
Harnessing the Potential of Enzymes as Inhaled Therapeutics in Respiratory Tract Diseases: A Review of the Literature

Abstract
:1. Introduction
2. Review Methodology
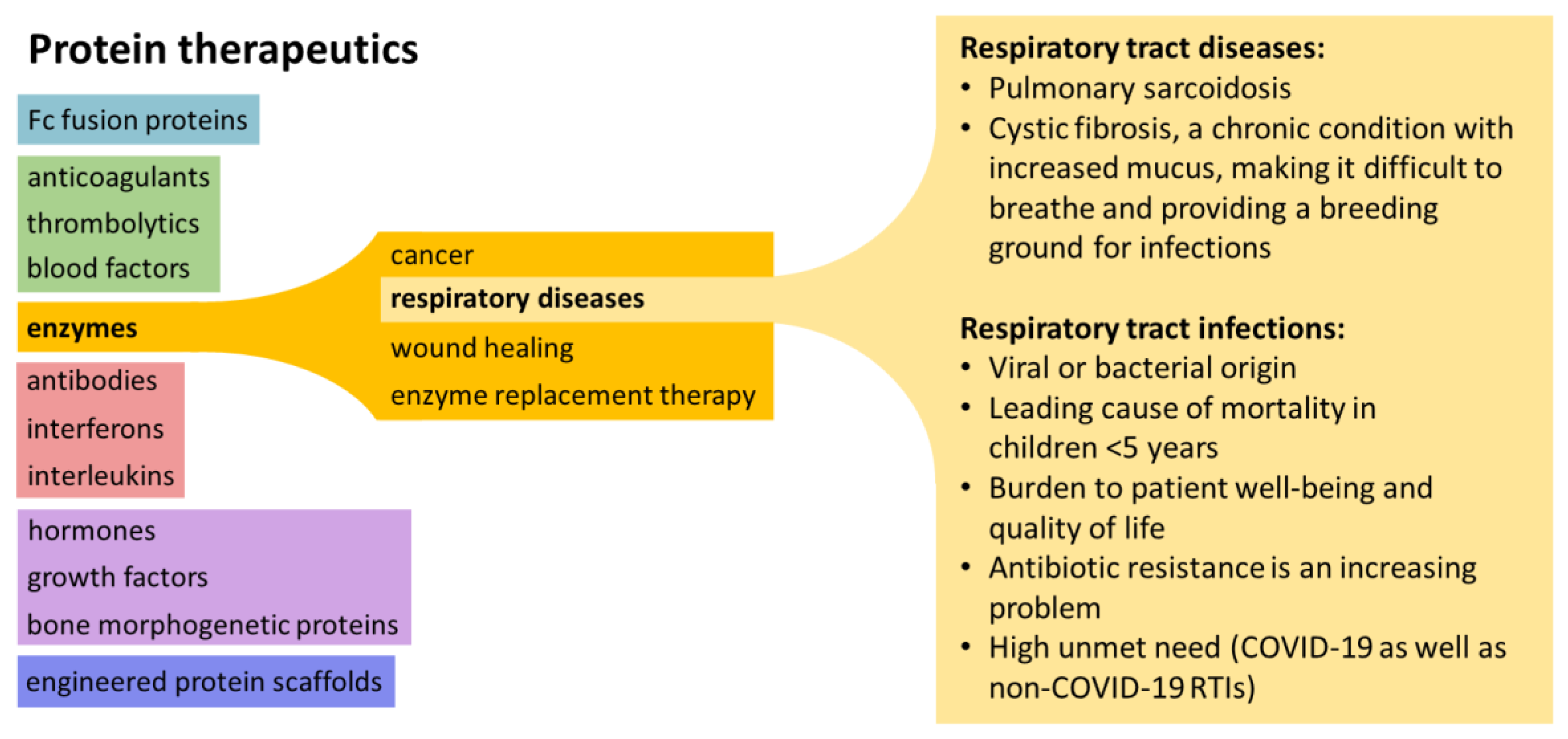
3. The Rationale for Enzyme Therapeutics
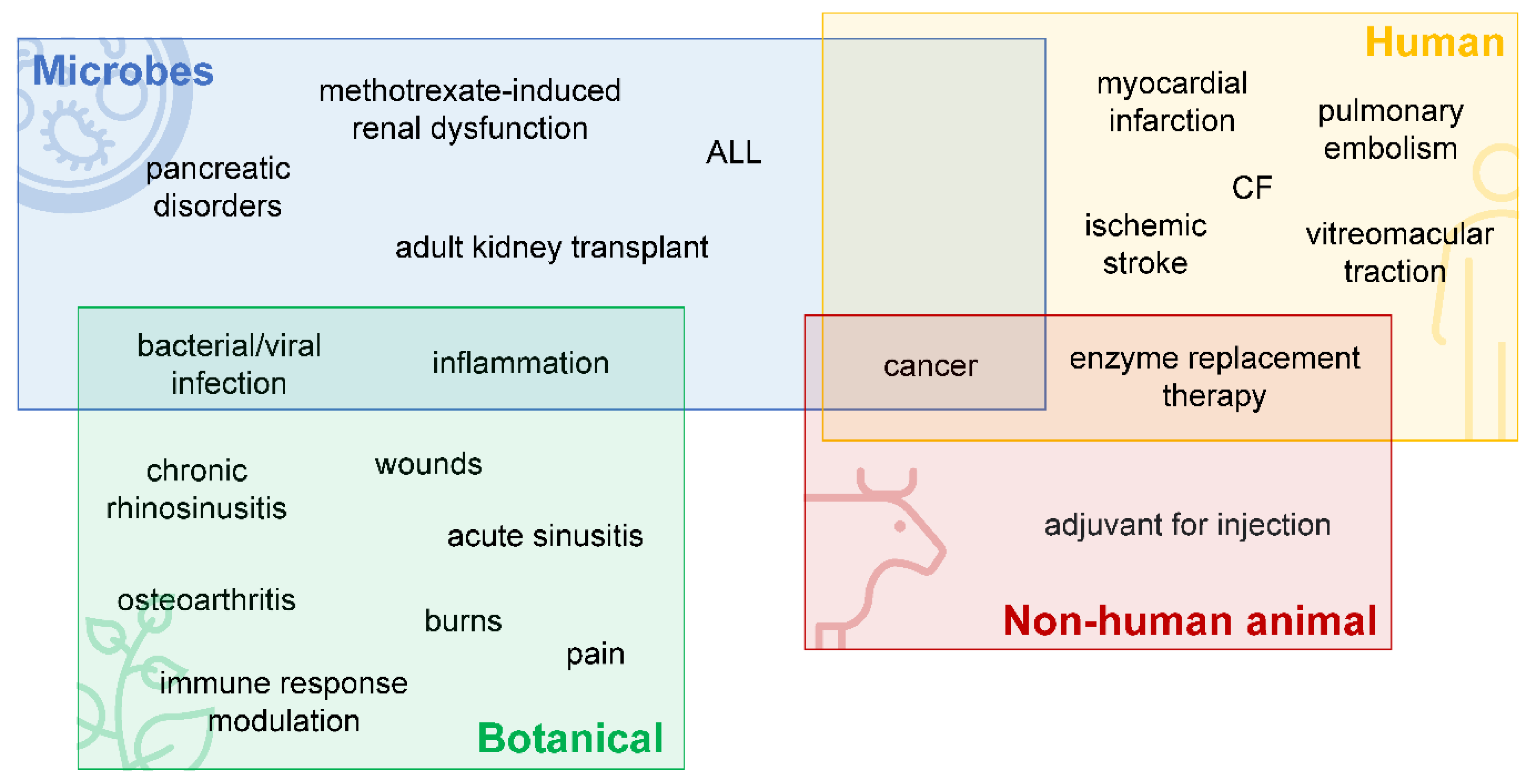
3.1. Enzymes Derived from Animals
3.2. Enzymes Derived from Microbes
3.3. Enzymes Derived from Botanical Sources
3.4. Challenges with Enzyme Therapeutics
4. Inhaled Enzyme Therapeutics to Treat RTDs
4.1. Advantages and Disadvantages of Inhaled Therapies
4.2. Current Uses of Inhaled Enzyme Therapeutics in RTDs
5. Developing Enzyme Therapeutics for RTD
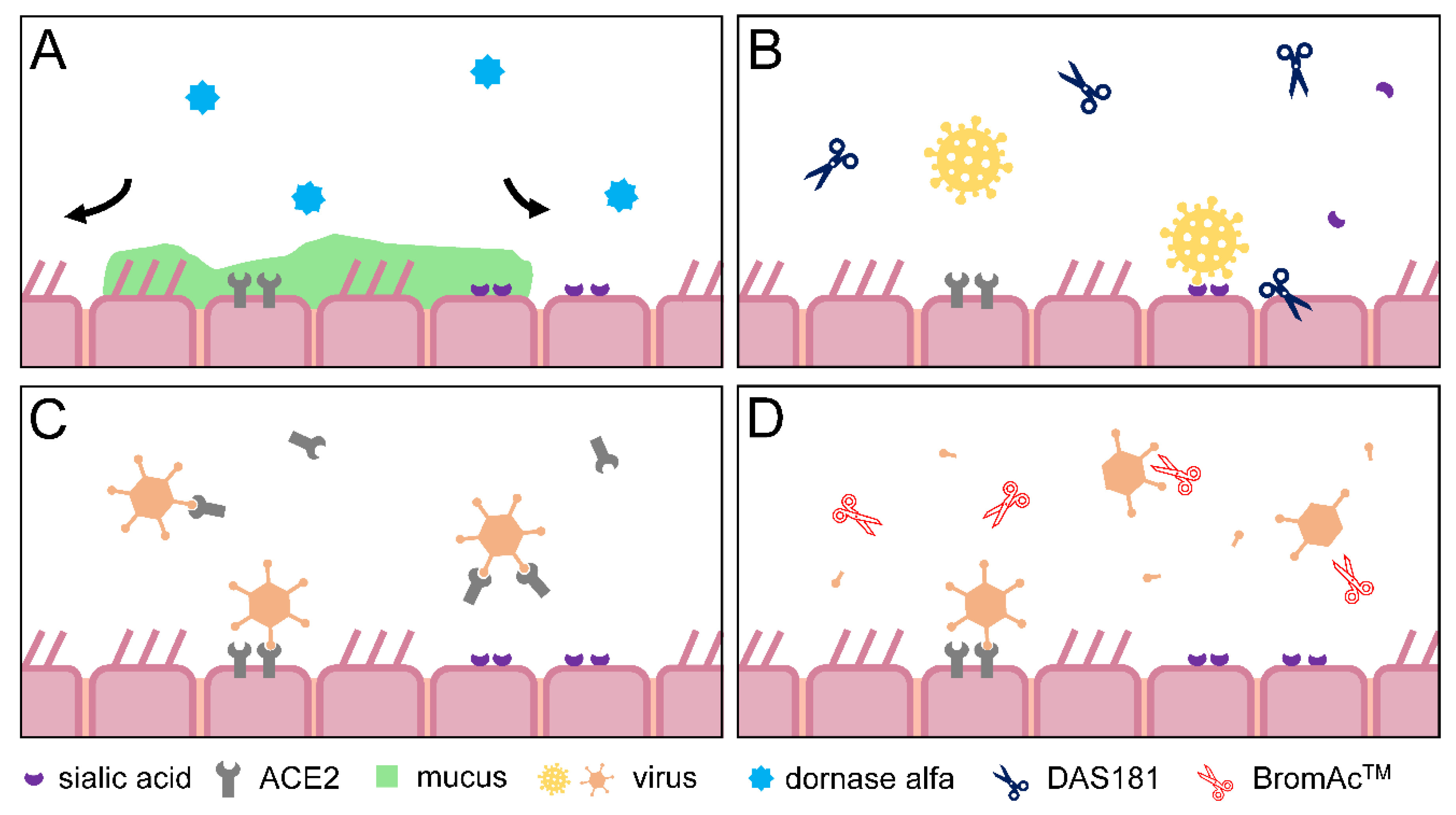
5.1. Dornase Alfa
5.2. DAS181
5.3. Angiotensin Converting Enzyme 2
5.4. Other Pipeline and Pre-Clinical Therapeutics
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dimitrov, D.S. Therapeutic proteins. Methods Mol. Biol. 2012, 899, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.S.; Stevens, R.C. Structural aspects of therapeutic enzymes to treat metabolic disorders. Hum. Mutat. 2009, 30, 1591–1610. [Google Scholar] [CrossRef] [PubMed]
- Leader, B.; Baca, Q.J.; Golan, D.E. Protein therapeutics: A summary and pharmacological classification. Nat. Rev. Drug Discov. 2008, 7, 21–39. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, M.; Lombardero, L.; Gomez-Gonzalez, A.; Solari, C.; Angulo-Barturen, I.; Acera, A.; Vecino, E.; Astigarraga, E.; Barreda-Gomez, G. Enzyme Therapy: Current Challenges and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 9181. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.; Muro, S. Lysosomal enzyme replacement therapies: Historical development, clinical outcomes, and future perspectives. Adv. Drug Deliv. Rev. 2017, 118, 109–134. [Google Scholar] [CrossRef]
- Balakireva, A.V.; Kuznetsova, N.V.; Petushkova, A.I.; Savvateeva, L.V.; Zamyatnin, A.A., Jr. Trends and Prospects of Plant Proteases in Therapeutics. Curr. Med. Chem. 2019, 26, 465–486. [Google Scholar] [CrossRef]
- Singh, R.; Kumar, M.; Mittal, A.; Mehta, P.K. Microbial enzymes: Industrial progress in 21st century. 3 Biotech 2016, 6, 174. [Google Scholar] [CrossRef] [Green Version]
- Mane, P.; Tale, V. Overview of Microbial Therapeutic Enzymes. Int. J. Curr. Microbiol. Appl. Sci. 2015, 4, 17–26. [Google Scholar]
- Datta, S.; Rajnish, K.N.; George Priya Doss, C.; Melvin Samuel, S.; Selvarajan, E.; Zayed, H. Enzyme therapy: A forerunner in catalyzing a healthy society? Expert Opin. Biol. Ther. 2020, 20, 1151–1174. [Google Scholar] [CrossRef]
- Lazarus, R.A.; Wagener, J.S. Recombinant Human Deoxyribonuclease I. In Pharmaceutical Biotechnology; Springer Nature: Cham, Switzerland, 2019; pp. 471–488. [Google Scholar] [CrossRef]
- Biopharma, H. Idefirix® (Imlifidase). Available online: https://www.hansabiopharma.com/files/Corporate-Communications/Media-Toolkit/Media-Toolkit-En/HansaBiopharma_MediaRes_Idefirix_Backgrounder_20210726.pdf (accessed on 21 January 2022).
- Hansa Biopharma and Sarepta Therapeutics Agreement. Available online: https://s24.q4cdn.com/980434894/files/doc_presentations/2020/07/202000702-HNSA-GT-Partnership-Sarepta-FINAL2.pdf (accessed on 21 January 2022).
- BTG International Inc. Voraxaze® (Glucarpidase)—The Earlier You Treat Methotrexate Toxicity with Voraxaze®, the Better. Available online: https://voraxaze.com/ (accessed on 21 January 2022).
- Inceptua AB. JETREA®—Summary of Product Characteristics. 2017. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/jetrea (accessed on 21 January 2022).
- MediWound Ltd. NexoBrid® Disruptive Therapy for Burn Care. Available online: https://www.mediwound.com/products/nexobrid/ (accessed on 21 January 2022).
- Amphastar Pharmaceuticals, I. AMPHADASE®—Prescribing Information. 2014. Available online: https://amphastar.com/assets/amphadase-insert-5-2014.pdf (accessed on 21 January 2022).
- Sanofi-aventis U.S. LLC. Elitek Rasburicase IV Infusion. Available online: https://www.elitekpro.com/ (accessed on 21 January 2022).
- Cioni, P.; Gabellieri, E.; Campanini, B.; Bettati, S.; Raboni, S. Use of Exogenous Enzymes in Human Therapy: Approved Drugs and Potential Applications. Curr. Med. Chem. 2022, 29, 411–452. [Google Scholar] [CrossRef]
- Chiesi USA Inc. Retavase (Reteplase) for Injection. Available online: https://retavase.com/ (accessed on 21 January 2022).
- U.S. Food & Drug Administration. Drugs@FDA: FDA-Approved Drugs. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=103532 (accessed on 7 November 2021).
- Genentech. Pulmozyme (Dornase Alfa) Inhalation Solution. Available online: https://www.pulmozyme.com/patient/dosing-administration/preparing-for-treatment.html (accessed on 25 January 2022).
- Baldo, B.A. Enzymes approved for human therapy: Indications, mechanisms and adverse effects. BioDrugs 2015, 29, 31–55. [Google Scholar] [CrossRef] [PubMed]
- Boehringer Ingelheim. About Actilyse®. Available online: https://www.boehringer-ingelheim.com/products/actilyse (accessed on 21 January 2022).
- Lundbeck Inc. ELSPAR®—Highlights of Prescribing Information; 2013. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/101063s5169lbl.pdf (accessed on 21 January 2022).
- Servier Pharmaceuticals LLC. ONCASPAR: A Proven Treatment That Helps You Fight ALL. Available online: https://www.oncaspar.com/ (accessed on 21 January 2022).
- Servier Pharmaceuticals LLC. ASPARLAS™—Highlights of Prescribing Information. 2018. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761102s000lbl.pdf (accessed on 21 January 2022).
- Kinch, M.S. An overview of FDA-approved biologics medicines. Drug Discov. Today 2015, 20, 393–398. [Google Scholar] [CrossRef]
- World Health Organization. Urgent Health Challenges for the Next Decade. Available online: https://www.who.int/news-room/photo-story/photo-story-detail/urgent-health-challenges-for-the-next-decade (accessed on 25 January 2022).
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 25 January 2022).
- WHO. Chronic Respiratory Diseases. Available online: https://www.who.int/gard/publications/chronic_respiratory_diseases.pdf (accessed on 6 September 2021).
- Collaborators, G.L. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.A.; Singer, D.E. Health-related quality of life of adults with upper respiratory tract infections. J. Gen. Int. Med. 2003, 18, 802–807. [Google Scholar] [CrossRef] [Green Version]
- Kokoska, L.; Kloucek, P.; Leuner, O.; Novy, P. Plant-Derived Products as Antibacterial and Antifungal Agents in Human Health Care. Curr. Med. Chem. 2019, 26, 5501–5541. [Google Scholar] [CrossRef]
- Parham, S.; Kharazi, A.Z.; Bakhsheshi-Rad, H.R.; Nur, H.; Ismail, A.F.; Sharif, S.; RamaKrishna, S.; Berto, F. Antioxidant, Antimicrobial and Antiviral Properties of Herbal Materials. Antioxidants 2020, 9, 1309. [Google Scholar] [CrossRef]
- UmaMaheswari, T.; Hemalatha, T.; Sankaranarayanan, P.; Puvanakrishnan, R. Enzyme Therapy: Current Perspectives. Indian J. Exp. Biol. 2016, 54, 7–16. [Google Scholar]
- Meghwanshi, G.K.; Kaur, N.; Verma, S.; Dabi, N.K.; Vashishtha, A.; Charan, P.D.; Purohit, P.; Bhandari, H.S.; Bhojak, N.; Kumar, R. Enzymes for pharmaceutical and therapeutic applications. Biotechnol. Appl. Biochem. 2020, 67, 586–601. [Google Scholar] [CrossRef]
- Concolino, D.; Deodato, F.; Parini, R. Enzyme replacement therapy: Efficacy and limitations. Ital. J. Pediatr. 2018, 44, 120. [Google Scholar] [CrossRef]
- Lindkvist, B. Diagnosis and treatment of pancreatic exocrine insufficiency. World J. Gastroenterol. 2013, 19, 7258–7266. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Ketwaroo, G.A.; Money, M.E.; Opekun, A.R. Enzyme therapy for functional bowel disease-like post-prandial distress. J. Dig. Dis. 2018, 19, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Dajani, R.; Zhang, Y.; Taft, P.J.; Travis, S.M.; Starner, T.D.; Olsen, A.; Zabner, J.; Welsh, M.J.; Engelhardt, J.F. Lysozyme secretion by submucosal glands protects the airway from bacterial infection. Am. J. Respir. Cell Mol. Biol. 2005, 32, 548–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vachher, M.; Sen, A.; Kapila, R.; Nigam, A. Microbial therapeutic enzymes: A promising area of biopharmaceuticals. Curr. Res. Biotechnol. 2021, 3, 195–208. [Google Scholar] [CrossRef]
- Robinson, P.K. Enzymes: Principles and biotechnological applications. Essays Biochem. 2015, 59, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.; Loomis, L.; Fischetti, V.A. Prevention and elimination of upper respiratory colonization of mice by group A streptococci by using a bacteriophage lytic enzyme. Proc. Natl. Acad. Sci. USA 2001, 98, 4107–4112. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Lu, H.; Huang, J.; Li, G.; Huang, Q. EnzyBase: A novel database for enzybiotic studies. BMC Microbiol. 2012, 12, 54. [Google Scholar] [CrossRef] [Green Version]
- Ferriol-Gonzalez, C.; Domingo-Calap, P. Phages for Biofilm Removal. Antibiotics 2020, 9, 268. [Google Scholar] [CrossRef]
- Pires, D.P.; Oliveira, H.; Melo, L.D.; Sillankorva, S.; Azeredo, J. Bacteriophage-encoded depolymerases: Their diversity and biotechnological applications. Appl. Microbiol. Biotechnol. 2016, 100, 2141–2151. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, H.; Sao-Jose, C.; Azeredo, J. Phage-Derived Peptidoglycan Degrading Enzymes: Challenges and Future Prospects for In Vivo Therapy. Viruses 2018, 10, 292. [Google Scholar] [CrossRef] [Green Version]
- Fowler, V.G., Jr.; Das, A.F.; Lipka-Diamond, J.; Schuch, R.; Pomerantz, R.; Jauregui-Peredo, L.; Bressler, A.; Evans, D.; Moran, G.J.; Rupp, M.E.; et al. Exebacase for patients with Staphylococcus aureus bloodstream infection and endocarditis. J. Clin. Investig. 2020, 130, 3750–3760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazquez, R.; Garcia, E.; Garcia, P. Phage Lysins for Fighting Bacterial Respiratory Infections: A New Generation of Antimicrobials. Front. Immunol. 2018, 9, 2252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstmans, H.; Criel, B.; Briers, Y. Synthetic biology of modular endolysins. Biotechnol. Adv. 2018, 36, 624–640. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S. Chapter 1—Introduction to enzymes and their applications. In Introduction to Pharmaceutical Biotechnology; IOP Publishing Ltd.: Bristol, UK, 2018; Volume 2. [Google Scholar]
- Barrett, A.J.; Buttle, D.J. Names and numbers of papaya proteinases. Biochem. J. 1985, 228, 527. [Google Scholar] [CrossRef] [Green Version]
- Dando, P.M.; Sharp, S.L.; Buttle, D.J.; Barrett, A.J. Immunoglobulin E antibodies to papaya proteinases and their relevance to chemonucleolysis. Spine 1995, 20, 981–985. [Google Scholar] [CrossRef]
- Chaiwut, P.; Nitsawang, S.; Shank, L.; Kanasawud, P. A Comparative Study on Properties and Proteolytic Components of Papaya Peel and Latex Proteases. Chiang Mai J. Sci. 2007, 34, 109–118. [Google Scholar]
- Rowan, A.D.; Buttle, D.J.; Barrett, A.J. The cysteine proteinases of the pineapple plant. Biochem. J. 1990, 266, 869–875. [Google Scholar]
- Anaga, A.O.; Onehi, E.V. Antinociceptive and anti-inflammatory effects of the methanol seed extract of Carica papaya in mice and rats. Afr. J. Pharm. Pharmacol. 2010, 4, 140–144. [Google Scholar]
- Danborno, A.M.; Ibrahim, S.H.; Mallo, M.J. The Anti-Inflammatory and Analgesic Effects Of the Aqueous Leaves Extract of Carica Papaya. IOSR J. Pharm. Biol. Sci. 2018, 13, 60–63. [Google Scholar]
- Pandey, S.; Cabot, P.J.; Shaw, P.N.; Hewavitharana, A.K. Anti-inflammatory and immunomodulatory properties of Carica papaya. J. Immunotoxicol. 2016, 13, 590–602. [Google Scholar] [CrossRef] [Green Version]
- Ajlia, S.A.; Majid, F.A.; Suvik, A.; Effendy, M.A.; Nouri, H.S. Efficacy of papain-based wound cleanser in promoting wound regeneration. Pak. J. Biol. Sci. 2010, 13, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knezevic, N.N.; Mandalia, S.; Raasch, J.; Knezevic, I.; Candido, K.D. Treatment of chronic low back pain—New approaches on the horizon. J. Pain Res. 2017, 10, 1111–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milne, J.; Brand, S. Occupational asthma after inhalation of dust of the proteolytic enzyme, papain. Br. J. Ind. Med. 1975, 32, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; McIntosh, J.; Liu, J. Current prevalence rate of latex allergy: Why it remains a problem? J. Occup. Health 2016, 58, 138–144. [Google Scholar] [CrossRef]
- McCarty, S.M.; Percival, S.L. Proteases and Delayed Wound Healing. Adv. Wound Care 2013, 2, 438–447. [Google Scholar] [CrossRef]
- Chakraborty, A.J.; Mitra, S.; Tallei, T.E.; Tareq, A.M.; Nainu, F.; Cicia, D.; Dhama, K.; Emran, T.B.; Simal-Gandara, J.; Capasso, R. Bromelain a Potential Bioactive Compound: A Comprehensive Overview from a Pharmacological Perspective. Life 2021, 11, 317. [Google Scholar] [CrossRef]
- Pavan, R.; Jain, S.; Shraddha; Kumar, A. Properties and therapeutic application of bromelain: A review. Biotechnol. Res. Int. 2012, 2012, 976203. [Google Scholar] [CrossRef] [Green Version]
- Llivisaca-Contreras, S.A.; Naranjo-Moran, J.; Pino-Acosta, A.; Pieters, L.; Vanden Berghe, W.; Manzano, P.; Vargas-Perez, J.; Leon-Tamariz, F.; Cevallos-Cevallos, J.M. Plants and Natural Products with Activity against Various Types of Coronaviruses: A Review with Focus on SARS-CoV-2. Molecules 2021, 26, 4099. [Google Scholar] [CrossRef]
- Buttner, L.; Achilles, N.; Bohm, M.; Shah-Hosseini, K.; Mosges, R. Efficacy and tolerability of bromelain in patients with chronic rhinosinusitis–A pilot study. B-ENT 2013, 9, 217–225. [Google Scholar]
- Passali, D.; Passali, G.C.; Bellussi, L.M.; Sarafoleanu, C.; Loglisci, M.; Manea, C.; Iosif, C.; Passali, F.M. Bromelain’s penetration into the blood and sinonasal mucosa in patients with chronic rhinosinusitis. Acta Otorhinolaryngol. Ital. 2018, 38, 225–228. [Google Scholar] [CrossRef]
- Braun, J.M.; Schneider, B.; Beuth, H.J. Therapeutic use, efficiency and safety of the proteolytic pineapple enzyme Bromelain-POS in children with acute sinusitis in Germany. In Vivo 2005, 19, 417–421. [Google Scholar] [PubMed]
- Baur, X. Studies on the specificity of human IgE-antibodies to the plant proteases papain and bromelain. Clin. Allergy. 1979, 9, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Pereira de Sousa, I.; Cattoz, B.; Wilcox, M.D.; Griffiths, P.C.; Dalgliesh, R.; Rogers, S.; Bernkop-Schnurch, A. Nanoparticles decorated with proteolytic enzymes, a promising strategy to overcome the mucus barrier. Eur. J. Pharm. Biopharm. 2015, 97, 257–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlapfer, P.; Zhang, P.; Wang, C.; Kim, T.; Banf, M.; Chae, L.; Dreher, K.; Chavali, A.K.; Nilo-Poyanco, R.; Bernard, T.; et al. Genome-Wide Prediction of Metabolic Enzymes, Pathways, and Gene Clusters in Plants. Plant Physiol. 2017, 173, 2041–2059. [Google Scholar] [CrossRef] [Green Version]
- Matthews, A.A.; Ee, P.L.R.; Ge, R. Developing inhaled protein therapeutics for lung diseases. Mol. Biomed. 2020, 1, 11. [Google Scholar] [CrossRef]
- Craik, C.S.; Page, M.J.; Madison, E.L. Proteases as therapeutics. Biochem. J. 2011, 435, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Bax, B.E.; Bain, M.D.; Fairbanks, L.D.; Webster, A.D.; Chalmers, R.A. In vitro and in vivo studies with human carrier erythrocytes loaded with polyethylene glycol-conjugated and native adenosine deaminase. Br. J. Haematol. 2000, 109, 549–554. [Google Scholar] [CrossRef]
- Ahuja, K.; Rawat, A. Enzymes Market Size By Product (Proteases, Lipases, Carbohydrases [Amylases, Xylanases, Cellulases, Pectinases, Lactases], Polymerases & Nucleases, Phytases, Catalyses), By Application (Food & Beverage, Processed Food, Diary, Bakery, Confectionary), Industry Analysis Report, Regional Outlook, Growth Potential, Price Trends, Competitive Market Share & Forecast, 2018–2024; 2019. Available online: https://www.gminsights.com/industry-analysis/enzymes-market (accessed on 14 October 2021).
- Gupta, P.V.; Nirwane, A.M.; Nagarsenker, M.S. Inhalable Levofloxacin Liposomes Complemented with Lysozyme for Treatment of Pulmonary Infection in Rats: Effective Antimicrobial and Antibiofilm Strategy. AAPS PharmSciTech 2018, 19, 1454–1467. [Google Scholar] [CrossRef]
- Nakamura, S.; Hashimoto, Y.; Mikami, M.; Yamanaka, E.; Soma, T.; Hino, M.; Azuma, A.; Kudoh, S. Effect of the proteolytic enzyme serrapeptase in patients with chronic airway disease. Respirology 2003, 8, 316–320. [Google Scholar] [CrossRef]
- Shahid, S. Role of Systemic Enzymes in Infections. WebmedCentral Complement. Med. 2011, 2, WMC002495. [Google Scholar] [CrossRef]
- Tiwari, M. The role of serratiopeptidase in the resolution of inflammation. Asian. J. Pharm. Sci. 2017, 12, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part I: Physiological factors affecting therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 56, 588–599. [Google Scholar] [CrossRef] [PubMed]
- Rau, J.L. The inhalation of drugs: Advantages and problems. Respir. Care 2005, 50, 367–382. [Google Scholar] [PubMed]
- Sécher, T.; Mayor, A.; Heuzé-Vourc’h, N. Inhalation of Immuno-Therapeutics/-Prophylactics to Fight Respiratory Tract Infections: An Appropriate Drug at the Right Place! Front. Immunol. 2019, 10, 2760. [Google Scholar] [CrossRef] [Green Version]
- Pintucci, J.P.; Corno, S.; Garotta, M. Biofilms and infections of the upper respiratory tract. Eur. Rev. Med. Pharmacol. Sci. 2010, 14, 683–690. [Google Scholar]
- Hall, C.W.; Mah, T.F. Molecular mechanisms of biofilm-based antibiotic resistance and tolerance in pathogenic bacteria. FEMS Microbiol. Rev. 2017, 41, 276–301. [Google Scholar] [CrossRef]
- Rabin, N.; Zheng, Y.; Opoku-Temeng, C.; Du, Y.; Bonsu, E.; Sintim, H.O. Biofilm formation mechanisms and targets for developing antibiofilm agents. Future Med. Chem. 2015, 7, 493–512. [Google Scholar] [CrossRef]
- Martin, I.; Waters, V.; Grasemann, H. Approaches to Targeting Bacterial Biofilms in Cystic Fibrosis Airways. Int. J. Mol. Sci. 2021, 22, 2155. [Google Scholar] [CrossRef]
- Inspira Pharmaceuticals Ltd. Inspira Pharmaceuticals and University of Oxford Demonstrate Proof-of-Concept of Novel IPA Formulations for COVID-19. 2021. Available online: https://www.inspiraph.com/news (accessed on 9 June 2022).
- VanDrisse, C.M.; Lipsh-Sokolik, R.; Khersonsky, O.; Fleishman, S.J.; Newman, D.K. Computationally designed pyocyanin demethylase acts synergistically with tobramycin to kill recalcitrant Pseudomonas aeruginosa biofilms. Proc. Natl. Acad. Sci. USA 2021, 118, e2022012118. [Google Scholar] [CrossRef]
- Geller, D.E. Aerosol antibiotics in cystic fibrosis. Respir. Care 2009, 54, 658–670. [Google Scholar] [CrossRef]
- Heyder, J. Deposition of inhaled particles in the human respiratory tract and consequences for regional targeting in respiratory drug delivery. Proc. Am. Thorac. Soc. 2004, 1, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part II: The role of inhalant delivery devices and drug formulations in therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 56, 600–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghardt, J.M.; Kloft, C.; Sharma, A. Inhaled Therapy in Respiratory Disease: The Complex Interplay of Pulmonary Kinetic Processes. Can. Respir. J. 2018, 2018, 2732017. [Google Scholar] [CrossRef] [Green Version]
- Moussa, E.M.; Panchal, J.P.; Moorthy, B.S.; Blum, J.S.; Joubert, M.K.; Narhi, L.O.; Topp, E.M. Immunogenicity of Therapeutic Protein Aggregates. J. Pharm. Sci. 2016, 105, 417–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pharmapproach. Pulmonary Route of Drug Administration: Advantages and Disadvantages. Available online: https://www.pharmapproach.com/pulmonary-route-of-drug-administration-advantages-and-disadvantages/ (accessed on 25 January 2022).
- Coleman, C.I.; Limone, B.; Sobieraj, D.M.; Lee, S.; Roberts, M.S.; Kaur, R.; Alam, T. Dosing frequency and medication adherence in chronic disease. J. Manag. Care. Pharm. 2012, 18, 527–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodier-Montagutelli, E.; Mayor, A.; Vecellio, L.; Respaud, R.; Heuzé-Vourc’h, N. Designing inhaled protein therapeutics for topical lung delivery: What are the next steps? Expert Opin. Drug Deliv. 2018, 15, 729–736. [Google Scholar] [CrossRef]
- Pritchard, J.N.; Hatley, R.H.; Denyer, J.; Hollen, D.v. Mesh nebulizers have become the first choice for new nebulized pharmaceutical drug developments. Therapeutic Deliv. 2018, 9, 121–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shak, S.; Capon, D.J.; Hellmiss, R.; Marsters, S.A.; Baker, C.L. Recombinant human DNase I reduces the viscosity of cystic fibrosis sputum. Proc. Natl. Acad. Sci. USA 1990, 87, 9188–9192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Food & Drug Administration. Orphan Drug Designations and Approvals—Alidornase Alfa. Available online: https://www.accessdata.fda.gov/scripts/opdlisting/oopd/detailedIndex.cfm?cfgridkey=754820 (accessed on 8 November 2021).
- Protalix Biotherapeutics. Protalix BioTherapeutics Announces Phase II Clinical Trial Results for alidornase alfa in Cystic Fibrosis. In Proceedings of the 40th European Cystic Fibrosis Society Conference, Seville, Spain, 7–10 June 2017. [Google Scholar]
- Apeiron Biologics. APEIRON Biologics Initiates Phase II Clinical Trial of APN01 for Treatment of COVID-19. 2020. Available online: https://www.apeiron-biologics.com/wp-content/uploads/2020/05/20200402_APEIRON_Phase-2-EU-trial_APN01_ENG.pdf (accessed on 3 February 2022).
- Chan, R.W.; Chan, M.C.; Wong, A.C.; Karamanska, R.; Dell, A.; Haslam, S.M.; Sihoe, A.D.; Chui, W.H.; Triana-Baltzer, G.; Li, Q.; et al. DAS181 inhibits H5N1 influenza virus infection of human lung tissues. Antimicrob. Agents Chemother. 2009, 53, 3935–3941. [Google Scholar] [CrossRef] [Green Version]
- PRNewswire. Ansun Biopharma Enrolls First Patient in Proof of Concept Trial of DAS181 for the Treatment of COVID-19. 2020. Available online: https://www.prnewswire.com/news-releases/ansun-biopharma-enrolls-first-patient-in-proof-of-concept-trial-of-das181-for-the-treatment-of-covid-19-301040739.html (accessed on 3 February 2022).
- Akhter, J.; Queromes, G.; Pillai, K.; Kepenekian, V.; Badar, S.; Mekkawy, A.H.; Frobert, E.; Valle, S.J.; Morris, D.L. The Combination of Bromelain and Acetylcysteine (BromAc) Synergistically Inactivates SARS-CoV-2. Viruses 2021, 13, 425. [Google Scholar] [CrossRef]
- Mucpharm. An Australian Treatment for COVID-19, Despite Mutation. Available online: https://mucpharm.com/covid (accessed on 4 January 2022).
- Weber, A.G.; Chau, A.S.; Egeblad, M.; Barnes, B.J.; Janowitz, T. Nebulized in-line endotracheal dornase alfa and albuterol administered to mechanically ventilated COVID-19 patients: A case series. Mol. Med. 2020, 26, 91. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.H.; Zhao, Y.; Liu, Z.; Zhou, X.; Chen, X.; Xianyu, Y.; Lewis, S.; Fan, L.; Tian, Y.; Chang, N.; et al. Resolution of Coronavirus Disease 2019 Infection and Pulmonary Pathology With Nebulized DAS181: A Pilot Study. Crit. Care Explor. 2020, 2, e0263. [Google Scholar] [CrossRef] [PubMed]
- Chemaly, R.F.; Marty, F.M.; Wolfe, C.R.; Lawrence, S.J.; Dadwal, S.; Soave, R.; Farthing, J.; Hawley, S.; Montanez, P.; Hwang, J.; et al. DAS181 Treatment of Severe Lower Respiratory Tract Parainfluenza Virus Infection in Immunocompromised Patients: A Phase 2 Randomized, Placebo-Controlled Study. Clin. Infect. Dis. 2021, 73, e773–e781. [Google Scholar] [CrossRef] [PubMed]
- Ameratunga, R.; Lehnert, K.; Leung, E.; Comoletti, D.; Snell, R.; Woon, S.T.; Abbott, W.; Mears, E.; Steele, R.; McKee, J.; et al. Inhaled modified angiotensin converting enzyme 2 (ACE2) as a decoy to mitigate SARS-CoV-2 infection. NZ Med. J. 2020, 133, 112–118. [Google Scholar]
- Owoyele, B.V.; Bakare, A.O.; Ologe, M.O. Bromelain: A Review on its Potential as a Therapy for the Management of COVID-19. Niger. J. Physiol. Sci. 2020, 35, 10–19. [Google Scholar]
- Teneback, C.C.; Scanlon, T.C.; Wargo, M.J.; Bement, J.L.; Griswold, K.E.; Leclair, L.W. Bioengineered lysozyme reduces bacterial burden and inflammation in a murine model of mucoid Pseudomonas aeruginosa lung infection. Antimicrob. Agents Chemother. 2013, 57, 5559–5564. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.K.; Ndung’u, T. The potential of lactoferrin, ovotransferrin and lysozyme as antiviral and immune-modulating agents in COVID-19. Future Med. 2020, 15, 609–624. [Google Scholar] [CrossRef]
- Rogan, M.P.; Geraghty, P.; Greene, C.M.; O’Neill, S.J.; Taggart, C.C.; McElvaney, N.G. Antimicrobial proteins and polypeptides in pulmonary innate defence. Respir. Res. 2006, 7, 29. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.L.; Sharma, S.; Singh, T.P. Comments on the Discussion Forum: Oromucosal immunomodulation as clinical spectrum mitigating factor in SARS-CoV-2 infection. Scand. J. Immunol. 2021, 95, e13111. [Google Scholar] [CrossRef]
- Sharma, C.; Jha, N.K.; Meeran, M.F.N.; Patil, C.R.; Goyal, S.N.; Ojha, S. Serratiopeptidase, A Serine Protease Anti-Inflammatory, Fibrinolytic, and Mucolytic Drug, Can Be a Useful Adjuvant for Management in COVID-19. Front. Pharmacol. 2021, 12, 603997. [Google Scholar] [CrossRef]
- Shah, N. Effects of Systemic Enzyme Supplements on Symptoms and Quality of Life in Patients with Pulmonary Fibrosis-A Pilot Study. Medicines 2021, 8, 68. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year Approved a | Drug (Brand Name) | Approved Indication(s); Clinical Trials If Applicable | Mechanism of Action | Reference(s) |
|---|---|---|---|---|
| FDA: Not approved EMA: 2020 | Cysteine protease Imlifidase (Idefirix®) | Desensitization treatment in highly sensitized adult kidney transplant (EMA only and currently in clinical trials in the USA) In clinical trials for: GBS, AMR pre-treatment in DMD and LGMD (to enable gene therapy), and anti-GBM antibody disease | The enzyme is derived from Streptococcus pyogenes and works by degrading IgG antibodies | Idefirix® product website [11] Hansa Biopharma and Sarepta Therapeutics agreement [12] |
| FDA: 2012 EMA: 2022 | Glutamate carboxypeptidase Glucarpidase (Voraxaze®) | Methotrexate-induced renal dysfunction In clinical trials for: Certain types of cancer, including lymphoma, osteosarcoma, and leukemia | Methotrexate hydrolysed to glutamate and less toxic 2,4- diamino-N10-methyl-pteroic acid largely excreted by the liver | Voraxaze® product website [13] |
| FDA: 2012 EMA: 2013 | Microplasmin Ocriplasmin (Jetrea®) | Vitreomacular traction In clinical trials for: exudative age-related macular degeneration, vitreomacular traction/adhesion etc. | Active against fibronectin and laminin, components of the vitreomacular interface. Enzyme dissolves proteins that link the vitreous humour to the retina | Jetrea® SmPC [14] |
| FDA: Not approved EMA: 2012 | Enzyme mixture including bromelain NexoBrid® | Removal of eschar from deep partial-thickness and full-thickness burns of the skin caused by heat or fire In clinical trials for: (thermal) burns | Concentrate of proteolytic enzymes enriched in bromelain | NexoBrid® product website [15] |
| FDA: 2005 EMA: Not approved | Hyaluronidase (Amphadase®; Hylenex Hylenex®; Vitrase®) | Adjuvant to increase absorption/dispersion of other injected drugs; hypodermoclysis; as an adjunct in subcutaneous urography for improving resorption of radiopaque agents In clinical trials for: combination therapy for different cancers, combination therapy for CIDP and MMN | Degradation of hyaluronic acid (a main component of extracellular matrix) | Amphadase® prescribing information [16] |
| FDA: 2002 EMA: 2001 | Urate hydroxylaseRasburicase (Elitek®; Fasturtec®) | Management of plasma uric acid levels during anticancer therapy In clinical trials for: Other types of cancer, including leukemia, lymphoma and tumor lysis syndrome | Recombinant urate-oxidase enzyme produced by a genetically modified Saccharomyces cerevisiae strain. Converts uric acid to allantoin in patients with hyperuricemia. Soluble allantoin is excreted via the kidneys | Elitek® product website [17] |
| FDA: approx. 1999 and later EMA: approx. 2001 and later | Various enzymes for cancer | Various cancers | Nutrient deprivation Remodelling of the fibrotic tumour microenvironment Management of tumour lysis syndrome Inhibition of protein synthesis | Cioini et al. 2022 [18] |
| FDA: 1996 EMA: 1996 | Tissue plasminogen activator Reteplase (Retavase®; Rapilysin®) | Suspected heart attack to dissolve blood clots (use within 12 h) In clinical trials for: myocardial infarction | Activates production of plasmin, which breaks up blood clots | Retevase® product website [19] |
| FDA: 1993 EMA: 1994 | DNase Dornase alfa (Pulmozyme®) | CF In clinical trials for: ARS, ARDS in COVID-19 | Mucolytic that cleaves extracellular DNA, reducing mucus viscosity | US FDA [20] Genentech [21] Lazarus et al. 2019 [10] |
| FDA/EMA: 1990 and later | Various enzymes for ERT | Enzymes for ERT, most are developed to treat inborn errors of metabolism | ERT to make up for a missing or defected native enzyme | Baldo et al. [22] |
| FDA: 1987 EMA: 2002 | Tissue plasminogen activator Alteplase (Activase®; Actilyse®; Cathflo®) | Myocardial infarction with ST elevation; acute ischemic stroke; pulmonary embolism In clinical trials for: kidney disease and certain types of stroke | The recombinant tissue plasminogen activator binds fibrin in the thrombus and cleaves a specific bond in plasminogen which creates plasmin, causing local fibrinolysis | Actilyse® product website [23] |
| FDA: 1978 EMA: 2016 FDA: 1994 EMA: 2016 FDA: 2018 EMA: Not approved | Asparaginase b Crisantaspase Pegaspargase Calaspargase pegol | ALL (in combination with other drugs) In clinical trials for: lymphoma, multiple myeloma, other types of leukemia | Contains asparaginase that reduces blood levels of asparagine, an amino acid that healthy cells can produce and cancer cells cannot, resulting in cancer cell death | Elspar® highlights of prescribing information [24] Oncaspar product website [25] AsparlasTM prescribing information [26] |
| Advantages | Challenges |
|---|---|
| Established delivery method for existing approved drugs | Drug not reaching intended site of action due to clearance mechanisms or degradation/aggregation [94] |
| Ability to deliver high doses of drug directly to the site where it is needed [91] | Drug metabolised too quickly or dissolution upon reaching the lungs [94] |
| Minimizes systemic exposure and systemic side effects [91] | Potential formation of antidrug antibodies (ADAs) [95] which can affect pharmacokinetics, efficacy, and lead to severe adverse events [74] |
| Rapid clinical action | Only a few excipients (needed for formulation stability etc.) have been approved for inhalation [74] |
| Inhalation devices can be used at home by the patient, avoiding the need for a hospital visit | Chronic inhalation with protein/peptide-based therapies may lead to local immunogenicity or irritation to the throat [83,96] |
| Difficulty in ensuring therapy has properties suitable for inhalation such as pH, osmolality, viscosity, and appropriate droplet size | |
| Requirement for development of treatment-specific devices, particularly if agent is unstable |
| Molecule (Drug Name); Company | In Development for: Indication (Phase, Trial Number) | Mechanism of Action (MoA) | Reference(s) |
|---|---|---|---|
| Deoxyribo-nuclease I: Alidornase alfa (AIR DNaseTM, PRX-110); Protalix | In development for: CF (Phase 2, NCT02722122), | Mucolytic that cleaves extracellular DNA, reducing mucus viscosity | US FDA [101] Protalix [102] |
| Deoxyribo-nuclease I: rhDNase | In development for: neutrophilic asthma (Phase 1/2, NCT03994380) | Mucolytic that cleaves extracellular DNA, reducing mucus viscosity | Lazarus et al. 2019 [10] |
| Alunacedase alfa (rhACE2; APN01); | In development for: acute lung injury, pulmonary arterial hypertension; COVID-19 (Phase 1, NCT05065645) | ACE2 is the cellular receptor used by some viruses to enter the cells. Administering rhACE2 is expected to function as a decoy for viruses to block viral entry | Apeiron Biologics press release 2020 [103] |
| Sialidase (Fludase, DAS181); Remin Hospital of Wuhan University; Ansun Biopharma | In development for:
| Catalyses sialic acid cleavage from glycoproteins and glycolipids in the lung epithelium, which interferes with the lifecycle of some viruses | Chan et al. 2009 [104] PRNewswire press release [105] |
| BromAcTM; mucpharm | In development for: COVID-19 with respiratory complications | Degrades the spike protein of the SARS-CoV-2 virus, rendering the virus unable to infect cells | Akhter et al. 2021 [106] mucpharm company website [107] |
| IPX formulation; Inspira Pharmaceuticals | In development for: COVID-19 and other RTIs | MOA not yet known | Inspira Pharmaceuticals press release (2021) [89] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanderstocken, G.; Woolf, N.L.; Trigiante, G.; Jackson, J.; McGoldrick, R. Harnessing the Potential of Enzymes as Inhaled Therapeutics in Respiratory Tract Diseases: A Review of the Literature. Biomedicines 2022, 10, 1440. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061440
Vanderstocken G, Woolf NL, Trigiante G, Jackson J, McGoldrick R. Harnessing the Potential of Enzymes as Inhaled Therapeutics in Respiratory Tract Diseases: A Review of the Literature. Biomedicines. 2022; 10(6):1440. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061440
Chicago/Turabian StyleVanderstocken, Gilles, Nicholas L. Woolf, Giuseppe Trigiante, Jessica Jackson, and Rory McGoldrick. 2022. "Harnessing the Potential of Enzymes as Inhaled Therapeutics in Respiratory Tract Diseases: A Review of the Literature" Biomedicines 10, no. 6: 1440. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061440