
SARS-CoV-2 and Skin: The Pathologist’s Point of View

 ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
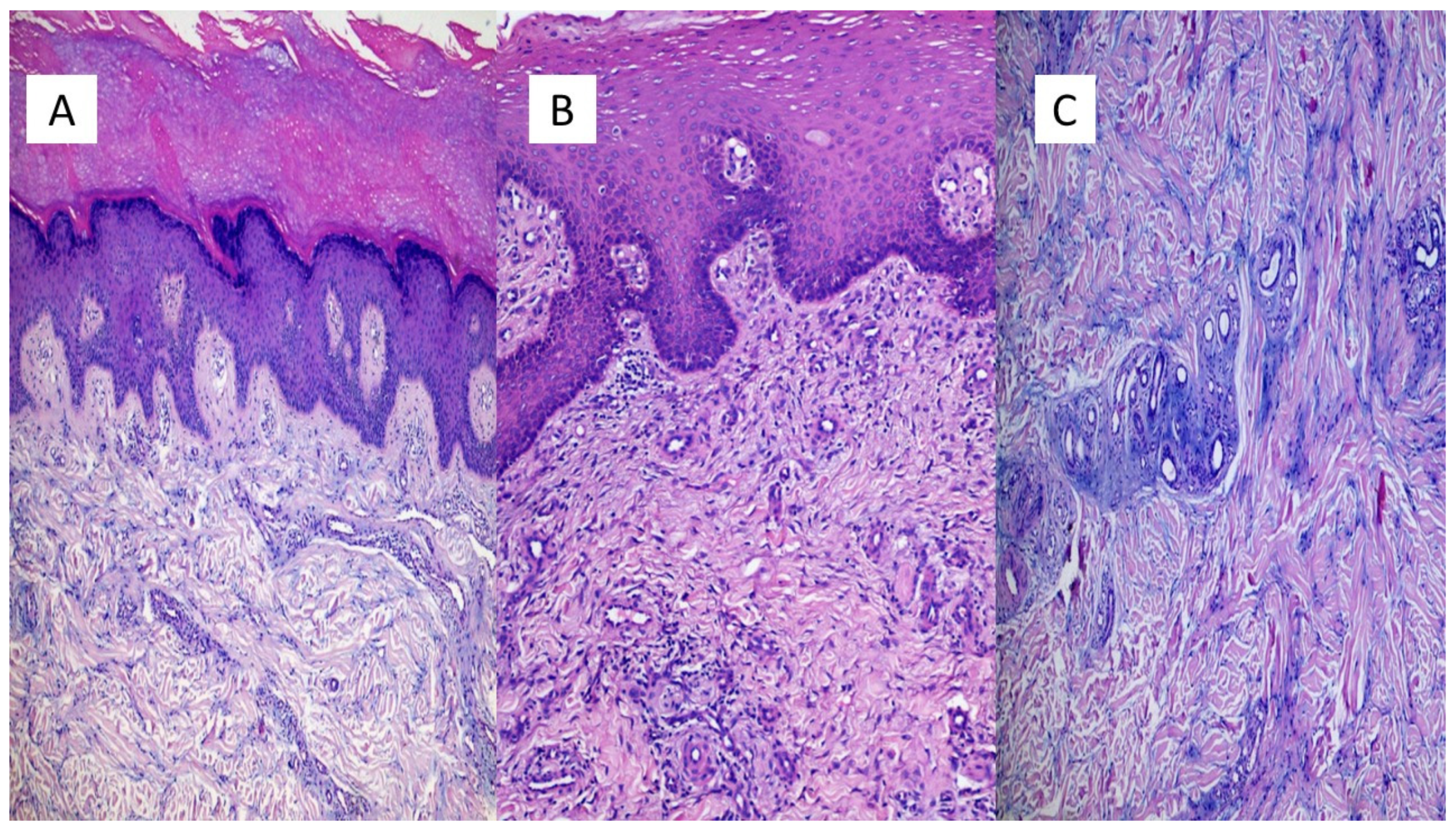
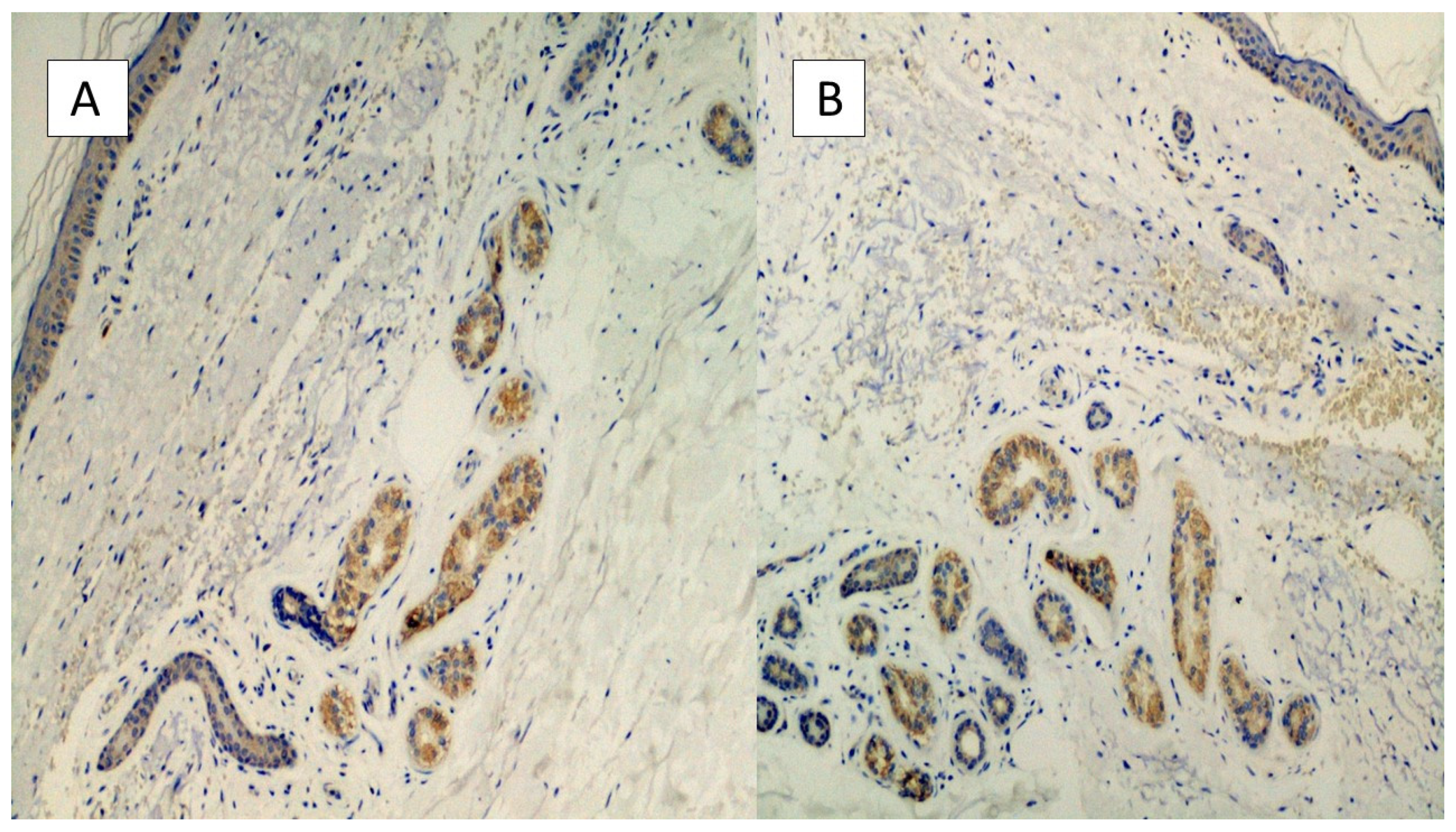
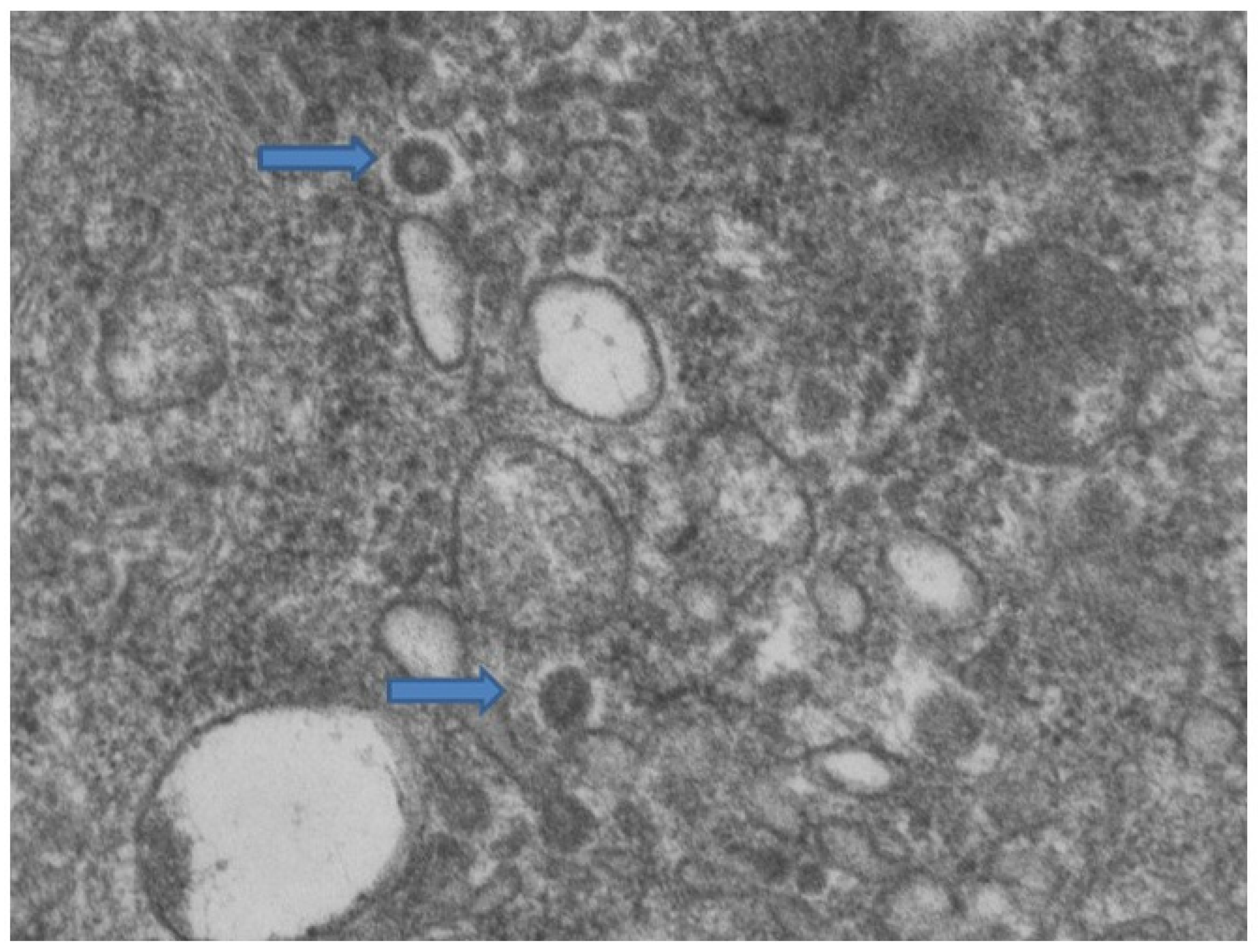
3.1. Erythema-Multiforme Like Eruptions
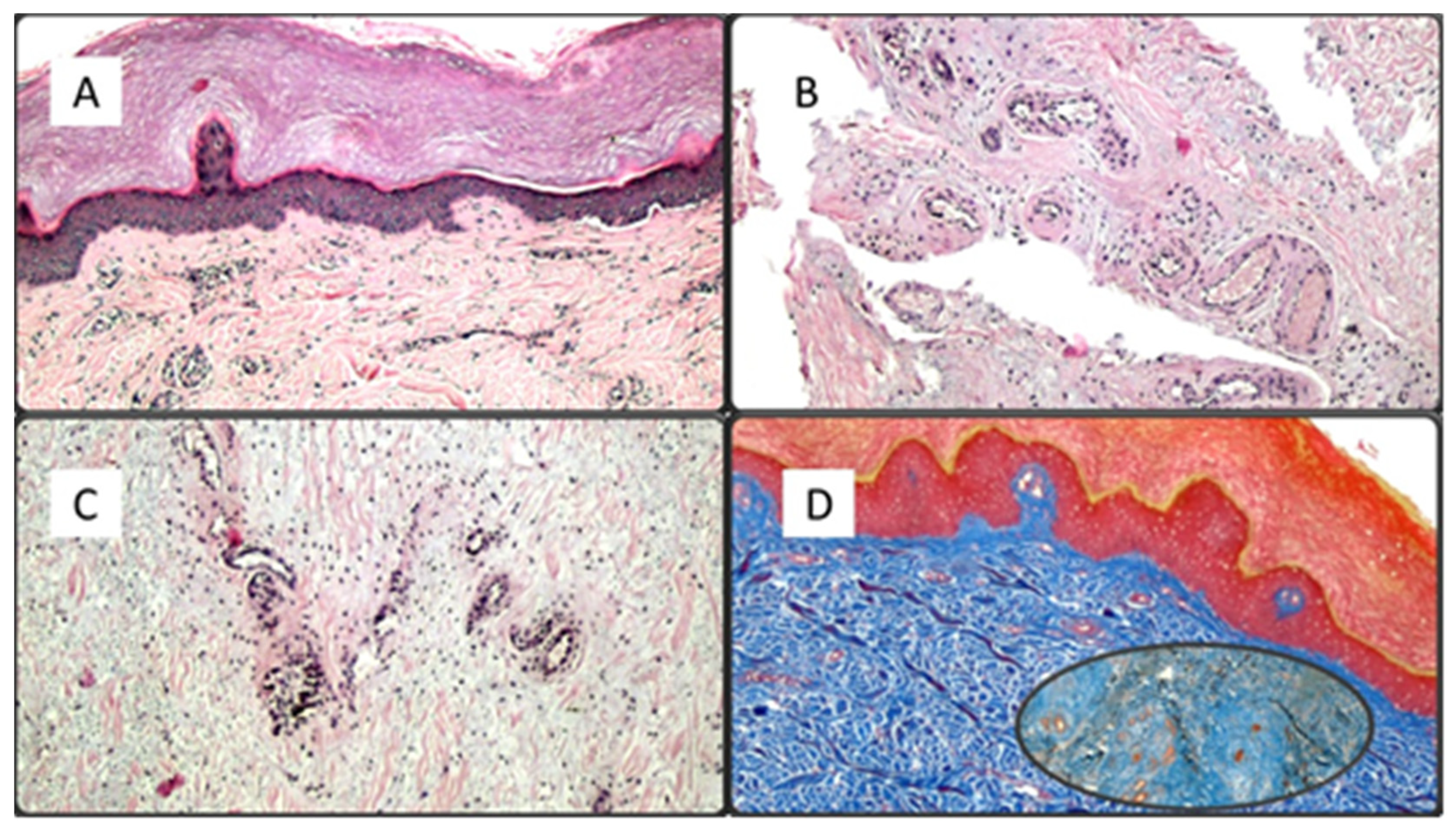
3.2. Pseudochildblains
3.3. Chickenpox Rush
3.4. Urticarioid Rash
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Mohamadian, M.; Chiti, H.; Shoghli, A.; Biglari, S.; Parsamanesh, N.; Esmaeilzadeh, A. COVID-19: Virology, biology and novel laboratory diagnosis. J. Gene Med. 2021, 23, e3303. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. Available online: https://COVID19.who.int/ (accessed on 10 May 2021).
- Tratner, I. SARS-CoV: 1. The virus. Med. Sci. 2003, 19, 885–891. [Google Scholar]
- De Wit, E.; van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention (CDC). CDC 2019—Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. 2020. Available online: https://www.fda.gov/media/134922/download (accessed on 11 May 2021).
- Cepheid. Xpert® Xpress SARS-CoV-2: Instructions for Use for Labs. Available online: https://www.fda.gov/media/136314/download (accessed on 10 May 2021).
- Taleghani, N.; Taghipour, F. Diagnosis of COVID-19 for controlling the pandemic: A review of the state-of-the-art. Biosens. Bioelectron. 2021, 15, 112830. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, M.; Gianotti, R.; Shah, M.; Bradanini, L.; Tosi, D.; Veraldi, S.; Ziv, M.; Leshem, E.; Dodiuk-Gad, R.P. Cutaneous manifestations of COVID-19: Report of three cases and a review of literature. J. Dermatol. Sci. 2020, 98, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, G.; Foti, C.; Colagrande, A.; Cimmino, A.; Scarcella, S.; Cicco, G.; Sablone, S.; Arezzo, F.; Romita, P.; Lettini, T.; et al. Skin Manifestation of SARS-CoV-2: The Italian Experience. J. Clin. Med. 2021, 8, 1566. [Google Scholar] [CrossRef] [PubMed]
- Rongioletti, F.; Ferreli, C.; Sena, P.; Caputo, V.; Atzori, L. Clinicopathologic correlations of COVID-19-related cutaneous manifestations with special emphasis on histopathologic patterns. Clin. Dermatol. 2021, 39, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Colmenero, I.; Santonja, C.; Alonso-Riaño, M.; Noguera-Morel, L.; Hernández-Martín, A.; Andina, D.; Wiesner, T.; Rodríguez-Peralto, J.L.; Requena, L.; Torrelo, A. SARS-CoV-2 endothelial infection causes COVID-19 chilblains: Histopathological, immunohistochemical and ultrastructural study of seven paediatric cases. Br. J. Dermatol. 2020, 183, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Torrelo, A.; Andina, D.; Santonja, C.; Noguera-Morel, L.; Bascuas-Arribas, M.; Gaitero-Tristan, J.; Alonso-Cadenas, J.A.; Escalada-Pellitero, S.; Hernandez-Martin, A.; de la Torre-Espi, M.; et al. Erythema multiforme-like lesions in children and COVID-19. Pediatr. Dermatol. 2020, 37, 442–446. [Google Scholar] [CrossRef] [PubMed]
- El Hachem, M.; Diociaiuti, A.; Concato, C.; Carsetti, R.; Carnevale, C.; Ciofi Degli Atti, M.; Giovannelli, L.; Latella, E.; Porzio, O.; Rossi, S.; et al. A clinical, histopathological and laboratory study of 19 consecutive Italian paediatric patients with chilblain-like lesions: Lights and shadows on the relationship with COVID-19 infection. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2620–2629. [Google Scholar] [CrossRef] [PubMed]
- Andina, D.; Colmenero, I.; Santonja, C.; Muñoz de León, I.; Noguera-Morel, L.; Hernández-Martín, A.; Torrelo, A. Suspected COVID-19-related reticulated purpura of the soles in an infant. Pediatr. Dermatol. 2021, 38, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Ingravallo, G.; Mazzotta, F.; Resta, L.; Sablone, S.; Cazzato, G.; Cimmino, A.; Rossi, R.; Colagrande, A.; Ferrante, B.; Troccoli, T.; et al. Inflammatory Skin Lesions in Three SARS-CoV-2 Swab-Negative Adolescents: A Possible COVID-19 Sneaky Manifestation? Pediatr. Rep. 2021, 9, 181–188. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skin Manifestation | Number of Patients | Age (Years) | Localization | Immunohistochemistry | Electron Microscopy |
|---|---|---|---|---|---|
| Erythema Multiforme-Like | 7 | 39–64 | Widespread | Positive | Positive |
| Pseudochildblains | 7 | 12–23 | Foot and malleolar region | Positive | Positive |
| Chickenpox rash | 2 | 38,42 | Chest, back, and face | Positive | Not carried out |
| Urticarioid rash | 1 | 43 | Widespread | Positive | Not carried out |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazzato, G.; Mazzia, G.; Cimmino, A.; Colagrande, A.; Sablone, S.; Lettini, T.; Rossi, R.; Santarella, N.; Elia, R.; Nacchiero, E.; et al. SARS-CoV-2 and Skin: The Pathologist’s Point of View. Biomolecules 2021, 11, 838. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11060838
Cazzato G, Mazzia G, Cimmino A, Colagrande A, Sablone S, Lettini T, Rossi R, Santarella N, Elia R, Nacchiero E, et al. SARS-CoV-2 and Skin: The Pathologist’s Point of View. Biomolecules. 2021; 11(6):838. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11060838
Chicago/Turabian StyleCazzato, Gerardo, Giulia Mazzia, Antonietta Cimmino, Anna Colagrande, Sara Sablone, Teresa Lettini, Roberta Rossi, Nadia Santarella, Rossella Elia, Eleonora Nacchiero, and et al. 2021. "SARS-CoV-2 and Skin: The Pathologist’s Point of View" Biomolecules 11, no. 6: 838. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11060838