
Testosterone Levels in Adolescents and Young Men with Type 1 Diabetes and Their Association with Diabetic Nephropathy

 ,
,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
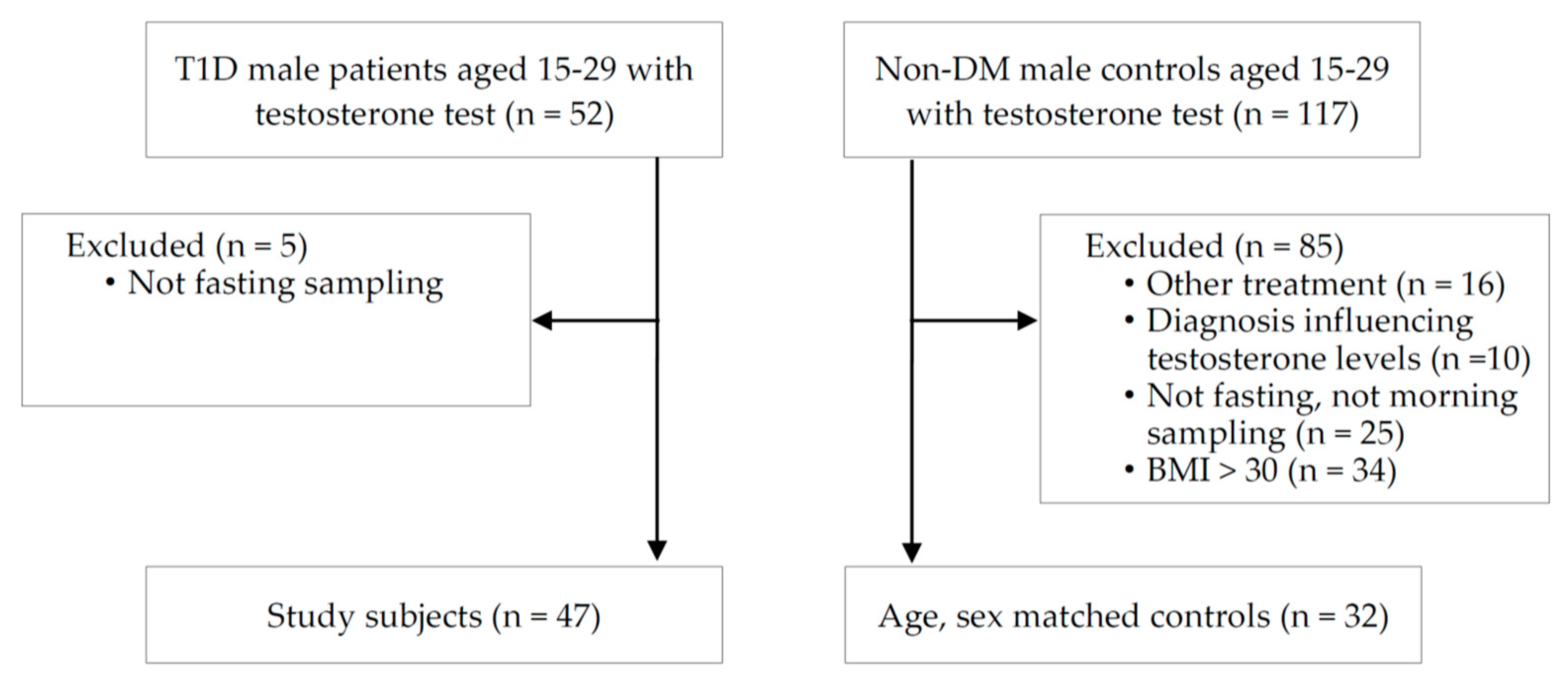
2.1. Participants
2.2. Laboratory Measurements
2.3. Statistical Analyses
2.4. Ethics Statement
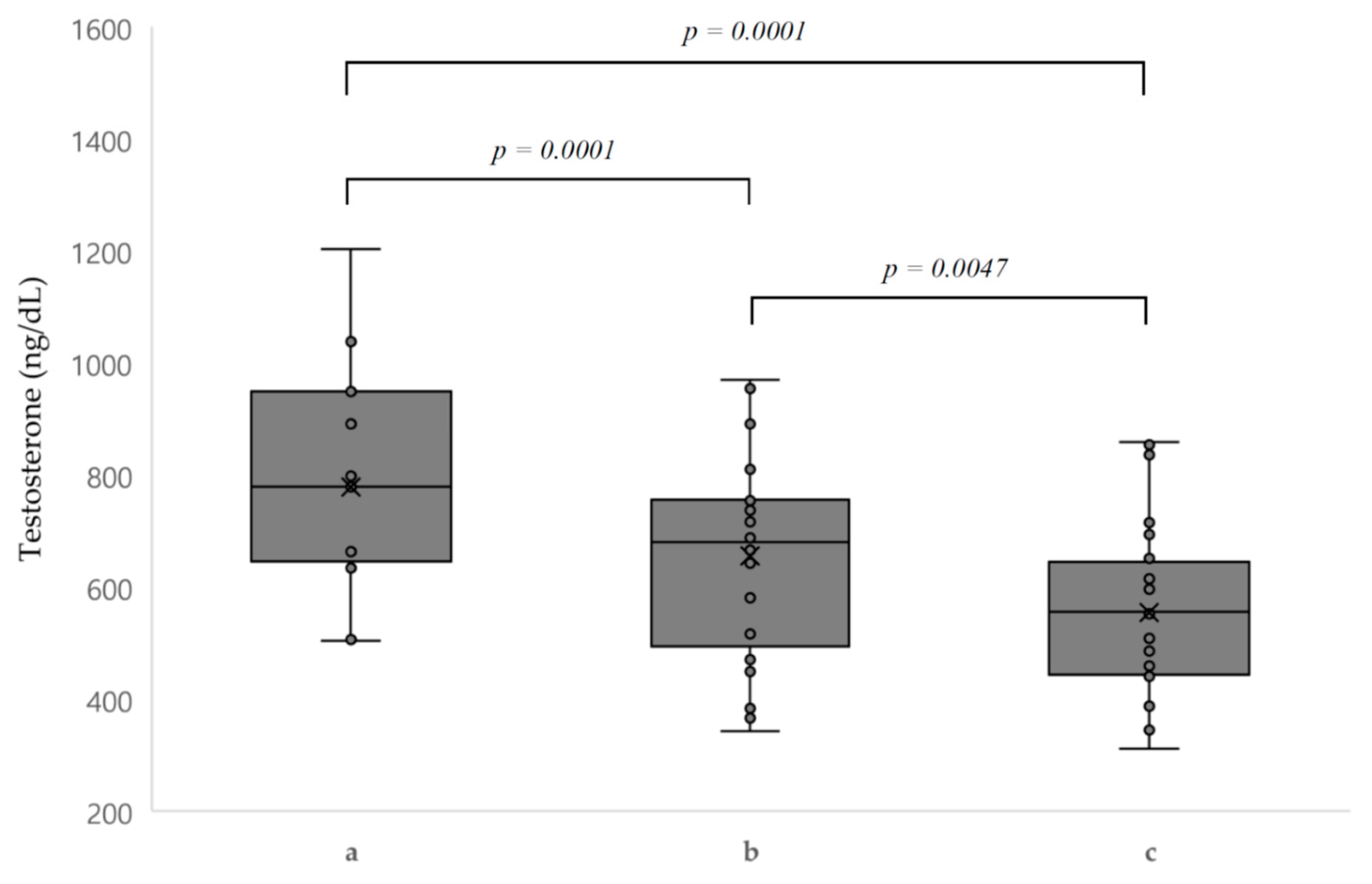
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Corona, G.; Monami, M.; Rastrelli, G.; Aversa, A.; Sforza, A.; Lenzi, A.; Forti, G.; Mannucci, E.; Maggi, M. Type 2 diabetes mellitus and testosterone: A meta-analysis study. Int. J. Androl. 2011, 34, 528–540. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.J. Diagnosis and management of endocrine impotence. Br. Med. J. 1972, 2, 34–36. [Google Scholar] [CrossRef] [Green Version]
- Schoeller, E.L.; Schon, S.; Moley, K.H. The effects of type 1 diabetes on the hypothalamic, pituitary and testes axis. Cell Tissue Res. 2012, 349, 839–847. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Lee, J. Role of obesity-induced inflammation in the development of insulin resistance and type 2 diabetes: History of the research and remaining questions. Ann. Pediatr. Endocrinol. Metab. 2021, 26, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kelsey, M.M.; Bjornstad, P.; McFann, K.; Nadeau, K. Testosterone concentration and insulin sensitivity in young men with type 1 and type 2 diabetes. Pediatr. Diabetes 2016, 17, 184–190. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Nieschlag, E.; Swerdloff, R.; Behre, H.M.; Hellstrom, W.J.; Gooren, L.J.; Kaufman, J.M.; Legros, J.J.; Lunenfeld, B.; Morales, A.; et al. Investigation, treatment and monitoring of late-onset hypogonadism in males: Isa, issam, eau, eaa and asa recommendations. Eur. J. Endocrinol. 2008, 159, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzola, M.; Bozzola, E.; Montalbano, C.; Stamati, F.A.; Ferrara, P.; Villani, A. Delayed puberty versus hypogonadism: A challenge for the pediatrician. Ann. Pediatr. Endocrinol. Metab. 2018, 23, 57–61. [Google Scholar] [CrossRef]
- Zitzmann, M.; Faber, S.; Nieschlag, E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J. Clin. Endocrinol. Metab. 2006, 91, 4335–4343. [Google Scholar] [CrossRef]
- Selvin, E.; Feinleib, M.; Zhang, L.; Rohrmann, S.; Rifai, N.; Nelson, W.G.; Dobs, A.; Basaria, S.; Golden, S.H.; Platz, E.A. Androgens and diabetes in men. Diabetes Care 2007, 30, 234. [Google Scholar] [CrossRef] [Green Version]
- Corona, G.; Mannucci, E.; Forti, G.; Maggi, M. Following the common association between testosterone deficiency and diabetes mellitus, can testosterone be regarded as a new therapy for diabetes? Int. J. Androl. 2009, 32, 431–441. [Google Scholar] [CrossRef]
- Corona, G.; Mannucci, E.; Forti, G.; Maggi, M. Hypogonadism, ed, metabolic syndrome and obesity: A pathological link supporting cardiovascular diseases. Int. J. Androl. 2009, 32, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Danielson, K.K.; Drum, M.L.; Lipton, R.B. Sex hormone-binding globulin and testosterone in individuals with childhood diabetes. Diabetes Care 2008, 31, 1207–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrer, T.; Stierkorb, E.; Heger, S.; Karges, B.; Raile, K.; Schwab, K.O.; Holl, R.W. Delayed pubertal onset and development in german children and adolescents with type 1 diabetes: Cross-sectional analysis of recent data from the dpv diabetes documentation and quality management system. Eur. J. Endocrinol. 2007, 157, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson, J.; Ekström, L.; Inotsume, N.; Garle, M.; Lorentzon, M.; Ohlsson, C.; Roh, H.-K.; Carlström, K.; Rane, A. Large differences in testosterone excretion in korean and swedish men are strongly associated with a udp-glucuronosyl transferase 2b17 polymorphism. J. Clin. Endocrinol. Metab. 2006, 91, 687–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesper, H.W.; Wang, Y.; Vidal, M.; Botelho, J.C.; Caudill, S.P. Serum total testosterone concentrations in the us household population from the nhanes 2011-2012 study population. Clin. Chem. 2015, 61, 1495–1504. [Google Scholar] [CrossRef] [Green Version]
- ADA. 11. Microvascular complications and foot care: Standards of medical care in diabetes—2019. Diabetes Care 2019, 42, S124. [Google Scholar] [CrossRef] [Green Version]
- Moriarty-Kelsey, M.; Harwood, J.E.; Travers, S.H.; Zeitler, P.S.; Nadeau, K.J. Testosterone, obesity and insulin resistance in young males: Evidence for an association between gonadal dysfunction and insulin resistance during puberty. J. Pediatr. Endocrinol. Metab. 2010, 23, 1281–1287. [Google Scholar] [CrossRef]
- Minooee, S.; Ramezani Tehrani, F.; Rahmati, M.; Amanollahi Soudmand, S.; Tohidi, M.; Sabet, Z.; Azizi, F. The association between serum total testosterone and progression of hyperglycemia: A 15-year prospective cohort study. Andrology 2019, 7, 148–155. [Google Scholar] [CrossRef]
- D’Souza, A.M.; Neumann, U.H.; Glavas, M.M.; Kieffer, T.J. The glucoregulatory actions of leptin. Mol. Metab. 2017, 6, 1052–1065. [Google Scholar] [CrossRef]
- Kaplowitz, P. Delayed puberty in obese boys: Comparison with constitutional delayed puberty and response to testosterone therapy. J. Pediatr. 1998, 133, 745–749. [Google Scholar] [CrossRef]
- Shin, J.H.; Cheong, J.I.; Cheuh, H.W.; Yoo, J.-H. Limitations of current screening methods for lipid disorders in korean adolescents and a proposal for an effective detection method: A nationwide, cross-sectional study. Ann. Pediatr. Endocrinol. Metab. 2020, 25, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Hylmarova, S.; Stechova, K.; Pavlinkova, G.; Peknicova, J.; Macek, M.; Kvapil, M. The impact of type 1 diabetes mellitus on male sexual functions and sex hormone levels. Endocr. J. 2020, 67, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.K.; Lopushnyan, N.; Hotaling, J.; Sarma, A.V.; Dunn, R.L.; Cleary, P.A.; Braffett, B.H.; Gatcomb, P.; Martin, C.; Herman, W.H.; et al. Prevalence of low testosterone and predisposing risk factors in men with type 1 diabetes mellitus: Findings from the dcct/edic. J. Clin. Endocrinol. Metab. 2014, 99, E1655–E1660. [Google Scholar] [CrossRef]
- Gaete, X.; Vivanco, M.; Lopez, P.; Rocha, A.; Sepúlveda, C.; Codner, E. Earlier puberty in boys with type 1 diabetes mellitus compared to a simultaneously recruited group of control adolescents. Pediatr. Diabetes 2019, 20, 197–201. [Google Scholar] [CrossRef]
- Condorelli, R.A.; La Vignera, S.; Mongioi, L.M.; Alamo, A.; Calogero, A.E. Diabetes mellitus and infertility: Different pathophysiological effects in type 1 and type 2 on sperm function. Front. Endocrinol. 2018, 9, 268. [Google Scholar] [CrossRef] [Green Version]
- Giménez, M.; Aguilera, E.; Castell, C.; de Lara, N.; Nicolau, J.; Conget, I. Relationship between bmi and age at diagnosis of type 1 diabetes in a mediterranean area in the period of 1990–2004. Diabetes Care 2007, 30, 1593–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandel, A.; Dhindsa, S.; Topiwala, S.; Chaudhuri, A.; Dandona, P. Testosterone concentration in young patients with diabetes. Diabetes Care 2008, 31, 2013–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.-Y.; Yu, X.; Lee, Y.; McCorkle, S.K.; Clark, G.O.; Strowig, S.; Unger, R.H.; Raskin, P. Iatrogenic hyperinsulinemia in type 1 diabetes: Its effect on atherogenic risk markers. J. Diabetes Complicat. 2013, 27, 70–74. [Google Scholar] [CrossRef]
- Wagner, I.V.; Oliver, E.; Dötsch, J.; Söder, O. Adverse effects of metabolic disorders in childhood on adult reproductive function and fertility in the male. J. Pediatr. Endocrinol. Metab. 2020. [Google Scholar] [CrossRef]
- Hart, R.; Doherty, D.; Mori, T.; Adams, L.; Huang, R.; Minaee, N.; Handelsman, D.; McLachlan, R.; Norman, R.; Dickinson, J.; et al. Features of the metabolic syndrome in late adolescence are associated with impaired testicular function at 20 years of age. Hum. Reprod. 2019, 34, 389–402. [Google Scholar] [CrossRef] [Green Version]
- Chillarón, J.J.; Fernández-Miró, M.; Albareda, M.; Vila, L.; Colom, C.; Fontserè, S.; Pedro-Botet, J.; Flores-Le Roux, J.A. Age, insulin requirements, waist circumference, and triglycerides predict hypogonadotropic hypogonadism in patients with type 1 diabetes. J. Sex. Med. 2015, 12, 76–82. [Google Scholar] [CrossRef]
- Williamson, J.R.; Rowold, E.; Chang, K.; Marvel, J.; Tomlinson, M.; Sherman, W.R.; Ackermann, K.E.; Berger, R.A.; Kilo, C. Sex steroid dependency of diabetes-induced changes in polyol metabolism, vascular permeability, and collagen cross-linking. Diabetes 1986, 35, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.; Schultz, C.; Ong, K.; Frystyk, J.; Dalton, R.N.; Perry, L.; Orskov, H.; Dunger, D.B. Low igf-i and elevated testosterone during puberty in subjects with type 1 diabetes developing microalbuminuria in comparison to normoalbuminuric control subjects: The oxford regional prospective study. Diabetes Care 2003, 26, 1456–1461. [Google Scholar] [CrossRef] [Green Version]
- Schultz, C.J.; Konopelska-Bahu, T.; Dalton, R.N.; Carroll, T.A.; Stratton, I.; Gale, E.A.; Neil, A.; Dunger, D.B. Microalbuminuria prevalence varies with age, sex, and puberty in children with type 1 diabetes followed from diagnosis in a longitudinal study. Oxford regional prospective study group. Diabetes Care 1999, 22, 495–502. [Google Scholar] [CrossRef]
- Doublier, S.; Lupia, E.; Catanuto, P.; Periera-Simon, S.; Xia, X.; Korach, K.; Berho, M.; Elliot, S.J.; Karl, M. Testosterone and 17beta-estradiol have opposite effects on podocyte apoptosis that precedes glomerulosclerosis in female estrogen receptor knockout mice. Kidney Int. 2011, 79, 404–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esmeijer, K.; Dekkers, O.M.; de Fijter, J.W.; Dekker, F.W.; Hoogeveen, E.K. Effect of different types of statins on kidney function decline and proteinuria: A network meta-analysis. Sci. Rep. 2019, 9, 16632. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| T1D (N = 47) | Control Group (N = 32) | p-Value | |
|---|---|---|---|
| Age (year) | 20.2 ± 4.4 | 19.6 ± 2.9 | 0.486 |
| Disease duration (year) | 11.3 ± 4.3 | - | - |
| Height (cm) | 172.7 ± 5.3 | 170.4 ± 8.7 | 0.288 |
| Weight (kg) | 63.9 ± 8.8 | 65.4 ± 10.2 | 0.563 |
| BMI (kg/m2) | 21.3 ± 2.4 | 22.9 ± 3.2 | 0.064 |
| Testosterone (ng/dL) | 694.6 ± 182.2 | 554.1 ± 147.4 | 0.001 |
| FSH (IU/L) | 3.6 ± 1.4 | 4.0 ± 2.1 | 0.427 |
| LH (IU/L) | 3.9 ± 1.3 | 3.8 ± 1.3 | 0.723 |
| Total cholesterol (mg/dL) | 147.7 ± 26.6 | 168.4 ± 32.5 | 0.003 |
| LDL cholesterol (mg/dL) | 91.6 ± 25.7 | 104.0 ± 31.2 | 0.064 |
| Triglycerides (mg/dL) | 81.8 ± 56.8 | 91.6 ± 40.7 | 0.422 |
| Glucose (mg/dL) | 156.8 ± 38.1 | 88.8 ± 12.5 | 0.001 |
| BUN (mg/dL) | 12.7 ± 3.1 | 11.2 ± 3.3 | 0.053 |
| Serum creatinine (mg/dL) | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.607 |
| HbA1c at diagnosis (%) | 12.0 ± 4.4 | - | - |
| Average HbA1c (%) | 7.9 ± 1.2 | - | - |
| C-peptide (ng/mL) | 0.5 ± 0.2 | - | - |
| 24-h urine albumin (mg/day) | 23.2 ± 22.8 | - | - |
| Spot urine ACR (mg/g) | 18.6 ± 39.6 | - | - |
| Variable | Testosterone | Nephropathy | ||
|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Age (year) | 0.208 | 0.162 | 0.309 | 0.035 |
| Disease duration (year) | 0.118 | 0.429 | 0.353 | 0.015 |
| BMI (kg/m2) | −0.184 | 0.238 | 0.225 | 0.146 |
| Total cholesterol (mg/dL) | 0.105 | 0.501 | 0.187 | 0.229 |
| LDL cholesterol (mg/dL) | 0.203 | 0.191 | 0.174 | 0.264 |
| Triglycerides (mg/dL) | −0.069 | 0.658 | 0.046 | 0.769 |
| BUN (mg/dL) | 0.055 | 0.713 | 0.026 | 0.865 |
| Serum creatinine (mg/dL) | −0.048 | 0.755 | −0.106 | 0.494 |
| HbA1c (%) | −0.040 | 0.787 | −0.064 | 0.669 |
| HbA1c at diagnosis (%) | 0.075 | 0.623 | 0.048 | 0.755 |
| Average HbA1c (%) | −0.121 | 0.416 | −0.073 | 0.624 |
| C-peptide (ng/mL) | 0.130 | 0.385 | −0.042 | 0.780 |
| Insulin dose (unit/kg/day) | −0.229 | 0.121 | −0.213 | 0.151 |
| 24-h urine albumin (mg/day) | 0.415 | 0.004 | 0.802 | 0.001 |
| Spot urine ACR (mg/g) | 0.402 | 0.005 | 0.342 | 0.018 |
| Testosterone (ng/dL) | - | - | 0.318 | 0.029 |
| Parameter | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| β ± SE | p-Value | β ± SE | p-Value | β ± SE | p-Value | β ± SE | p-Value | |
| Age | - | - | 6.4 ± 6.6 | 0.340 | 15.0 ± 6.6 | 0.030 | - | - |
| Nephropathy | 94.9 ± 55.2 | 0.093 | 74.9 ± 58.9 | 0.208 | 77.5 ± 55.2 | 0.169 | 115.1 ± 55.7 | 0.046 |
| BMI (kg/m2) | - | - | - | - | −37.7 ± 11.9 | 0.003 | −31.2 ± 12.2 | 0.015 |
| LDL cholesterol (mg/dL) | 1.1 ± 1.0 | 0.289 | 0.9 ± 1.0 | 0.143 | 0.9 ± 1.0 | 0.147 | 1.4 ± 1.0 | 0.020 |
| Average HbA1c (%) | −7.7 ± 22.0 | 0.727 | −9.4 ± 22.1 | 0.674 | −48.5 ± 24.7 | 0.058 | −40.1 ± 25.8 | 0.129 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, J.; Choi, H.S.; Choi, Y.H.; Oh, J.S.; Song, K.; Suh, J.; Kwon, A.; Kim, H.-S.; Chae, H.W. Testosterone Levels in Adolescents and Young Men with Type 1 Diabetes and Their Association with Diabetic Nephropathy. Biology 2021, 10, 615. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10070615
Kang J, Choi HS, Choi YH, Oh JS, Song K, Suh J, Kwon A, Kim H-S, Chae HW. Testosterone Levels in Adolescents and Young Men with Type 1 Diabetes and Their Association with Diabetic Nephropathy. Biology. 2021; 10(7):615. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10070615
Chicago/Turabian StyleKang, Jeongwoo, Han Saem Choi, Young Ha Choi, Jun Suk Oh, Kyungchul Song, Junghwan Suh, Ahreum Kwon, Ho-Seong Kim, and Hyun Wook Chae. 2021. "Testosterone Levels in Adolescents and Young Men with Type 1 Diabetes and Their Association with Diabetic Nephropathy" Biology 10, no. 7: 615. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10070615