
Cardiac Function after Modern Radiation Therapy with Volumetric Modulated Arc Therapy or Helical Tomotherapy for Advanced Left-Breast Cancer Receiving Regional Nodal Irradiation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
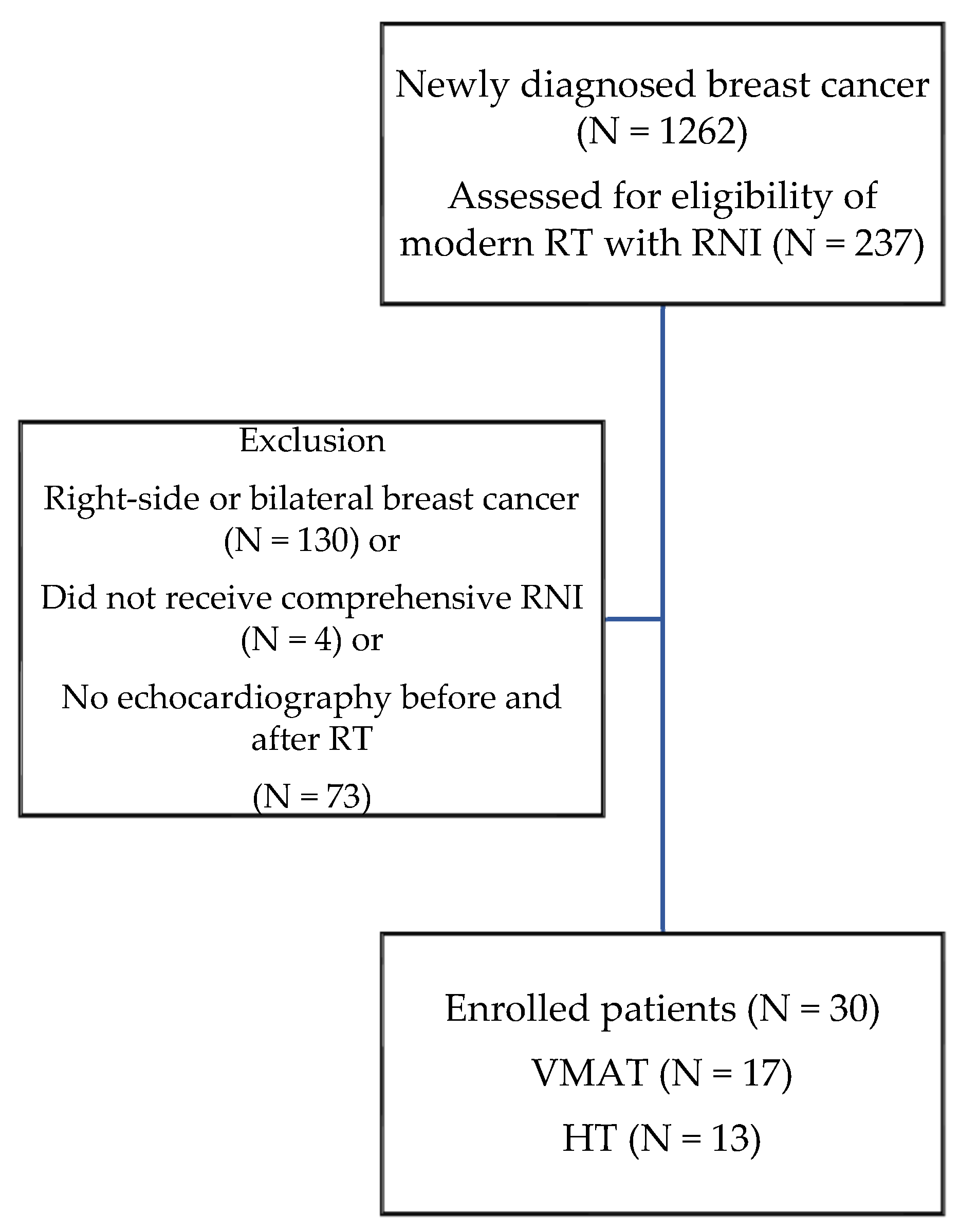
2.1. Patient Population and Cardiac Function Surveillance
2.2. RT Treatment Plan
2.3. RT Techniques and Dosimetry Evaluation
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. RT Dosimetry Outcomes
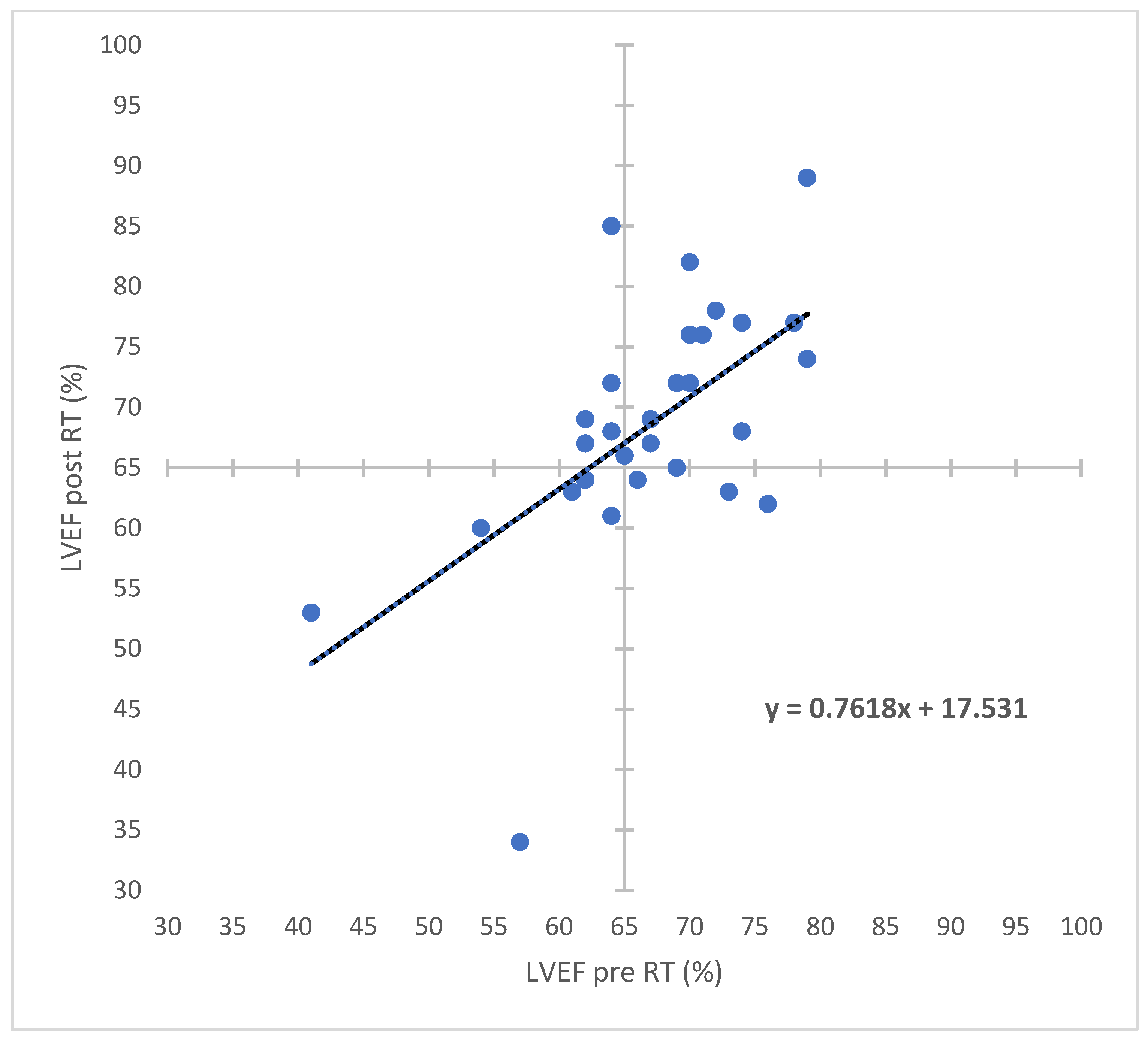
3.3. Cardiac Dose and Cardiac Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Darby, S.; McGale, P.; Correa, C.; Taylor, C. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10 801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [PubMed] [Green Version]
- McGale, P.; Correa, C.; Cutter, D.; Duane, F.; Ewertz, M.; Gray, R.; Mannu, G.; Peto, R.; Whelan, T.; Darby, S. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: Meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 2014, 383, 2127–2135. [Google Scholar] [PubMed]
- Poortmans, P.M.; Weltens, C.; Fortpied, C.; Kirkove, C.; Peignaux-Casasnovas, K.; Budach, V.; van der Leij, F.; Vonk, E.; Weidner, N.; Rivera, S. Internal mammary and medial supraclavicular lymph node chain irradiation in stage I–III breast cancer (EORTC 22922/10925): 15-year results of a randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1602–1610. [Google Scholar] [CrossRef]
- Jones, B.M.; Osborn, V.W. Postmastectomy radiation: An evolution. Ann. Breast Surg. 2021, 5, 38. [Google Scholar] [CrossRef]
- Whelan, T.J.; Olivotto, I.A.; Parulekar, W.R.; Ackerman, I.; Chua, B.H.; Nabid, A.; Vallis, K.A.; White, J.R.; Rousseau, P.; Fortin, A. Regional nodal irradiation in early-stage breast cancer. N. Engl. J. Med. 2015, 373, 307–316. [Google Scholar] [CrossRef] [Green Version]
- Correa, C.R.; Litt, H.I.; Hwang, W.-T.; Ferrari, V.A.; Solin, L.J.; Harris, E.E. Coronary artery findings after left-sided compared with right-sided radiation treatment for early-stage breast cancer. J. Clin. Oncol. 2007, 25, 3031–3037. [Google Scholar] [CrossRef]
- Harris, E.E.; Correa, C.; Hwang, W.-T.; Liao, J.; Litt, H.I.; Ferrari, V.A.; Solin, L.J. Late cardiac mortality and morbidity in early-stage breast cancer patients after breast-conservation treatment. J. Clin. Oncol. 2006, 24, 4100–4106. [Google Scholar] [CrossRef]
- Hooning, M.J.; Botma, A.; Aleman, B.M.; Baaijens, M.H.; Bartelink, H.; Klijn, J.G.; Taylor, C.W.; Van Leeuwen, F.E. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J. Natl. Cancer Inst. 2007, 99, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Jagsi, R.; Griffith, K.A.; Koelling, T.; Roberts, R.; Pierce, L.J. Rates of myocardial infarction and coronary artery disease and risk factors in patients treated with radiation therapy for early-stage breast cancer. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2007, 109, 650–657. [Google Scholar] [CrossRef] [Green Version]
- Carlson, L.E.; Watt, G.P.; Tonorezos, E.S.; Chow, E.J.; Yu, A.F.; Woods, M.; Lynch, C.F.; John, E.M.; Mellemkjær, L.; Brooks, J.D. Coronary artery disease in young women after radiation therapy for breast cancer: The WECARE Study. Cardio Oncol. 2021, 3, 381–392. [Google Scholar] [CrossRef]
- Jagsi, R.; Griffith, K.A.; Moran, J.M.; Ficaro, E.; Marsh, R.; Dess, R.T.; Chung, E.; Liss, A.L.; Hayman, J.A.; Mayo, C.S. A randomized comparison of radiation therapy techniques in the management of node-positive breast cancer: Primary outcomes analysis. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Tyran, M.; Mailleux, H.; Tallet, A.; Fau, P.; Gonzague, L.; Minsat, M.; Moureau-Zabotto, L.; Resbeut, M. Volumetric-modulated arc therapy for left-sided breast cancer and all regional nodes improves target volumes coverage and reduces treatment time and doses to the heart and left coronary artery, compared with a field-in-field technique. J. Radiat. Res. 2015, 56, 927–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popescu, C.C.; Olivotto, I.A.; Beckham, W.A.; Ansbacher, W.; Zavgorodni, S.; Shaffer, R.; Wai, E.S.; Otto, K. Volumetric modulated arc therapy improves dosimetry and reduces treatment time compared to conventional intensity-modulated radiotherapy for locoregional radiotherapy of left-sided breast cancer and internal mammary nodes. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Nobnop, W.; Phakoetsuk, P.; Chitapanarux, I.; Tippanya, D.; Khamchompoo, D. Dosimetric comparison of TomoDirect, helical tomotherapy, and volumetric modulated arc therapy for postmastectomy treatment. J. Appl. Clin. Med. Phys. 2020, 21, 155–162. [Google Scholar] [CrossRef]
- Lauche, O.; Kirova, Y.M.; Fenoglietto, P.; Costa, E.; Lemanski, C.; Bourgier, C.; Riou, O.; Tiberi, D.; Campana, F.; Fourquet, A. Helical tomotherapy and volumetric modulated arc therapy: New therapeutic arms in the breast cancer radiotherapy. World J. Radiol. 2016, 8, 735–742. [Google Scholar] [CrossRef]
- Taylor, C.; Correa, C.; Duane, F.K.; Aznar, M.C.; Anderson, S.J.; Bergh, J.; Dodwell, D.; Ewertz, M.; Gray, R.; Jagsi, R. Estimating the risks of breast cancer radiotherapy: Evidence from modern radiation doses to the lungs and heart and from previous randomized trials. J. Clin. Oncol. 2017, 35, 1641–1649. [Google Scholar] [CrossRef]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [Green Version]
- Volkova, M.; Russell, R. Anthracycline cardiotoxicity: Prevalence, pathogenesis and treatment. Curr. Cardiol. Rev. 2011, 7, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Hayek, E.R.; Speakman, E.; Rehmus, E. Acute doxorubicin cardiotoxicity. N. Engl. J. Med. 2005, 352, 2456–2457. [Google Scholar] [CrossRef]
- Dazzi, H.; Kaufmann, K.; Follath, F. Anthracycline-induced acute cardiotoxicity in adults treated for leukaemia: Analysis of the clinico-pathological aspects of documented acute anthracycline-induced cardiotoxicity in patients treated for acute leukaemia at the University Hospital of Zurich, Switzerland, between 1990 and 1996. Ann. Oncol. 2001, 12, 963–966. [Google Scholar]
- Bristow, M.R.; Thompson, P.D.; Martin, R.P.; Mason, J.W.; Billingham, M.E.; Harrison, D.C. Early anthracycline cardiotoxicity. Am. J. Med. 1978, 65, 823–832. [Google Scholar] [CrossRef]
- Keefe, D.L. Trastuzumab-associated cardiotoxicity. Cancer 2002, 95, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Dirican, A.; Levent, F.; Alacacioglu, A.; Kucukzeybek, Y.; Varol, U.; Kocabas, U.; Şenöz, O.; Emren, S.V.; Demir, L.; Coban, E. Acute cardiotoxic effects of adjuvant trastuzumab treatment and its relation to oxidative stress. Angiology 2014, 65, 944–949. [Google Scholar] [CrossRef]
- Dodwell, D.; Taylor, C.; McGale, P.; Coles, C.; Duane, F.; Gray, R.; Kühn, T.; Hennequin, C.; Oliveros, S.; Wang, Y. Abstract GS4-02: Regional lymph node irradiation in early stage breast cancer: An EBCTCG meta-analysis of 13,000 women in 14 trials. Cancer Res. 2019, 79, GS4-02. [Google Scholar]
- Ho, A.Y.; Ballangrud, A.; Li, G.; Gupta, G.P.; McCormick, B.; Gewanter, R.; Gelblum, D.; Zinovoy, M.; Mueller, B.; Mychalczak, B. Long-term pulmonary outcomes of a feasibility study of inverse-planned, multibeam intensity modulated radiation therapy in node-positive breast cancer patients receiving regional nodal irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.T.; Ward, R.; Latty, D.; Owen, C.; Gebski, V.; Chojnowski, J.; Kelly, C.; Ahern, V.; Tiver, K.; Stuart, K. Left-sided breast cancer loco-regional radiotherapy with deep inspiration breath-hold: Does volumetric-modulated arc radiotherapy reduce heart dose further compared with tangential intensity-modulated radiotherapy? J. Med. Imaging Radiat. Oncol. 2016, 60, 545–553. [Google Scholar] [CrossRef] [Green Version]
- Ko, H.; Chang, J.S.; Moon, J.Y.; Lee, W.H.; Shah, C.; Shim, J.S.A.; Han, M.C.; Baek, J.G.; Park, R.H.; Kim, Y.B. Dosimetric Comparison of Radiation Techniques for Comprehensive Regional Nodal Radiation Therapy for Left-Sided Breast Cancer: A Treatment Planning Study. Front. Oncol. 2021, 11, 645328. [Google Scholar] [CrossRef]
- Hou, P.Y.; Hsieh, C.H.; Wu, L.J.; Hsu, C.X.; Kuo, D.Y.; Lu, Y.F.; Tien, H.J.; Hsiao, H.W.; Shueng, P.W.; Hsu, S.M. Modern Rotational Radiation Techniques with Volumetric Modulated Arc Therapy or Helical Tomotherapy for Optimal Sparing of the Lung and Heart in Left-Breast Cancer Radiotherapy Plus Regional Nodal Irradiation: A Comparative Dosimetric Analysis. Cancers 2021, 13, 5043. [Google Scholar] [CrossRef]
- Tan, C.; Tasaka, H.; Yu, K.P.; Murphy, M.L.; Karnofsky, D.A. Daunomycin, an antitumor antibiotic, in the treatment of neoplastic disease. Clinical evaluation with special reference to childhood leukemia. Cancer 1967, 20, 333–353. [Google Scholar] [CrossRef]
- De Azambuja, E.; Bedard, P.L.; Suter, T.; Piccart-Gebhart, M. Cardiac toxicity with anti-HER-2 therapies-what have we learned so far? Target. Oncol. 2009, 4, 77–88. [Google Scholar] [CrossRef]
- Florido, R.; Smith, K.L.; Cuomo, K.K.; Russell, S.D. Cardiotoxicity from Human Epidermal Growth Factor Receptor-2 (HER 2) Targeted Therapies. J. Am. Heart Assoc. 2017, 6, e006915. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.P.; Sokol, S.I.; Wang, Y.; Rathore, S.S.; Ko, D.T.; Jadbabaie, F.; Portnay, E.L.; Marshalko, S.J.; Radford, M.J.; Krumholz, H.M. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J. Am. Coll. Cardiol. 2003, 42, 736–742. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angaran, P.; Dorian, P.; Ha, A.C.; Thavendiranathan, P.; Tsang, W.; Leong-Poi, H.; Woo, A.; Dias, B.; Wang, X.; Austin, P.C. Association of left ventricular ejection fraction with mortality and hospitalizations. J. Am. Soc. Echocardiogr. 2020, 33, 802–811.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, E.; Marwick, T.H. Assessment of left ventricular function by echocardiography: The case for routinely adding global longitudinal strain to ejection fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M. Prevention and monitoring of cardiac dysfunction in survivors of adult cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.; Lancellotti, P. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Bouwer, N.; Steenbruggen, T.; van Rosmalen, J.; Rier, H.; Kitzen, J.; van Bekkum, M.; Ten Tije, A.; de Jong, P.; Drooger, J.; Holterhues, C. Cardiotoxicity during long-term trastuzumab use in patients with HER2-positive metastatic breast cancer: Who needs cardiac monitoring? Breast Cancer Res. Treat. 2021, 186, 851–862. [Google Scholar] [CrossRef]
- Meattini, I.; Poortmans, P.M.; Aznar, M.C.; Becherini, C.; Bonzano, E.; Cardinale, D.; Lenihan, D.J.; Marrazzo, L.; Curigliano, G.; Livi, L. Association of breast cancer irradiation with cardiac toxic effects: A narrative review. JAMA Oncol. 2021, 7, 924–932. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Characteristics | ||
|---|---|---|---|
| Age (years) (SD) (range) | 57.5 (11) (39–80) | Smoking: N (%) | 3 (10) |
| BMI (kg/m2) (SD) (range) | 25.3 (5.24) (17.4–37.9) | Chemotherapy before RT: N (%) | 29 (96.7) |
| Baseline LVEF (%) (SD) (range) | 68 (8.17) (41–79) | Anthracycline-containing chemotherapy regimen: N (%) | 24 (80) |
| Cardiac disease: N (%) | 3 (10) | Taxane-containing chemotherapy regimen: N (%) | 21 (70) |
| Diabetes mellitus: N (%) | 9 (30) | Anti HER-2/ErbB2 target therapy: N (%) | 11 (36.7) |
| Hypertension: N (%) | 12 (40) | Aromatase inhibitor therapy: N (%) | 12 (40) |
| Dyslipidemia: N (%) | 19 (63.3) | Tamoxifen therapy: N (%) | 14 (46.7) |
| RT Treatment Factors | RT Dosimetry | Median | |
|---|---|---|---|
| VMAT: N (%) HT: N (%) | 17 (56.7) 13 (43.3) | RT total dose (Gy) (SD) (range) | 55 (5.73) (43.5–70) |
| Lumpectomy: N (%) Mastectomy: N (%) | 15 (50%) 15 (50%) | Number of fractions (SD) (range) | 30 (4.34) (15–35) |
| Conventional fractionation: N (%) Hypofractionation: N (%) | 28 (93.3%) 2 (6.7%) | Heart Volume (SD) (range) | 489.5 (115.7) (356.5–947) |
| CTV (mL) (SD) (range) | 450 (392.2) (158.5–1845.6) | Mean heart dose (Gy) (SD) (range) | 3.73 (1.9) (1.95–9.36) |
| PTV (mL) (SD) (range) | 892.9 (574.9) (402.2–2937.1) | V5 (%) | 13.5 |
| RT target volume | V10 (%) | 6.6 | |
| Breast_SCF | 9 (30%) | V15 (%) | 4.5 |
| Breast_SCF_IMN | 6 (20%) | V20 (%) | 2.25 |
| CW_SCF | 6 (20%) | V25 (%) | 1.15 |
| CW_SCF_IMN | 9 (30%) | V30 (%) | 0.5 |
| LVEF_Change | LVEF Pre-RT | LVEF Post-RT | Heart Mean Dose | Heart V5 | Heart V10 | Heart V15 | Heart V20 | Heart V25 | Heart V30 | |
|---|---|---|---|---|---|---|---|---|---|---|
| LVEF_Change | 1 | |||||||||
| LVEF pre-RT | −0.233 | 1 | ||||||||
| LVEF post-RT | 0.631 *** | 0.608 *** | 1 | |||||||
| Heart Mean | −0.125 | 0.009 | −0.095 | 1 | ||||||
| Heart V5 | −0.135 | 0.014 | −0.099 | 0.942 *** | 1 | |||||
| Heart V10 | −0.171 | −0.092 | −0.213 | 0.963 *** | 0.917 *** | 1 | ||||
| Heart V15 | −0.175 | −0.109 | −0.230 | 0.915 *** | 0.773 *** | 0.949 *** | 1 | |||
| Heart V20 | −0.174 | −0.068 | −0.197 | 0.859 *** | 0.670 *** | 0.878 *** | 0.977 *** | 1 | ||
| Heart V25 | −0.114 | −0.023 | −0.111 | 0.763 *** | 0.541 ** | 0.770 *** | 0.909 *** | 0.962 *** | 1 | |
| Heart V30 | −0.059 | −0.017 | −0.062 | 0.658 *** | 0.425 * | 0.626 *** | 0.781 *** | 0.862 *** | 0.938 *** | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, P.-Y.; Hsieh, C.-H.; Wu, L.-J.; Hsu, C.-X.; Kuo, D.-Y.; Lu, Y.-F.; Wu, Y.-W.; Tien, H.-J.; Hsu, S.-M.; Shueng, P.-W. Cardiac Function after Modern Radiation Therapy with Volumetric Modulated Arc Therapy or Helical Tomotherapy for Advanced Left-Breast Cancer Receiving Regional Nodal Irradiation. Bioengineering 2022, 9, 213. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050213
Hou P-Y, Hsieh C-H, Wu L-J, Hsu C-X, Kuo D-Y, Lu Y-F, Wu Y-W, Tien H-J, Hsu S-M, Shueng P-W. Cardiac Function after Modern Radiation Therapy with Volumetric Modulated Arc Therapy or Helical Tomotherapy for Advanced Left-Breast Cancer Receiving Regional Nodal Irradiation. Bioengineering. 2022; 9(5):213. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050213
Chicago/Turabian StyleHou, Pei-Yu, Chen-Hsi Hsieh, Le-Jung Wu, Chen-Xiong Hsu, Deng-Yu Kuo, Yueh-Feng Lu, Yen-Wen Wu, Hui-Ju Tien, Shih-Ming Hsu, and Pei-Wei Shueng. 2022. "Cardiac Function after Modern Radiation Therapy with Volumetric Modulated Arc Therapy or Helical Tomotherapy for Advanced Left-Breast Cancer Receiving Regional Nodal Irradiation" Bioengineering 9, no. 5: 213. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050213