
Clinical Relevance of the Microbiome in Odontogenic Abscesses

 , , ,
, , ,  , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
- Which bacteria can be detected that may not entirely or partially be detected by cultural methods alone?
- Is it possible to improve the accuracy and completeness of the established cultural methods with such additional diagnostics?
- Do biomolecular pathogen diagnostics offer advantages in comparison to classical culture?
2. Materials and Methods
3. Results
4. Discussion
4.1. Does Culture Provide the Identification of the “Culprit Pathogen”?
- Careful disinfection of the skin (or mucosa) at the incision site: in this way, contamination by Staphylococci from the skin can be prevented [29].
- Swabbing the depth of the abscess cavity instead of the flowing pus on the skin surface of the incision site: Pus itself represents a hostile medium for bacteria. Swabbing the living tissue at the depth of the abscess may increase the likelihood of obtaining living anaerobes for culturing while decreasing the likelihood of contamination by skin flora.
- Selection of a suitable transport medium: Liquid-based media with a flocked swab can be a better alternative compared to gel-based media with traditional fiber swabs [30]. These media probably allow sufficient survival of the anaerobes and, at the same time, still enable further processing by molecular biological methods [31,32].
4.2. Is Swab Collection Necessary at All?
4.3. Does Antibiotic Resistance Have Clinical Relevance in Odontogenic Infections?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flynn, T.R. The swollen face. Severe odontogenic infections. Emerg. Med. Clin. N. Am. 2000, 18, 481–519. [Google Scholar] [CrossRef]
- Connors, W.J.; Rabie, H.H.; Figueiredo, R.L.; Holton, D.L.; Parkins, M.D. Acute dental infections managed in an outpatient parenteral antibiotic program setting: Prospective analysis and public health implications. BMC Infect. Dis. 2017, 17, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, T.R.; Shanti, R.M.; Hayes, C. Severe Odontogenic Infections, Part 2: Prospective Outcomes Study. J. Oral Maxillofac. Surg. 2006, 64, 1104–1113. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawas, B.; Maeurer, M. Severe versus Local Odontogenic Bacterial Infections: Comparison of Microbial Isolates. Eur. Surg. Res. 2007, 40, 220–224. [Google Scholar] [CrossRef]
- Bertossi, D.; Barone, A.; Iurlaro, A.; Marconcini, S.; De Santis, D.; Finotti, M.; Procacci, P. Odontogenic Orofacial Infections. J. Craniofac. Surg. 2017, 28, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böttger, S.; Lautenbacher, K.; Domann, E.; Howaldt, H.-P.; Attia, S.; Streckbein, P.; Wilbrand, J.-F. Indication for an additional postoperative antibiotic treatment after surgical incision of serious odontogenic abscesses. J. Cranio-Maxillofac. Surg. 2020, 48, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Eckert, A.W.; Höhne, C.; Schubert, J. Erregerspektrum und Resistenzsituation bei rein anaeroben odontogenen Infektionen. Mund Kiefer Gesichtschirurgie 2000, 4, 153–158. [Google Scholar] [CrossRef]
- Rasmussen, B.A.; Bush, K.; Tally, F.B. Antimicrobial Resistance in Anaerobes. Clin. Infect. Dis. 1997, 24, S110–S120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimdahl, A.; von Konow, L.; Satoh, T.; Nord, C.E. Clinical appearance of orofacial infections of odontogenic origin in relation to microbiological findings. J. Clin. Microbiol. 1985, 22, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Celakovsky, P.; Kalfert, D.; Smatanova, K.; Tuček, L.; Čermáková, E.; Mejzlik, J.; Kotulek, M.; Vrbacky, A.; Matoušek, P.; Stanikova, L.; et al. Bacteriology of deep neck infections: Analysis of 634 patients. Aust. Dent. J. 2015, 60, 212–215. [Google Scholar] [CrossRef] [Green Version]
- Wiese, K.G.; Merten, H.A.; Wiltfang, J.; Luhr, H.G. Klinische Untersuchungen zur Pathophysiologie dentogen bedingter Abszesse. Mund Kiefer Gesichtschirurgie 1999, 3, 242–246. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Rôças, I.N. Microbiology and Treatment of Acute Apical Abscesses. Clin. Microbiol. Rev. 2013, 26, 255–273. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, J.F.; Rôças, I.N. The Oral Microbiota in Health and Disease: An Overview of Molecular Findings. Methods Mol. Biol. 2016, 1537, 127–138. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rôças, I.N. As-yet-uncultivated oral bacteria: Breadth and association with oral and extra-oral diseases. J. Oral Microbiol. 2013, 5. [Google Scholar] [CrossRef]
- Chen, T.; Yu, W.-H.; Izard, J.; Baranova, O.V.; Lakshmanan, A.; Dewhirst, F.E. The Human Oral Microbiome Database: A web accessible resource for investigating oral microbe taxonomic and genomic information. Database 2010, 2010, baq013. [Google Scholar] [CrossRef]
- Brook, I.; Wexler, H.M.; Goldstein, E.J.C. Antianaerobic Antimicrobials: Spectrum and Susceptibility Testing. Clin. Microbiol. Rev. 2013, 26, 526–546. [Google Scholar] [CrossRef] [Green Version]
- Böttger, S.; Zechel-Gran, S.; Schmermund, D.; Streckbein, P.; Wilbrand, J.-F.; Knitschke, M.; Pons-Kühnemann, J.; Hain, T.; Weigel, M.; Howaldt, H.-P.; et al. Microbiome of Odontogenic Abscesses. Microorganisms 2021, 9, 1307. [Google Scholar] [CrossRef]
- Keller, P.M.; Hombach, M.; Bloemberg, G.V. 16S-rRNA-Gen-basierte Identifikation bakterieller Infektionen. Biospektrum Mag. Biowiss. 2010, 16, 755–758. [Google Scholar]
- Voelkerding, K.V.; Dames, S.A.; Durtschi, J.D. Next-Generation Sequencing: From Basic Research to Diagnostics. Clin. Chem. 2009, 55, 641–658. [Google Scholar] [CrossRef] [Green Version]
- Böttger, S.; Zechel-Gran, S.; Streckbein, P.; Knitschke, M.; Hain, T.; Weigel, M.; Wilbrand, J.-F.; Domann, E.; Howaldt, H.-P.; Attia, S. A New Type of Chronic Wound Infection after Wisdom Tooth Extraction: A Diagnostic Approach with 16S-rRNA Gene Analysis, Next-Generation Sequencing, and Bioinformatics. Pathogens 2020, 9, 798. [Google Scholar] [CrossRef]
- Woo, P.C.Y.; Lau, S.K.P.; Teng, J.L.L.; Tse, H.; Yuen, K.-Y. Then and now: Use of 16S rDNA gene sequencing for bacterial identification and discovery of novel bacteria in clinical microbiology laboratories. Clin. Microbiol. Infect. 2008, 14, 908–934. [Google Scholar] [CrossRef] [Green Version]
- Regier, Y.; Komma, K.; Weigel, M.; Kraiczy, P.; Laisi, A.; Pulliainen, A.T.; Hain, T.; Kempf, V.A.J. Combination of microbiome analysis and serodiagnostics to assess the risk of pathogen transmission by ticks to humans and animals in central Germany. Parasites Vectors 2019, 12, 11. [Google Scholar] [CrossRef]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2012, 41, D590–D596. [Google Scholar] [CrossRef]
- Bahl, R.; Sandhu, S.; Sahai, N.; Gupta, M.; Singh, K. Odontogenic infections: Microbiology and management. Contemp. Clin. Dent. 2014, 5, 307–311. [Google Scholar] [CrossRef]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawas, B.; Karbach, J. S3-Leitlinie (Langversion): Odontogene Infektionen. In Leitlinien Zahnmedizin; Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften: Berlin, Germany, 2016; Available online: www.awmf.org (accessed on 10 March 2020).
- Rôças, I.; Siqueira, J. Culture-Independent Detection of Eikenella corrodens and Veillonella parvula in Primary Endodontic Infections. J. Endod. 2006, 32, 509–512. [Google Scholar] [CrossRef]
- Dargère, S.; Cormier, H.; Verdon, R. Contaminants in blood cultures: Importance, implications, interpretation and prevention. Clin. Microbiol. Infect. 2018, 24, 964–969. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gilligan, P.H.; Gonzalez, M.D.; Jerris, R.C.; Kehl, S.C.; Patel, R.; et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiologya. Clin. Infect. Dis. 2018, 67, e1–e94. [Google Scholar] [CrossRef]
- Demuyser, T.; De Geyter, D.; Van Dorpe, D.; Vandoorslaer, K.; Wybo, I. Extensive evaluation of fastidious anaerobic bacteria recovery from the Copan eSwab® transport system. J. Microbiol. Methods 2018, 144, 73–78. [Google Scholar] [CrossRef]
- Van Horn, K.G.; Audette, C.D.; Sebeck, D.; Tucker, K.A. Comparison of the Copan ESwab System with Two Amies Agar Swab Transport Systems for Maintenance of Microorganism Viability. J. Clin. Microbiol. 2008, 46, 1655–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, A.W.; Maurer, P.; Wilhelms, D.; Schubert, J. Weichteilinfektionen in der Mund-, Kiefer- und Plastischen Gesichtschirurgie. Mund Kiefer Gesichtschirurgie 2005, 9, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, A.N. Antimicrobial Resistance and Susceptibility Testing of Anaerobic Bacteria. Clin. Infect. Dis. 2014, 59, 698–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wybo, I.; Bossche, D.V.D.; Soetens, O.; Vekens, E.; Vandoorslaer, K.; Claeys, G.; Glupczynski, Y.; Ieven, M.; Melin, P.; Nonhoff, C.; et al. Fourth Belgian multicentre survey of antibiotic susceptibility of anaerobic bacteria. J. Antimicrob. Chemother. 2013, 69, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Brescó-Salinas, M.; Costa-Riu, N.; Berini-Aytés, L.; Gay-Escoda, C. Antibiotic susceptibility of the bacteria causing odontogenic infections. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, E70–E75. [Google Scholar]
- Heim, N.; Faron, A.; Wiedemeyer, V.; Reich, R.; Martini, M. Microbiology and antibiotic sensitivity of head and neck space infections of odontogenic origin. Differences in inpatient and outpatient management. J. Cranio-Maxillofac. Surg. 2017, 45, 1731–1735. [Google Scholar] [CrossRef]
- Sobottka, I.; Cachovan, G.; Stürenburg, E.; Ahlers, M.O.; Laufs, R.; Platzer, U.; Mack, D. In Vitro Activity of Moxifloxacin against Bacteria Isolated from Odontogenic Abscesses. Antimicrob. Agents Chemother. 2002, 46, 4019–4021. [Google Scholar] [CrossRef] [Green Version]
- Warnke, P.H.; Becker, S.T.; Springer, I.N.; Haerle, F.; Ullmann, U.; Russo, P.A.; Wiltfang, J.; Fickenscher, H.; Schubert, S. Penicillin compared with other advanced broad spectrum antibiotics regarding antibacterial activity against oral pathogens isolated from odontogenic abscesses. J. Cranio-Maxillofac. Surg. 2008, 36, 462–467. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
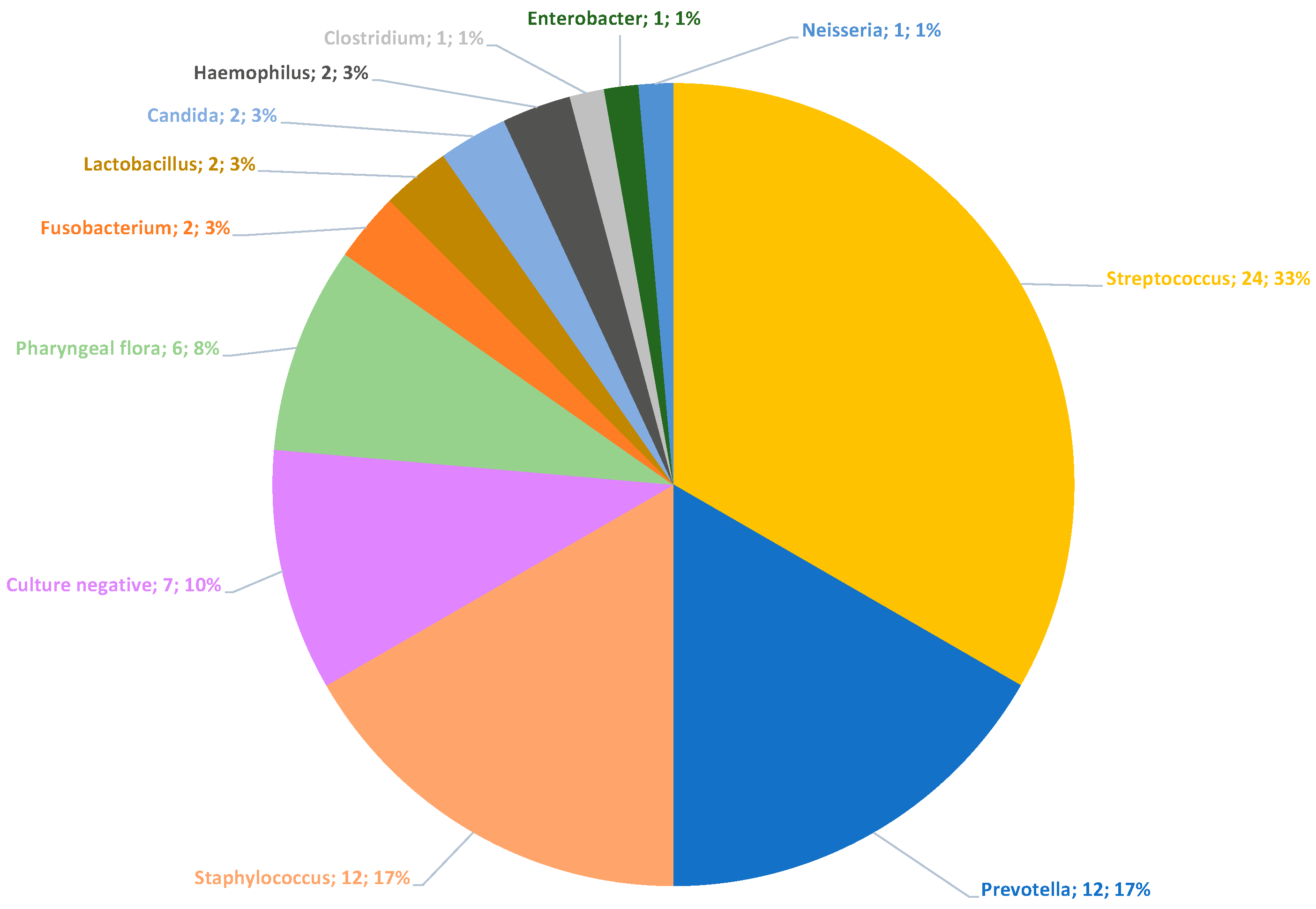
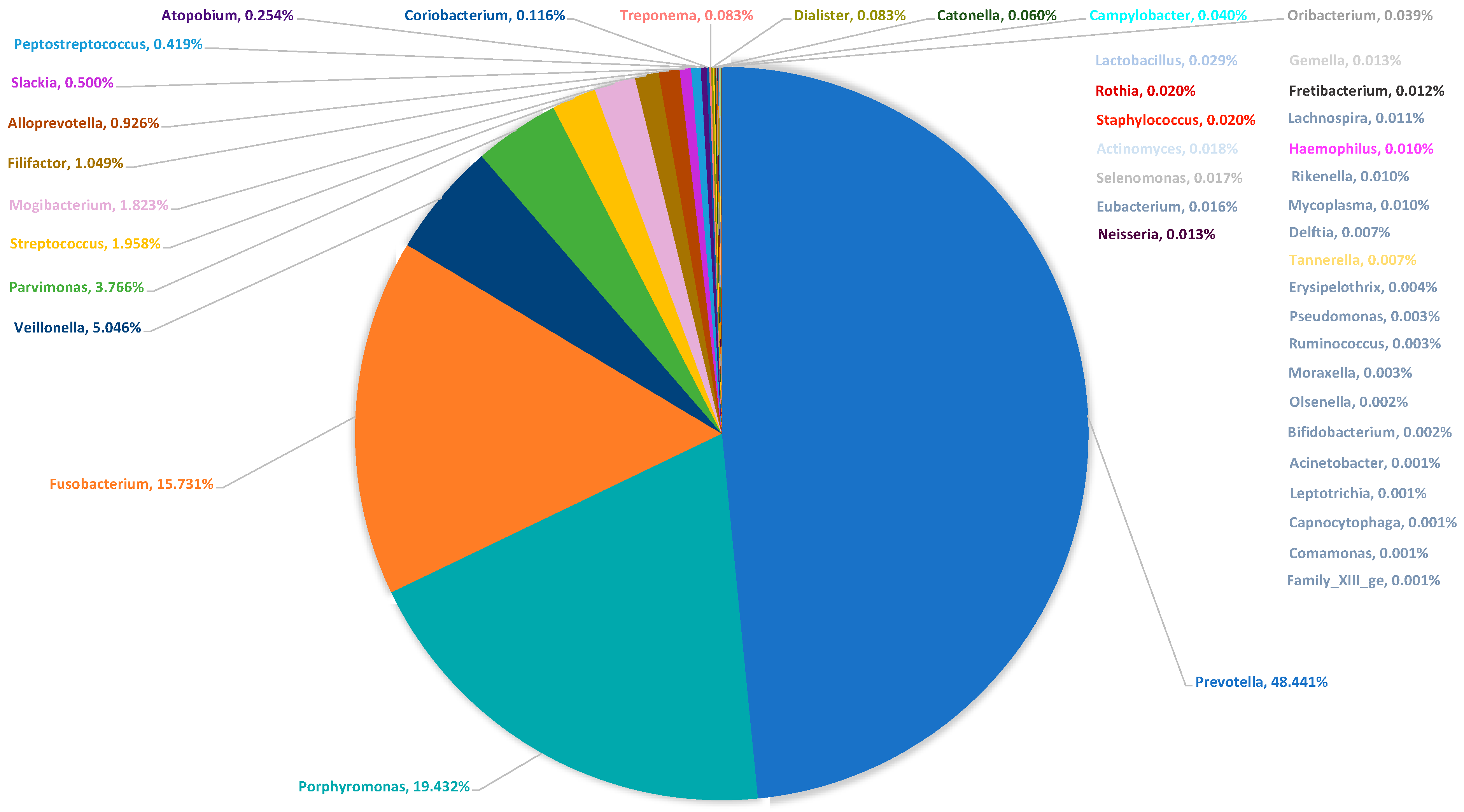
| Culture | Culture (%) | Microbiome | Microbiome (%) | |
|---|---|---|---|---|
| Prevotella | 12 | 21.43 | 45 | 39.82 |
| Fusobacterium | 2 | 3.57 | 25 | 22.12 |
| Streptococcus | 24 | 42.86 | 35 | 30.97 |
| Neisseria | 1 | 1.79 | 1 | 0.89 |
| Haemophilus | 2 | 3.57 | 3 | 2.66 |
| Staphylococcus | 12 | 21.43 | 2 | 1.77 |
| Clostridium | 1 | 1.79 | 0 | 0.00 |
| Lactobacillus | 2 | 3.57 | 2 | 1.77 |
| 56 | 100 | 113 | 100 |
| Streptococcus | Staphylococcus | Prevotella | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Penicillin | 2 | / | 17 | 11.76% | 11 | / | 14 | 78.57% | ||||
| Ampicillin/Sulbactam | 1 | / | 14 | 7.14% | 0 | / | 14 | 0.00% | ||||
| Clindamycin | 3 | / | 16 | 18.75% | 1 | / | 3 | 33.33% | 6 | / | 14 | 42.86% |
| Metronidazol | 2 | / | 2 | 100.00% | 0 | / | 14 | 0.00% | ||||
| Piperacillin/Tazobactam | 1 | / | 11 | 9.09% | 0 | / | 14 | 0.00% | ||||
| Meropenem | 0 | / | 8 | 0.00% | 0 | / | 13 | 0.00% | ||||
| Vancomycin | 0 | / | 16 | 0.00% | 0 | / | 3 | 0.00% | 12 | / | 12 | 100.00% |
| Levofloxacin | 0 | / | 11 | 0.00% | 0 | / | 1 | 0.00% | 0 | / | 1 | 0.00% |
| Cotrimoxacol | 0 | / | 3 | 0.00% | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böttger, S.; Zechel-Gran, S.; Schmermund, D.; Streckbein, P.; Wilbrand, J.-F.; Knitschke, M.; Pons-Kühnemann, J.; Hain, T.; Weigel, M.; Imirzalioglu, C.; et al. Clinical Relevance of the Microbiome in Odontogenic Abscesses. Biology 2021, 10, 916. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10090916
Böttger S, Zechel-Gran S, Schmermund D, Streckbein P, Wilbrand J-F, Knitschke M, Pons-Kühnemann J, Hain T, Weigel M, Imirzalioglu C, et al. Clinical Relevance of the Microbiome in Odontogenic Abscesses. Biology. 2021; 10(9):916. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10090916
Chicago/Turabian StyleBöttger, Sebastian, Silke Zechel-Gran, Daniel Schmermund, Philipp Streckbein, Jan-Falco Wilbrand, Michael Knitschke, Jörn Pons-Kühnemann, Torsten Hain, Markus Weigel, Can Imirzalioglu, and et al. 2021. "Clinical Relevance of the Microbiome in Odontogenic Abscesses" Biology 10, no. 9: 916. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10090916