The Relationship Between Air Pollution and All-Cause Mortality in Singapore

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Southeast Asian (SEA) Transboundary Haze Situation
2.3. Exposure Variables
2.4. Outcome Variable
2.5. Ethics Approval
2.6. Statistical Analysis
3. Results
3.1. Study Population
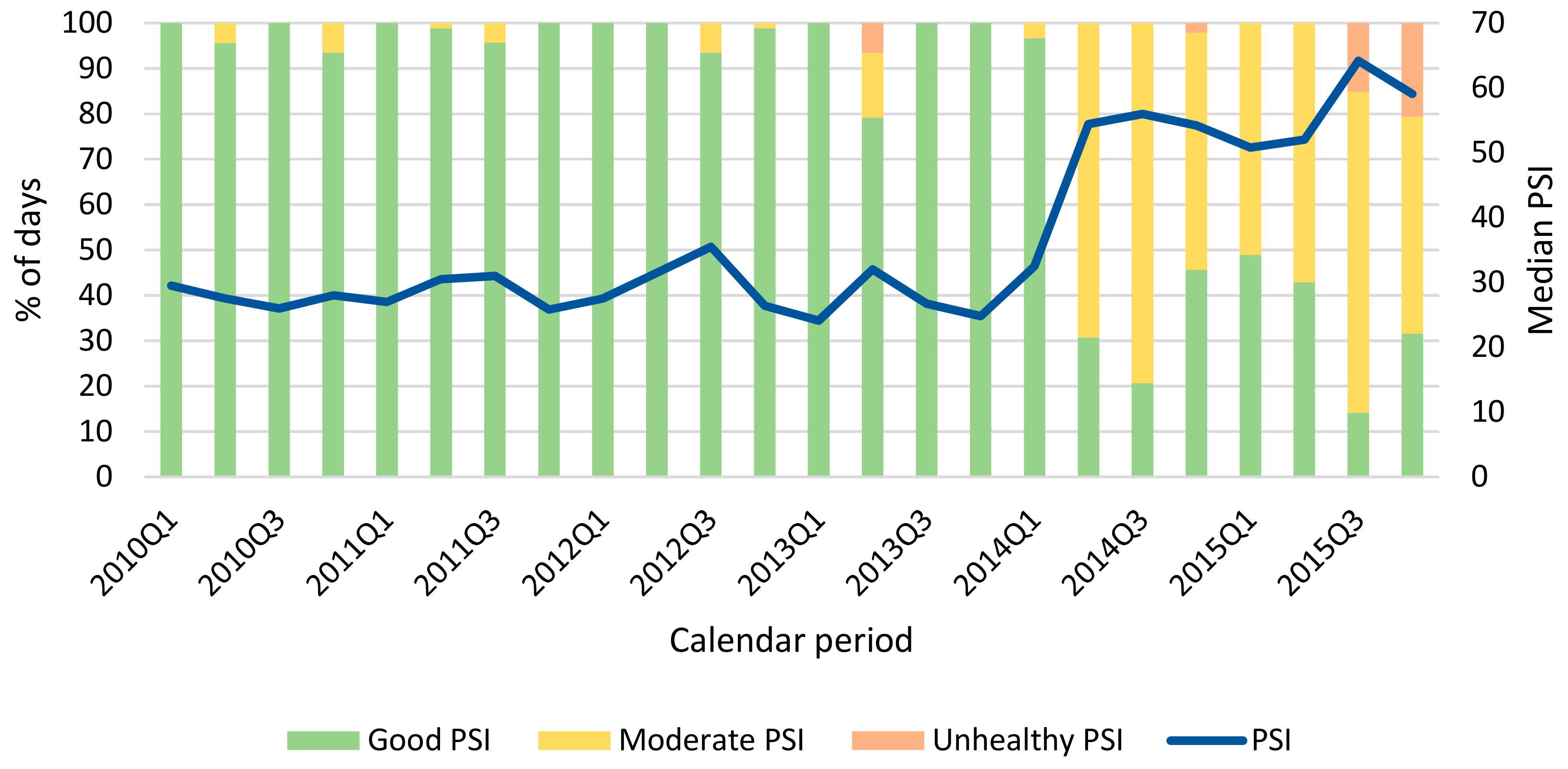
3.2. Description of Environmental Variables
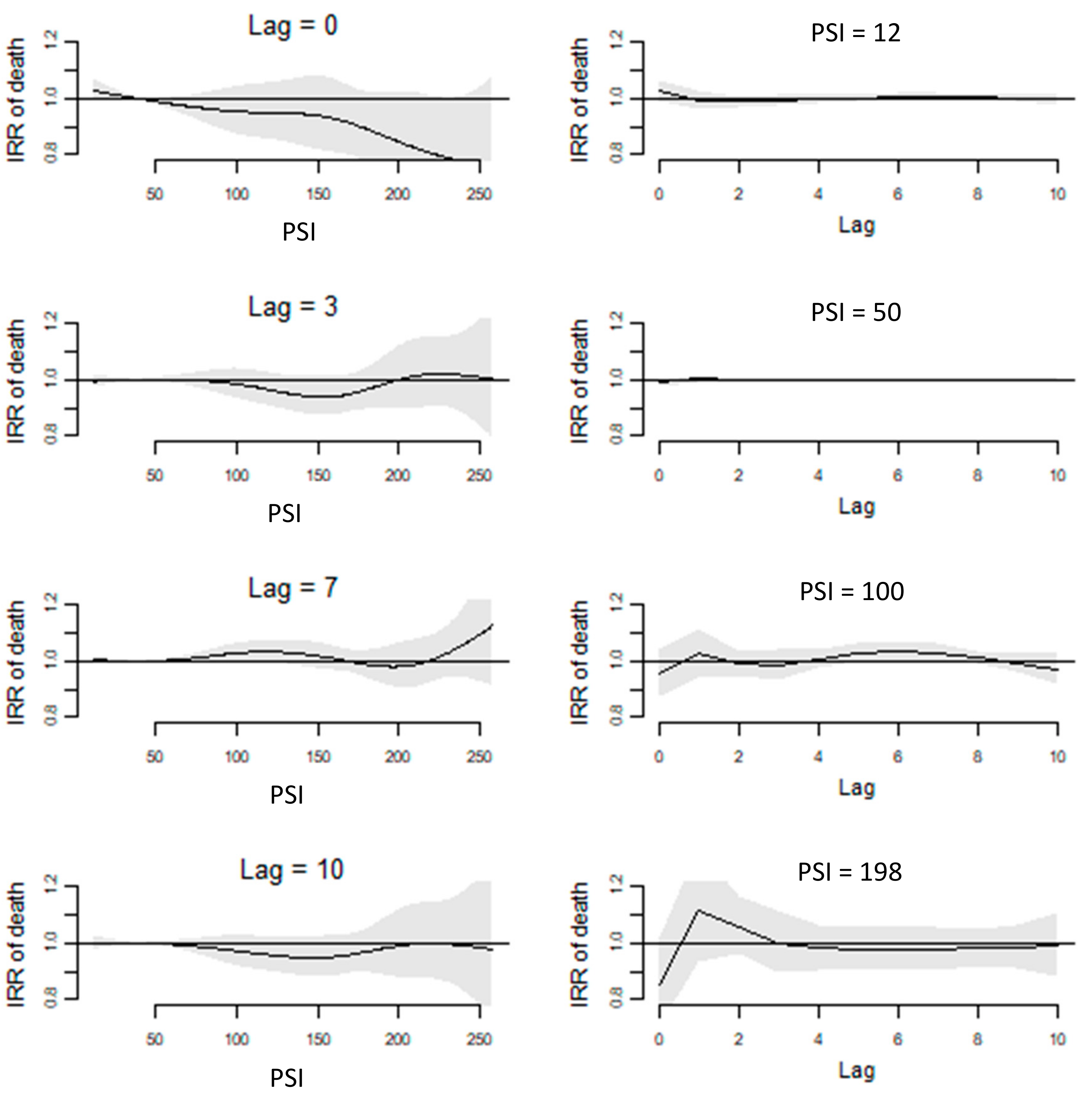
3.3. Short-Term Effects of PSI on Mortality
3.4. Intermediate-Term Effects of PSI on Mortality
4. Discussion
4.1. Study Strengths
4.2. Future Work
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brauer, M. Air pollution, stroke and anxiety. BMJ 2015, 350, h1510. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Beelen, R.; Hoek, G.; Schouten, L.; Bausch-Goldbohm, S.; Fischer, P.; Armstrong, B.; Hughes, E.; Jerrett, M. Effects of long-term exposure to traffic-related air pollution on respiratory and cardiovascular mortality in the Netherlands: The NLCS-AIR study. Res. Rep. Health Eff. Inst. 2009, 139, 5–71. [Google Scholar]
- Achilleos, S.; Kioumourtzoglou, M.; Wu, C.; Schwartz, J.; Koutrakis, P.; Papatheodorou, S. Acute effects of fine particulate matter constituents on mortality: A systematic review and meta-regression analysis. Environ. Int. 2017, 109, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Fajersztajn, L.; Saldiva, P.; Pereira, L.; Leite, V.; Buehler, A. Short-term effects of fine particulate matter pollution on daily health events in Latin America: A systematic review and meta-analysis. Int. J. Public Health 2017, 62, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.; Mills, I.; Walton, H.; Anderson, H. Fine particle components and health--a systematic review and meta-analysis of epidemiological time series studies of daily mortality and hospital admissions. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 208–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beelen, R.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M.; Vineis, P.; et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014, 383, 785–795. [Google Scholar] [CrossRef]
- Di, Q.; Zanobetti, A.; Wang, Y.; Koutrakis, P.; Choirat, C.; Dominici, F.; Schwartz, J.D. Air Pollution and Mortality in the Medicare Population. N. Engl. J. Med. 2017, 376, 2513–2522. [Google Scholar] [CrossRef]
- Wichmann, J.; Torp-Pedersen, C.; Lippert, F.; Ketzel, M.; Ellermann, T.; Loft, S. Out-of-Hospital Cardiac Arrests and Outdoor Air Pollution Exposure in Copenhagen, Denmark. PLoS ONE 2013, 8, e53684. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.; Vichit-Vadakan, N.; Vajanapoom, N.; Ostro, B.; Thach, T.; Chau, P.; Chan, E.K.; Chungn, R.Y.; Ou, C.Q.; Yang, L.; et al. Part 5. Public health and air pollution in Asia (PAPA): A combined analysis of four studies of air pollution and mortality. Res. Rep. Health Eff. Inst. 2010, 154, 377–418. [Google Scholar]
- Chen, C.C.; Yang, C.Y. Association between Fine Particulate Air Pollution and Daily Clinic Visits for Migraine in a Subtropical City: Taipei, Taiwan. Int. J. Environ. Res. Public Health 2015, 12, 4697–4708. [Google Scholar] [CrossRef] [Green Version]
- Ho, A.; Wah, W.; Earnest, A.; Ng, Y.; Xie, Z.; Shahidah, N.; Yap, S.; Pek, P.P.; Liu, N.; Lam, S.S.W.; et al. Health impacts of the Southeast Asian haze problem—A time-stratified case crossover study of the relationship between ambient air pollution and sudden cardiac deaths in Singapore. Int. J. Cardiol. 2018, 271, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.Y.; Leow, A.S.; Ngiam, N.J.; Ng, B.S.; Sharma, M.; Yeo, L.L.; Seow, P.A.; Hong, C.S.; Chee, Y.H.; Chen, J.; et al. Psychosomatic symptoms during South East Asian haze crisis are related to changes in cerebral hemodynamics. PLoS ONE 2019, 14, e0208724. [Google Scholar] [CrossRef] [PubMed]
- Xiang, H.M.; Arena, V.C.; Brink, L.L.; Xu, X.; Bi, Y.; Talbott, E.O. Estimation of Short-Term Effects of Air Pollution on Stroke Hospital Admissions in Wuhan, China. PLoS ONE 2013, 8, e61168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, P.H.G.; Fan, M.; Chiu, K.Y.; Fan, M.; Liu, C.; Xue, A.; Liu, T.; Pan, Y.; Mu, Q.; Zhou, M. Particulate air pollution and mortality in 38 of China′s largest cities: Time series analysis. BMJ 2017, 356, j1379. [Google Scholar]
- Qiu, H.; Pun, V.; Tian, L. Short-term effects of fine and coarse particles on deaths in Hong Kong elderly population: An analysis of mortality displacement. Environ. Pollut. 2018, 241, 148–154. [Google Scholar] [CrossRef]
- Wu, R.; Zhong, L.; Huang, X.; Xu, H.; Liu, S.; Feng, B.; Wang, T.; Song, X.; Bai, Y.; Wu, F.; et al. Temporal variations in ambient particulate matter reduction associated short-term mortality risks in Guangzhou, China: A time-series analysis (2006–2016). Sci. Total Environ. 2018, 645, 491–498. [Google Scholar] [CrossRef]
- Maji, K.; Arora, M.; Dikshit, A. Burden of disease attributed to ambient PM2.5 and PM10 exposure in 190 cities in China. Environ. Sci. Pollut. Res. Int. 2017, 24, 11559–11572. [Google Scholar] [CrossRef]
- Khoo, K. The haze and health: A blog about the fog. Ann. Acad. Med. Singap. 2006, 35, 909–910. [Google Scholar]
- Ho, A.F.W.; Zeng, H.; Earnest, A.; Cheong, K.H.; Pek, P.P.; Sia, C.-H.; Jeon, Y.S.; Tan, B.Y.Q.; Liu, N.; Kwan, Y.H.; et al. A time-stratified case crossover study of the association of outdoor ambient air pollution with the risk of acute myocardial infarction in the context of seasonal exposure to the Southeast Asian Haze problem. J. Am. Heart Assoc. 2019, 8, e011272. [Google Scholar] [CrossRef] [Green Version]
- Vadrevu, K.; Lasko, K.; Giglio, L.; Justice, C. Analysis of Southeast Asian pollution episode during June 2013 using satellite remote sensing datasets. Environ. Pollut. 2014, 195, 245–256. [Google Scholar] [CrossRef]
- Xu, J.; Tai, X.; Betha, R.; He, J.; Balasubramanian, R. Comparison of physical and chemical properties of ambient aerosols during the 2009 haze and non-haze periods in Southeast Asia. Environ. Geochem. Health 2015, 37, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, S.C. Impact to lung health of haze from forest fires: The Singapore experience. Respirology 2000, 5, 175–182. [Google Scholar] [CrossRef]
- Yeo, B.; Liew, C.; Oon, H. Clinical experience and impact of a community-led volunteer atmospheric haze clinic in Singapore. Southeast Asian J. Trop. Med. Public. Health 2014, 45, 1448–1453. [Google Scholar] [PubMed]
- Chew, R.; Andrea, B.; Mohammad, F.; Mohd, T.; Nurashikin, M.; Tidi, H. Annual Southeast Asia haze increases respiratory admissions:A 2-year large single institution experience. Respirology 2018, 23, 914–920. [Google Scholar]
- Ho, A.F.; Zheng, H.; De Silva, D.A.; Wah, W.; Earnest, A.; Pang, Y.H.; Xie, Z.; Pek, P.P.; Liu, N.; Ng, Y.Y.; et al. The Relationship Between Ambient Air Pollution and Acute Ischemic Stroke: A Time-Stratified Case-Crossover Study in a City-State With Seasonal Exposure to the Southeast Asian Haze Problem. Ann. Emerg. Med. 2018, 72, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Tian, L.; Cao, W.; Lai, P.; Wong, P.; Lee, R.S.Y.; Mason, T.G.; Krämer, A.; Wong, C.M. Urban climate modified short-term association of air pollution with pneumonia mortality in Hong Kong. Sci. Total. Environ. 2018, 646, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics Singopare. Population and Population Structure, Singapore; Government of Singapore: Singapore, 2018. Available online: https://www.singstat.gov.sg/find-data/search-by-theme/population/population-and-population-structure/latest-data (accessed on 15 December 2018).
- CIA. CIA World Factbook—East Asia/Southeast Asia; CIA: Singapore, 2018. Available online: https://www.cia.gov/library/publications/the-world-factbook/geos/sn.html (accessed on 9 December 2018).
- Ho, A.F.W.; Chew, D.; Wong, T.H.; Ng, Y.Y.; Pek, P.P.; Lim, S.H.; Anantharaman, V.; Hock Ong, M.E. Prehospital Trauma Care in Singapore. Prehosp. Emerg. Care 2015, 19, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Suwarsono, R.; Noviar, H.; Albar, I.; Phonekeo, C.; Song, Y. Influence of climate variation and vegetation greenness on fire occurrence: A case study in Central Kalimantan province. In Technology; Indonesian National Institute of Aeronautics and Space and Geoinformatics Center: Jakarta, Indonesia, 2007. [Google Scholar]
- Dennis, R.; Mayer, J.; Applegate, G. Fire, people and pixels: Linking social science and remote sensing to understand underlying causes and impacts of fires in Indonesia. Hum. Ecol. 2005, 33, 465–504. [Google Scholar] [CrossRef]
- Tan, A. The ‘haze’ crisis in Southeast Asia: Assessing Singapore′s transboundary haze pollution act 2014. NUS Law Work. Pap. Ser. 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- The National Environment Agency. Computation of the Pollutant Standards Index (PSI). In Ministry of Environment and Water Resources; Government of Singapore: Singapore, 2015. [Google Scholar]
- Registration of Births and Deaths Act (Chapter 267). Available online: https://sso.agc.gov.sg/Act/RBDA1937 (accessed on 15 January 2019).
- Ministry of Health, Singapore. Principal Causes of Death. Available online: https://www.moh.gov.sg/resources-statistics/singapore-health-facts/principal-causes-of-death (accessed on 15 January 2019).
- Armstrong, B.; Gasparrini, A.; Tobias, A. Conditional Poisson models: A flexible alternative to conditional logistic case cross-over analysis. BMC Med. Res. Methodol. 2014, 14, 122. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Armstrong, B.; Kenward, M. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muggeo, V. Modeling temperature effects on mortality: Multiple segmented relationships with common break points. Biostatistics 2008, 9, 613–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, R.; Dominici, F. A Bayesian hierarchical distributed lag model for estimating the time course of risk of hospitalization associated with particulate matter air pollution. J. R. Stat. Soc. Ser. A 2009, 58, 3–24. [Google Scholar] [CrossRef]
- Peng, R.; Dominici, F.; Louis, T. Model choice in time series studies of air pollution and mortality. J. R. Stat. Soc. Ser. A 2006, 169, 179–203. [Google Scholar] [CrossRef] [Green Version]
- National Environment Agency. Historical PSI Readings. Available online: https://www.haze.gov.sg/resources/historical-readings (accessed on 8 August 2019).
- Ministry of the Environment and Water Resources Singapore. Public Consultation on Transboundary Haze Pollution Bill; Ministry of the Environment and Water Resources Singapore: Singapore, 2014. [Google Scholar]
- Today. PM2.5 Levels Hit 471 as Haze Situation Worsens. Available online: https://www.todayonline.com/world/asia/pm25-levels-hit-471-haze-situation-worsens (accessed on 15 December 2018).
- Schwartz, J. Is there harvesting in the association of airborne particles with daily deaths and hospital admissions. Epidemiology 2001, 12, 55–61. [Google Scholar] [CrossRef]
- Rabl, A. Air pollution mortality: Harvesting and loss of life expectancy. J. Toxicol. Environ. Health Part A 2005, 68, 1175–1180. [Google Scholar] [CrossRef]
- Ramakreshnan, L.; Aghamohammadi, N.; Fong, C.; Bulgiba, A.; Zaki, R.; Wong, L.; Sulaiman, N.M. Haze and health impacts in ASEAN countries: A systematic review. Environ. Sci. Pollut. Res. Int. 2018, 25, 2096–2111. [Google Scholar] [CrossRef]
- Sahani, M.; Zainon, N.; Wan Mahiyuddin, W.; Latif, M.; Hod, R.; Khan, M.; Tahir, N.M.; Chan, C.-C. A case-crossover analysis of forest fire haze events and mortality in Malaysia. Atmos. Environ. 2014, 96, 257–265. [Google Scholar] [CrossRef]
- Johnston, F.; Henderson, S.; Morgan, G.; Bowman, D. Extreme air pollution events from bushfires and dust storms and their association with mortality in Sydney, Australia 1994–2007. Environ. Res. 2011, 111, 811–816. [Google Scholar] [CrossRef]
- Morgan, G.; Corbett, S.; Wlodarczyk, J.; Lewis, P. Air pollution and daily mortality in Sydney, Australia, 1989 through 1993. Am. J. Public Health 1998, 88, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Fischer, P.H.; Ameling, C.B.; Hoek, G.; Beelen, R.; de Hoogh, K.; Breugelmans, O.; Kruize, H.; Janssen, N.A.; Houthuijs, D. Air Pollution and Mortality in Seven Million Adults: The Dutch Environmental Longitudinal Study(DUELS). Environ. Health Perspect. 2015, 123, 697–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohebbi, M.; Wolfe, R.; Forbes, A. Disease Mapping and Regression with Count Data in the Presence of Overdispersion and Spatial Autocorrelation: A Bayesian Model Averaging Approach. Int. J. Environ. Res. Public Health 2014, 11, 883–902. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Z.J.; Kristiansen, L.C.; Andersen, K.K.; Olsen, T.S.; Hvidberg, M.; Jensen, S.S.; Ketzel, M.; Loft, S.; Sørensen, M.; Tjønneland, A.; et al. Stroke and long-term exposure to outdoor air pollution from nitrogen dioxide: A cohort study. Stroke 2012, 43, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, G.; Khalaj, B.; Ayyar, A.; Lincoln, D.; Jalaludin, B.; Beard, J.; Corbett, S.; Lumley, T. Effects of bushfire smoke on daily mortality and hospital admissions in Sydney, Australia. Epidemiology 2010, 21, 47–55. [Google Scholar] [CrossRef]
- Reid, C.E.; Johnston, F.H.; Jerrett, M.; Balmes, J.R.; Elliott, C.T. Critical Review of Health Impacts of Wildfire Smoke Exposure. Environ. Health Perspect. 2016, 124, 1334–1343. [Google Scholar] [CrossRef] [Green Version]
- Nadarajan, G.D.; Tiah, L.; Ho, A.F.W.; Azazh, A.; Castren, M.K.; Chong, S.L.; El Sayed, M.J.; Hara, T.; Leong, B.S.; Lippert, F.K.; et al. Global Resuscitation Alliance Utstein Recommendations for Developing Emergency Care Systems to improve Cardiac Arrest Survival. Resuscitation 2018, 132, 85–89. [Google Scholar] [CrossRef]
- Cheong, K.H.; Ngiam, N.J.; Morgan, G.G.; Pek, P.P.; Tan, B.Y.Q.; Lai, J.W.; Koh, J.M.; Ong, M.E.H.; Ho, A.F.W. Acute Health Impacts of the Southeast Asian Transboundary Haze Problem—A Review. Int. J. Environ. Res. Public Health 2019, 16, 3286. [Google Scholar]



{kind=link}
{kind=link}
| Overall (n = 2191) | Good PSI (n = 1721) | Moderate PSI (n = 429) | Unhealthy PSI (n = 41) | p-Value | |
|---|---|---|---|---|---|
| Daily average PSI, median (IQR) | 32.8 | 29.5 | 58.4 | 130.3 | - |
| (25.7–47.0) | (24.5–36.0) | (54.5–65.6) | (109.2–150.4) | ||
| Daily average temperature in °C, median (IQR) | 27.9 | 27.7 | 28.5 | 28.9 | <0.001 |
| (27.0–28.7) | (26.9–28.5) | (27.8–29.0) | (28.4–29.2) | ||
| Daily average wind speed in km/h, median (IQR) | 7.8 | 7.7 | 8.5 | 8.1 | 0.020 |
| (6.4–10.5) | (6.3–10.3) | (6.4–11.1) | (6.7–11.0) | ||
| Daily total rainfall in mm, median (IQR) | 0.0 | 0.2 | 0.0 | 0.0 | <0.001 |
| (0.0–4.0) | (0.0–4.8) | (0.0–2.2) | (0.0–0.2) | ||
| Number of days with rain, n (%) | 1051 (48.0) | 874 (50.8) | 166 (38.7) | 11 (26.8) | <0.001 |
| Risk Associated with Each PSI Range Compared to Good PSI | Risk Associated with Each 10-Unit Increase in PSI | |||
|---|---|---|---|---|
| Unadjusted IRR (95% CI) | Adjusted IRR (95% CI) ^ | Unadjusted IRR (95% CI) | Adjusted IRR (95% CI) ^ | |
| Overall | Not applicable | Not applicable | 1.01 | 1.01 |
| (1.01–1.02) * | (1.00–1.01) * | |||
| Good PSI | 1.00 | 1.00 | 1.02 | 1.01 |
| (reference) | (reference) | (1.01–1.03) * | (1.00–1.02) * | |
| Moderate PSI | 1.06 | 1.05 | 0.98 | 0.98 |
| (1.04–1.08) * | (1.03–1.07) * | (0.95–1.02) | (0.94–1.02) | |
| Unhealthy PSI | 1.10 | 1.08 | 0.99 | 0.99 |
| (1.05–1.16) * | (1.03–1.14) * | (0.87–1.14) | (0.85–1.16) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, A.F.W.; Zheng, H.; Cheong, K.H.; En, W.L.; Pek, P.P.; Zhao, X.; Morgan, G.G.; Earnest, A.; Tan, B.Y.Q.; Ng, Y.Y.; et al. The Relationship Between Air Pollution and All-Cause Mortality in Singapore. Atmosphere 2020, 11, 9. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos11010009
Ho AFW, Zheng H, Cheong KH, En WL, Pek PP, Zhao X, Morgan GG, Earnest A, Tan BYQ, Ng YY, et al. The Relationship Between Air Pollution and All-Cause Mortality in Singapore. Atmosphere. 2020; 11(1):9. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos11010009
Chicago/Turabian StyleHo, Andrew Fu Wah, Huili Zheng, Kang Hao Cheong, Wee Liang En, Pin Pin Pek, Xinxing Zhao, Geoffrey G. Morgan, Arul Earnest, Benjamin Yong Qiang Tan, Yih Yng Ng, and et al. 2020. "The Relationship Between Air Pollution and All-Cause Mortality in Singapore" Atmosphere 11, no. 1: 9. https://0-doi-org.brum.beds.ac.uk/10.3390/atmos11010009