schulz, H.; Schmid, O. Deducing in vivo toxicity of combustion-derived nanoparticles from a cell-free oxidative potency assay and metabolic activation of organic compounds. Environ. Health Perspect. 2009, 117, 54–60. [Google Scholar] [CrossRef]
- Waters, K.M.; Masiello, L.M.; Zangar, R.C.; Tarasevich, B.J.; Karin, N.J.; Quesenberry, R.D.; Bandyopadhyay, S.; Teeguarden, J.G.; Pounds, J.G.; Thrall, B.D. Macrophage responses to silica nanoparticles are highly conserved across particle sizes. Toxicol. Sci. 2009, 107, 553–569. [Google Scholar] [CrossRef]
- Braakhuis, H.M.; Cassee, F.R.; Fokkens, P.H.; De La Fonteyne, L.J.; Oomen, A.G.; Krystek, P.; De Jong, W.H.; Van Loveren, H.; Park, M.V. Identification of the appropriate dosemetric for pulmonary inflammation of silver nanoparticles in an inhalation toxicity study. Nanotoxicology 2016, 10, 63–73. [Google Scholar]
- Schmid, O.; Stoeger, T. Surface area is the biologicallymost effective dosemetric for acute nanoparticle toxicity in the lung. J. Aerosol Sci. 2016, 99, 133–143. [Google Scholar] [CrossRef]
- Fadeel, B.; Bussy, C.; Merino, S.; Vázquez, E.; Flahaut, E.; Mouchet, F.; Evariste, L.; Gauthier, L.; Koivisto, J.; Vogel, U.; et al. Safety Assessment of Graphene-Based Materials: Focus on Human Health and the Environment. ACS Nano 2018, 12, 10582–10620. [Google Scholar] [CrossRef]
- Oberdörster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Kreyling, W.; Cox, C. Translocation of Inhaled Ultrafine Particles to the Brain. Inhal. Toxicol. 2004, 16, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Hussein, T.; Löndahl, J.; Paasonen, P.; Koivisto, A.J.; Petäjä, T.; Hämeri, K.; Kulmala, M. Modeling Regional Deposited Dose of Submicron Aerosol Particles. Sci. Total Environ. 2013, 458, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Hussein, T.; Boor, B.E.; Dos Santos, V.N.; Kangasluoma, J.; Petäjä, T.; Lihavainen, H. Mobile aerosol measurement in the eastern Mediterranean—A utilization of portable instruments. Aerosol Air Qual. Res. 2017, 17, 1775–1786. [Google Scholar] [CrossRef]
- Hussein, T.; Juwhari, H.; AlKuisi, M.; Alkattan, H.; Lahlouh, B.; Al-Hunaiti, A. Accumulation and coarse mode aerosol concentrations and carbonaceous contents in the urban background atmosphere in Amman—Jordan. Arab. J. Geosci. 2018, 11, 617. [Google Scholar] [CrossRef]
- Hussein, T.; Halayka, M.; Abu Al-Ruz, R.; Abdullah, H.; Mølgaard, B.; Petäjä, T. Fine particle number concentrations in Amman and Zarqa during spring 2014. Jordan J. Phys. 2016, 9, 31–46. [Google Scholar]
- Hussein, T.; Rasha, A.; Tuukka, P.; Heikki, J.; Arafah, D.; Kaarle, H.; Markku, K. Local air pollution versus short–range transported dust episodes: A comparative study for submicron particle number concentration. Aerosol Air Qual. Res. 2011, 11, 109–119. [Google Scholar] [CrossRef]
- Hussein, T.; Betar, A. Size fractionated number and mass concentrations in the urban background atmosphere during spring 2014 in Amman—Jordan. Jordan J. Phys. 2017, 10, 51–60. [Google Scholar]
- Holmes, J.R. How much Air Do We Breath? California Environmental Protection Agency: Sacramento, CA, USA, 1994; Research Note 94–11.
- Hussein, T.; Saleh, S.; dos Santos, V.N.; Abdullah, H.; Boor, B.E. Black Carbon and Particulate Matter Concentrations in Eastern Mediterranean Urban Conditions–An Assessment Based on Integrated Stationary and Mobile Observations. Atmosphere 2019, 10, 323. [Google Scholar] [CrossRef]
- Abdeen, Z.; Qasrawi, R.; Heo, J.; Wu, B.; Shpund, J.; Vanger, A.; Sharf, G.; Moise, T.; Brenner, S.; Nassar, K.; et al. Spatial and Temporal Variation in Fine Particulate Matter Mass and Chemical Composition: The Middle East Consortium for Aerosol Research Study. Sci. World J. 2014, 878704, 1–16. [Google Scholar] [CrossRef]
- Wu, T.; Boor, B.E. Urban Atmos. Aerosol Size Distributions: A Global Perspective. In Preparation.
- Rissler, J.; Nordin, E.Z.; Eriksson, A.C.; Nilsson, P.T.; Frosch, M.; Sporre, M.K.; Wierzbicka, A.; Svenningsson, B.; Löndahl, J.; Messing, M.E.; et al. Effective Density and Mixing State of Aerosol Particles in a Near-Traffic Urban Environment. Environ. Sci. Technol. 2014, 48, 6300–6308. [Google Scholar] [CrossRef]
- Lin, Y.; Bahreini, R.; Zimmerman, S.; Fofie, E.A.; Asa-Awuku, A.; Park, K.; Lee, S.-B.; Bae, G.-N.; Jung, H.S. Investigation of ambient aerosol effective density with and without using a catalytic stripper. Atmos. Environ. 2018, 187, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Swietlicki, E.; Hansson, H.C.; Hämeri, K.; Svenningsson, B.; Massling, A.; McFiggans, G.; McMurry, P.H.; Petäjä, T.; Tunved, P.; Gysel, M.; et al. Hygroscopic properties of submicrometer atmospheric aerosol particles measured with H–TDMA instruments in various environments—A review. Tellus B 2008, 60, 432–469. [Google Scholar] [CrossRef]
- Löndahl, J.; Pagels, J.; Boman, C.; Swietlicki, E.; Massling, A.; Rissler, J.; Blomberg, A.; Bohgard, M.; Sandström, T. Deposition of biomass combustion aerosol particles in the human respiratory tract. Inhal. Toxicol. 2008, 20, 923–933. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Activity | Females | Males | DF Curve Type |
|---|---|---|---|
| Yard work | 1.08 | 1.74 | Exercise |
| Running (8.0 km/h) | 3.03 | 3.48 | Exercise |
| Walking (4.0 km/h) | 1.20 | 1.38 | Exercise |
| Driving car | 0.51 | 0.66 | at rest |
| Riding in car | 0.48 | 0.60 | at rest |
| Standing | 0.48 | 0.66 | at rest |
| Sitting | 0.42 | 0.54 | at rest |
| Range of Dp [µm] | 0.01–0.025 | 0.025–0.3 | 0.3–0.5 | 0.5–1 | 1–2.5 | 2.5–5 | 5–10 |
| Eff ρp [kg/m3] | 1400 | 1400 | 1650 | 1750 | 1650 | 1500 | 1500 |
| Scenario | Occupation or Social Status | Gender | Activity (s) | Location (s) | Short Description |
|---|---|---|---|---|---|
| In-vehicle | Taxi Driver | Male | Driving | Roads Downtown Urban Background | Urban inhabitants might spend long periods in transit and transportation; this can take several hours per day, especially when traffic congestion is very common in some cities |
| Urban inhabitant Tourist | Male Female | Riding | |||
| Police Officer | Male Female | Driving Riding | Roads Downtown Urban Background | Some police officers in Amman spend a long time in-vehicle as traffic surveillance | |
| On road | Urban inhabitant Tourist | Male Female | Standing Walking | Roads Downtown | Gather at nearby attraction sites in different places |
| Police Officer | Male Female | Standing Walking | Roads Downtown Urban Background | Some police officers in Amman spend a long time on road trying to traffic in order and reduce on road congestion | |
| Service Worker | Male | (eq.) Yard Work | Waste service workers and road construction spend most of their working time on road | ||
| University Student | Male Female | Standing Walking Running | Urban Background | University students spend most of their daytime either on campus or in its surrounding | |
| Outdoor Sports | Male Female | Running | Anywhere in the city | Some people enjoy outdoor sports such jogging, walking, biking, etc. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, T.; Saleh, S.S.A.; dos Santos, V.N.; Boor, B.E.; Koivisto, A.J.; Löndahl, J. Regional Inhaled Deposited Dose of Urban Aerosols in an Eastern Mediterranean City. Atmosphere 2019, 10, 530. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos10090530
Hussein T, Saleh SSA, dos Santos VN, Boor BE, Koivisto AJ, Löndahl J. Regional Inhaled Deposited Dose of Urban Aerosols in an Eastern Mediterranean City. Atmosphere. 2019; 10(9):530. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos10090530
Chicago/Turabian StyleHussein, Tareq, Shatha Suleiman Ali Saleh, Vanessa N. dos Santos, Brandon E. Boor, Antti J. Koivisto, and Jakob Löndahl. 2019. "Regional Inhaled Deposited Dose of Urban Aerosols in an Eastern Mediterranean City" Atmosphere 10, no. 9: 530. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos10090530