Does Medication-Related Osteonecrosis of the Jaw Influence the Quality of Life of Cancer Patients?

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B. American Association of Oral and Maxillofacial Surgeons Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaws—2009 Update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef] [PubMed]
- Di Fede, O.; Panzarella, V.; Mauceri, R.; Fusco, V.; Bedogni, A.; Muzio, L.L.; Board, S.O.; Campisi, G. The Dental Management of Patients at Risk of Medication-Related Osteonecrosis of the Jaw: New Paradigm of Primary Prevention. BioMed Res. Int. 2018, 2018, 2684924. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Hamadeh, I.S.; Song, S.; Katz, J.; Moreb, J.S.; Langaee, T.Y.; Lesko, L.J.; Gong, Y. Osteonecrosis of the Jaw in the United States Food and Drug Administration’s Adverse Event Reporting System (FAERS). J. Bone Miner. Res. 2016, 31, 336–340. [Google Scholar] [CrossRef] [Green Version]
- Lahtinen, S.; Koivunen, P.; Ala-Kokko, T.; Laurila, P.; Kaarela, O.; Liisanantti, J.H. Quality of life after free flap surgery for cancer of the head and neck in patients with or without postoperative complications. Eur. Arch. Oto Rhino Laryngol. 2018, 275, 2575–2584. [Google Scholar] [CrossRef]
- Momeni, A.; Kim, R.Y.; Kattan, A.; Lee, G.K. Microsurgical head and neck reconstruction after oncologic ablation: A study analyzing health-related quality of life. Ann. Plast. Surg. 2013, 70, 462–469. [Google Scholar] [CrossRef]
- Romeo, U.; Galanakis, A.; Marias, C.; Vecchio, A.D.; Tenore, G.; Palaia, G.; Vescovi, P.; Polimeni, A. Observation of Pain Control in Patients with Bisphosphonate-Induced Osteonecrosis Using Low Level Laser Therapy: Preliminary Results. Photomed. Laser Surg. 2011, 29, 447–452. [Google Scholar] [CrossRef]
- Vescovi, P.; Merigo, E.; Meleti, M.; Fornaini, C.; Namour, S.; Manfredi, M. Nd: YAG laser biostimulation of bisphosphonate-associated necrosis of the jawbone with and without surgical treatment. Br. J. Oral Maxillofac. Surg. 2007, 45, 628–632. [Google Scholar] [CrossRef]
- McGowan, K.; McGowan, T.; Ivanovski, S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review. Oral Dis. 2017, 24, 527–536. [Google Scholar] [CrossRef]
- Arraras, J.I.; De La Vega, F.A.; Asin, G.; Rico, M.; Zarandona, U.; Eito, C.; Cambra, K.; Barrondo, M.; Errasti, M.; Verdún, J.; et al. The EORTC QLQ-C15-PAL questionnaire: validation study for Spanish bone metastases patients. Qual. Life Res. 2014, 23, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Caissie, A.; Zeng, L.; Nguyen, J.; Zhang, L.; Jon, F.; Dennis, K.; Holden, L.; Culleton, S.; Koo, K.; Tsao, M.; et al. Assessment of Health-related Quality of Life with the European Organization for Research and Treatment of Cancer QLQ-C15-PAL after Palliative Radiotherapy of Bone Metastases. Clin. Oncol. 2012, 24, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Groenvold, M.; Petersen, M.A.; Aaronson, N.K.; Arraras, J.I.; Blazeby, J.M.; Bottomley, A.; Fayers, P.M.; de Graeff, A.; Hammerlid, E.; Kaasa, S.; et al. The development of the EORTC QLQ-C15-PAL: A shortened questionnaire for cancer patients in palliative care. Eur. J. Cancer 2006, 42, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Soelver, L.; Oestergaard, B.; Rydahl-Hansen, S.; Wagner, L. Advanced cancer patients’ self-assessed physical and emotional problems on admission and discharge from hospital general wards—A questionnaire study. Eur. J. Cancer Care 2012, 21, 667–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, J.; Mannion, C. Medication-related osteonecrosis of the jaws and quality of life: review and structured analysis. Br. J. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hagell, P.; Westergren, A.; Årestedt, K. Beware of the origin of numbers: Standard scoring of the SF-12 and SF-36 summary measures distorts measurement and score interpretations. Res. Nurs. Health 2017, 40, 378–386. [Google Scholar] [CrossRef]
- Capocci, M.; Romeo, U.; Guerra, F.; Mannocci, A.; Tenore, G.; Annibali, S.; Ottolenghi, L. Medication-related osteonecrosis of the jaws (MRONJ) and quality of life evaluation: a pilot study. Clin. Ter. 2017, 168, e253–e257. [Google Scholar] [CrossRef]
- Cassoni, A.; Romeo, U.; Terenzi, V.; Della Monaca, M.; Rajabtork Zadeh, O.; Raponi, I.; Fadda, M.T.; Polimeni, A.; Valentini, V. Adalimumab: Another Medication Related to Osteonecrosis of the Jaws? Case Rep. Dent. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Allen, M.R.; Burr, D.B. The Pathogenesis of Bisphosphonate-Related Osteonecrosis of the Jaw: So Many Hypotheses, So Few Data. J. Oral Maxillofac. Surg. 2009, 67 (Suppl. 5), 61–70. [Google Scholar] [CrossRef] [Green Version]
- Rosella, D.; Papi, P.; Giardino, R.; Cicalini, E.; Piccoli, L.; Pompa, G. Medication-related osteonecrosis of the jaw: Clinical and practical guidelines. J. Int. Soc. Prev. Community Dent. 2016, 6, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Marx, R.E. Oral and Intravenous Bisphosphonate-Induced Osteonecrosis of the Jaws, History, Etiology, Prevention, and Treatment; Quintessence Publishing Company: Batavia, IL, USA, 2011. [Google Scholar]
- Stanton, D.C.; Balasanian, E. Outcome of Surgical Management of Bisphosphonate-Related Osteonecrosis of the Jaws: Review of 33 Surgical Cases. J. Oral Maxillofac. Surg. 2009, 67, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Freiberger, J.; Padilla-Burgos, R.; McGraw, T.; Suliman, H.B.; Kraft, K.H.; Stolp, B.W.; Moon, R.E.; Piantadosi, C.A. Utility of hyperbaric oxygen in treatment of bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2012, 70, 1573–1583. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; De Vincentiis, M.; Valentini, V.; Musio, D.; Mezi, S.; Lo Mele, L.; Terenzi, V.; D’Aguanno, V.; Cassoni, A.; Di Brino, M.; et al. Follow-up program in head and neck cancer. Crit. Rev. Oncol. 2017, 113, 151–155. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; De Vincentiis, M.; Valentini, V.; Musio, D.; Mezi, S.; Lo Mele, L.; Della Monaca, M.; D’Aguanno, V.; Terenzi, V.; Di Brino, M.; et al. Management of salivary gland malignant tumor: the Policlinico Umberto I, “Sapienza” University of Rome Head and Neck Unit clinical recommendations. Crit. Rev. Oncol. 2017, 120, 93–97. [Google Scholar] [CrossRef]
- Lamb, B.W.; Brown, K.F.; Nagpal, K.; Vincent, C.; Green, J.S.; Sevdalis, N. Quality of Care Management Decisions by Multidisciplinary Cancer Teams: A Systematic Review. Ann. Surg. Oncol. 2011, 18, 2116–2125. [Google Scholar] [CrossRef]
- Müller-Nordhorn, J.; Roll, S.; Willich, S.N. Comparison of the short form (SF)-12 health status instrument with the SF-36 in patients with coronary heart disease. Heart 2004, 90, 523–527. [Google Scholar] [CrossRef]
- Tucker, G.; Adams, R.; Wilson, D. Results from several population studies show that recommended scoring methods of the SF-36 and the SF-12 may lead to incorrect conclusions and subsequent health decisions. Qual. Life Res. 2014, 23, 2195–2203. [Google Scholar] [CrossRef]
- Miksad, R.A.; Lai, K.C.; Dodson, T.B.; Woo, S.B.; Treister, N.S.; Akinyemi, O.; Bihrle, M.; Maytal, G.; August, M.; Gazelle, G.S.; et al. Quality of Life Implications of Bisphosphonate-Associated Osteonecrosis of the Jaw. Oncologist 2011, 16, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Romeo, U.; Tenore, G.; Cassoni, A.; Rocchetti, F.; Mohsen, A.; Pompa, G.; Valentini, V.; Polimeni, A. A multidisciplinary team for the management of oral cancer: A project called MoMax. Ann. Stomatol. 2018, 9, 134–140. [Google Scholar]
- Nortvedt, M.W.; Riise, T.; Myhr, K.-M.; Nyland, H.I. Performance of the SF-36, SF-12, and RAND-36 Summary Scales in a Multiple Sclerosis Population. Med. Care 2000, 38, 1022–1028. [Google Scholar] [CrossRef]
- Pickard, A.S.; Johnson, J.A.; Penn, A.; Lau, F.; Noseworthy, T. Replicability of SF-36 summary scores by the SF-12 in stroke patients. Stroke 1999, 30, 1213–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busija, L.; Pausenberger, E.; Haines, T.P.; Haymes, S.; Buchbinder, R.; Osborne, R.H. Adult measures of general health and health-related quality of life: Medical Outcomes Study Short Form 36-Item (SF-36) and Short Form 12-Item (SF-12) Health Surveys, Nottingham Health Profile (NHP), Sickness Impact Profile (SIP), Medical Outcomes Study Short Form 6D (SF-6D), Health Utilities Index Mark 3 (HUI3), Quality of Well-Being Scale (QWB), and Assessment of Quality of Life (AQoL). Arthritis Care Res. 2011, 63 (Suppl. 11), S383–S412. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Distribution (%) |
|---|---|
| Age | |
| Under 60 | 4 (20%) |
| Over 60 | 16 (80%) |
| Gender | |
| Male | 8 (40%) |
| Female | 12 (60%) |
| Marital status | |
| Single | 5 (25%) |
| Married | 14 (70%) |
| Tumor | |
| Cancer | 8 (40%) |
| Cancer with bone metastasis | 12 (60%) |
| Anti-resorptive medication timing | |
| Past | 15 (75%) |
| Current | 5 (25%) |
| Active principle | |
| Zoledronic acid | 9 (45%) |
| Clodronic acid | 1 (5%) |
| Alendronic acid | 1 (5%) |
| Denosumab (one dose every month) | 3 (15%) |
| Adalimumab | 1 (5%) |
| Combination | 5 (25%) |
| Method of administration | |
| I.V | 11 (55%) |
| I.M/S.C | 5 (25%) |
| Oral | 1 (5%) |
| Association | 3 (15%) |
| Anti-resorptive medications duration | |
| <3 years | 8 (40%) |
| >3 years | 12 (60%) |
| I.V. < 8 infusions | 2 (10%) |
| I.V. + 8 infusions | 12 (60%) |
| MRONJ stage | |
| 0 | 6 (30%) |
| I | 2 (10%) |
| II | 11 (55%) |
| III | 1 (5%) |
| Localization | |
| Maxilla | 3 (15%) |
| Mandible | 12 (60%) |
| Both | 5 (25%) |
| Variable | n | Score of PCS-12 Median (min–max) | p-Value | Score of MCS-12 Median (max–min) | p-Value |
|---|---|---|---|---|---|
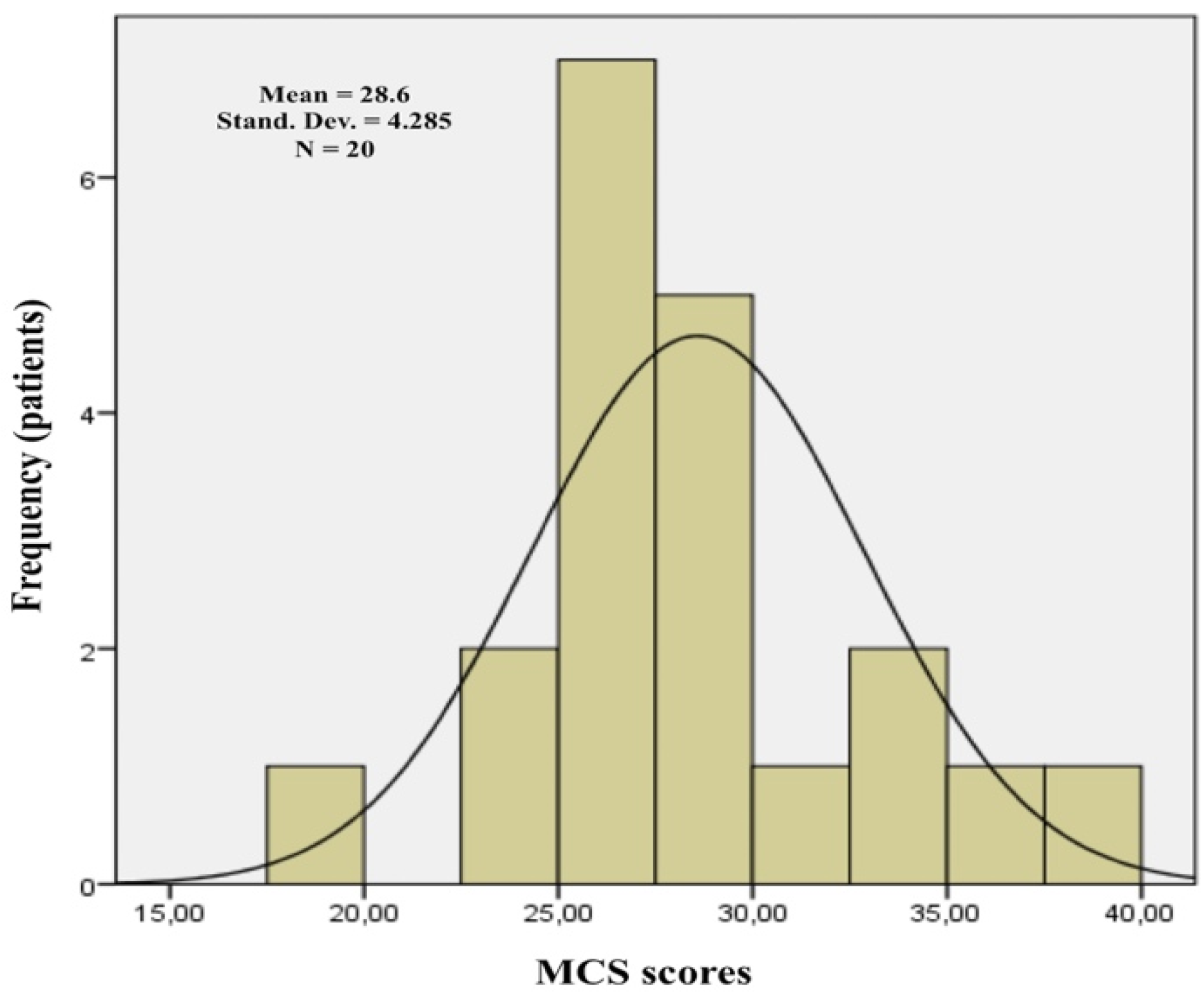
| All the sample | 20 | 53.6 (43.7–60.6) | 28.6 (19.6–37.9) | ||
| Age | 0.06 | 0.018 | |||
| Under 60 | 4 | 48.8 (44.5–53.4) | 31.9 (29.9–35.2) | ||
| Over 60 | 16 | 56.2 (43.7–60.6) | 27.4 (19.6–37.97) | ||
| Gender | 0.70 | 0.22 | |||
| Male | 8 | 54.02 (43.7–60.3) | 28.789 (26.2–37.97) | ||
| Female | 12 | 54.5 (44.5–60.6) | 27.4 (19.6–35.2) | ||
| Marital status | 0.71 | 0.58 | |||
| Single | 5 | 54.7 (43.8–60.1) | 27.5 (25.4–37.97) | ||
| Married | 14 | 54.5 (44.5–60.6) | 27.7 (19.6–35.2) | ||
| Not declared | 1 | 53.4 | 30.8 | ||
| Tumor | 0.28 | 0.68 | |||
| Cancer | 8 | 57.4 (50.2–60.1) | 27.7 (24.4–29.7) | ||
| Cancer with bone metastasis | 12 | 52.96 (44.5–60.6) | 28.6 (19.6–37.97) | ||
| Anti-resorptive medication timing | 0.86 | 0.73 | |||
| Past | 15 | 53.5 (43.7–60.6) | 27.9 (19.6–37.97) | ||
| Current | 5 | 57.1 (45–60.1) | 27.4 (25.4–35.2) | ||
| Active principle | 0.57 | 0.54 | |||
| Zoledronic acid | 9 | 54.7 (43.7–60.6) | 27.5 (19.6–37.97) | ||
| Clodronic acid | 1 | 57.1 | 28.8 | ||
| Alendronic acid | 1 | 60.1 | 25.4 | ||
| Denosumab (one dose every month) | 3 | 57.8 (50.8–60.3) | 27.9 (26.5–29.8) | ||
| Adalimumab | 1 | 53.5 | 23.6 | ||
| Combination | 5 | 50.2 (45–59.4) | 29.7 (26.3–35.2) | ||
| Method of administration | 0.38 | 0.38 | |||
| I.V | 11 | 53.4 (43.7–60.6) | 27.5 (19.6–37.97) | ||
| I.M/S.C | 5 | 57.1 (50.8–60.3) | 27.9 (23.6–29.8) | ||
| Oral | 1 | 60.1 | 25.4 | ||
| Association | 3 | 52.6 (45–59.4) | 32.99 (27.4–35.2) | ||
| Anti-resorptive medications duration | 0.25 | 0.45 | |||
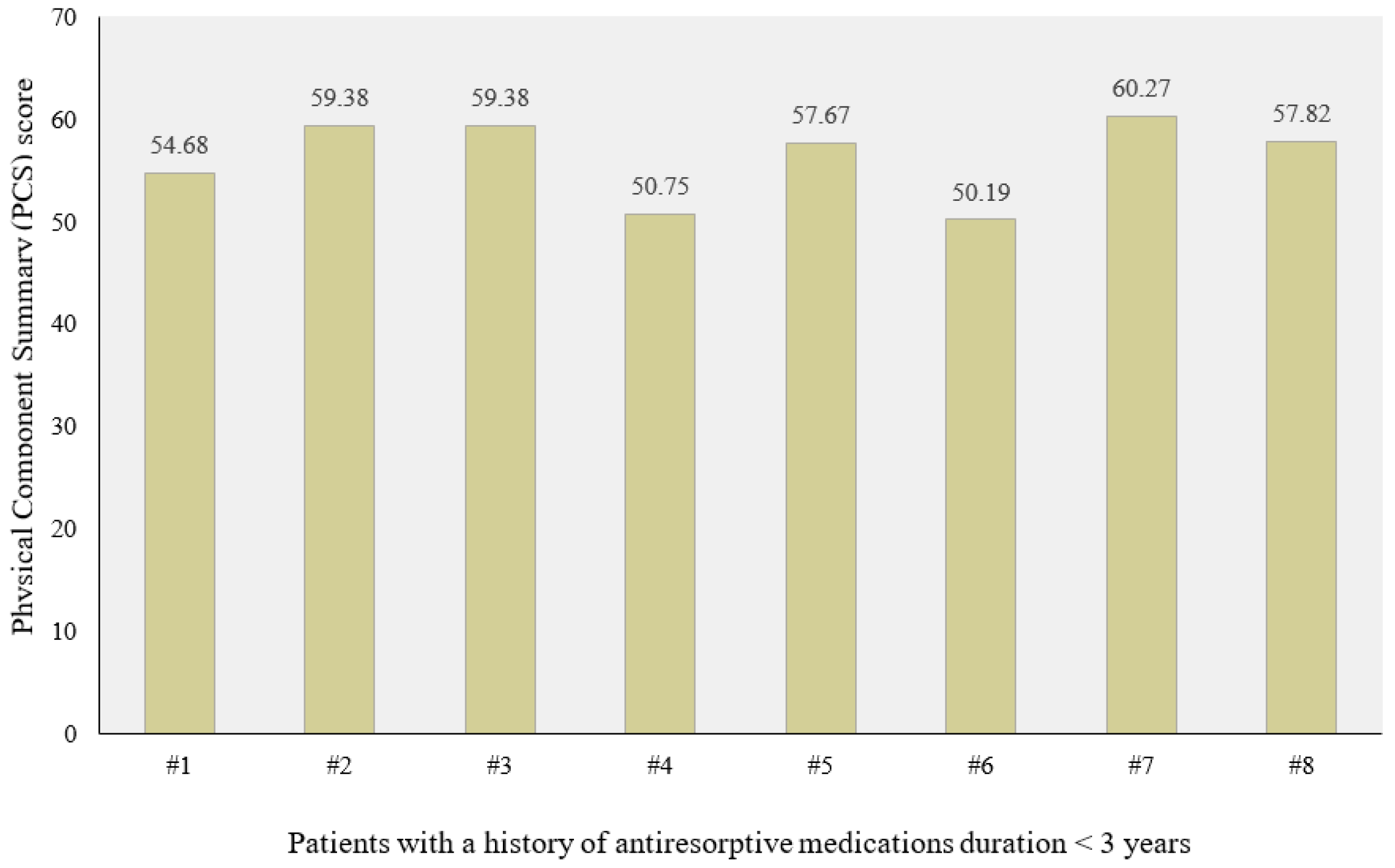
| <3 years | 8 | 57.1 (50.2–60.3) | 29.3 (26.6–37.97) | ||
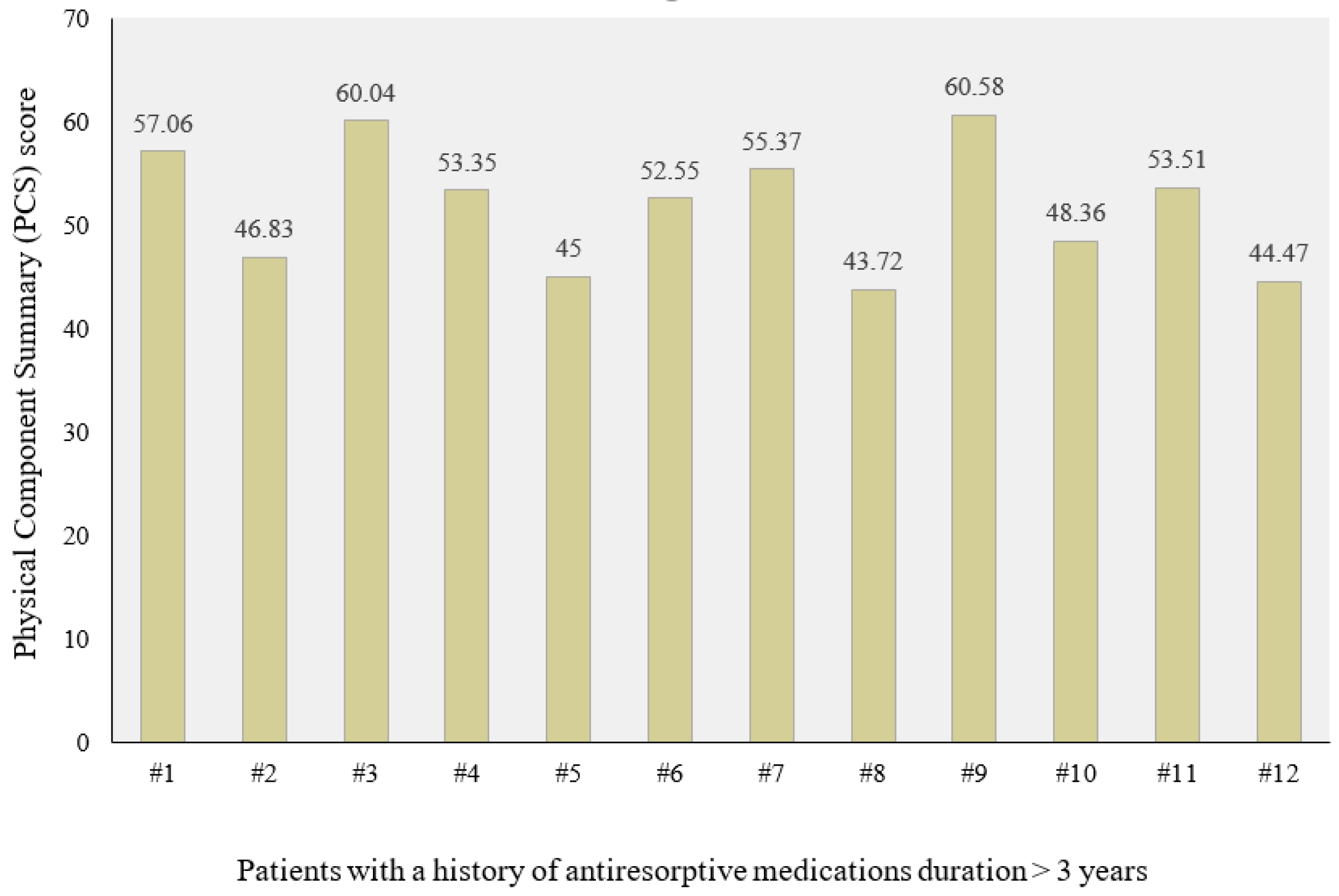
| >3 years | 12 | 51.7 (47.7–60.6) | 28.1 (19.6–35.2) | ||
| I.V < 8 infusions | 2 | 57.4 (55.4–59.4) | 25.9 (24.4–27.4) | ||
| I.V + 8 infusions | 12 | 51.4 (43.7–60.6) | 29.8 (19.6–37.97) | ||
| MRONJ stage | 0.85 | 0.15 | |||
| 0 | 6 | 53.4 (46.8–60.1) | 27.5 (23.6–30.8) | ||
| I | 2 | 51.4 (45–57.7) | 31.4 (27.5–35.2) | ||
| II | 11 | 55.4 (43.7–60.6) | 27.4 (19.6–34.5) | ||
| III | 1 | 54.7 | 37.97 | ||
| Localization | 0.47 | 1.00 | |||
| Maxilla | 3 | 54.1 (43.7–60.3) | 27.438 (23.6–37.97) | ||
| Mandible | 12 | 57.8 (45–60.6) | 27.9 (19.6–35.2) | ||
| Both | 5 | 54.3 (46.8–60.1) | 28.2 (25.4–30.8) | ||
| Variable | PCS-12 | MCS-12 | ||
|---|---|---|---|---|
| β | p-Value | β | p-Value | |
| Age | −0.188 | 0.55 | −0.123 | 0.77 |
| Gender | 0.632 | 0.15 | −0.633 | 0.25 |
| Marital status | 0.320 | 0.37 | −0.136 | 0.76 |
| Anti-resorptive medication timing | −0.830 | 0.08 | 1.018 | 0.09 |
| Anti-resorptive medications duration | −1.137 | 0.03 | 0.471 | 0.32 |
| Number of infusions | 0.715 | 0.10 | −0.652 | 0.21 |
| MRONJ stage | −0.007 | 0.98 | 0.410 | 0.31 |
| Localization | 0.729 | 0.09 | −0.643 | 0.21 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tenore, G.; Mohsen, A.; Rossi, A.F.; Palaia, G.; Rocchetti, F.; Cassoni, A.; Valentini, V.; Ottolenghi, L.; Polimeni, A.; Romeo, U. Does Medication-Related Osteonecrosis of the Jaw Influence the Quality of Life of Cancer Patients? Biomedicines 2020, 8, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8040095
Tenore G, Mohsen A, Rossi AF, Palaia G, Rocchetti F, Cassoni A, Valentini V, Ottolenghi L, Polimeni A, Romeo U. Does Medication-Related Osteonecrosis of the Jaw Influence the Quality of Life of Cancer Patients? Biomedicines. 2020; 8(4):95. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8040095
Chicago/Turabian StyleTenore, Gianluca, Ahmed Mohsen, Antonella Francesca Rossi, Gaspare Palaia, Federica Rocchetti, Andrea Cassoni, Valentino Valentini, Livia Ottolenghi, Antonella Polimeni, and Umberto Romeo. 2020. "Does Medication-Related Osteonecrosis of the Jaw Influence the Quality of Life of Cancer Patients?" Biomedicines 8, no. 4: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8040095